
Abstract
BACKGROUND:
Previous studies on the recombinant form of human relaxin-2 (serelaxin) have shown a decrease of pulmonary hemodynamics after serelaxin injection. Currently, the effect of serelaxin treatment during hypovolemia in a large animal model remains mostly unknown.
METHODS:
12 sheep were randomly assigned to a sham or serelaxin (30μg/kg serelaxin) group and underwent right heart catheterization. 50% of the estimated total blood volume were removed to induce hypovolemia, and subsequently retransfused 20 min later (reinfusion). Blood gases, heart rate, peripheral and pulmonary arterial oxygen saturation, systolic, diastolic and mean values of both pulmonary artery pressure (PAP) and pulmonary capillary wedge pressure (PCW) were measured. Cardiac output (CO), pulmonary vascular resistance (PVR), pulmonary arterial compliance (PAcompl) and systemic vascular resistance (SVR) were calculated.
RESULTS:
Hypovolemia and shock led to a similar decrease of PAP and PCW in both groups (p≤0.001). CO, SV and PAcompl decreased only in the control group (p≤0.05) and remained higher in the serelaxin-treated group. The results of this study suggest that serelaxin treatment did not negatively influence hemodynamic parameters during hypovolemic shock.
CONCLUSION:
The main conclusion of this study is that cardiopulmonary adaption mechanisms are not critically altered by serelaxin administration during severe hypovolemia and retransfusion.
Keywords
Abbreviations
heart rate
femoral arterial oxygen saturation
pulmonary arterial oxygen saturation
systolic pulmonary artery pressure
diastolic pulmonary artery pressure
mean pulmonary artery pressure
systolic pulmonary capillary wedge
diastolic pulmonary capillary wedge
mean pulmonary capillary wedge pressure
were measured, cardiac output
pulmonary vascular resistance
pulmonary arterial compliance
systemic vascular resistance
stroke volume
Introduction
Relaxin-2 is a human hormone that modulates the endothelial vasodilatatory function, particularly systemic and renal vasodilatation in humans [1]. These effects can be induced in non-pregnant animals and in non-pregnant humans via relaxin administration [2, 3]. The recombinant form of human relaxin-2 (serelaxin, Novartis Pharma AG, Basel, Switzerland) increases the cerebral blood flow (CBF), renal blood flow and arterial compliance, and furthermore improves pulmonary hemodynamics [4–6]. In patients below 45 years of age, severe hemorrhage constitutes the leading cause of death [7]. The potential catastrophic impact of such injuries is demonstrated by the fact that they are the reason for 11% of disability-adjusted life years in 2010 [8]. In such severe cases of hemorrhagic shock, the limits of the cerebral autoregulatory capacity are surpassed [9], with subsequent cerebral damages due to hypoperfusion [10]. Specific neuropotective strategies during hemorrhagic shock do not exist at this point, and while interventions are under investigation, the general state of research remains sparse [11]. However, a new method for visualising the microcirculation using Incident Dark Field technology to investigate the microcirculation during hemorrhagic shock exists now and could positively influence the diagnostic and informative value of future studies [12]. Since serelaxin improves the cerebral cortical microcirculation [13], future studies investigating neuroprotective properties of serelaxin during hypovolemia are conceivable – albeit only if serelaxin were found to be safely applicable under hypovolemic conditions. Until now, the specific effects of serelaxin during hypovolemia, shock and retransfusion have not been investigated. However, a deterioration of hemodynamic parameters at least seems conceivable, since the endothelial modulation leads to a distinct vasodilatation. Comprehending the influence serelaxin poses on hemodynamic parameters in a hypovolemic setting is quite important though; both for its potential future applications as mentioned above, and furthermore since it has already been under investigation for the treatment of acute heart failure, a setting in which cardiopulmonary instability would constitute a serious contraindication. In these previous studies, however, patients with a systolic blood pressure below 125 mmHg and shock patients have been excluded [14, 15].
We utilized the large animal model sheep, with its similar cardiovascular physiology to humans, to investigate the effect of relaxin-2 on pulmonary hemodynamics during severe hypovolemia. We applied right heart catheterization, which is considered to be a safe invasive procedure and the gold standard for hemodynamic assessment [16, 17], to measure the necessary hemodynamic parameters.
Materials and methods
Animal care, surgical instrumentation, anaesthesia and experimental protocol
All experimental procedures were performed in compliance with the ARRIVE guidelines and with the approval of the Thuringia Animal Welfare Committee (Bad Langensalza; permission number: TVV 02-056/13 valid from 13 December 2013 until 20 December 2016). Twelve 2–6 year old female Merino long wool sheep, weighing 79.3±10.1 kg, underwent surgery in accordance to the Guide for the Care and Use of Laboratory Animals [18]. Our methods for the surgical instrumentation, the anaesthesia, data recording and blood gas measurements have previously been described in detail [13]. Anaesthesia was induced by intramuscular injection of 10–15 mg/kg ketamine (Ketamin-Hydrochlorid®, Pfizer, Berlin, Germany) and 0.2 mg/kg midazolam (Midazolam-Hameln®, Hameln Pharmaceuticals, Hameln, Germany) and was followed by orotracheal intubation. Anaesthesia was maintained via inhalation of 1.5% isoflurane (Isofluran–Actavis®, Actavis, Langenfeld, Germany) in 50% oxygen over the course of the entire experiment. The right heart data acquisition was continuously performed. The sheep were randomly assigned to experimental groups. Subsequent to the baseline recordings, 6 sheep (control group) received a bolus injection of 20 ml saline (Isotonische Kochsalzlösung®, Fresenius, Bad Homburg, Germany), and 6 sheep (serelaxin treated-group) received an injection of 30μg/kg serelaxin (0.1–0.15 ml stock solution) diluted in saline (serelaxin, Novartis Pharma AG, Basel, Switzerland).
