
Abstract
BACKGROUND:
Patients undergoing cardiac surgery commonly develop systemic inflammation associated with tissue edema, which impairs outcome. One main pathomechanism leading to the edema is the deterioration of the endothelial glycocalyx, a key component of the vascular barrier. In animal models hydrocortisone has proved to be protective for the glycocalyx.
OBJECTIVE:
This trial evaluates the effect of hydrocortisone on glycocalyx integrity in patients undergoing cardiac surgery with cardiopulmonary bypass.
METHODS:
In a prospective, randomized interventional pilot trial, 30 patients received either hydrocortisone (100 mg over 10 min) or placebo (saline control) before surgery. Plasma concentrations of glycocalyx constituents (syndecan-1, heparan sulfate) and various clinical parameters (respiratory and renal function, inflammatory markers, use of vasopressors, length of stay at the intensive care unit) were measured. Primary endpoint was a significant difference of glycocalyx constituents in plasma. Comparisons were made with Friedman’s and Wilcoxon tests (paired data), or the Kruskal-Wallis and Mann-Whitney U tests (unpaired data). Holm-Bonferroni method was used for post-hoc corrections.
RESULTS:
Heparan sulfate and syndecan-1 increased significantly during and after cardiac surgery with cardiopulmonary bypass in both groups. Whereas the maximum increase of heparan sulfate was 12.3-fold in the control vs. 3.8-fold in the pretreated group (p < 0.05), syndecan-1 values showed no significant difference between the groups (maximal increase 3-fold). The inflammatory markers C-reactive protein and interleukin-6 were also higher in the control than in the hydrocortisone group, but there was no difference in patient mortality (zero), or in any clinical parameters.
CONCLUSIONS:
Pretreatment with hydrocortisone ameliorated shedding of heparan sulfate, a major constituent of the endothelial glycocalyx, in patients undergoing cardiac surgery with cardiopulmonary bypass, but had no relevant influence on various clinical parameters or patient mortality. The relatively small number of patients in this pilot study probably precluded detection of positive outcome differences.
Introduction
Vascular endothelium has several vital functions, foremost in regulating blood flow, fluid shifts, vasomotor tone and hemostatic balance [1–3]. Involved in all of these actions is the endothelial glycocalyx, which coats all healthy vascular endothelium. Basically, it consists of membrane-bound and transmembrane proteoglycans, predominantly syndecan-1, carrying negatively charged side chains, mainly heparan sulfate [4]. Together with receptor-bound hyaluronan molecule chains and intercalated plasma proteins, the glycocalyx forms the endothelial surface layer. With a thickness of approximately 1μm, this surface layer plays a major role concerning vascular barrier function, anti-inflammatory behaviour and regulation of microvascular blood flow [5, 6]. The thickness of the endothelial glycocalyx and, thus, of the surface layer, is known to be reduced by ischemia/reperfusion, septic shock and hypervolemia, among other causes. This reduction increases capillary permeability and, thereby, contributes to tissue edema. Additionally it’s demonstrated, that in vitro cultured cells change their morphology and detach under shear load in a septic environment [7]. This alterations are associated with a higher mortality [8]. Experimental studies have shown hydrocortisone to have glycocalyx protective properties, most probably due to stabilisation of mast cells and, thus, amelioration of the release of histamine, cytokines, lyases and proteases [9–11]. Furthermore, the endothelial production of pro inflammatory cytokines and chemokines like IL-6, IL-17F, IL-8 and MCP-1 is inhibited and cell-adhesion receptors like ICAM-1 and VCAM-1 are downregulated by glucocorticoids [12–15].
Patients having undergone cardiac surgery may develop a systemic inflammatory response syndrome (SIRS) in the postoperative period, with a deleterious influence on postoperative morbidity [16]. SIRS is considered to be the result of a complex immunologic reaction comprising humoral, cellular and hemostatic factors, and caused by an imbalance of pro- and anti-inflammatory mechanisms [17]. Interestingly, stress doses of hydrocortisone have been shown to reduce systemic inflammation in patients undergoing cardiac surgery and to improve early outcome [18, 19]. For example, a previous double-blind, randomized trial by Weis and colleagues showed that stress doses of hydrocortisone attenuate the proinflammatory evolution of the IL-6/IL-10 ratio in patients with SIRS after cardiac surgery [18].
