
Abstract
BACKGROUND:
Intracellular calcium overload has been implicated in various pathological conditions including ischemia reperfusion injury. This study aims to explore the effect and probable mechanism of dantrolene, a ryanodine receptor and intracellular calcium antagonist, on the skeletal muscle ischemia reperfusion injury.
MATERIALS AND METHODS:
SD rats were randomly divided into three groups: sham group which underwent anaesthesia and exposure of femoral vein, reperfusion group that received 2 h ischemia and the amount of diluent via femoral vein before 4 h reperfusion, dantrolene group that underwent 2 h ischemia and was given 2 mg/kg dantrolene via femoral vein before 4 h reperfusion. The parameters measured at the end of reperfusion included serum maleic dialdehyde (MDA), tissue myeloperoxidase (MPO) and muscle histology, as well as serum TNF-α and IL-10.
RESULTS:
Levels of MDA, MPO and TNF-α increased in the reperfusion group, whereas the relevant expressions in the dantrolene group decreased significantly. Histological examination demonstrated significant improvements between the same both groups. IL-10 reflected the protection observed above with a significant up-regulation of expression after dantrolene administration.
CONCLUSION:
Ryanodine receptor antagonist dantrolene exerted a significant protective effect against the inflammatory injury of skeletal muscle ischemia reperfusion. The underlying molecular mechanism is probably related to the suppression of TNF-α levels and the increment of IL-10 expression.
Introduction
The ischemia reperfusion injury is very common yet inevitable among clinical practice, which often contributes to high disability rate of disease. Calcium overload, oxygen free radicals, and inflammatory reactions mediated by white cells have been proved to play the major roles in the pathogenesis of ischemia reperfusion injury [1–3]. Hence, restoring the abnormal intracellular calcium homeostasis could be a potential therapeutic strategy against reperfusion injury.
Researches on the ryanodine receptor and intracellular calcium antagonist dantrolene have advanced rapidly in recent years. Dantrolene is a compound that regulates endoplasmic reticulum and sarcoplasmic reticulum calcium release by interacting with the ryanodine receptor. It has been strongly suggested to mediate cardioprotection against heart diseases, including ischemia reperfusion injury and postischemic arrhythmia [4–7]. Other studies showed that dantrolene was capable of exerting protective effects to organs such as brain, spinal cord, liver and kidney under ischemic conditions [7–11]. However, the report about its effects in the skeletal muscle ischemia reperfusion is currently poor.
Here, by constructing rat ischemia reperfusion model, this study tried to investigate the effect and probable mechanism of dantrolene on the skeletal muscle ischemia reperfusion injury. We hypothesized that the blockade of ryanodine receptor with dantrolene could protect the skeletal muscle against inflammatory damage during ischemia reperfusion, by affecting multiple inflammatory related cytokines including TNF-α and IL-10 [11, 12].
Materials and methods
The animal study protocol applied in this work was approved by Laboratory Animal Ethics Committee of the medical university (Ref nr. SYXK(FJ)2008-0001). Twenty-four SPF-grade male SD rats (weighing 280±50 g) were selected and randomly divided into three groups (n = 8/group): sham group which underwent anaesthesia and exposure of left femoral vein, reperfusion group that received 2 h ischemia and the amount of diluent (mannitol 5%) via left femoral vein before 4 h reperfusion, dantrolene group that underwent 2 h ischemia and was given 2 mg/kg dantrolene (resolved in mannitol 5%) via left femoral vein before 4 h reperfusion [13].
All rats were subjected to 4 h abrosia but had full access to water before experiment. Then a tourniquet was applied to the left hind limb to creat an ischemia model [14]. The tourniquet was released after 2 h ischemia and the animal was allowed to reperfuse for 4 h. At the beginning of reperfusion, animals received the procedures respectively as mentioned above. After 4 h reperfusion, blood and gastrocnemius muscle samples were collected to include serum maleic dialdehyde (MDA), tissue myeloperoxidase (MPO) and muscle histology as markers of ischemic damage. Serum TNF-α and IL-10 were measured in Bio-Rad model 550 automatic meter using enzyme linked immunosorbent assay (ELISA) kits from R&D Systems Inc.
Samples for serum MDA and tissue MPO were processed with test kits of Nanjing Jiancheng Bioengineering Institute; then they were analyzed by UV4802 double beam spectrophotometer (Unico Instrument Co., Ltd.). Muscle samples were maintained in formalin 10% before they were cut into parafin sections and stained in hematoxylin and eosin (H&E). A pathologist who was experienced in the assessment of ischemic reperfusion injury carefully observed the muscle light histology under Olympus BX51 biomicroscope. He was blinded to the group of samples being evaluated.
