
Abstract
BACKGROUND:
Arteriovenous fistula (AVF) may affect erythrocytes through many pathways (e.g., mechanical, inflammatory). However, these effects haven’t been elucidated completely yet.
OBJECTIVE:
To follow-up the hemorheological and the hematological changes in the presence of artificial carotid-jugular fistula in rats.
METHODS:
Female Wistar rats were subjected to sham-operated group (SG, n = 6) and to fistula group (FG, n = 10). Under general anesthesia, the right carotid artery and jugular vein were isolated via a neck incision, and in the FG carotid-jugular fistula was performed by microsurgical techniques. Hematological variables, red blood cell (RBC) deformability and membrane (mechanical) stability parameters were determined before operation and on the 1st and 6th postoperative weeks. Density separated samples (‘young’ and ‘old’ RBCs) were also tested.
RESULTS:
In FG group hematocrit, RBC and platelet counts increased gradually to reach highly significant level of increment on the 6th postoperative week. RBC deformability significantly was impaired. The membrane stability test showed lower deformability values after applying mechanical shearing. No significant differences were observed between density separated RBC subpopulations.
CONCLUSIONS:
The presence of arteriovenous fistula may lead to an increment of RBC mass and impairment of RBC deformability. These changes could be one of the pathways through which the fistula influences the microcirculation.
Keywords
Introduction
Arteriovenous fistula (AVF) is considered as an important modification of the cardiovascular system since it is a direct connection between the arterial and venous circulations and has several regional and systemic effects especially in the presence of comorbidities or high-flow AVF [1, 2].
AVF affects markedly red blood cell (RBC). Some of these effects are mechanical effects, others are mediated by molecular mechanisms [3]. Blood flows through the AVF at high velocities due to the large pressure gradient between the artery and the vein, this high-velocity flow leads to high shear stress and turbulent flow. Other mechanical effects in human include the effect of the extracorporeal circulation and the peripheral dialysis needles [4]. All these stresses could cause intravascular hemolysis, and if they weren’t high enough to disrupt the RBC membrane, they could result in alteration in the hemorheological properties and the metabolism of RBCs [5]. The fistula has also effects on RBCs through other pathways such as inflammation and hypoxia [1, 3].
In turn, RBC properties could influence on the AVF itself, since the role of RBCs is not limited to transferring the oxygen, but RBCs have also effects on the flow, both on microcirculation level due to their deformability and aggregability and on the fistula flow due to the contribution of impaired hemorheological properties to thrombosis formation [6–8]. RBC mass also affects the blood viscosity thus blood flow, and one of the open question is the appropriate hematocrit level for fistula patient, since low hematocrit prevents microcirculatory stasis but reduces tissue oxygenation, while high hematocrit enhance oxygen transport but lead to an increased blood viscosity with a concomitant increase in tissue hypoxia [5, 9–12].
It is proven that the micro-rheological properties of RBCs influence the microcirculation [13–16]. Hence it is clinically important to evaluate the hemorheological changes in the cases of AVF, because it could clarify other mechanisms of microcirculation impairment in addition to the known role of steal syndrome. According to our knowledge, there is a lack of studies about the effects of AVF on RBC properties [17], and most of the studies focus on the effects of RBC properties on the AVF [6, 7], or on the effects of AVF on gene expression [18, 19]. Therefore, our hypothesis is that the arteriovenous fistula worsens the micro-rheological properties of RBCs as a suggested mechanism of impaired tissue perfusion. We assumed that more information will be available from studying the hemorheological differences between RBCs subpopulations, since the AVF could influence on the old RBCs populations through some mechanisms such as intravascular hemolysis.
Materials and methods
Experimental animals
The experiments were approved by the University of Debrecen, Committee of Animal Welfare (permission Nr.: 25/2016/UDCAW) in accordance with the Hungarian Animal Protection Act Law XXVIII/1998, EU Directive 2010/63/EU and the Ordinance 40/2013.