One major characteristic of SIRS is impairment of vascular barrier function with consecutive tissue edema, implicating the involvement of the endothelium. Shedding of the endothelial glycocalyx, a relevant aspect of inflammation and especially of enhanced vascular leak, has been detected in cardiac surgery, both of infants and adults [20, 21]. In this situation, one should expect that any mitigation of severe inflammation by prophylactic treatment would benefit patients.
The interventional trial presented here evaluates the effects of stress doses of hydrocortisone, infused prior to cardiac surgery, on damage to the glycocalyx and, therefore, implicitly on the integrity of the vascular barrier. It is a prospective, randomized, double-blind pilot study conducted on 30 patients undergoing cardiac surgery with cardiopulmonary bypass.
Material and methods
In the present pilot study, 30 patients were enrolled for evaluation of the effect of hydrocortisone on the endothelial glycocalyx before, during and after cardiac surgery with cardiopulmonary bypass (CPB). As detailed in previous work, exclusion criteria were: age <18 years, pregnancy, preoperative IL-6 levels >10 pg/mL, hepatic insufficiency (bilirubin >3 mg/dL), renal insufficiency (creatinine >2 mg/dL), a positive serologic test for HIV, manifest insulin-dependent diabetes mellitus, adipositas per magna (body mass index >30 kg/m2), use of steroidal or nonsteroidal ant-inflammatory drugs during the last 7 days (apart from 100 mg acetylsalicyl acid per day), any septic focus, or chronic or acute inflammatory diseases [18, 19]. The study protocol was approved by the Institutional Review Board of the Medical Faculty of the Ludwig-Maximilians-University Munich (No. 149/00) and the study was registered at clinicaltrials.gov (Clinical Trial Registration Information: NCT00490828). The abbreviations are listed at Table 3.
Measurement time points
The study protocol is outlined in Fig. 1. Plasma concentrations of constituent parts of the endothelial glycocalyx were determined preoperatively (T0), after induction of general anesthesia (T1), 30 min after onset of surgery (T2), 30 min after end of CPB (T3), 1 hour after termination of CPB (T4) and 4 hours after termination of CPB (T5). Inflammatory parameters were measured preoperatively (CRP and leukocytes) and at postoperative days 1, 2 and 3 (IL-6, CRP and leukocytes), cytokine and CRP being determined in serum. Blood gas was analysed at every time point. Measured clinical (outcome) values were: length of stay in the intensive care unit (ICU), length of stay in the intermediate care unit (IMC), duration and maximum dose of norepinephrine and epinephrine, duration of mechanical ventilation, lowest Horovitz index, maximum serum level of creatinine, incidence and duration of hemodiafiltration and dialysis, incidence of delayed awakening, and occurrence of delirium. Intraoperative use (kind and number) of blood products (fresh frozen plasma, packed red blood cells or platelets) was also recorded. All patients were followed up for 28 days after surgery to evaluate the primary study endpoints, i.e., the possible prevalence of significant differences in levels of glycocalyx constituents in plasma and of mortality.