All groups were subjected to a complete statistical analysis in SPSS17 software after experiment. Results were expressed as mean±standard deviation (M±SD) with the statistical significance set at a P value of <0.05. Homogeneity of variance among groups was examined by Levene’s test. If there was a statistical significance, then one-way analysis of variance (ANOVA) and SNK-q test were used for comparisons. Otherwise, the Games-Howell test was used for data analysis.
Results
The levels of serum MDA and tissue MPO increased dramatically after reperfusion as reperfusion group compared to sham group. However, these marker levels were significantly down-regulated in dantrolene group where dantrolene was given before reperfusion (Fig. 1). There was a statistical difference between dantrolene group and reperfusion group (P < 0.05).
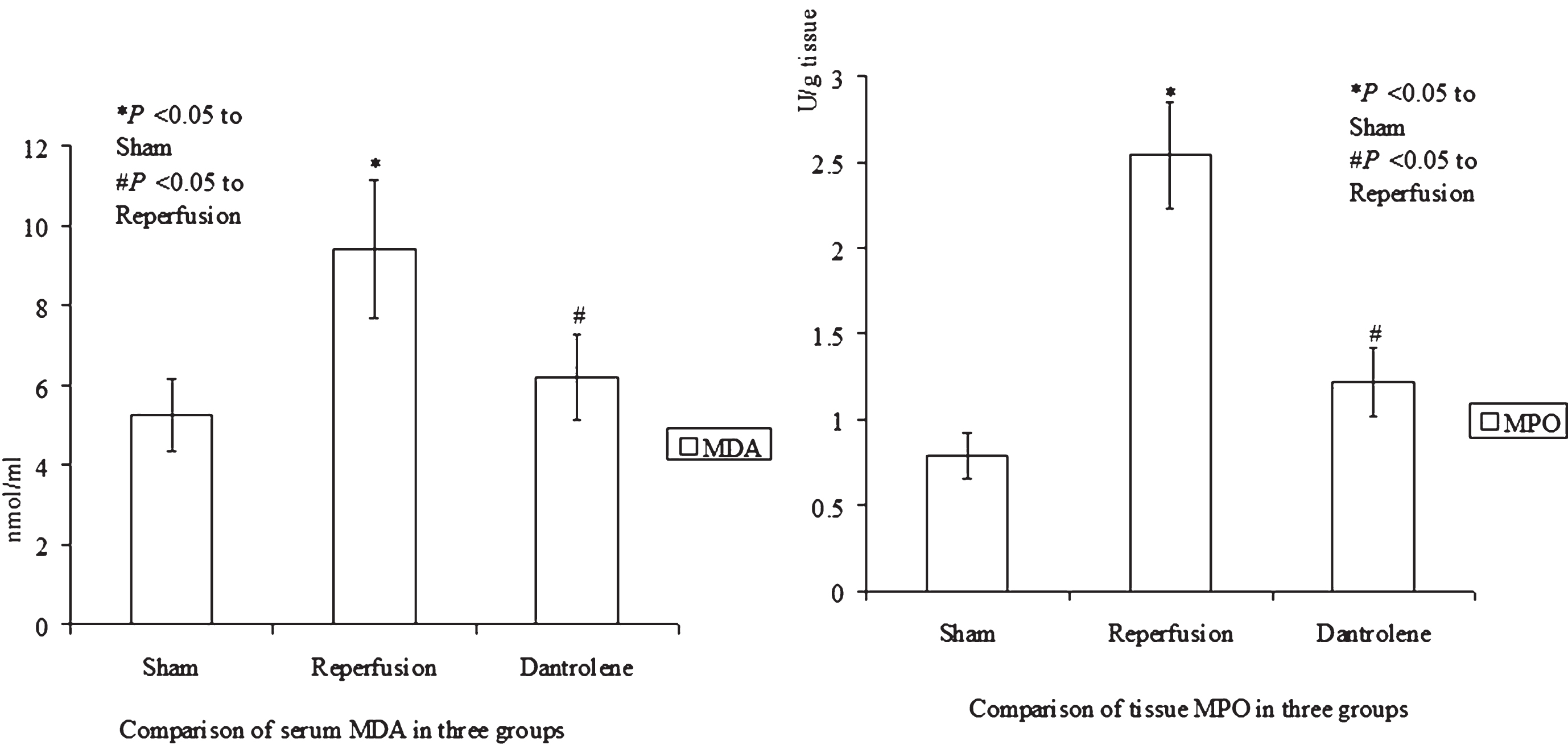
Serum MDA and tissue MPO tests showing statistical differences among sham, reperfusion and dantrolene groups (M±SD).