Sixteen healthy female Wistar (Crl:WI) rats were used at 10–12 weeks of age. The rats were housed in standard cages with free access to water and commercially available food. After at least ten days acclimation period, the rats were divided into two groups: fistula group (FG, n = 10, bodyweight: 272±22 g) and sham-operated group (SG, n = 6, bodyweight: 267±11 g). The rats were anesthetized always by the same protocol using sodium-thiopenthal (60 mg/kg, i.p., Thiobarbital 0.5 g, B. Braun Medical S.A., Spain), Atropine (0.05 mg/kg, s.c.) was administered before the surgery [20], and Flunixin (2.5 mg/kg, s.c.) was administered after the surgery for pain management.
Operative techniques
In the FG, the neck and the upper chest were shaved and prepared with Betadine ®. A 1.5-cm incision was made above the right clavicle, subcutaneous tissues and salivary glands were retracted upward and the right external jugular vein (EJV) and the right common carotid artery (CCA) were isolated without the resection of sternocleidomastoid muscle (SCM). The distal ends of EJV and CCA were ligated and the proximal ends were controlled using temporary clips, then the vessels divided in the middle, and end-to-end anastomosis was created between the proximal ends of EJV and CCA in front of the SCM using continuous suture with 10-0 polyamide suture material (Silon, Chirmax, Prague, Czech Republic). At the end, the clips were released, the patency of the fistula was confirmed, and the anastomosis and the incision were checked for any bleeding. The skin was closed with a 4-0 Glycolide-ɛ-Caprolactone (Monolac, Chirmax, Prague, Czech Republic).
Just after the procedure, 1-2 ml of 0.9% sodium chloride was injected to replenish any blood loss. After recovery, the animals were returned to individual cage. The rats were monitored regularly with wound care.
The rats in SG were prepared as FG rats, and the right EJV and CCA were totally isolated without any further procedures, then the skin was closed. For the procedures, an operating microscope (Leica Wild M650, LEICA Ltd., Germany) was used, and the procedures were documented by photos and video recordings.
Follow-up protocol
The rats were followed for 6 weeks. This period was determined to study the isolated effects of arteriovenous fistula, i.e., before the developing of heart failure, usually after 8 weeks [21]. The measurements were carried out before the surgery as baseline (FG-base and SG-base) and one week (FG-1W and SG-1W) and six weeks (FG-6W and SG-6W) after the surgery. The measurements included hematological and hemorheological measurements according to the protocol (described below). By the end of the measurements at 6th week follow-up the rats were sacrificed by exsanguination.
Blood sampling
Blood samples for baseline measurements in FG and SG were drawn from the lateral tail veins or directly from the EJV. On the 1st and 6th postoperative week, the blood samples were taken from the lateral tail veins (about 0.3 ml, as non-terminal sampling) and the caudal caval vein (about 2-3 ml, as terminal sampling), respectively. BD Vacutainer ® tubes were used (K3-EDTA 5.4 mg/3 ml). The laboratory measurements and procedures were begun within about 30 minutes after blood sampling.
Hematological measurements
Hematological parameters were tested using (Sysmex F-800 automate, Sysmex Co., Ltd. Japan). The measurement requires about 70 μl of blood. The studied parameters involved: white blood cell count (WBC [103/μl]), red blood cell count (RBC [106/μl]), hemoglobin (Hgb [g/dl]), hematocrit (Hct [% ]), mean corpuscular volume (MCV [fl]), mean corpuscular hemoglobin (MCH [pg]), mean corpuscular hemoglobin concentration (MCHC [g/dl]), red blood cell size distribution (RDW-CV%), platelet count (Plt [103/μl]) and mean platelet volume (MPV [fl]).
Hemorheological measurements
RBC deformability and membrane (mechanical) stability were studied using a LoRRca MaxSis Osmoscan ektacytometer (Mechatromics BV, The Netherlands). The test requires about 10 μl of blood mixed in 2 ml of polyvinylpyrrolidone (PVP) – phosphate buffered saline (PBS) solution (viscosity: 27 mPas, osmolarity: 300 mOsm/kg, pH: ∼7.3). The RBC deformability was studied by analyzing the laser diffraction pattern while applying increased shear stress (SS) from 0.3 to 30 Pa. The software calculates the elongation index (EI) and presents the data as EI-SS curves. EI values are proportional to the RBC deformability [22]. The maximal EI (EImax) and the shear stress at half-maximal deformation (SS1/2 [Pa]) were calculated using Lineweaver-Burke analysis. The ratio of EImax and SS1/2 was also compared [23, 24].