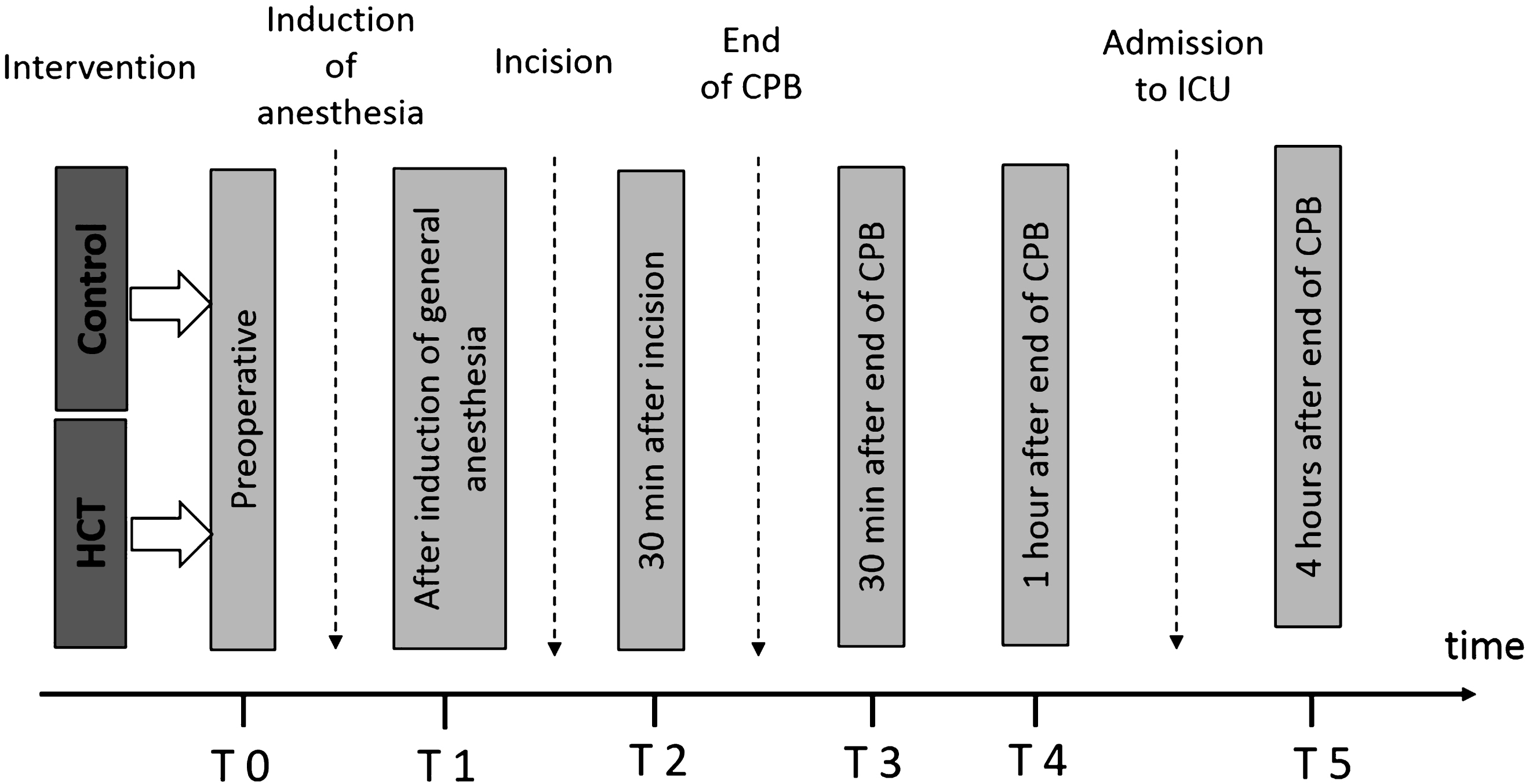
Study Protocol. HCT = hydrocortisone group (patients receiving stress doses of hydrocortisone), Control = control group (patients receiving 0,9% saline), CPB = cardiopulmonary bypass.
Patients were assigned to two groups by block randomization. In a double-blinded design, Group 1 received an intravenous stress dose (100 mg over 10 minutes) of hydrocortisone (Pharmacia & Upjohn, Erlangen, Germany) before induction of anesthesia. This was followed by a continuous infusion of 10 mg/h hydrocortisone for 24 hours (postoperative day [POD] 1). Infusion was reduced to 5 mg/h on POD 2, tapering off to 3×20 mg on POD 3. Group 2 served as control group and received placebo (0.9% saline solution). No other steroids were given during the study period.
Patient management
Anesthesia
Patients received oral midazolam (0.1 mg/kg) 1 hour before the induction of anesthesia. Patient’s long-term medication was continued until surgery, with the exception of oral anti-diabetic drugs and monoamine oxidase inhibitors. Monitoring included ECG with ST-segment analysis, blood pressure and pulse oximetry. Anesthesia was induced with midazolam (0.2 mg/kg), sufentanil (2μg/kg) and pancuronium (0.1 mg/kg), and maintained with sufentanil IV (1–2μg/kg/hr) supplemented by isoflurane 0.5 to 1.0 vol.%. Orotracheal intubation was followed by routine insertion of a central venous catheter and an introducer for a pulmonary artery catheter, both into the right internal jugular vein. In addition, transesophageal echocardiography was performed. Ventilation with 100% oxygen was controlled by intermittent blood gas analysis to achieve end-expiratory CO2 concentrations of 40±5 mmHg. If, despite sufficient hydration, a mean arterial pressure of 70 mmHg could not be achieved, norepinephrine was used as first-line vasopressor drug; epinephrine being first choice for inotropic support.