Experimental protocol on hypovolemia
After baseline recordings, a controlled severe hemorrhage was induced in all sheep via removal of 50% of the estimated total blood volume, which approximates 7% of the total body weight in sheep [19]. The blood removal, performed at a constant rate, lasted 20 minutes. The hypovolemia (50% blood volume) was maintained for 20 minutes (=shock phase), thereafter, reinfusion of the removed blood was carried out at a constant rate over 20 minutes. Removed blood was kept in empty infusion bags (Isotonische Kochsalzlösung, freeflex®, Fresenius Kabi, Bad Homburg, Germany), with the addition of 1000 IE Heparin (Heparin-Natrium 5000, Ratiopharm, Ulm, Germany). Blood gases and lactate samples were taken before and at the end of blood removal. Arterial blood pressure and mean arterial blood pressure (MABP), electrocardiogram (ECG), body temperature and oxygen saturation (SO2art, SO2pul) were recorded continuously.
Pulmonary hemodynamics
The systolic, diastolic and mean pulmonary artery pressure (PAPs, PAPd, PAPm), as well as systolic, diastolic and mean pulmonary capillary wedge pressure (PCWs, PCWd, PCWm) were measured through right heart catheterization. Measurements were performed at baseline, 10 minutes after the bolus injection of NaCl or serelaxin, at 25% of hypovolemia, at deep hypovolemia (50% blood volume), at the end of the shock period (after 20 min established hypovolemia), at 25% of reinfusion, at 50% of reinfusion and 20 minutes after completed reinfusion. Blood gases and heart rate (HR) were recorded as previously described [20]. Cardiac output (CO) was calculated with Ficks method [21]. The pulmonary vascular resistance (PVR) was calculated as (PAPm – PCWPm)/CO [22]. The systemic vascular resistance (SVR) was calculated as MAP/CO. The stroke volume (SV) was calculated as CO/HR. The pulmonary artery compliance (PAcompl) was calculated by SV/(PAPs-PAPd) [22].
Statistical analysis
Descriptive statistics (means±standard deviation (SD)) were utilized to summarize the outcome parameters of the different measurements. The data are normally distributed. Linear mixed regression models were fitted to compare the trend of pulmonary hemodynamic parameters between both groups. This approach allows for the correlation of repeated measurements of an individual animal. Independent variables of the models are group (serelaxin/control) and time of measurement, as well as their interaction. A separate model was calculated for each condition (hypovolemia, no hypovolemia). Regression coefficients of the models were presented to describe the average change of pulmonary hemodynamic parameters per minute.
The significance level was set to p = 0.05. All statistical analyses were performed with SPSS 22.0 (IBM, New York, NY, USA).
Results
Blood parameters and vital parameters under serelaxin treatment during severe hypovolemia and reperfusion
Arterial blood gases and lactate were within their physiological range before the onset of the experiments (Table 1). Hemorrhage induced a decrease of pH and pO2, and an increase of pCO2 and lactate (P < 0.05, Table 1). pH and pCO2 reached normal levels during the reperfusion, whereas pO2 was restored to baseline level only after completion of the reperfusion. No differences were observed between the serelaxin-treated and the control group.
Blood parameters during hypovolemia
Blood parameters during hypovolemia
Blood samples were drawn from the arteria femoralis. Samples were taken at baseline (Basal), immediately during severe hypovolemia after 50% of blood loss, respectively (50% of blood loss), after reperfused of 50% of the total blood volume, respectively (end of reinfusion), or 20 min after reinfusion (total 70 min). All data are given as mean±SD. Abbreviations used: pCO2/pO2, partial pressure of carbon dioxide/oxygen; BE, base excess; Hct, hematocrit.
The MABP quickly decreased after initiation of hypovolemia, (P = 0.018) and was restored during reinfusion (Fig. 1A, P < 0.001). No differences could be observed between the groups. The initial serelaxin injection increased the HR slightly. Induction of hypovolemia resulted in an increase of HR in both groups (Fig. 1B, P < 0.05). Reinfusion restored HR to baseline level in the control group, but remained elevated in the serelaxin treated group (P < 0.03) as compared to the control group.
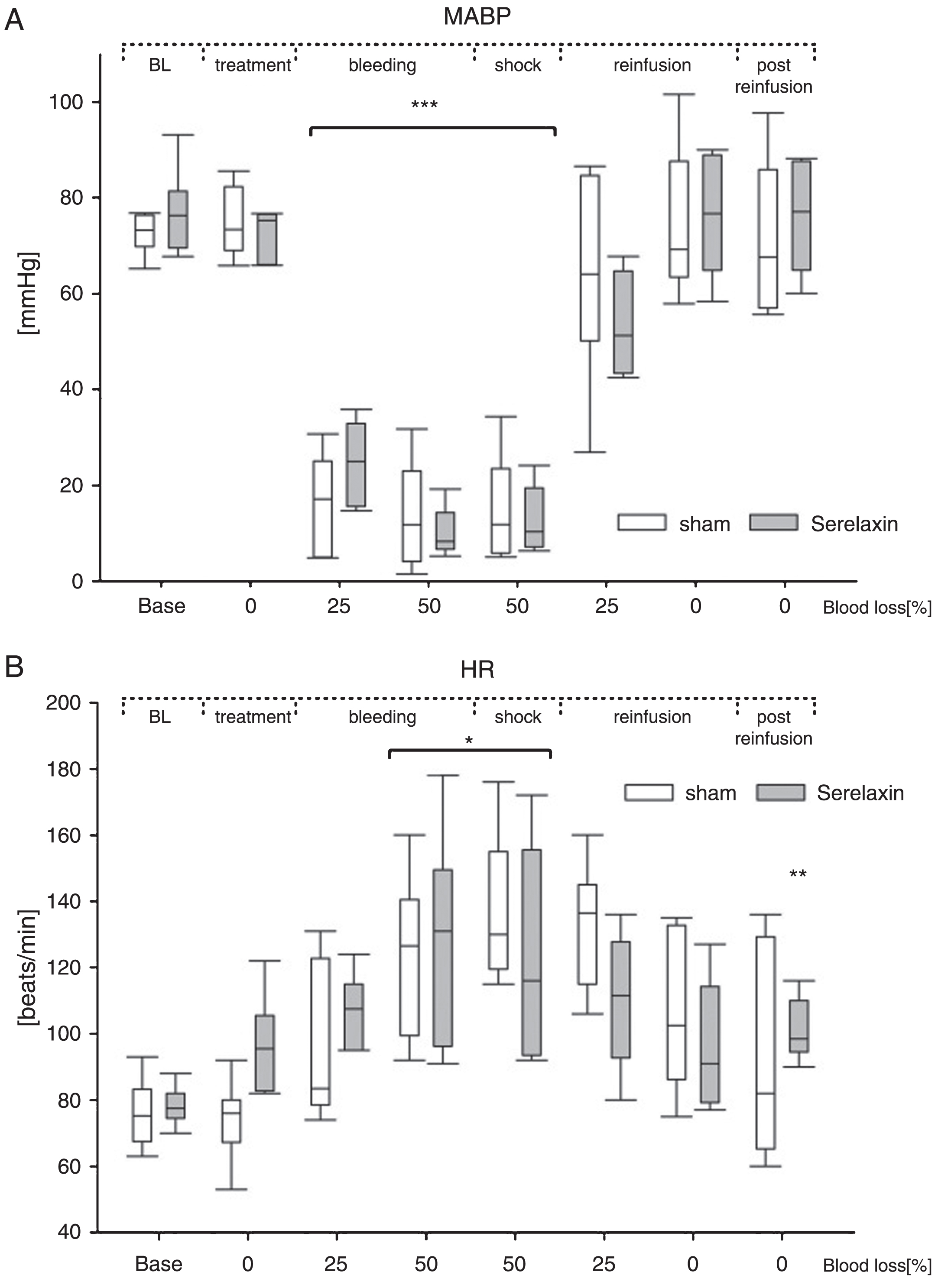
Effects of serelaxin during 50% blood loss, shock and reinfusion on mean arterial pressure and heart rate. Comparison on mean arterial pressure (MAP) (A) and heart rate (HR) (B). Data of the serelaxin treated (gray symbols) or control group (shame, white symbols). Means(±)SD, *P≤0.05, ***P≤0.001compared to baseline, **P≤0.03 for comparison between two experimental groups.