During membrane (mechanical) stability test RBC deformability measurements were performed before and after applying mechanical stress on the sample (100 Pa, 300 s) [25]. EI values, EImax and SS1/2 values were analyzed as ratio of data collected after/before applying the stress.
Density separation of RBC subpopulations and hematocrit standardization
The measurements of density separated RBCs require 2-3 ml of blood. This amount of blood is quite large relatively to rats, so these measurements were performed on other six healthy female rats as a negative control group (CG, n = 6, bodyweight: 271.33±11 g) and on 5 rats of FG-6W. About 2-3 ml of blood was drawn from the caudal caval vein, and hematological and hemorheological measurements were done. The rest of the sample was centrifuged at 4000 rpm (1800 g) for 60 min using centrifuge (Hettich Universal 32R, Germany), the layer of clear fluid (plasma) was aspirated and kept aside, and the ‘buffy-coat’ was removed. Since rat blood cells are known to be sensitive for physical effects, we did not wish to use centrifugation at higher force.
Selected variables comparing properties of RBC subpopulations after adjusting the sample hematocrit
Selected variables comparing properties of RBC subpopulations after adjusting the sample hematocrit
means±S.D.; CG: control group, n = 6. FG-6W: fistula group, sixth week after the construction of the fistula. Bottom and top: bottom 10% and top 10% of the RBC column in centrifuged samples, considered as dominantly ‘old’ or ‘young’ RBCs, respectively. *p < 0.05 vs. native Hct sample, #p < 0.05 vs. FG-6 W – Top.
The results were expressed as means±standard deviation (S.D.). For normally distributed data, the paired samples t-test and the one-way ANOVA test were used to evaluate the difference between paired two samples and independent two samples, respectively. For non-normally distributed data, the Wilcoxon signed-rank test and the Mann-Whitney U-test were used to evaluate the difference between paired two samples and independent two samples, respectively. P < 0.05 was considered statistically significant.
An IBM SPSS Statistics version 22 and Microsoft Excel 2016 were used for statistical analysis and graphs, respectively.
Results
General observations
One rat died in FG of accidental bleeding during the procedure. All other 15 rats survived for the period of follow-up, 6 weeks. All the wounds were healed well during the first week, and no other complications (bleeding, aneurysm or infection) were observed during the follow-up period.
Hematological parameters
Selected hematological results are shown in Fig. 1. First, the groups were compared at each stage. No significant differences were observed in the baseline measurements between the groups except in the value of Hct and Plt count. In FG, a gradual increase was observed during the follow-up period in RBC count, Hct and Plt count, and these increases became highly significant (p < 0.01) in FG-6W in comparison with SG-6W. WBC count increased temporarily in both groups 1 week after the surgery, but the values of WBC counts were significantly (p < 0.01) lower in FG-1W and FG-6W in comparison with SG-1W and SG-6W, respectively.