Surgical procedures
As detailed elsewhere, all operations were performed under mild hypothermia (32°C) with cold cardioplegic solution (Bretschneider Custodiol, Köhler Chemie, Alsbach-Hähnlein, Germany) [18, 19]. CPB was conducted with a roller pump (Stöckert, München, Germany) and a membrane oxygenator (Medtronic, Minneapolis, MN), the pump being primed with 1500 mL lactated Ringer’s solution containing 100 mmol/L of sodium bicarbonate and 10.000 IU of (porcine) heparin (Ratiopharm Ulm, Germany). During the operation, 2.5 g aprotinin (Trasylol, Bayer, Leverkusen, Germany) were administered. CPB was instituted at a flow rate of 2.4 L/min/m2 after systemic anticoagulation with (porcine) heparin 400 IU/kg BW (activated clotting time >400).
Determination of glycocalyx constituents
Arterial blood samples were withdrawn into serum vials and immediately centrifuged (2,000×g, 10 min). Afterwards, serum was frozen and stored at –80 °C until assayed.
As previously reported, serum heparan sulfate concentrations were quantified after pretreatment of serum with Actinase E (Sigma, St. Louis, MO, USA) and using the enzyme-linked immunosorbent assay of Seikagaku Corporation, Tokyo, Japan [22]. Serum syndecan-1 concentrations were determined using the enzyme-linked immunosorbent assay of Diaclone Research, Besancon, France, as reported [21, 22].
Statistical analysis
At the outset, the sample size required for the study groups was determined by means of a power analysis. Comparisons of paired data were made with Friedman’s test and the Wilcoxon test, as appropriate. For unpaired data, comparisons were made with the Kruskal-Wallis test and the Mann-Whitney U test, as appropriate. When indicated, post-hoc corrections for multiple measurements were performed with the Holm-Bonferroni method. We considered results from tests with p < 0.05 to indicate statistically significant differences in data values (IBM SPSS Statistics, Armonk, NY). All data in the paper are presented as median with interquartile range (IQR) or 95% confidence interval.
Results
The demographic data and procedural characteristics listed in Table 1 reveal that there were no significant differences between the two groups initially. In particular, there were no significant differences regarding pre-existing diseases, duration of surgery or the length of CPB.
Baseline values of intervention and control group
Baseline values of intervention and control group
Comparison of baseline values between the placebo and hydrocortisone group. Values are presented as median and interquartile range, p < 0.05 was considered significant.
Heparan sulfate
Baseline values of heparan sulfate at T0 did not differ (Fig. 2). Significant increases from baseline values were detected in both groups during surgery from T2 to T5 (Fig. 2, p < 0.05). There was a significant increase of serum heparan sulfate values in the control group from T1 to T5, with a maximum 12.7-fold increase at T3, 30 min after the end of cardiopulmonary bypass (Fig. 2, p < 0.05). In contrast, the maximum increase was 3.8-fold at T3 in patients who received hydrocortisone.