The femoral arterial oxygen saturation (SO2art) significantly decreased during hemorrhage and the shock phase in both groups (P < 0.05), but was restored to baseline levels during the course of the reinfusion in both the control and serelaxin-treated group (Fig. 2A). No significant changes regarding SOart could be observed between the groups. While the pulmonal arterial oxygen saturation (SO2pul) decreased in the control group as a result of the hypovolemia (Fig. 2B, P < 0.05), no significant effect was observed in the serelaxin-treated group. Reinfusion led to restoration of SO2pul values to baseline levels in both groups.
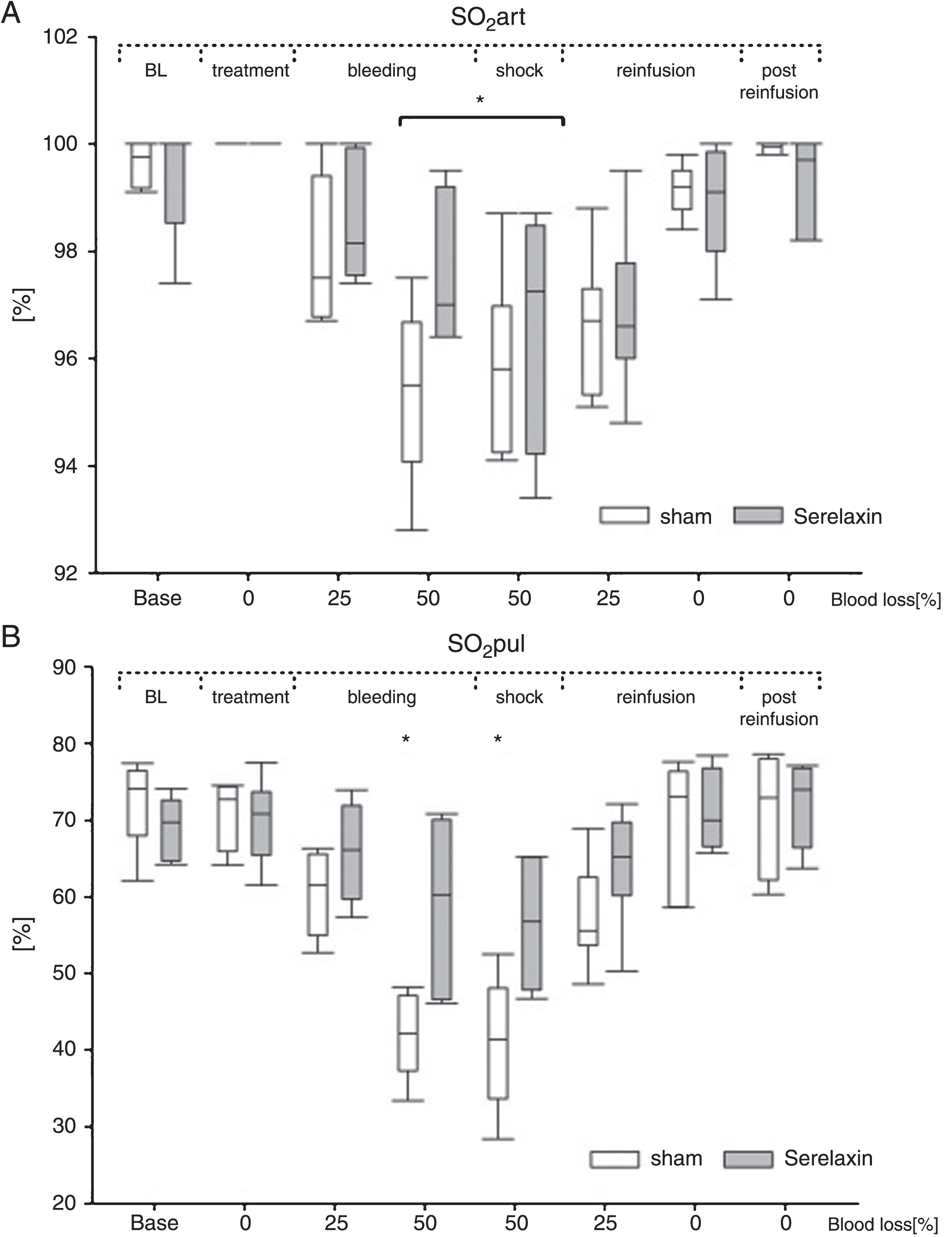
Effects of serelaxin during 50% blood loss, shock and reinfusion on arterial blood gases. Arterial oxygen saturation (SO2 art) (A) and pulmonary arterial oxygen saturation (SO2 pul) (B). Means(±)SD, *P≤0.05 compared to baseline in A) for each group and in B) for the control group.
