
Abstract
Keywords
Introduction
Liver transplantation has been established as a curative therapy option for acute and end-stage liver disease. Postoperative perfusion of the liver and vascular complications in the postoperative period are one of the main complications associated with an increased mortality [1]. Furthermore vascular complications can occur in patients with transplant rejection and rejection probably is pathophysiologically linked with hepatic artery thrombosis and other vascular pathologies in at least some cases [1–3]. Prognosis and overall outcome heavily relies on allograft function, therefore monitoring of patients after liver transplantation with imaging techniques and biomarkers is important for follow-up [4–6]. Contrast-enhanced ultrasound (CEUS) is an imaging technique that relies on a contrast agent that purely acts as an intravascular blood pool marker and dynamically shows the microcirculation of vascularized tissue [7–9]. For the assessment of liver allograft pathology needle biopsy is considered as the desirable method for the diagnosis of liver rejection [10]. CEUS could be a useful non-invasive imaging alternative as it can visualize vascular complications with transplant rejection in the postoperative period [11–13]. This study retrospectively analysed CEUS findings in patients after liver transplantation and postoperatively developed vascular complications with transplant rejection and correlated this findings to histopathological results. To our knowledge, no other study has described this correlation so far in a clinical setting, as only little data in an animal model exists [14].
Materials and methods
This study was approved by the local ethics committee. All study data were collected in compliance with the principles of the Helsinki/Edinburgh Declaration of 2002. The authors followed the ethical guidelines for publication in Clinical Hemorheology and Microcirculation [15]. Oral and written informed consent of all patients was obtained prior to each CEUS examination.
We retrieved and retrospectively analysed the CEUS examination from patients after liver transplantation from our database with initial imaging series between January 2006 and December 2015. All of these patients had additional liver biopsies with diagnostic pathological material. We additionally retrieved the results from these biopsies from the patient record file. Original dates of liver transplantation of these patients ranged from January 1993 to November 2015 and mean age at the time of the transplantation of these patients was 47.49 years (Min: 18; Max: 72; SD±13.78 years). Mean age at examination was 49.56 years (Min: 18; Max: 72; SD±13.05 years). Time between CEUS and histopathological result ranged from –36 to 46 weeks with a mean time of 0.96 weeks (SD±13.06 weeks). 28 out of 45 patients were male (62.2%). The initial reason for liver transplantation was alcoholic abuse disorder in 21 patients (46.7%) hepatitis in 13 patients (28.9%) and auto-immune disorders with hepatic complications in 11 patients (24.4%).
All examinatons were carried out on high-end ultrasound machines with adapted scanning protocols available between 2006 and 2015 and included systems from two different vendors and three different machines in total (Siemens Acuson Sequoia and Siemens S2000 with C4-1 and C6-1 HD probes, EPIQ 7, Philips Ultrasound) with C9-2 probe). A single DEGUM Level 3 examiner evaluated all sonograms during clinical routine.
SonoVue® (Bracco, Milan, Italy) was given in all examinations as an ultrasound contrast agent and was injected through a peripheral venous needle as a bolus with a flush of up to 10 ml of 0.9% NaCl. Average contrast agent doses varied dependant on the patient from 1.4 to 2.0 ml (min. 1.0 ml; max 4.8 ml) with repetitive doses given to some patients to acquire further digital cine loops for further diagnostic insights.
Results
CEUS and histological liver biopsy could successfully performed in all patients and no major side effects or adverse events occurred during these procedures. All images acquired using CEUS turned out to be in diagnostic quality and all histological material was satisfactory for histopathological testing. No patient withdrew consent after being examined or after biopsy so no patient hat to be excluded. Resonating to the literature that describes a low incidence of adverse events after the injection of SonoVue® no serious adverse event occurred during scanning.