Selected hematological parameters in the sham-operated and the fistula group before surgery (base) and on the 1st and 6th postoperative weeks. A: white blood cell count (WBC), B: red blood cell count (RBC), C: hematocrit (Hct) and D: platelet count (Plt). means±S.D.; *p < 0.01 SG, #p < 0.01 vs. FG-base.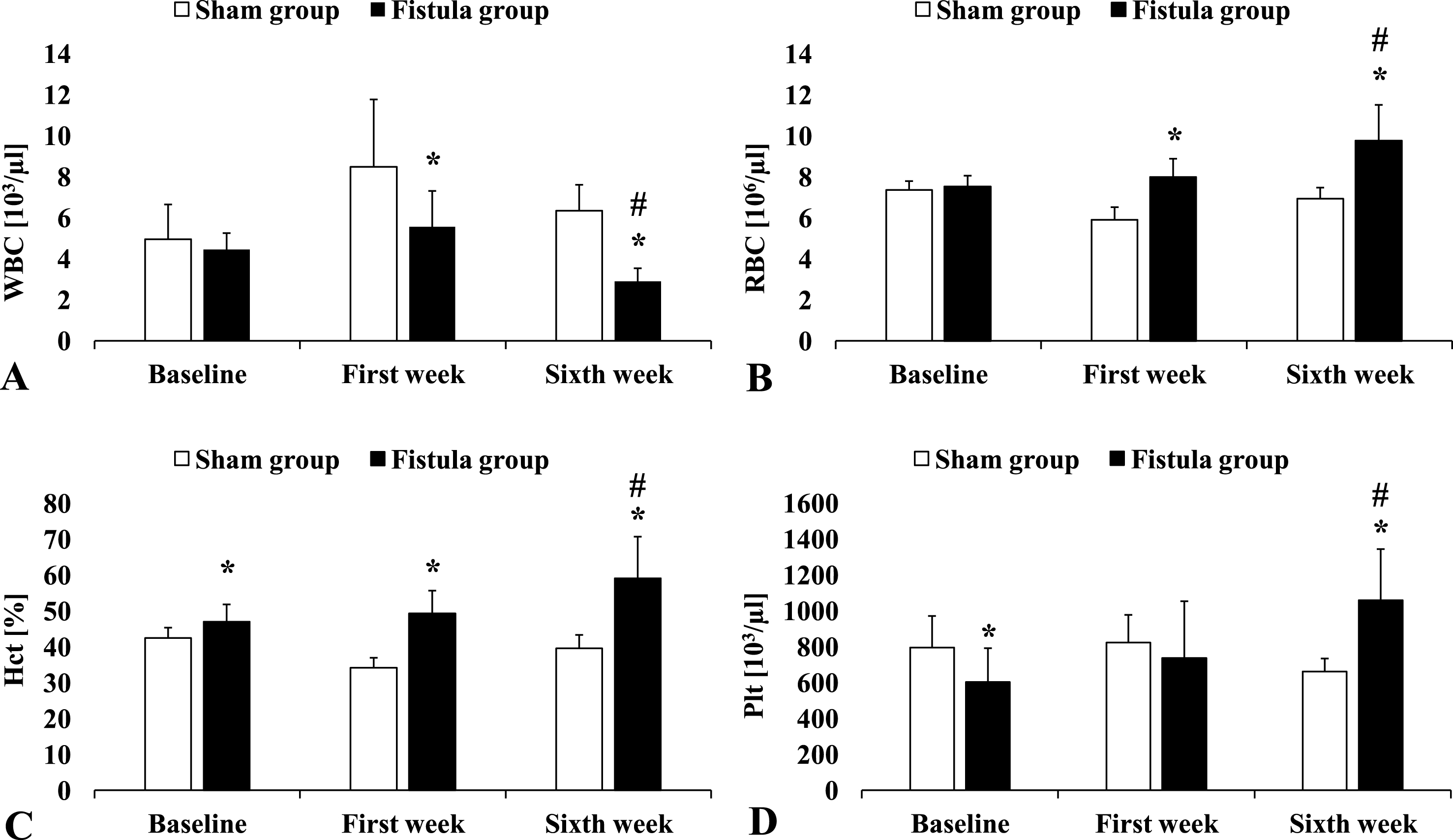
In comparison with baseline measurements (FG-base), the parameters of RBC mass, RBC count (p < 0.001) and Hct (p < 0.001), were increased significantly in FG-6W measurements. RBC indices showed also hypochromic RBCs and wider distribution in RBC size in FG-6W in comparison with FG-base, as MCH decreased significantly (p = 0.002) from 15.8±0.7 in FG-base to 13±2.2 in FG-6W and RDW-CV increased significantly (p = 0.007) from 13.09±0.54 in FG-base to 13.76±0.7 in FG-6W.
The SS1/2 and the ratio EImax/SS1/2 were calculated from EI-SS curves and presented in Fig. 2 to compare the differences of RBC deformability between the groups. No significant differences were found between the baseline measurements of FG and SG. However, EImax/SS1/2 ratio was significantly lower in FG-1W (p = 0.025) and FG-6W (p = 0.039) in comparison with SG-1W and SG-6W, respectively. The SS1/2 value was significantly higher in FG-1W (p = 0.003) and FG-6W (p = 0.043) in comparison with SG-1W and SG-6W, respectively.