Induction of hypovolemia resulted in a decrease of PAPm, PAPs and PAPd (Fig. 3A- C, P < 0.001), with no significant differences between both groups. Reinfusion restored PAPm, PAPs and PAPd to baseline levels (Fig. 3A- C). Analysis of the PCWP revealed a comparable situation. Hypovolemia resulted in a decrease of PCWPm, PCWPs and PCWPd in both groups (Fig. 4A-C, P < 0.001). After reinfusion the levels of PCWPm, PCWPs and PCWPd normalized to baseline levels in both groups (Fig. 4A-C). No significant differences between the control and serelaxin-treated group were detectable during the procedure.
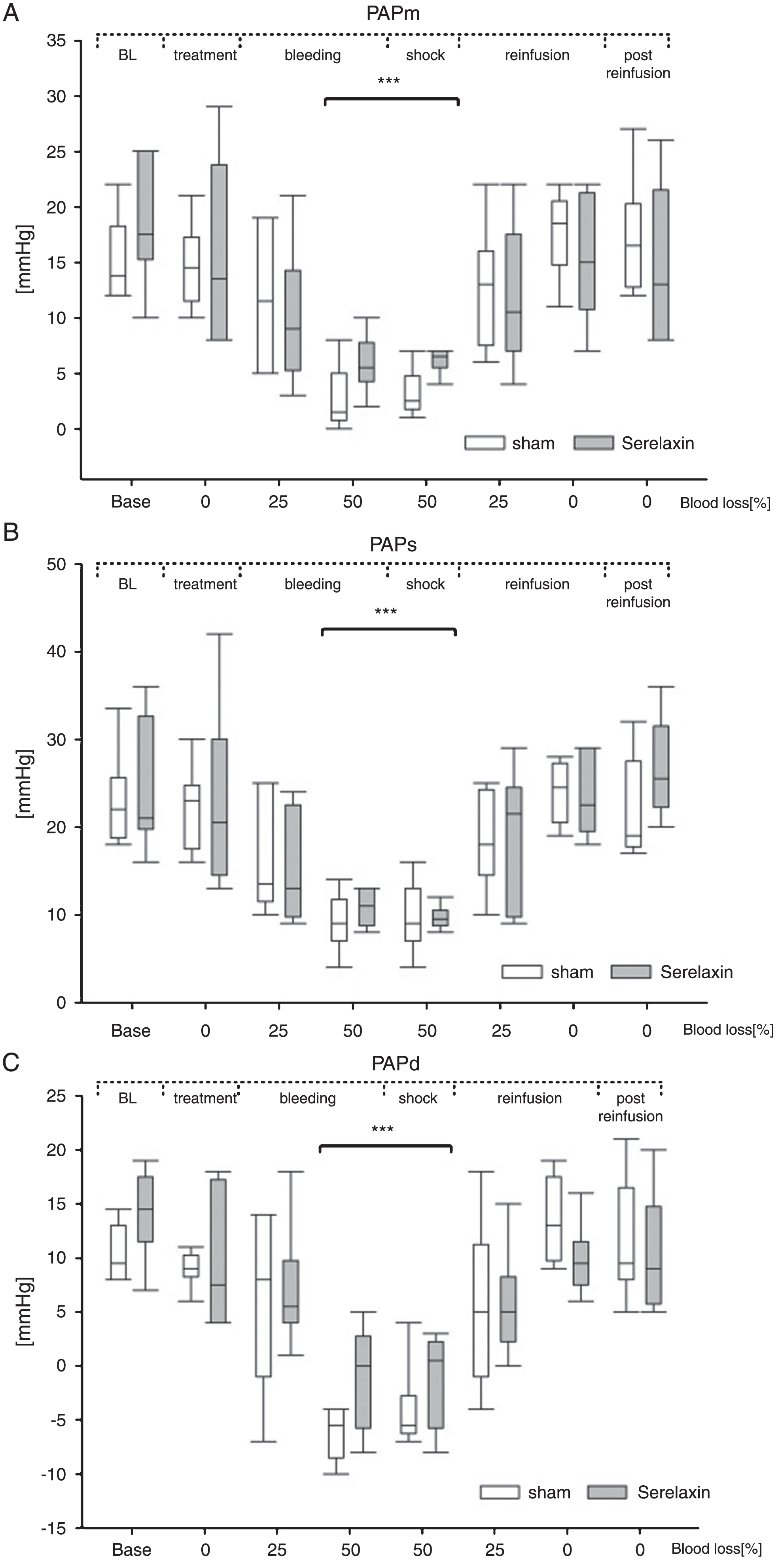
Effects of serelaxin during 50% blood loss, shock and reinfusion on pulmonary artery pressure. Mean pulmonary artery pressure (PAPm) (A), systolic pulmonary artery pressure (PAPs) (B), diastolic pulmonary artery pressure (PAPd) (C), serelaxin (gray symbols) or saline (white symbols). Means(±)SD, ***P≤0.001 compared to baseline for each group.
