
Abstract
BACKGROUND:
Breast Carcinoma is the most common malign tumor disease in women. 20–30% of these tumors have to be treated by removing all of the breast tissue. After that kind of therapeutic procedure, most of the women are severely traumatized and ask for reconstruction. The goldstandard of breast reconstruction is the free perforator flap from the lower abdomen (DIEAP-flap), which can provide body-own tissue and natural shape for the reconstructed breast.
Many studies evaluate the shape of the reconstructed breast but neglect the skin sensitivity. Claim of this study was to compare this important part of reconstruction on two different techniques of mastectomy.
OBJECTIVE:
In this retrospective study we evaluated which technique of mastectomy and breast reconstruction with DIEAP-Flap offers the highest outcome for sensibility of the reconstructed breast. Skin sparing mastectomy was compared with conventional mastectomy and the results of skin sensitivity were measured.
METHODS:
Ten patients underwent breast reconstruction with free abdominal perforator flap between 2011 and 2015 after conventional mastectomy (CM) and were compared with ten patients, who had a skin sparing mastectomy (SSM) with immediate reconstruction by DIEAP-flap during the same time interval. These two groups were matched by age, height, weight and the time between reconstruction and examination. The sensitivity of the skin was measured by Semmes-Weinstein-Filaments in the strength beginning from 0,07 g till 300 g for deep sensation. The logarithmic profile of these measurements had been transferred into a continuous data system beginning from 1 point, which stands for no sensation, till 7 points for pressure threshold of 0,07 g.
RESULTS:
Patients who underwent DIEAP-reconstruction after skin sparing mastectomy showed a higher sensation at all regions of the new breast in comparison to reconstruction after conventional mastectomy, beginning from the nipple to the areola and the breast skin. The results in the CM-group were 1.0 points at the mamilla, 1.33 pts. at the areola and 1.78 pts. at the breast skin. In the SSM-group, the findings were 3 pts. at the mamilla, 3.25 pts. at the areola and 5.25 pts. at the breast skin.
CONCLUSION:
The skin sparing mastectomy combined with immediate reconstruction by DIEAP-flap provides an excellent therapeutic option for patients, who are suitable for this technique, which takes into account not only the form but also the sensitivity of the breast.
Introduction
Breast cancer is the most common malignancy in women [1–3]. Although today the majority of malignant breast diseases can be treated with breast conserving procedure, an average of 20–30% of the affected women still have to undergo a mastectomy. The mutilating aspect of this therapeutic measure is perceived as severely traumatising by the majority of the affected patients and often leads to psychological malfunctions [4].
For this reason the reconstruction of the female breast is an essential part of the therapeutic procedure [5] and is recognized as a standard repertoire of many plastic surgeons.
The autologous reconstruction with the microvascularly anastomosed, free abdominal perforator flap (DIEAP-flap) is defining the gold standard in reconstructive breast surgery [6].
While many studies have dealt with outcome [7, 8], form [9], and patient’s satisfaction [10–12] after autologous breast reconstruction, the sensitivity of the reconstructed breast, which is an important part of patients expectation, is rarely the subject of clinical examination.
Especially in cases of secondary reconstruction after mastectomy, a large skin island has usually to be inserted to form the breast. Since the reneurotization by nerve anastomosis often does not lead to the desired result due to the segmental innervation of the abdominal skin, the transplanted skin island has usually poor sensation [13, 14].
A clearly better situation results in the immediate reconstruction with the greatest possible preservation of the body’s skin coat. In the course of the skin sparing mastectomy, only the nipple-areola-complex is removed together with the gland and replaced by the free abdomen flap [15].
The aim of this study was to demonstrate the significantly better sensitivity of the breast skin after skin-sparing mastectomy and immediate DIEAP reconstruction compared to conventional mastectomy and DIEAP reconstruction with a large skin island.
Patients and methods
In this retrospective study, 10 patients after breast cancer were examined who had to undergo a conventional mastectomy (CM) followed by reconstruction with free abdominal perforator flap between 2011 and 2015 and were compared with ten patients who had a skin sparing mastectomy (SSM) [16] with immediate reconstruction by DIEAP-flap during the same period [17]. These two groups were matched according to the following criteria: age, height, weight and time interval between reconstruction and examination. The study was performed in accordance with the ethical guidelines of Clinical Hemorheology and Microcirculation [18].
In average 688 days after the reconstructive procedure (SSM group 692 days, CM group: 684 days), the women of each group were investigated. Biometric data were collected from each breasts, and skin sensation was measured. Standardized Semmes-Weinstein filaments [19] (Monofilament RFM, Rehaforum Medical, Germany) with the following contact pressure strengths were used as measuring instruments: 0.07 g, 0.4 g, 2 g, 4 g, 10 g; 300 g (deep sensation). The patients were examined in a tempered, quiet examination room in supine position; they were asked to keep their eyes closed. All tests were conducted by the same investigator to avoid errors due to different application of the filaments.