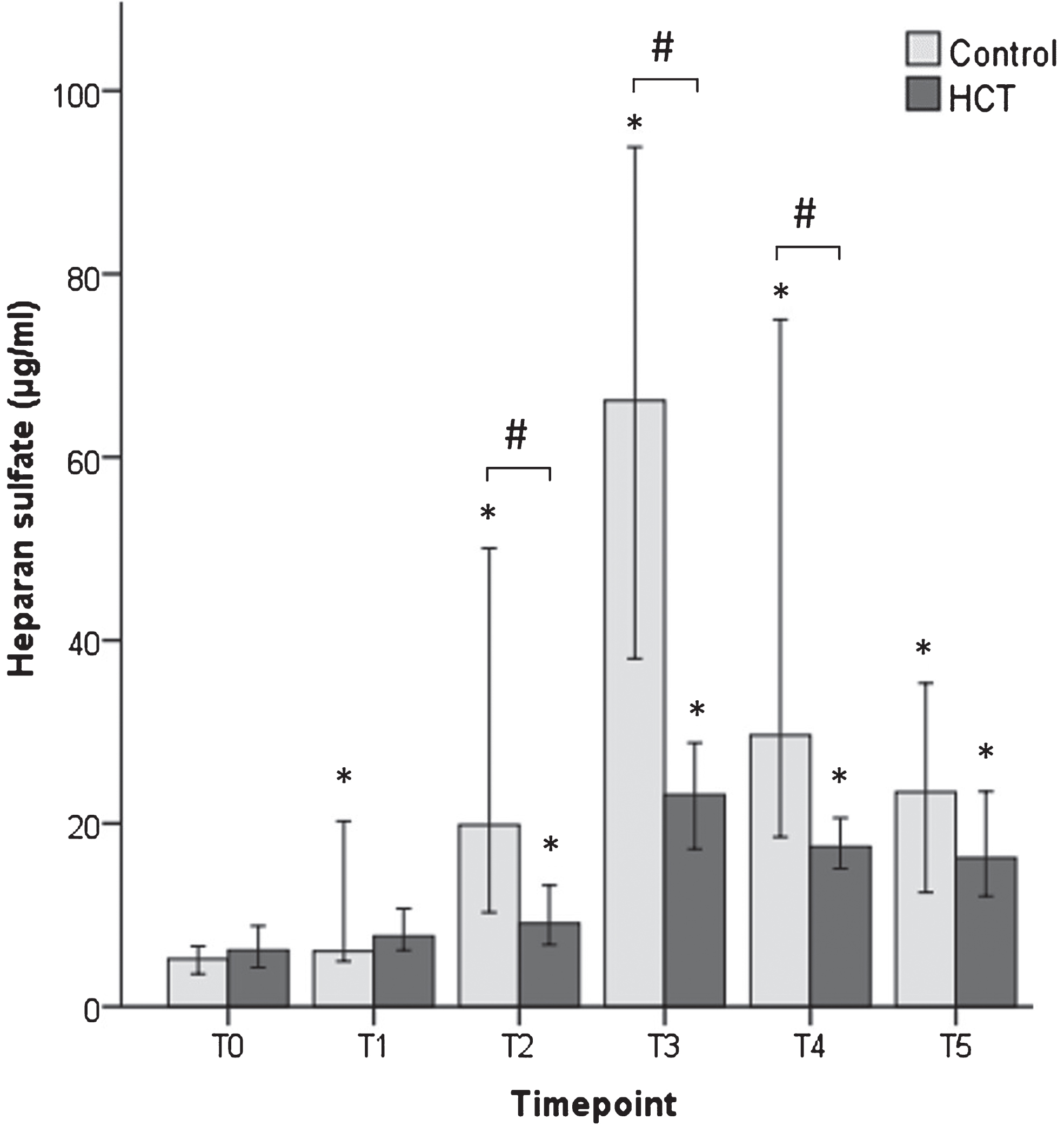
Release of heparan sulfate. Bars represent medians with 95% confidence intervals. * = significant difference to T0 within each group, # = significant difference between the control and intervention group at each timepoint (p < 0.05, resp).
Comparing the two groups, there was no significant difference between them after induction of general anesthesia (T1). However, 30 minutes after incision (T2), 30 minutes after beending CPB and one hour after the end of CPB, shedding had increased more in the control group than in the group that received hydrocortisone (intervention group; p < 0.05 at all 3 time points, Fig. 2). At 4 h after ending CPB, i.e., after admission to the ICU, shedding was still elevated above basal, but there was no longer a significant difference between the two groups (Fig. 2).
Baseline values of plasma syndecan-1 were identical in the two groups (Fig. 3). Shedding increased 3-fold before CPB in both groups (T2, p < 0.05) and tended to remain above the respective baseline level throughout the rest of the observation period. Although a significant difference from baseline existed at T4 in the intervention group (p < 0.05, Fig. 3), there were no significant differences between the two groups at any time point (Fig. 3).