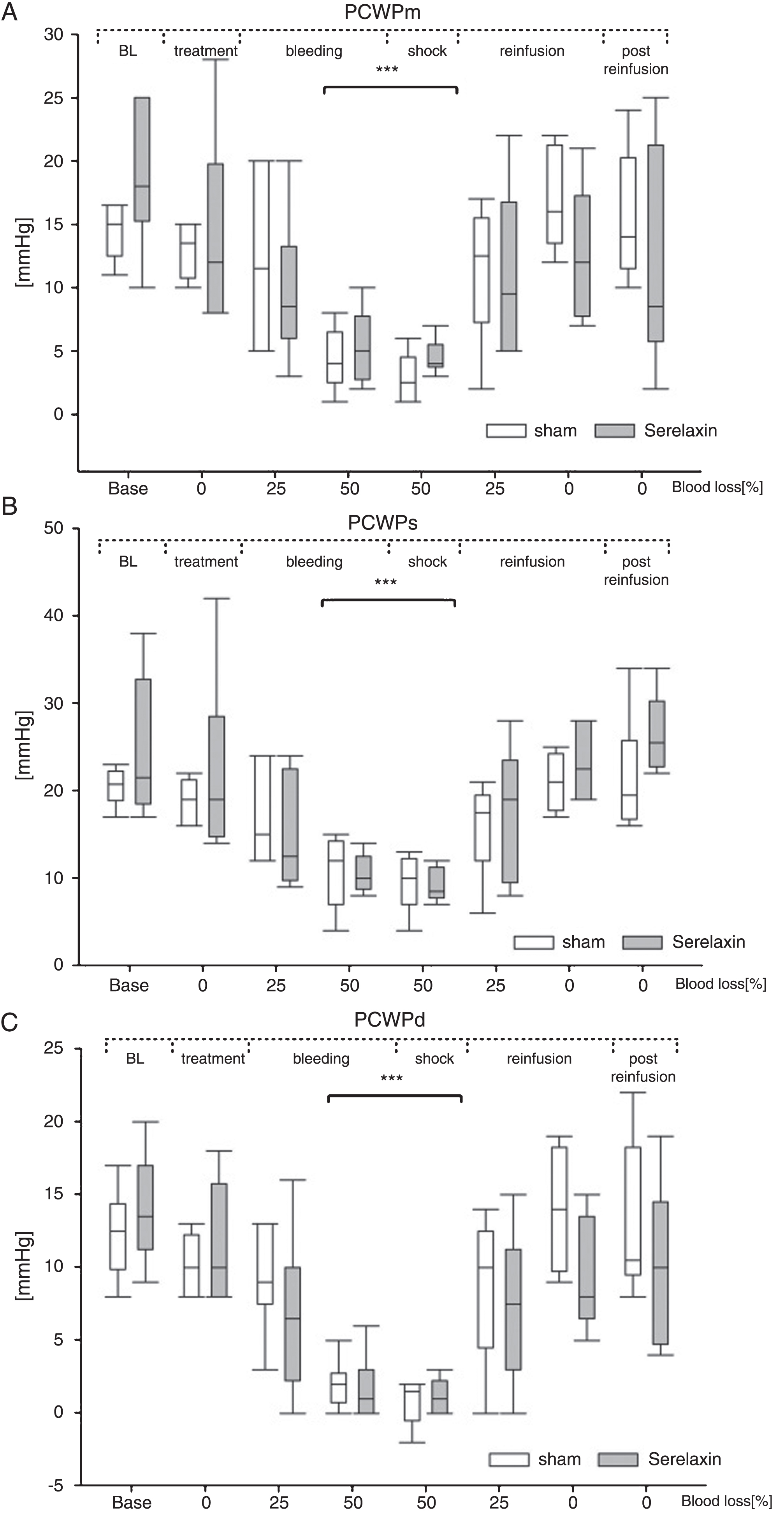
Effects of serelaxin during 50% blood loss, shock and reinfusion on pulmonary capillary wedge pressure. Mean pulmonary capillary wedge pressure (PCWPm) (A), systolic pulmonary capillary wedge pressure (PCWPs) (B) and diastolic pulmonary capillary wedge pressure (PCWPm) (C), serelaxin (gray symbols) or saline (white symbols). Means(±)SD, ***P≤0.001compared to baseline for each group.
CO and SV, as indicators of the heart’s efficiency in delivering blood to the body, were significantly decreased in the control group during hypovolemia (Fig. 5A-B, P < 0.05). The decrease of CO and SV was not significant in the serelaxin-treated group. CO and SV remained virtually higher in the serelaxin-treated group over the course of bleeding and shock phase. No ssignificant differences for the CO and the SV values between the control and serelaxin treated group were detectable over the observed time. We observed no significant differences in PVR over the course