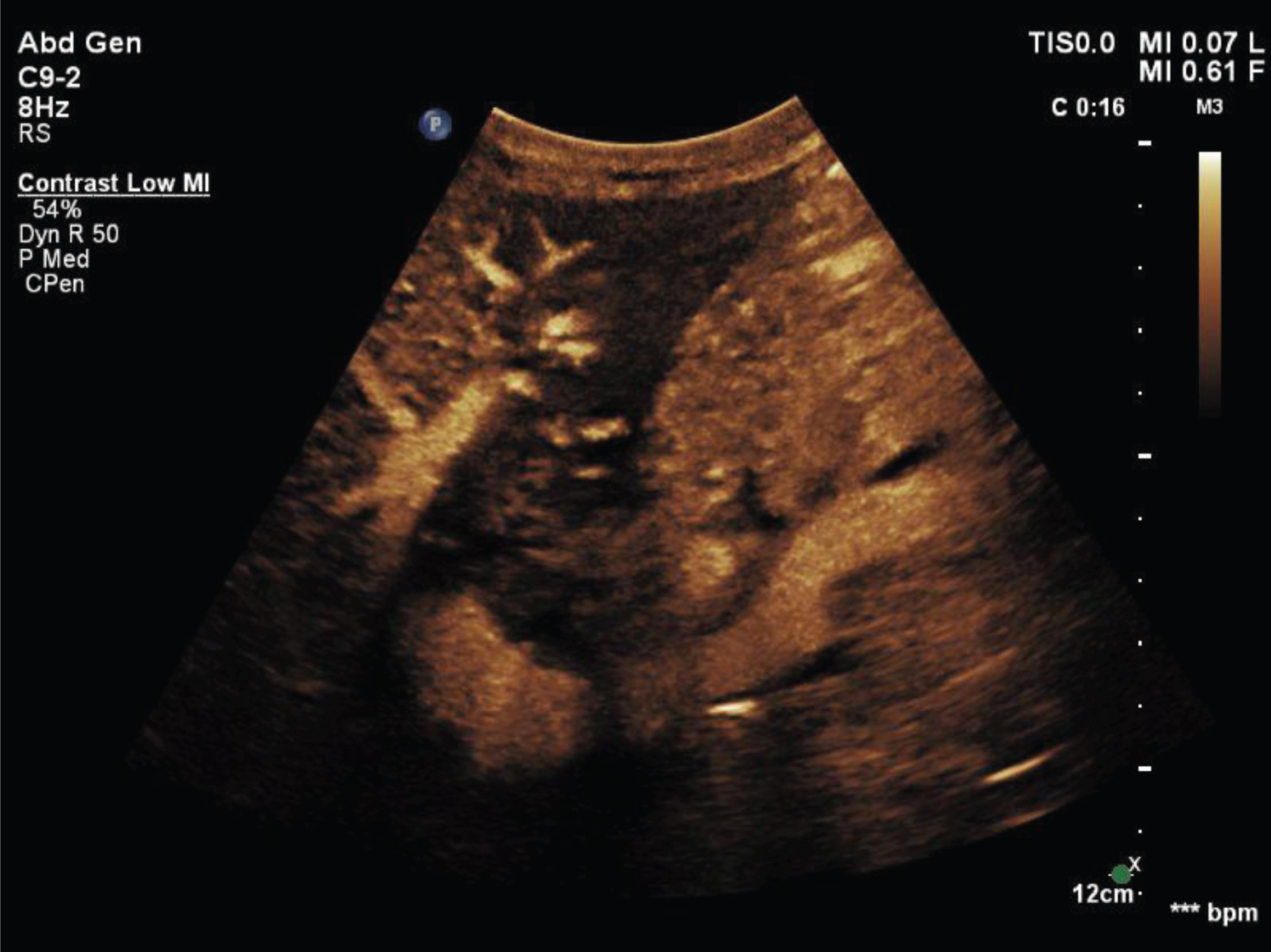
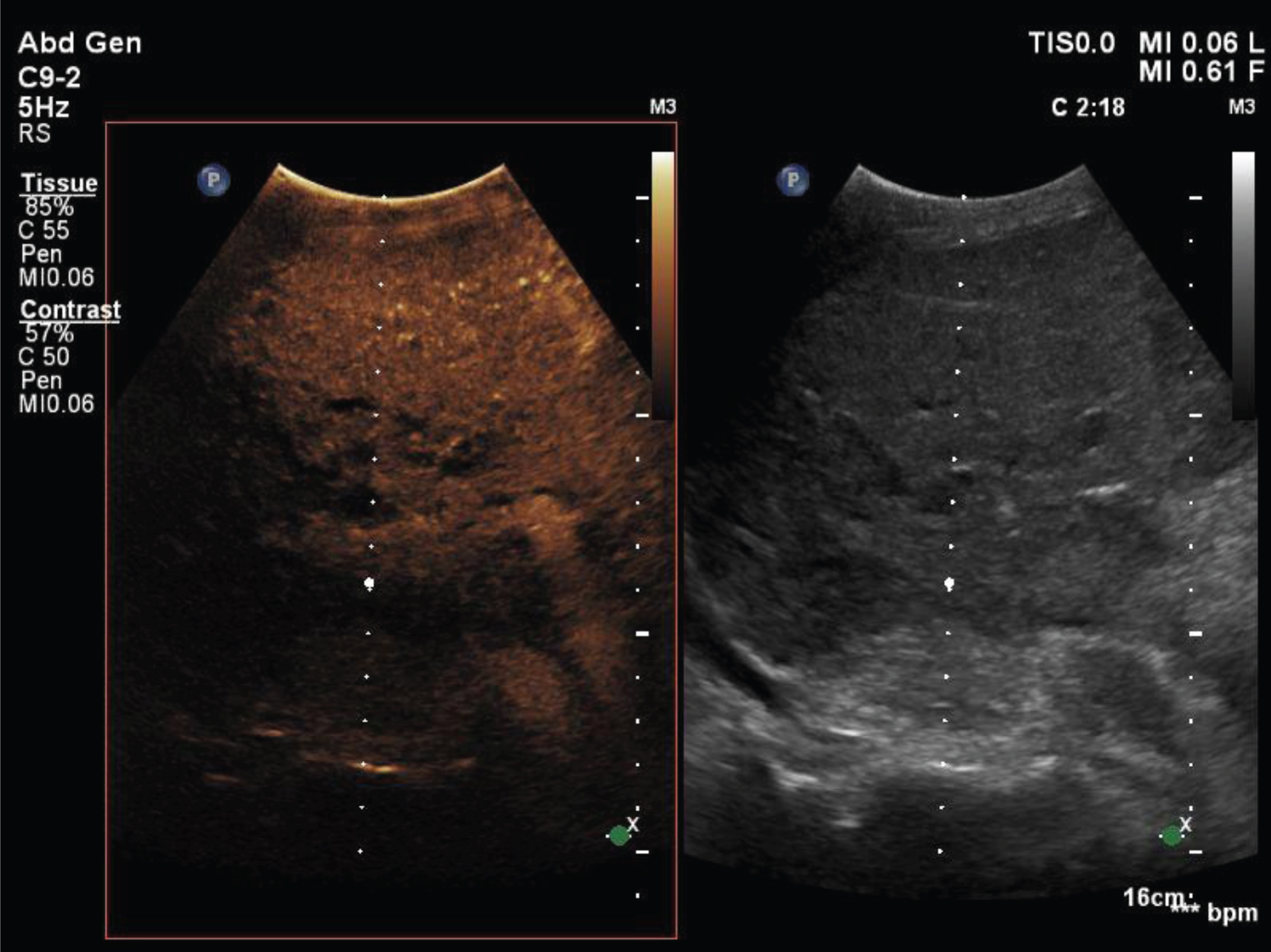
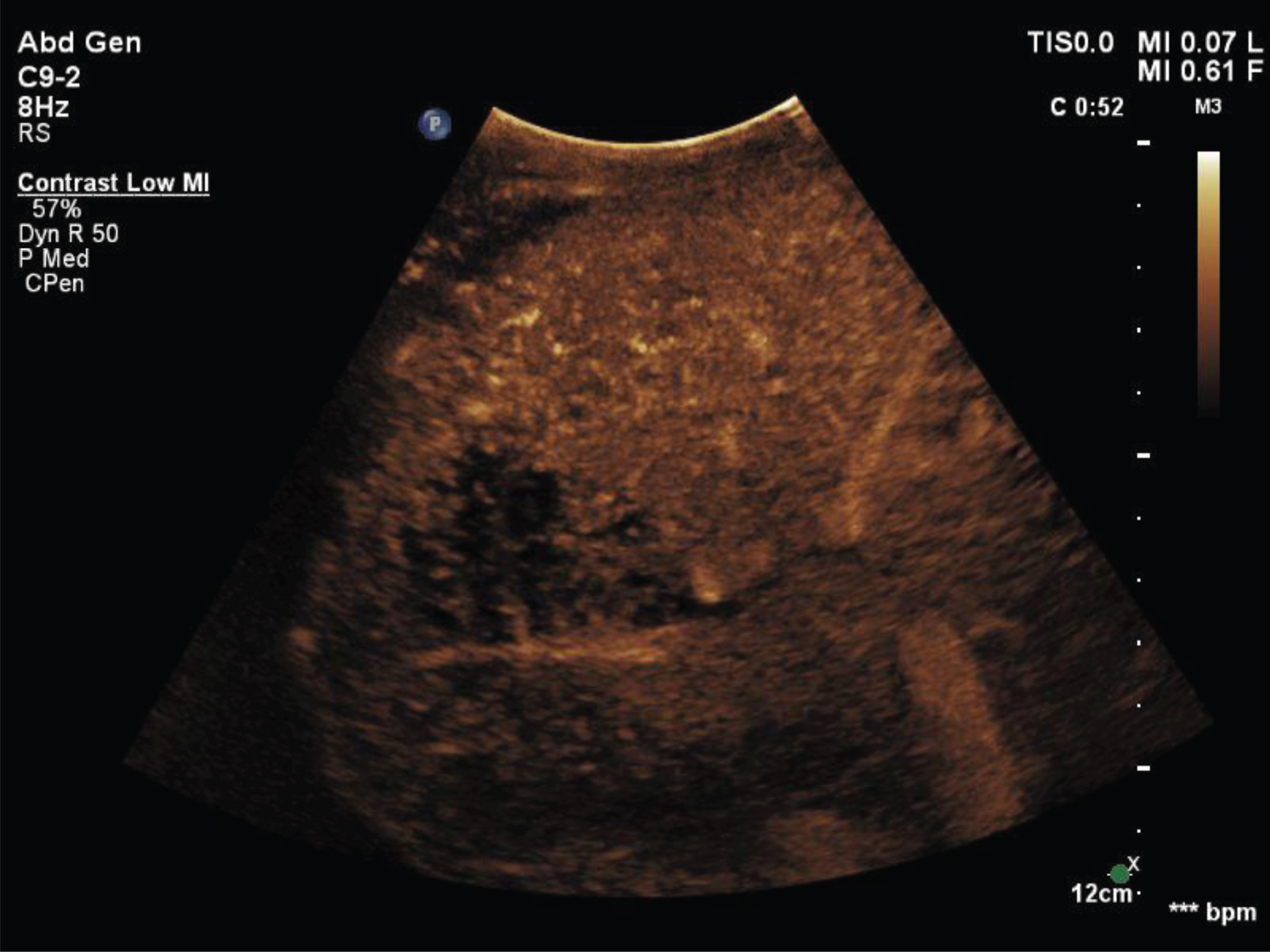
CEUS showed a sensitivity of 61.5%, a specificity of 100.0%, a positive predictive value (PPV) of 100.0% and a negative predictive value (NPV) of 86,5% in the detection of vascular complications with post-transplant rejection compared to the histopathological result that was considered as the gold-standard in this study (Figs. 1–5).