Red blood cell deformability describing parameters in the sham-operated and the fistula group before surgery (base) and on the 1st and 6th postoperative weeks. A: shear stress at half-maximal elongation index (SS1/2), B: ratio of maximal elongation index (EImax) and SS1/2. Means±SD; *p < 0.05 vs. SG.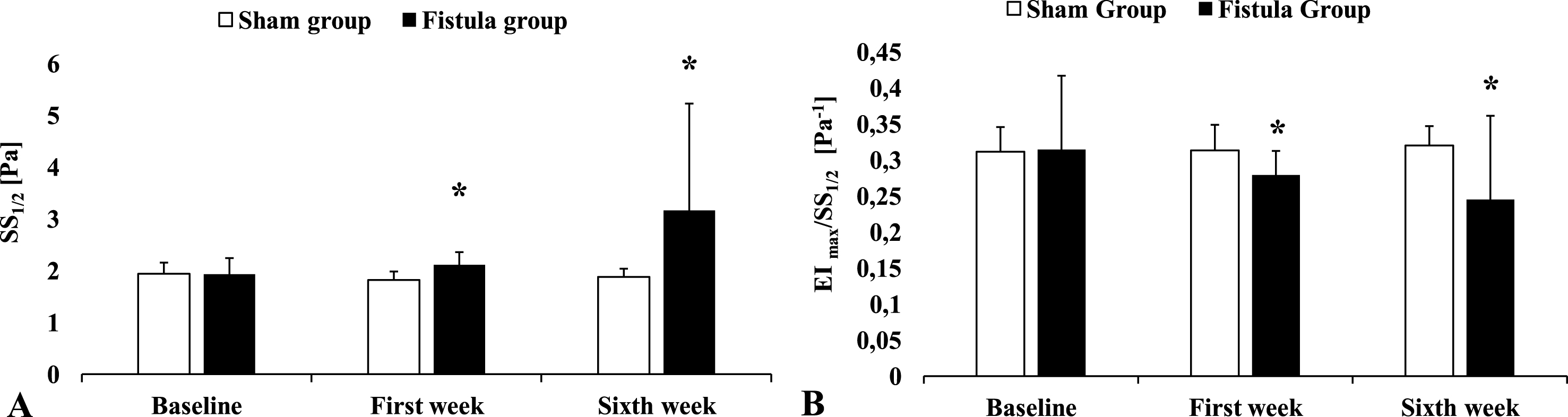
Figure 3 shows lower RBC deformability profile in FG-6W both before and after membrane stability test and Table 1 shows the changes of the parameters of RBC deformability before and after the membrane stability test.
Elongation index – shear stress curves of RBC deformability before and after applying mechanical shear stress (100 Pa for 300 s). Means; SG: sham group, n = 6. FG: fistula group, n = 8. 6W: sixth week after the surgery. Changes of EImax/SS1/2 and SS1/2 values before and after applying mechanical stress on the samples (100 Pa for 300 s) means±SD; SG: sham group, n = 6. FG: fistula group, n = 8. 6W: sixth week after the surgery. *p value <0.01 vs. before. #p value <0.05 vs. before.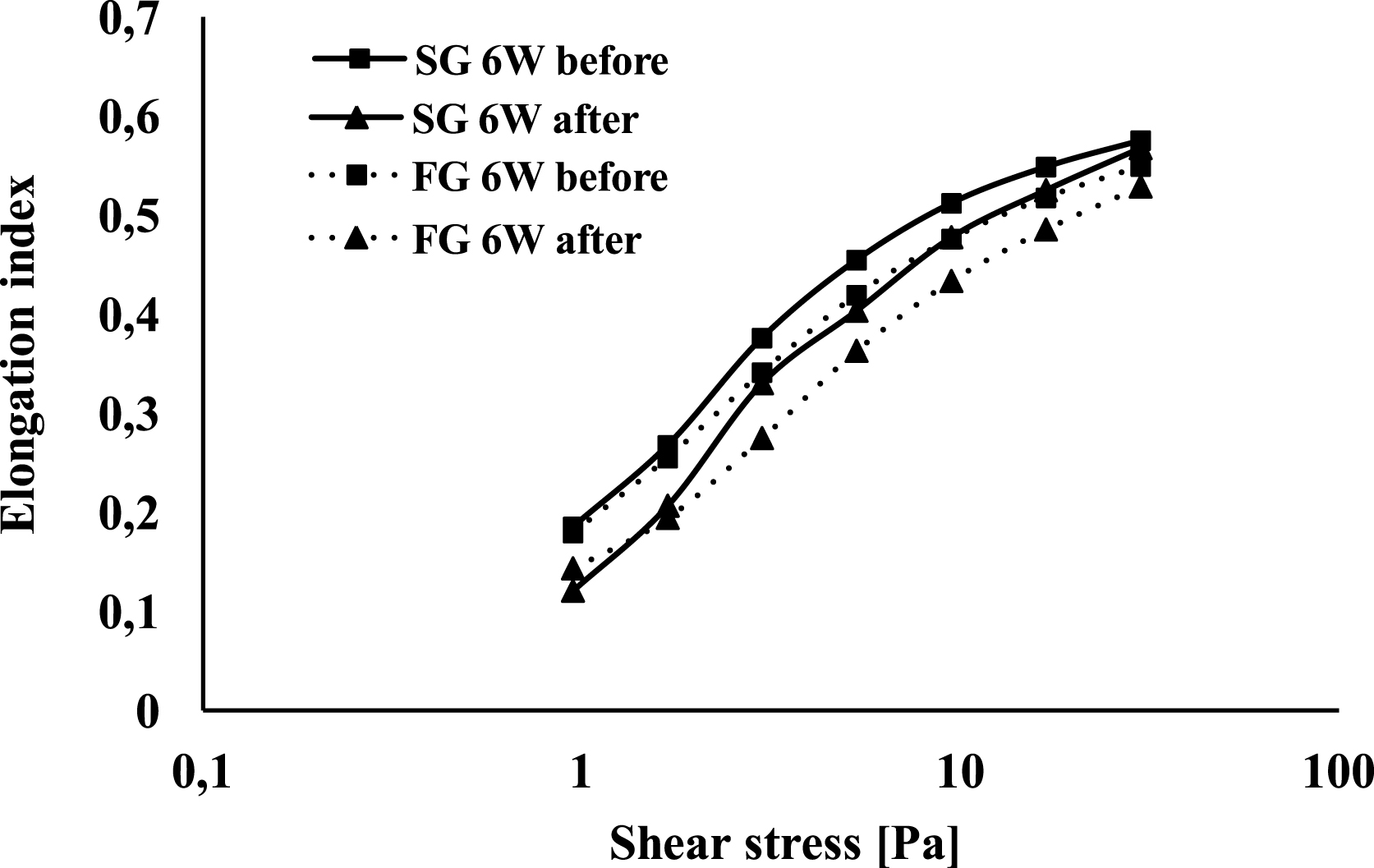
After applying membrane stability test (100 Pa shear stress for 300 s) on RBCs, the deformability of RBCs was decreased significantly (p < 0.01) in SG-6W for shear stress range (0.95–30 Pa) and in FG-6W for shear stress range (3–30 Pa). The ratio of RBC deformability values after/before applying the stress was calculated at each shear stress and compared between FG-6W and SG-6W. This ratio was smaller in FG-6W, however, without significant differences.
After the separation of the subpopulations of RBCs, no significant differences were observed in hematological parameters except significant increase (p = 0.014) of RDW-CV in the bottom 10% of FG-6W in comparison with the top 10% of FG-6W. Figure 4 shows EI-SS curves to compare the deformability of two RBC subpopulations, top 10% RBCs showed slightly higher deformability than bottom 10% RBCs without significant differences between the subpopulations.