of hypovolemia and reinfusion in both experimental groups (Fig. 6A). TPR was slightly decreased under hypovolemia, but was restored to baseline levels after reinfusion (Fig. 6B). The PAcompl decreased significantly in the control group during hypovolemia (Fig. 7, P < 0.05). We observed no changes for PAcompl over the observed time between both groups. Furthermore, PAcompl remained virtually higher in the serelaxin treated group over the course of bleeding, shock phase and the beginning of reinfusion.
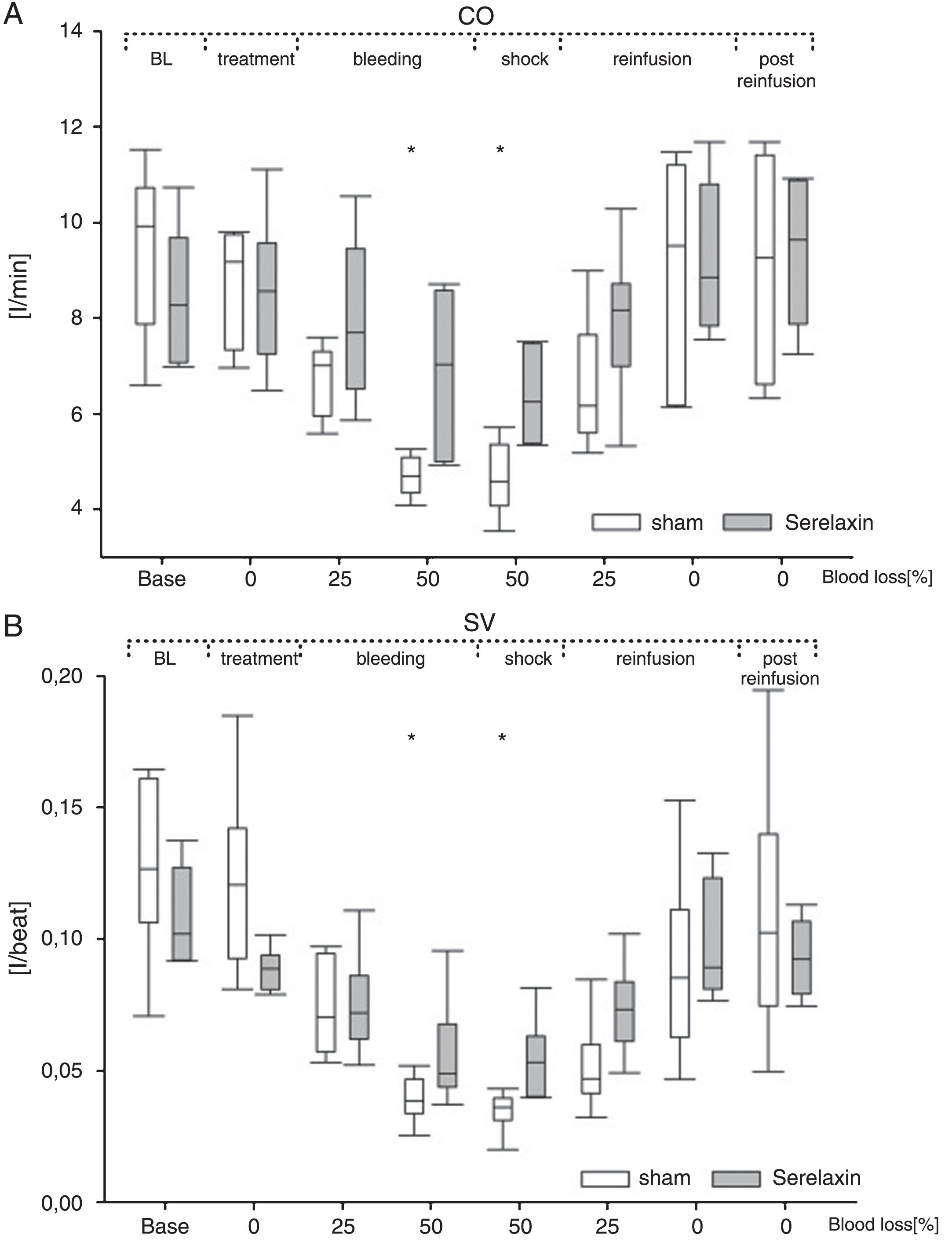
Effects of serelaxin during 50% blood loss, shock and reinfusion on cardiac output and stroke volume. Cardiac output (A) and stroke volume (B). Means(±)SD, *P≤0.05 compared to baseline for the control group.
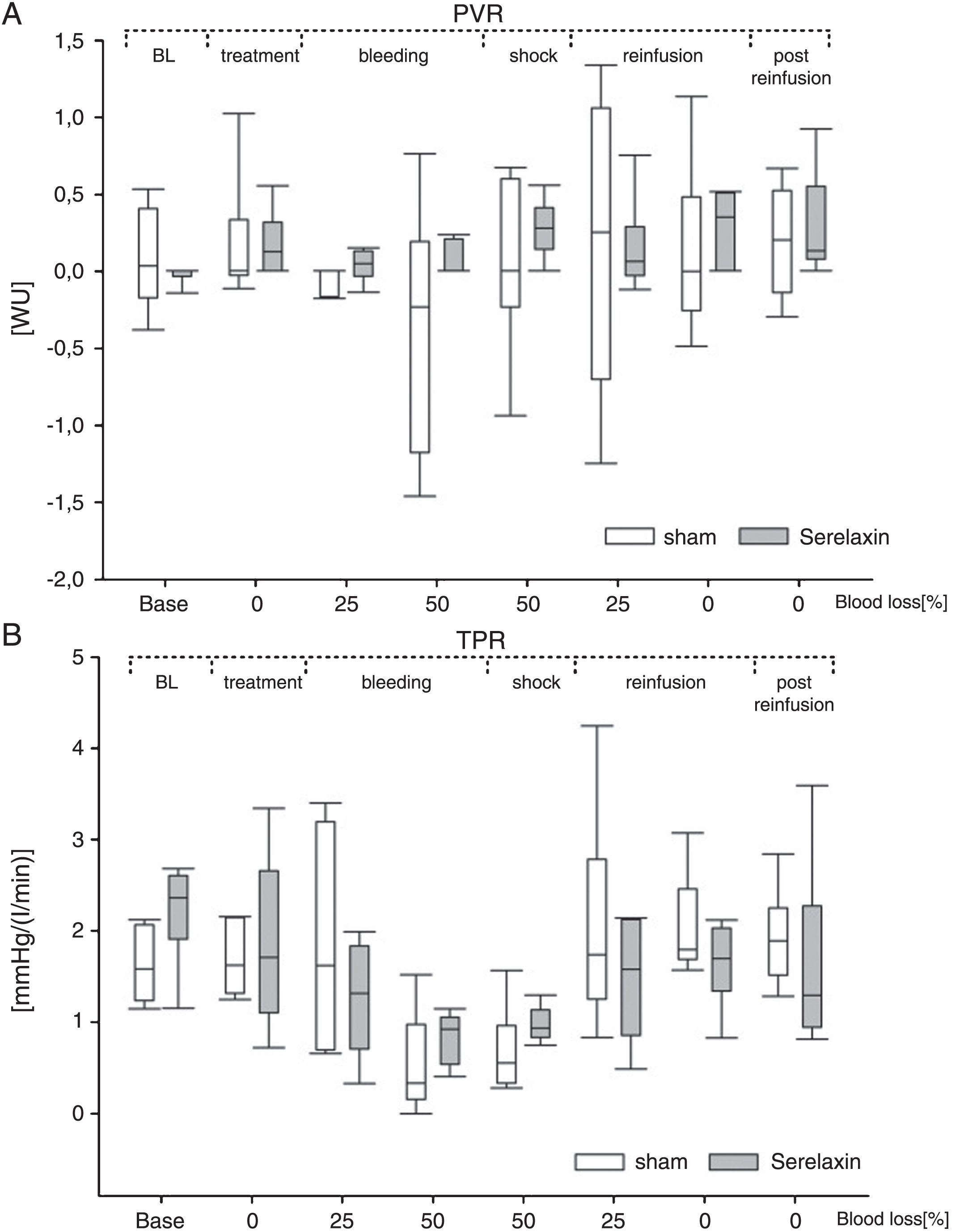
Effects of serelaxin during 50% blood loss, shock and reinfusion on pulmonary and systemic vascular resistance Pulmonary vascular resistance (PVR) (A) and systemic vascular resistance (SVR) (B). Means(±)SD.