Histological examination showed an evident improvement of leukocyte aggregation in dantrolene group when compared with reperfusion group. Important congestion, vacuolization and necrosis of the ischemic tissue were significantly less in dantrolene group than in reperfusion group (Fig. 2).
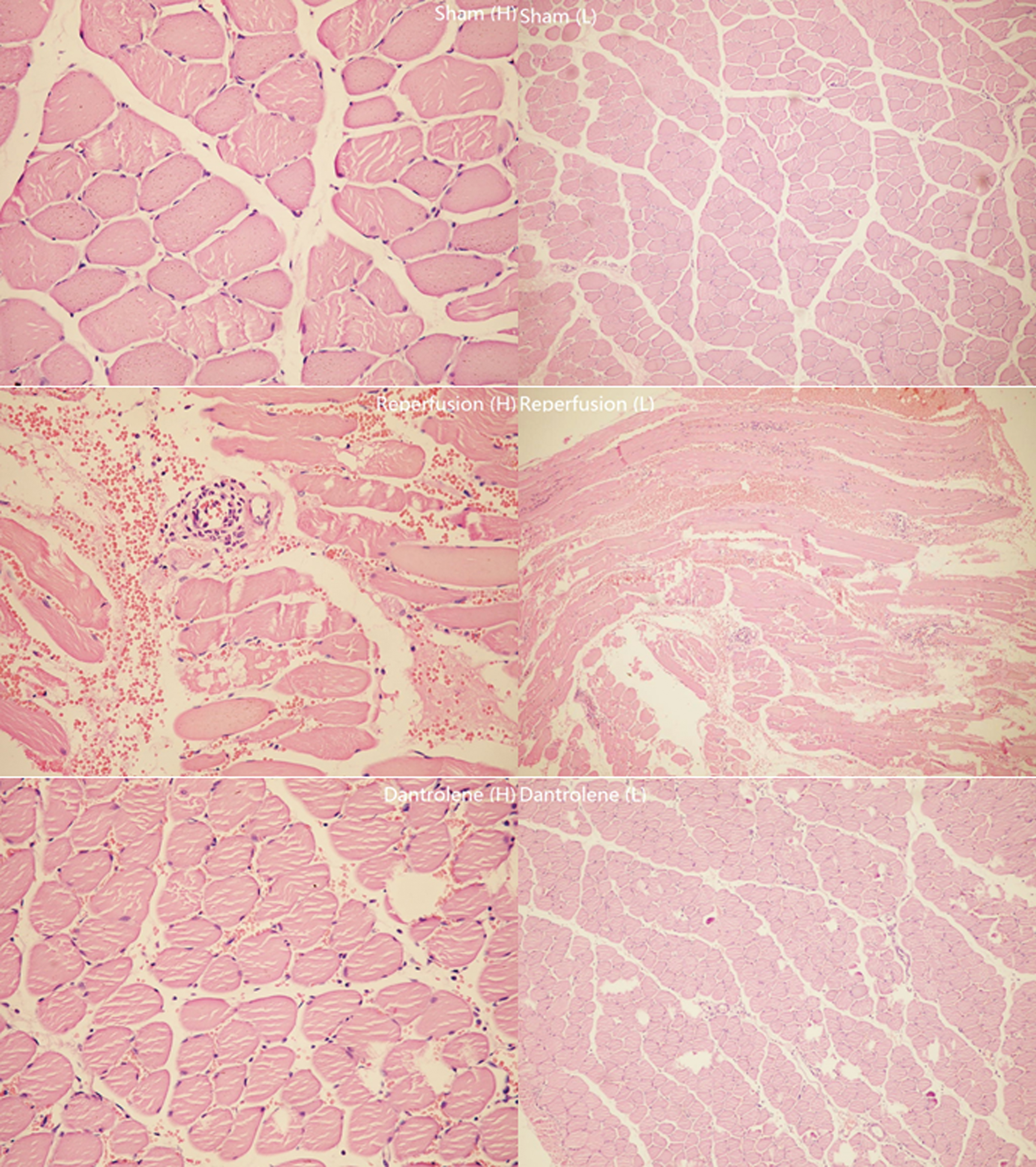
Light microscopy at low magnification (L) (100×) and high magnification (H) (400×) observed in three groups. Pathognomonic vacuolization and necrosis were consistent with reperfusion group, and very limited necrosis, vacuolization and congestion were found in dantrolene group.