Elongation index – shear stress curves of the ‘young’ (upper 10%) and ‘old’ (lower 10%) RBCs in fistula group (A) and in control group (B). Means±S.D.; CG: control group, FG: fistula group. Lower or bottom 10% and upper or top 10% of the RBC column in centrifuged samples, considered as dominantly ‘old’ or ‘young’ RBCs, respectively.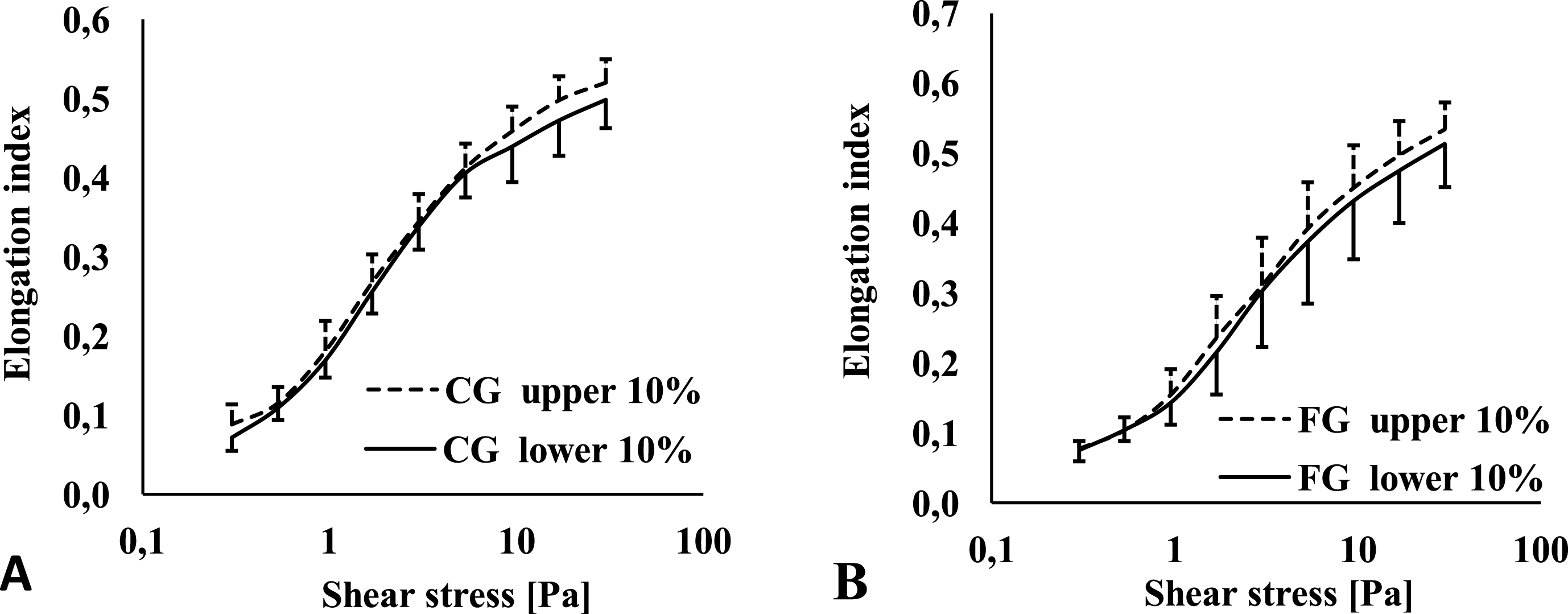
AVF is considered as a first option for hemodialysis in patients suffering from end-stage renal disease [26]. Researches have given importance to study the effects of AVFs, but these effects on RBCs haven’t been well understood yet. Current study showed a significant increment of the value of RBC count and Hct in FG-1W and FG-6W measurements in comparison with the parallel SG measurements, SG-1W and SG-6W. Although Hct was higher even before the AVF procedures in the FG group, but the differences between SG and FG became larger in first and sixth week measurements. This increment of RBC mass refers to a reactive process called secondary polycythemia characterized by an increase in serum erythropoietin [10]. As known, erythropoietin production is regulated by decreased oxygen delivery to tissues, and hypoxia-inducible factor-1 (HIF-1) has the central role in transcriptional activation of the erythropoietin gene [10, 28]. Tissue hypoxia accompanies the fistula both in the case of severe heart failure and in the case of steal syndrome [8, 29]. Some studies showed that the expression of HIF-1 increases also locally in the venous segment of AVF because of the damage of the vasa vasorum and thus local hypoxia [3, 30].