The following nine measuring points were tested in a fixed sequence: (reconstructed) nipple; areola at 3 h, 6 h, 9 h and 12 h, breast skin (halfway between nipple and breast border) at 3 h, 6 h, 9 h and 12 h. Beginning with the thinnest monofilament, it was pressed twice at each point until the filament was bent for at least 2 seconds; the lowest pressure, which was certainly perceived by the patient, was documented.
Results
The mean age of the patients at the time of the reconstruction was 51 years (range, 40–58a) in the SSM group and 49 years (range, 40–58a) in the group with conventional mastectomy. The average size of the women was measured with 168 cm (SSM, range, 160 cm–175 cm) and 165 cm (CM, range, 156 cm–176 cm). The body weight measured during examination was 76 and 71 kg, respectively.
In patients with SSM, four were operated on the left and six on the right breast (see Fig. 1; they were examined in average 692 days after the reconstruction.
Side of reconstruction for both patient groups “right side” and “left side”.
In the CM group, six women were affected at the left side and four at the right side; here, the follow-up interval was 684 days in average.
While on no patient of the CM group sensation could be measured on the reconstructed nipple, four out of ten patients of the SSM group registrated sensitivity on pressure with 2 g, 4 g or 10 g. On the areolar skin, only one individual of the CM group felt pressure of 10 g or less, while eight out of ten women in the SSM group registrated skin sensitivity in at least one part of the areola. Only one patient of the CM group was able to register sensation at the breast skin, whereas in all women of the SSM group this was detected at least in several areas.
Because the logarithmic profile of these measurements were not practicable for parametric data, they had to be transformed into a continuous data system. Therefore, the sensitivity outcome was transformed as follows: positive tests with the 0.07 g-filament were defined as value 7, tests with the 0.4 g-filament were defined as value 6 and following (see Table 1).
Transformation from logarithmic to continuous data system
Based on this algorithm, the results in the CM-group were 1.0 points at the mamilla, 1.33 pts. at the areola and 1.78 pts. at the breast skin. In the SSM-group, the findings were 3 pts. at the mamilla, 3.25 pts. at the areola and 5.25 pts. at the breast skin (see Table 2).