Decreased serum levels of TNF-α and increased levels of IL-10 reflected the protective effect observed in the above tests and muscle histopathology. High serum levels of TNF-α were seen in reperfusion group as compared to low levels found in dantrolene group (P < 0.05) (Fig. 3). As for serum IL-10, a significant increase was observed in dantrolene group with statistical difference when compared with reperfusion group (P < 0.05) (Fig. 3).
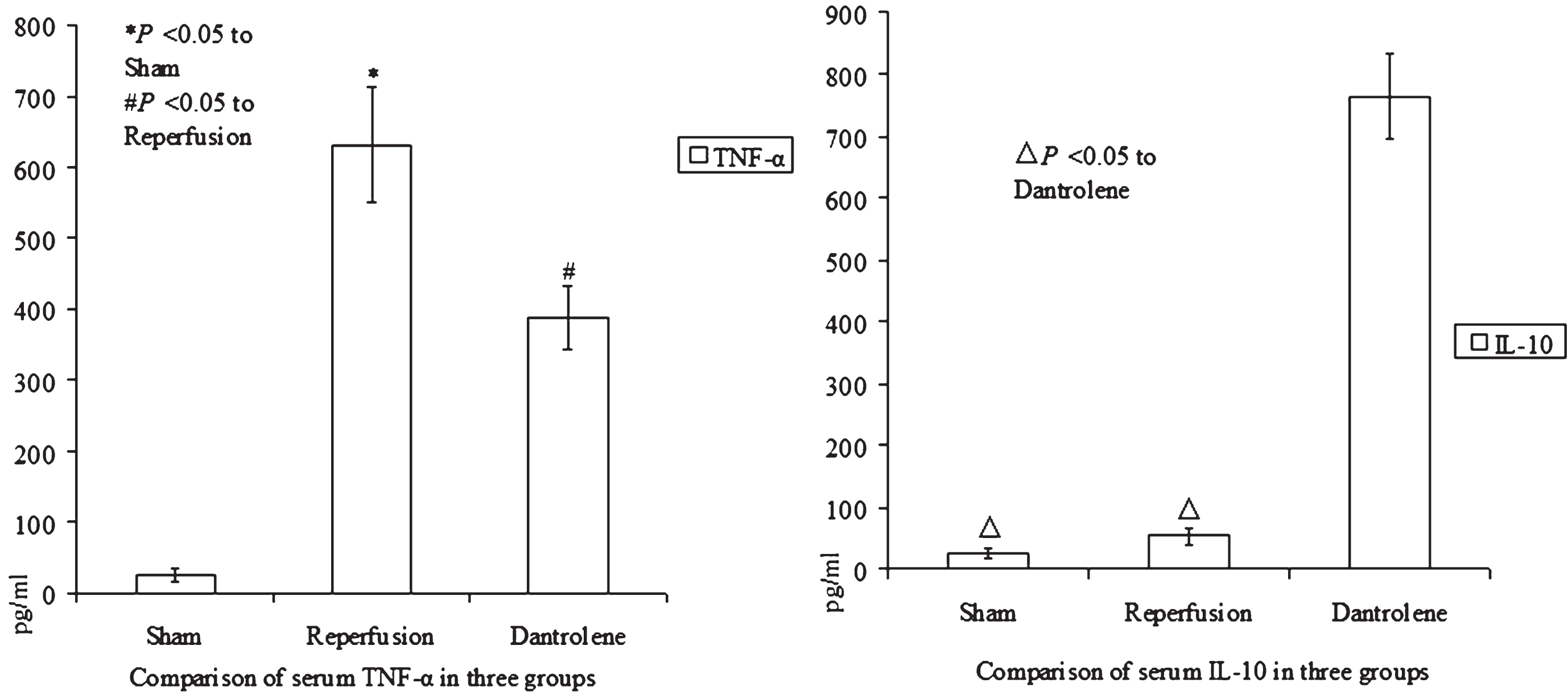
Serum levels of TNF-α and IL-10 obtained through ELISA. Note the significant decrease of TNF-α and increase of IL-10 in dantrolene group as compared to reperfusion group (M±SD).