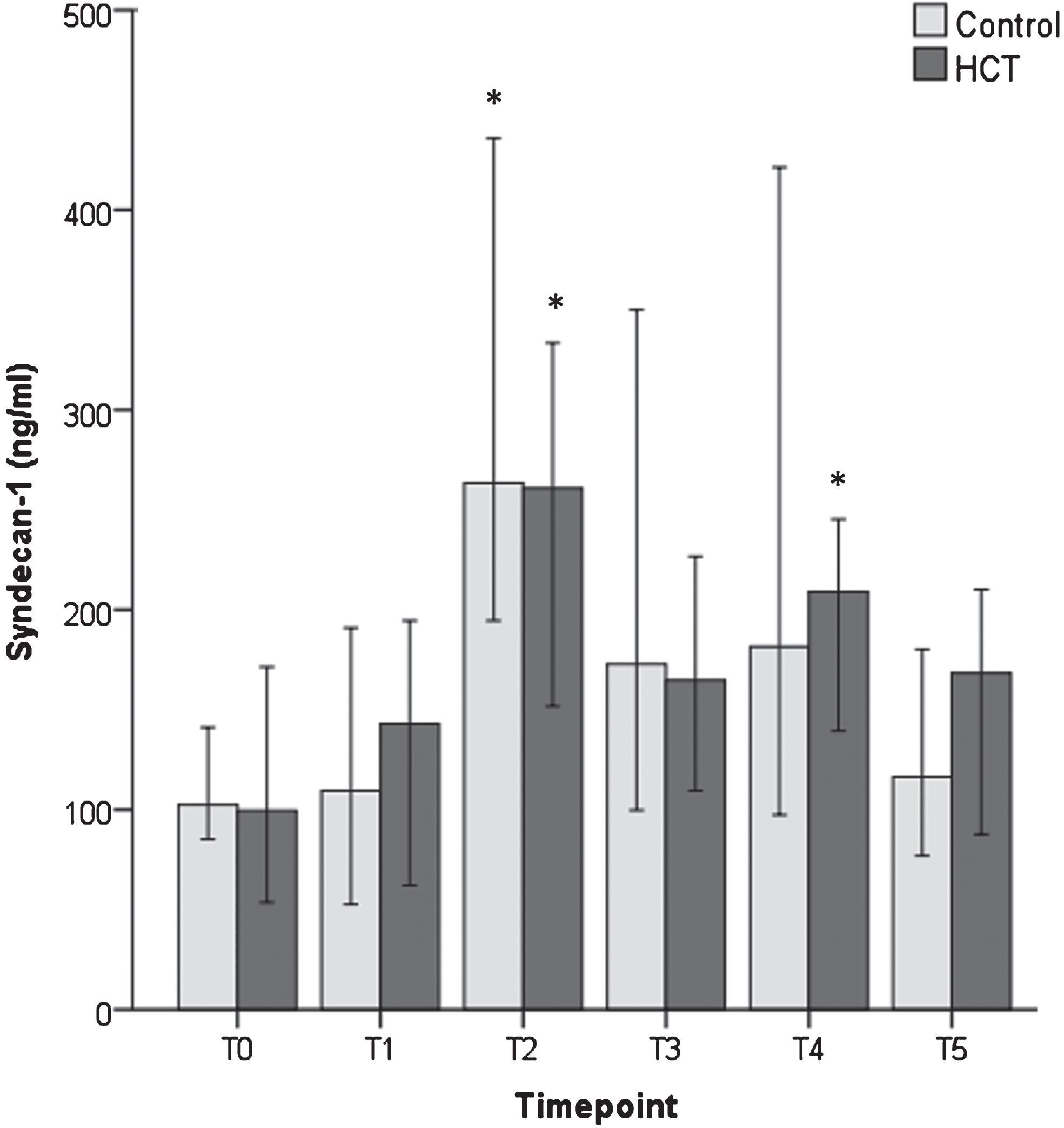
Release of syndecan-1. Bars represent medians with 95% confidence intervals. * = significant difference to T0 within each group, #=significant difference between the control and intervention group at each timepoint (p < 0.05, resp).
Table 2 lists inflammatory, clinical and outcome data of the study groups.
Outcome parameter
Outcome parameter
Outcome data. Data are presented as median and interquartile range. D = day, h = hour, hrs = hours, ICU = intensive care unit, IMC = intermediate care unit, CVVHDF = continuous veno-venous hemodiafiltration, PaO2 = arterial oxygen tension, FiO2 = inspiratory oxygen fraction.
Since no patient died in the observation period of 28 days post-surgery (POD28), there was no significant difference in the patients’ mortality.
There were no significant differences between the groups with respect to length of stay at the ICU or IMC, duration and maximum dosages of norepinephrine or epinephrine, duration of mechanical ventilation, lowest oxygenation index, renal function and renal replacement therapy, or delayed awakening and delirium (Table 2).