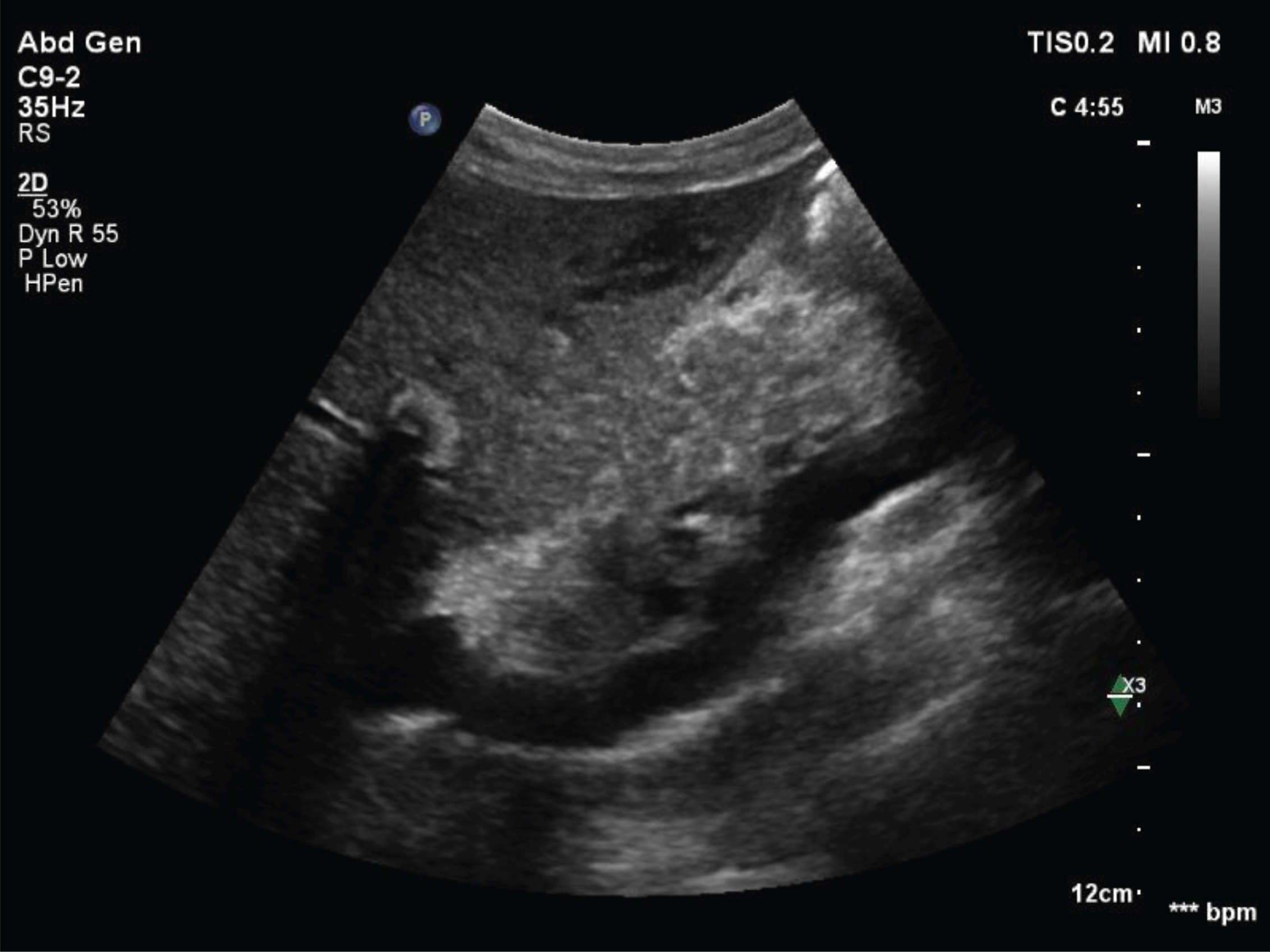
Unclear hypoechoic areal inside the parenchyma of the left liver lobe in a patient after liver transplantation.
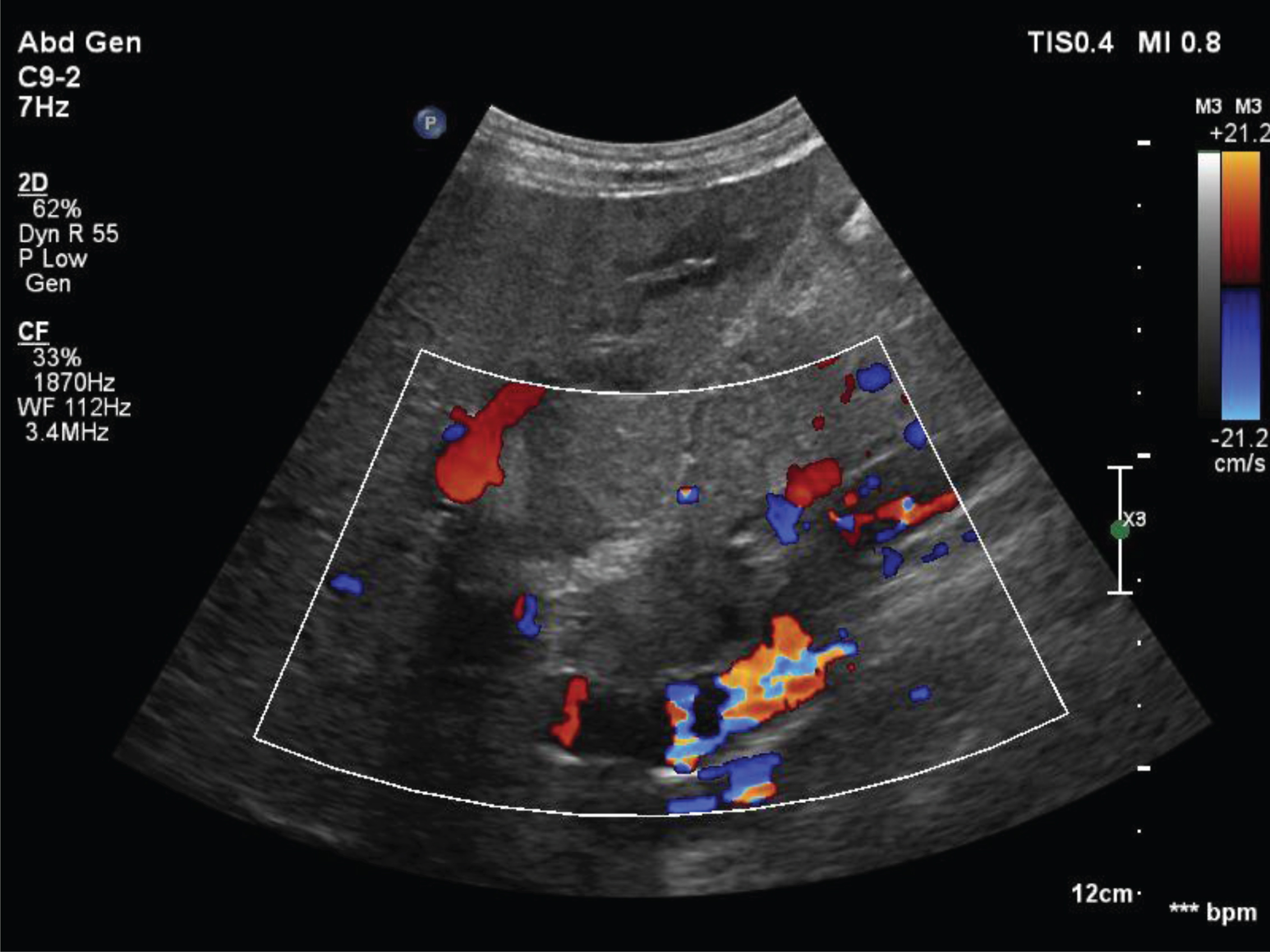
Same patient as in Fig. 1. Color Doppler shows no major visible vascular pathology.
Out of the 45 patients described above 13 patients showed a vascular complication with histopathologically confirmed transplant rejection (28.9%) whereas 32 patients did not (71.1%). In 8 out of 13 cases CEUS confirmed these findings, whereas in 5 cases the CEUS examination was read as normal (false-positive). No examination was read as false-negative.
Little to no data exists about the correlation between monitoring microvascularisation of vascular complications in patients after liver transplantation and histopathological results [16]. Monitoring transplant rejection in the postoperative period is important as rejection can occur at any given time point after transplantation [17]. This study suggests that with CEUS and its ultrasound contrast agent a marker for microvascularisation exists that can non-invasively measure vascular complications with transplant rejection with a high positive predictive value and a high specificity as well as with a good negative predictive value.
Patients with acute or chronic renal failure, abnormal function of the thyroid gland or known allergies to CT or/and MRI contrast agents can benefit from this method as CEUS is a practical alternative technique for the assessment of vascular problems after liver transplantation. CEUS is a real-time imaging modality that can be repetitively performed as a bed-side examination [18]. As a non-invasive technique this method can be used preinterventionally for the screening and follow-up of patients after liver transplantation as it might ease diagnosis and add diagnostic confidence to the clinicians.
The retrospective analysis character of this study was unfortunately a limiting factor and must be taken into consideration when discussing the results. Also this study was designed as a mono-center study only and all readings of the sonograms were done by only one radiologist possibly biasing the results. Future studies in this field should be conducted using a prospective multi-center approach to generate more valid data.
Conclusion
CEUS might be a useful additional non-invasive technique for the assessment of vascular complications with post-transplant rejection in patients after liver transplantation.