This study demonstrated that ryanodine receptor antagonist dantrolene could offer significant protection against rat skeletal muscle ischemia reperfusion injury when given at the beginning of reperfusion. The outcome was, at least partially, due to the modulation of multiple inflammatory related cytokines including TNF-α and IL-10, as it was revealed in this work.
There were some factors in this experiment that needed further investigation, such as changes of dantrolene dose, timing of administration, route of administration, as well as sample size, each of which may influence the results. Besides, the nonexclusive pathogenesis of ischemia reperfusion injury could also account for the variation in study outcomes.
Intracellular calcium and ryanodine receptor
Intracellular calcium overload is believed to play a key role in the cascade that leads to cell damage after ischemia reperfusion. The uncontrolled nonadequate increase of cytosolic calcium concentration during ischemia reperfusion activates various intracellular signaling pathways, which result in severe cell injuries even apoptosis [15–19].
So far as we know, there exist two families of intracellular calcium-releasing channels: ryanodine receptors and inositol 1,4,5-trisphosphate receptors, both of which compose on endoplasmic reticulum and sarcoplasmic reticulum. The former can be basically classified into three subtypes: ryanodine receptor-1, ryanodine receptor-2 and ryanodine receptor-3, which are widely expressed in skeletal muscle, heart, brain and smooth muscle.
Studies suggest that the asynchronous and inhomogeneous increase of intracellular calcium during ischemia reperfusion consists of two different phases. At first, the elementary calcium inflow activated calcium/calmodulin-dependent protein kinase type II then hyperphosphorylated the ryanodine receptor, consistent with causing a postischemic calcium leak from endoplasmic reticulum and sarcoplasmic reticulum [17–21]. Secondly, the influx of calcium through cell membrane is primarily responsible for the persistent increase of intracellular calcium concentration [22]. Thus, the release of calcium from endoplasmic reticulum and sarcoplasmic reticulum is of decisive importance in the early phase of reperfusion.
Therefore, the initial inhibition of calcium release resulted from suppression of ryanodine receptor activity may effectively alleviate the inflammatory damage during ischemia reperfusion. And ryanodine receptor antagonist dantrolene has been supposed to inhibit the release of calcium from endoplasmic reticulum and sarcoplasmic reticulum in the cells [23].
TNF-α and IL-10
TNF-α is the best-known member of tumor necrosis factor superfamily which were originally identified by their ability to cause cell death. It is a mainly monocyte-derived cytokine that has been implicated in tumor regression, septic shock, and also a wide range of ischemic diseases involving heart, brain, lung and liver [24–33].
As is known, the increase of TNF-α has been associated with inflammation, cell damage and lack of protection. Its necrotic effect on cells is mediated through tumor necrosis factor receptors which activate various apoptotic pathways [34–37]. In this study, treatment with dantrolene at the beginning of reperfusion had a down-regulating effect on the levels of TNF-α, accompanied by less inflammatory injury and histologic damage.
In humans, IL-10 is mostly produced by monocytes, while its expression is minimal in unstimulated tissues [38]. It has been shown that IL-10 is capable of inhibiting synthesis of multiple pro-inflammatory cytokines, and is associated with the limitation of inflammation and prevention of inappropriate immunological reactions [39–42].
Beneficial effects of IL-10 were observed in various inflammatory and autoimmune animal models including IL-10 knockout mice [40–44]. Expression of IL-10 from transfected tumor cell lines in IL-10 transgenic mice or dosing with IL-10 leads to control of primary tumor growth and decreased metastatic burden [45, 46]. Investigations suggest that IL-10 can block NF-κB activity, and is involved in the regulation of JAK-STAT signaling pathway [47–49].
In this work, the rise of IL-10 levels correlated with the protection found in dantrolene group, although its shortage was not necessarily a sign of damage as was seen in sham group. We found that ryanodine receptor antagonist dantrolene significantly up-regulated the expression of IL-10, offering the functional and structural protection on ischemic reperfusion muscle.
The potential clinical scope that ryanodine receptor antagnism could apply includes cardio-cerebrovascular diseases, such as myocardial ischemia, stroke, and may extend to hepatic and renal ischemia reperfusion.
Conclusions
In this study, we demonstrated for the first time the effects of ryanodine receptor antagonism on the skeletal muscle ischemia reperfusion injury. The ryanodine receptor and intracellular calcium antagonist dantrolene can effectively alleviate the inflammatory injury of skeletal muscle ischemia reperfusion when given at the beginning of reperfusion. The underlying molecular mechanism is probably related to the suppression of TNF-α levels and the increment of IL-10 expression.
Conflict of interest
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.