However, patients in the hydrocortisone group received significantly more fresh frozen plasma intra-operatively than those in the control group (median 6 vs. 3 packs, p = 0.025; Table 2). Substitutions by other blood components were similar in both groups (Table 2).
There was a significantly higher level of C-reactive protein in the control group than in the intervention group at post-operative days 1, 2 and 3, and also of Interleukin-6 at post-operative day 2 (p < 0.05, Table 2). Moreover, the maximum level of IL-6 attained post-operatively was higher in the control group, the median being about twice that of the intervention group (p < 0.05, Table 2).
The expected post-operative rise in leukocyte count took place on days 1, 2 and 3 in both groups. However, the number of leukocytes did not differ between groups on any of these days (Table 2).
Several studies exist to date that have examined shedding of the endothelial glycocalyx in patients during vascular and cardiac surgery, in septic shock and after trauma [20, 24]. In both latter situations, high plasma concentrations of glycocalyx components correlated with mortality. In fact, Nelson and co-workers showed that the plasma concentration of shed glycocalyx components correlated positively with mortality in patients suffering from septic shock [25].
The present prospective, randomized (double blinded) interventional trial confirms the finding that patients undergoing cardiac surgery have increased plasma levels of the glycocalyx constituents heparan sulfate and syndecan-1. More than this, it shows for the first time that the extraordinary, 12.3-fold increase in HS can be reduced by applying hydrocortisone preoperatively. Notably, the primary endpoint of a difference in glycocalyx shedding between both study groups was only achieved in the case of heparan sulfate, and not for syndecan-1. This finding is not only surprising, but may provide a very important lead to elucidating the processes involved in causing damage to the glycocalyx. Obviously, the mechanistic pathway responsible for shedding of heparan sulfate side chains evoked by the combined stimuli of surgery and CPB was more susceptible to inhibition by hydrocortisone than the one leading to cleavage of the transmembrane core protein syndecan-1.
Several clinical studies have previously evaluated the effects of hydrocortisone. Kilger et al. demonstrated that stress doses of hydrocortisone administered before cardiac surgery in high risk patients attenuated systemic inflammation and improved early outcome [26]. The same group presented evidence that this procedure also reduced perioperative stress exposure, decreased chronic stress symptoms, and improved health-related quality of life at 6 months after cardiac surgery [19]. In a further study, continuous intravenous hydrocortisone treatment was shown to attenuate severe SIRS by an immunomodulating effect and to improve outcome in high-risk patients after cardiac surgery. The authors suggested that the IL-6/IL-10 ratio might be a possible marker for guiding steroid treatment in patients [18]. A prospective, randomized, double-blind and placebo-controlled study demonstrated that hydrocortisone treatment induced a faster decrease in total organ dysfunction, predominantly based on a faster improvement of the cardiovascular organs, in critically ill patients [27]. Pertinently, it seems as though preoperatively infused hydrocortisone has a stronger effect, because a large multicenter trial showed no improvement of mortality when treating patients already suffering from septic shock [28]. However, if shock was reversible, patients receiving hydrocortisone recovered much more quickly. One reason could be that these patients had less glycocalyx damage than the ones in fulminant septic shock at the time when hydrocortisone was given. Although hydrocortisone also accelerates recovery from septic shock, no significant reduction of mortality was noted by the investigators in this scenario [28, 29], unless hydrocortisone was combined with vasopressin [30]. This suggests mechanistic differences in action of hydrocortisone between septic shock and damage associated with ischemia/reperfusion.
Despite the importance of hydrocortisone for treatment of various illnesses, and its widespread clinical use, the underlying cellular and molecular mechanisms of action are not completely understood and partially contradictory. For example, it is known that hydrocortisone is beneficial against ischemia/reperfusion injury by a process involving stimulation of the endothelial nitric oxide synthase [31]. Underlying cause for a beneficial action could, thus, be an anti-oxidative, radical-scavenging effect of enhanced NO [32]. In complete contrast, other work describes downregulation of expression and activity of enzymes producing vasodilatory agents such as nitric oxide and prostacyclin [33, 34]. By a different course of action, namely by attenuating the synthesis of various cytokines and chemokines, hydrocortisone prevents the adhesion and migration of inflammatory cells in the vascular system. This action probably encompasses a protective effect on the endothelial glycocalyx [35]. In line with this, hydrocortisone has also been shown to stabilize mast cells, inhibiting the release of various substances such as proteases, lyases or histamine [36]. Furthermore, glucocorticoids are known to achieve a decrease in transendothelial fluid flow and paracellular permeability for macromolecules. Consequently, they are routinely applied for the prevention of interstitial edema and swelling [37, 38]. Part of this effect may rely on an action directly on intercellular junctions. However, experimental studies have clearly revealed that hydrocortisone protects the glycocalyx after ischemia/reperfusion or inflammation, thereby reducing vascular permeability, tissue edema and adhesion of both, leukocytes and blood platelets [9, 39].