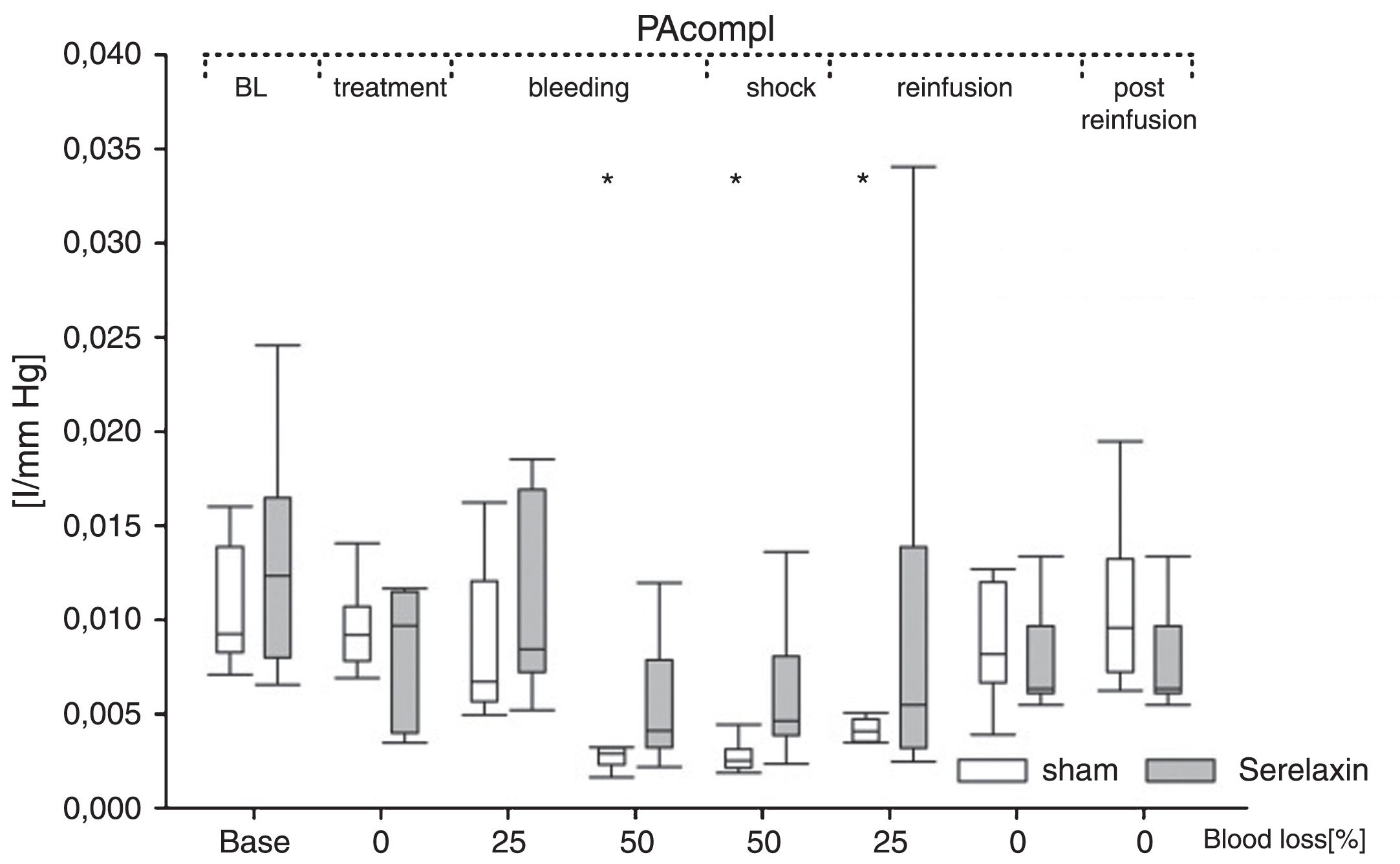
Effects of serelaxin during 50% blood loss, shock and reinfusion on pulmonary artery compliance Pulmonary artery compliance (PA compl), Means(±)SD, *P≤0.05 compared to baseline for the control group.
In this study, we investigated the influence serelaxin poses on the pulmonary hemodynamics during severe hypovolemia and reperfusion in a large animal model. The key finding revealed by our data is that relaxin-2(serelaxin) administration does not negatively influence pulmonary hemodynamics during the aforementioned conditions.
Our results indicate that serelaxin might potentially be used during hypovolemic conditions due to its positive hemodynamic effects, since it does not impair hemodynamic adaptation and does not lead to a significant decrease of the analyzed parameters. This is probably due to the small group size. This knowledge forms the basis for future investigations into relaxin-2’s potential neuroprotective properties in such scenarios. Acute blood loss cannot safely be derived from changes of the hematocrit, which is a general observation that should be considered in the assessment of a patient’s potential extent of bleeding [23]. Clinical parameters such as heart rate, blood pressure and changes of the blood gases, lactate and base excess have to be considered in a temporal context [24]. Alterations of the hematocrit level are dependent on time [25, 26]; while some studies have reported alterations of the hematocrit in the context of severe bleedings [27]. These changes do nonetheless not provide sufficient evidence for a bleeding since haematocrit changes depend significantly on the individual physical constitution [25]. While haematocrit changes can therefore not be used to safely diagnose severe bleedings, they might coincide with further acute events, such as myocardial infarction [28].
Induction of hypovolemia led to a decrease of both, arterial and pulmonary oxygen saturation, with a subsequent recovery after reinfusion. Although serelaxin treatment did not significantly affect the arterial and pulmonary oxygen saturation, our data furthermore suggest that serelaxin application may protect from a hypovolemic-dependent decline of the oxygen saturation. A positive effect of serelaxin on the pulmonary oxygen saturation under normal conditions in sheep has previously been verified by our research group [11]. Given a group size of 11–13 sheep in our previous work, and 6 sheep in this study, a significant improvement of the oxygen saturation under hypovolemic conditions could be expected in the context of a larger sample group.