However, studies about aortocaval fistula in rats showed significant decrease in Hct as opposed to our results [31, 32], while another study about saphenous fistula didn’t show significant difference in Hct between control group and fistula group [33]. We suppose that this significant difference between studies are related to the location of the fistula, since the inflow of CJF is proximal to the arteries of kidney and liver, the most important producers of erythropoietin. CJF could steal blood from these organs and induce hypoxia, the main regulator of erythropoietin production [27, 35].
Secondary polycythemia has some special aspects. Secondary polycythemia is individual, occurs in some hypoxia cases and doesn’t occur in others without obvious reasons [10, 36]. The same issue was noticed partially in current study, since Hct values increased for each rat after 6 weeks of the creation of the fistula, but the rate of increase was quite different from one rat to another.
Another aspect is the iron deficiency which accompanies polycythemia in more than 30% because of the depletion of iron stores to support erythropoiesis [10]. By comparing hematological results in FG-6W with those in FG-base, significant differences in the hematological parameters indicate iron deficiency such as elevated RDW, high platelet count, significant low MCH. Although HIFs enhance intestinal iron intake, the lack of iron in the used commercially food and chronic intravascular hemolysis through the AVF lead to more reduction in iron stores.
The Plt count increased gradually during the follow-up period, and mean platelet volume decreased. Thrombocythemia was considered as a sign of iron deficiency, but other factors could also contribute in this increment such as acute phase reactions and spurious increase related to fragmented RBCs [37–40].
Another purpose of the study was to evaluate the hemorheological profile. By studying the hemorheological parameters individually, some rats’ RBCs didn’t show changes in the deformability, others showed impairment of the deformability, and there is no explanation for these difference, since these rats had the same strain, gender, hematological changes and experimental environment. However, as an average, the deformability of RBCs was impaired significantly according to the studied deformability’s parameters: significant decrease of EImax/SS1/2 and significant increase of SS1/2, and these individual differences explains the high value of standard deviation. This impairment is due to the mechanical stresses applied on the RBCs through the disturbed high-flow in the AVFs [4]; In addition to other many accompanied mechanisms such as inflammation and hypoxia [1, 3].
Our plan was to gather more information about RBC’s deformability by separating the subpopulations of RBCs using centrifugation at 1800×g for 60 min, and the results showed that EIs for the young RBCs were slightly higher in comparison with EIs for old RBCs in both CG and FG-6W as shown in Fig. 4, but these differences were not significant. Maybe we had to centrifugate using higher forces or longer time as in other studies (e.g., 10000 g for 15 min) [22].
The Hct was standardized to 40% as described in the methods during the preparation of young and old RBCs, and it was interested to evaluate the difference of RBC’s properties after the standardization of Hct. The parameters of both top and bottom 10% blood sample were considered as a representative of standardized Hct, and the parameters of the baseline measurements were considered as a representative of native Hct. The results are summarized in the Table 2 and show significant differences in the parameters of FG-6W (SS1/2, EImax/SS1/2 and RDW-CV%) after the standardization of Hct in comparison with the parameters before the standardization (Native Hct). The same significant differences were not observed in CG, but the change of Hct in CG (approximately 7%) was lower than the change of Hct in FG-6W (approximately 19%).
Many studies focus these days on the role of RDW-CV% as a risk factor for AVF failure, heart failure and cerebrovascular diseases [7, 42]. In addition, it is an early sign of iron deficiency and a hemorheological parameter. The value of RDW-CW% was significantly higher in FG-6W in comparison with FG-base, and significantly higher in old RBCs of FG-6W in comparison with young RBCs of FG-6W.
Conclusion
The presence of the artificial arteriovenous fistula may lead to an increment of RBC mass and impairment of RBC deformability. These changes could be one of the pathways through which the fistula influences the microcirculation.
Footnotes
Acknowledgments
Authors are grateful to the technical and laboratory staff of the Department of Operative Techniques and Surgical Research at University of Debrecen, and a special thanks to Györgyné Gödény for her dedicated work. The study was supported by the Stipendium Hungaricum program.
The authors comply with the Ethical Guidelines for Publication in Clinical Hemorheology and Microcirculation as published on the IOS Press website and in Volume 63, 2016, pp. 1-2. of this journal.