Sensitivity outcome for each patient of both groups
To compare the measurements with a standard, the contralateral breast was examined in the same way; the collected data were transformed to the same parametric system from 1 to 7 pts.
In the CM-group, the findings of the contralateral breast were 4,7 pts. for the mamilla, 4,58 for the areola and 5,48 for the breast skin. In the SSM-group, we measured on the contralateral breast 5,3 at the mamilla, 5,25 at the areola and 5,75 at the breast skin (Fig. 2).
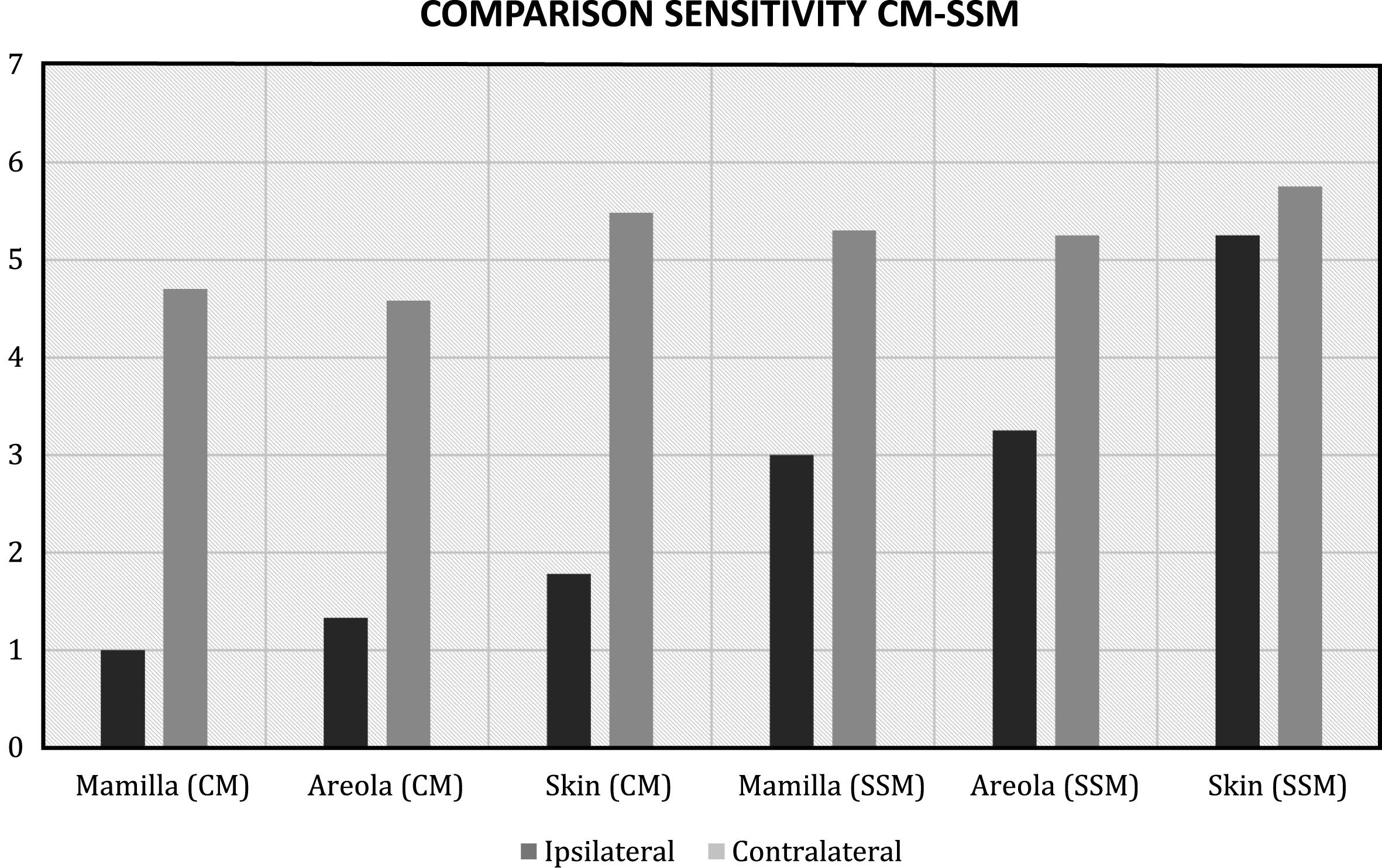
Comparison of the Sensitivity between conventional mastectomy and skin spared mastectomy.
To create a comparable standard for the non-operated breast following the identical measurement conditions, the median of both groups was calculated as follows: 5.0 pts. for the mamilla, 4,9 pts. for the areola and 5,6 pts. for the breast skin.
Patients' satisfaction between conventional mastectomy and skin sparing mastectomy is shown in Fig. 3.
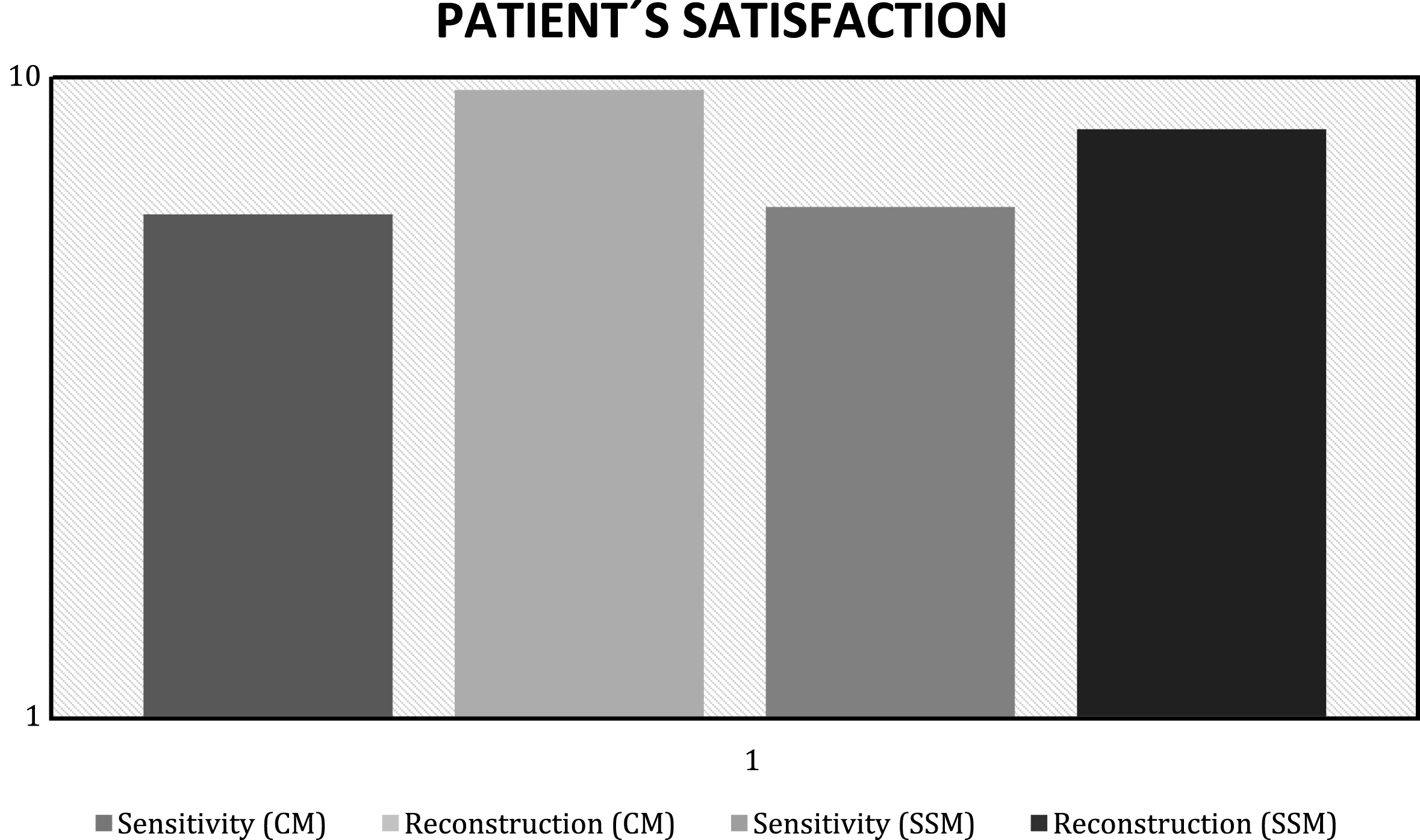
Comparison of patients satisfaction between conventional mastectomy and skin sparing mastectomy.
In this study the effect on skin sensation of two different techniques for mastectomy and breast reconstruction with DIEAP-flap were compared. The Semmes-Weinstein pressure treshold test was used to define objective parameters [20]. This test, which has been applied to each breast at 9 defined measuring points, has proven itself in many studies to measure the sensitivity on the breast skin, it is reproducible and quantitatively with controlled pressure stimulus [21, 25–27]. The Semmes-Weinstein-test is the most frequently published test for evaluating sensitivity on the skin [22, 23].
While conventional mastectomy always requires the replacement of a large skin area with the primarily insensitive flap tissue, skin sparing mastectomy with immediate reconstruction can provide the majority of the original skin envelope [24]. This not only provides an aesthetic advantage in shaping the new breast with preservation of the original décolleté, but also leads to significantly improved sensitivity compared to conventional mastectomy.