In both experimental groups, we observed changes consistent with the condition of severe hypovolemia. Thus, the decreases in MABP, CO, SV, PCW, PAP and the compensatory increase in HR can be attributed to the situation under hypovolemia [29–33]. The subsequent increase in MABP, CO, SV, PCW, PAP and decrease in HR in the context of reperfusion is mentioned in various studies and corresponds with contemporary knowledge [29, 34]. Since we observed a slight improvement of cardiac output, stroke volume, and PAPd/m during hypovolemia after serelaxin injection, the data not only negate the initially presumed adverse effects as described in the introduction, but furthermore indicate that serelaxin application could promote a positive outcome under such conditions (although the measurements are not significant within our small sample size of 6 animals). Inhalation anesthesia with isoflurane did not adversely affect the hemodynamic adaptation processes under hypovolemia with subsequent reperfusion [19, 33].
In our study we wanted to investigate whether hemodynamic redistribution and its effects on the pulmonary hemodynamics are efficient within the context of a strong volume deficiency. In order to survive the reallocation of blood in the context of severe bleeding, a hemodynamically intact redistribution system is necessary [32, 35]. The use of a very potent vasodilator such as relaxin-2, with its very fast onset time, has a direct effect on pulmonary hemodynamics [20].
Relaxin-2 is a very potent arterial vasodilator with immediate effects on the circulation (within minutes) [20, 36], the subsequent increase of vascular compliance has already been described [20, 37]. An improvement of peripheral vasodilatation and atrial inotropy has similarly been described in earlier studies [2, 38], albeit this latter effect has not been measured in this study. Serelaxin’s positive influence on pulmonary hemodynamics has furthermore already been described in studies utilizing right heart catheterizations in humans and sheep [20, 39]. A positive improvement of the CO subsequent to serelaxin application has similarly already been described in experiments utilising rats and sheep [20, 38], and in acute heart failure patients with preserved left ventricular ejection fraction undergoing serelaxin treatment [39]. Nonetheless, our results indicate that serelaxin improves the pulmonary hemodynamics even during critical scenarios e.g. a severe hypovolemia or shock – conditions under which the hormone had until now not been investigated. Since no significant alterations of the global hemodynamics could be observed, the results furthermore imply that complex receptor-mediated changes occur on a regional plane.
While the MABP and blood gas values did not differ between both experimental groups, increased values of HR during severe blood loss have already been described in other studies involving humans and large animal models [19, 35]. Furthermore, significant increases of HR after relaxin-2 injection are described in different studies [20, 41]. This increase of the HR was not as pronounced in our study as might have been expected, even if demonstrable. We utilised a bolus injection with a high dosage of serelaxin, contrary to serelaxin prescription schemes for heart failure [42], in order to allow us to detect even weak responses of the pulmonary hemodynamics. The animals received a bolus injection equivalent to a daily human dose [42] – since in humans the substance is administered over 24 hours [43] though, the animals received a tenfold dosage as compared to human plasma levels (which have already been successfully applied in previous studies). The chosen amount of 30μg/kg serelaxin is a rather high dose, though, and represents a potential limitation of this study. In previous studies we measured relaxin-2 concentrations in serum samples from controls and serelaxin-treated animals [13] as well as relalaxin-2 immunoreactivity and peak serelaxin levels. Therefore the choice of dosage is directly linked to our earlier and preliminary studies, especially those examining the right hemodynamics in a large animal model (22), to ensure comparability and continuity with our preceding results regarding the substance’s effects on system physiology. Nonetheless, in a previous large animal model utilised to explore the cardioprotective properties of relaxin-2, the maximum effective dosage was 5μg/kg [44]. A high dosage of relaxin-2 can decrease target organ response because of agonist-induced receptor desensitization - [45] this mechanism was furthermore a likely contributor to the failure of clinical trials with higher dosages, such as on scleroderma patients with dosages of 100μg/kg per day. In them, the high dosages of relaxin-2 led to paradoxical disappearances of its effects [46]. The observed findings in this present study may be similarly blunted by high-dose agonist effect. While our present study should therefore be seen in the context of our continuing study model and preliminary results, future studies should consider the system physiological effects, in particular microcirculation in various end organs and hemodynamic changes, under different concentrations of relaxin-2. We are aware of the fact that this pilot study should therefore be considered to be of an explorative character.
The observational period of our experimental setup (70 mins) was specifically chosen, as to reflect and to evaluate serelaxin’s potential use in a scenario that mimics an emergency medical setting. Especially in the field of emergency medicine, drugs with a short(er) onset of effect, between a few seconds and 30 mins, are preferred. Since the half-life period of serelaxin is 6–8 hour and our experimental setup only allowed for an evaluation of 70 mins [42], subsequent studies are required to investigate the longer effects of the substance.
The positive chronotropic effects of relaxin-2 have been previously described [47]. Serelaxin’s effect on the PAcompl suggests that region-specific control of hemodynamics may be caused by differing relaxin-receptor densities within a complex regulatory system. This assumption is strengthened by the fact that no circulatory instability could be observed, which could easily have been the result of combining the scenario of a physiological redistribution mechanism with an additional (potentially indiscriminate) vasodilation via serelaxin.
In conclusion, our study showed that the application of serelaxin under severe hypovolemia reflecting a shock situation in a sheep model had no adverse effect on hemodynamic parameters. The results indicate that serelaxin might be a suitable candidate for (still necessary) further research as a potential neuroprotective agent, due to both its general effects (which are indicative of potential neuroprotective effects) and the in this study evidenced safety of application even during states of hypovolemia. Albeit the RELAX AHF 2 study did not render positive results, our results indicate that serelaxin could nonetheless be beneficial in clinical scenarios where an improved state of pulmonary hemodynamics is desirable, for example pulmonary hypertension (of differing causes) or acute heart failure.
Author contributions
René Schiffner, Sabine Juliane Bischoff and Martin Schmidt designed the study, conducted most of the experiments. René Schiffner and Martin Schmidt analyzed and interpreted the data, and drafted the manuscript; Thomas Lehmann did statistical analyses and interpreted data; Marius Nistor and Timo Zippelius in the design of the study and critically discussed the concept and data. All authors read and approved the final manuscript.
Disclosure/conflict of interest
This project was supported by a grant from Novartis Pharma GmbH. However, the provider of the grant in no way influenced the performed research or the interpretation of the data. Therefore, the authors declare no conflicts of interest.
Footnotes
Acknowledgments
We are grateful to Dr. Juliane Reiche, Petra Dobermann, Simone Göbel, Dirk Hergt and Gabriele Grunert for skilful assistance and support.