Since degradation of the glycocalyx is a very fast event and resynthesis of this structure presumably takes several days [8], delayed or protracted application of hydrocortisone may find it lacking the substrate via which a beneficial action can be brought about. Along these lines and in the case of operations involving ischemia/reperfusion the application of hydrocortisone should, if possible, occur preischemically.
Syndecan-1 is a trans-membrane protein and requires activation of proteases - most likely metalloproteases - before it can be shed off the endothelial cell [40]. On the other hand, shedding of heparan sulfate side chains can only be realized by heparinases and heparanases [4]. In man, the endogenous lyase capable of performing such cleavage is the enzyme mammalian heparanase, which is found stored in perivascular mast cells [41]. Fittingly, hydrocortisone is known to stabilize mast cells [11]; effects on metalloprotease activation are, at best, indirect [42].
A confounding issue could arise from the approximately 2-fold higher incidence of donation of fresh frozen plasma in the hydrocortisone group (Table 2). This bears consideration, because especially the plasma constituent albumin (20% in fresh frozen plasma, 100 ml per pack) has been found to be protective towards the endothelial glycocalyx [43]. Since control of plasma albumin performed routinely throughout the CPB procedure revealed no difference between Groups 1 and 2, the additional amount of albumin would not appear to have been relevant.
Abbreviations
Beside the effect of hydrocortisone on the glycocalyx constituent HS, the present study also detected an attenuated increase of several inflammatory parameters. There were significantly lower levels of C-reactive protein and Interleukin-6 in the hydrocortisone group. Even though this lowering of parameters did not accompany or reflect any observable clinical consequences – expected could have been a shortened duration of mechanical ventilation, a reduced demand of catecholamines, or less renal failure - some correlation between the levels of proinflammatory markers and glycocalyx constituents would seem plausible. This effect of proinflammatory chemokines like tumor necrosis factor alpha on the endothelial glycocalyx has been demonstrated previously [10]. However, in the present study there was no significant correlation between maximum shedding of syndecan-1 or heparan sulfate, on the one hand, and maximum values of CRP or IL-6, on the other hand. This could, most likely, be due to the relatively low number of patients enrolled in the present pilot study (15 per group).
Gratifyingly, none of the patients in our study died, irrespective of whether they were in the hydrocortisone group or not. This may well reflect a generally low level of operative stress in both groups, perhaps on account of the use of moderate hypothermia in all cases (see Methods). The low stress level, combined with the relatively low number of enrolled patients, presumably obscures possible clinical consequences. The study size was based on detecting differences of EG shedding between the two groups, whereas the clinical consequences of a reduction of EG shedding, like reduction of catecholamine use by maintaining vascular barrier function, and improvement of the oxygenation index owing to a prevention of potential pulmonary interstitial edema, etc., were not the primary end points. Quite obviously, in a future study, the number of patients should be extended to identify clinical consequences of the conclusive protection of the endothelial glycocalyx by hydrocortisone. Furthermore, additional clinical parameters should be evaluated which could better discern the potential effects of an impaired vascular barrier. Likely candidates would be the pulmonary vascular permeability index, extravascular lung water, and protein concentrations in the urine or the bronchoalveolar lavage fluid.
Author contribution
FB, DC: analyzing data, writing manuscript; TN: writing manuscript; DH: analyzing data, collecting data; GS: analyzing data, study protocol; BB: analyzing data, writing manuscript; MR: analyzing data, writing manuscript, FW: collecting data, analyzing data, writing manuscript, study protocol.
Footnotes
Acknowledgments
The present study was supported by the Else-Kröner-Fresenius foundation.