This aspect, which has so far been neglected in many studies about breast reconstruction with autologous tissue, has been investigated in our study on the basis of objective criteria.
For this purpose, two groups of 10 patients each following conservative mastectomy and reconstruction with DIEAP-flap (CM) as well as following skin sparing mastectomy and immediate reconstruction with DIEAP-flap (SSM), which were matched by age, size, weight and time interval since reconstruction, were compared.
Patient demographics showed a high coincidence within the given matching criteria. The average age was 49,6 a (48,6 vs. 50,7 a, Table 1), the mean BMI was 26,7 (26,5 vs. 26,9) and the most important criteria, the time interval since the reconstructive procedure, was 688 days in average (684 days vs. 692 days).
While none of the investigated patients in the CM group achieved sensitivity over the reconstructed nipple, 5 of the 10 women in the SSM group reacted with pressure values between 2 and 10 g. In the region of the reconstructed areola, 9 of the 10 examined women after CM were insensitive, whereas in the SSM group 9 of the 10 examined patients declared sensation at least in one of the four tested zones. The biggest difference between the two groups was seen in the area of the breast skin: while in the CM group 9 out of 10 patients had no sensitivity, the SSM group registered pressure thresholds of 4 g or less in all patients.
To give objective and comparable criteria, the measurements during examination with the logarithmic Semmes-Weinstein filaments were transformed into continuous data. On this basis, the sensoric outcome of the two groups can be set against each other and can be compared with the findings of the contralateral breasts, which function as a standard.
In this way, it could be shown that the conventional DIEAP flap for breast reconstruction was mostly insensate, while the SSM reconstruction showed skin sensitivity that came close to the non-operated breast of the contralateral side.
Conclusion
The skin sparing mastectomy combined with immediate reconstruction by DIEAP-flap provides an excellent therapeutic option for patients who are suitable for this technique, which takes into account not only the form but also the sensitivity of the breast.
Disclosure and funding sources
There were no sources of support in the form of grants, equipment, drugs or of other nature. No conflicts of interest.