
Abstract
BACKGROUND:
Platelet activation is linked with thrombosis, inflammation or heart failure.
OBJECTIVE:
To establish clinical and analytical factors that may favor high mean platelet volume (MPV) and to determine if MPV levels favor major adverse cardiovascular events (MACE).
METHODS:
Stable CHD patients and a control population matched for age, sex and cardiovascular factors.
RESULTS:
658 CHD patients and 2092 controls were studied. Median age in CHD patients was 33 (25–41) year old with 56% of them being male. No significant differences were seen between MPV values and cardiac complexity (p = 0.308) nor between MPV values in the CHD and control groups (p = 0.911). CHD patients had significant lower platelet count and MPV levels than patients in the control group. In the binary logistic regression analysis NT-pro-BNP levels above 125 pg/ml, thrombocytopenia and having atrial fibrillation/flutter reached statistical significance as predictors of MPV levels above 11 fL. The Kaplan-Meier survival analysis showed no significance between MPV levels higher than 11 fL and MACE, cardiovascular mortality and thrombotic events in a median time follow-up of 6.7(1.5–10.6) years.
CONCLUSIONS:
Atrial fibrillation/flutter, heart failure and thrombocytopenia are predictors of high MPV levels. A MPV above 11 fL is not associated with MACE at a median follow-up time.
Introduction
Platelets secrete and express a large number of substances that are crucial mediators of coagulation, inflammation, thrombosis, and atherosclerosis [1]. Larger platelets are enzymatically and metabolically more dynamic than smaller ones, and they exhibit greater prothrombotic potential [2]. Within an individual, platelets are heterogeneous in size and density and mean platelet volume (MPV), the most commonly used measure of platelet size, is a potential marker of platelet reactivity [3], inflammation [4], heart failure [5] and thrombosis [6]. In fact, MPV is felt to be a surrogate marker on platelet function. In this context, some authors have found an association between raised MPV levels and an increased risk of stroke [7], myocardial infarction [8–10] or thrombotic events in adult congenital heart disease (CHD) patients with Eisenmenger syndrome [11]. With reference to the latter, the authors suggest that platelet activation plays an independent role in thrombosis in these patients beyond secondary erythrocytosis and its possible effect on blood viscosity. However, possible confounding effects on platelet function assessment may occur.
The aim of this study is to compare platelet count and MPV levels in CHD patients and a control population and to establish which clinical and analytical factors may favor high MPV values in addition to determine if MPV levels affect cardiovascular mortality and thrombotic events in CHD patients.
Methods
Study population
Retrospective study on all clinically stable CHD patients seen at our Adolescent and Adult CHD Unit between February 2000 and September 2018. Inclusion criteria were being older than 14 years, having a structural CHD and a routine blood test with the parameters of the study. Emergency blood tests and blood tests within 6 months after surgery/catheter intervention, major bleeding, or phlebotomies were excluded from the analysis. CHD patients were classified into diagnostic groups according to the underlying cardiac anatomy. Consistent with published classification schema, cardiac defects were categorized as simple, moderate or great complexity [12].
Clinical data
Arterial hypertension (blood pressure > 140/90 mmHg or with antihypertensive treatment) and diabetes mellitus (serum glucose > 126 mg/dL or under oral anti-diabetic agents or insulin medication) were diagnosed according to the European Society of Cardiology guidelines [13, 14]. Systemic arterial hypertension, in patients under 18 years old, was defined as blood pressure more than the 90th percentile for age, sex and height [15]. Dyslipidemia if the LDL cholesterol level was above 130 mg/dL or the patient was taking statins [16]. Patients were classified as smoker if they were current smokers. Body weight and height (BMI) were measured with the patients wearing light clothes and barefoot and BMI was calculated by the formula weight (kg)/[height (m)×height (m)]. Glomerular filtration rate (GFR) was estimated in all the patients with Modification of Diet in Renal Disease formulae (186×[creatinine (mg/dl)] – 1.154×[age (years)] – 0.203×[0.724 if female]) [17]. Thrombocytopenia was defined as a platelet count below 150 10∧3/μL. Atrial and flutter fibrillation were diagnosed by reviewing the medical history or an electrocardiogram test. The systemic ventricular ejection fraction of a morphologic left ventricle was calculated by the Simpson’s biplane method [18] and it was considered abnormal when it was less than 55% [19]. On the other hand, a systemic morphologic right ventricular function was determined with the tricuspid annular plane systolic excursion (TAPSE). A TAPSE under 16 mm was considered abnormal [20]. Cyanosis was defined as basal hemoglobin oxygen saturation <93%. Eisenmenger syndrome was defined as pulmonary arterial hypertension with cyanosis in the presence of a large non-restrictive intracardiac or extracardiac defect [21].
Cardiovascular and stroke endpoint events were classified as reported by the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards [22]. Major Adverse Cardiovascular Event (MACE) was defined as both arterial thrombotic events and cardiovascular mortality. CHD patients were followed up by reviewing the clinical history or telephone calls.
Control patients were obtained among patients attending the outpatient clinic of the community health centers of the same geographical area, between July 2017 and April 2018 due to trivial processes such as anxiety, palpitations, skin rash, itching, pains in muscles and back or common cold and matched for age, sex, arterial hypertension and diabetes mellitus to CHD patients. All patients gave informed consent to participate in the research study and the study protocol was approved by the hospital’s ethics committee.
Blood collection
EDTA blood samples (K3EDATA 7,2 mg vacumm blood colettion tubes; Vacutest Kima, Arzergrande (PD), Italy) were drawn from each patient on an outpatient basis and processed within 30 minutes of venipuncture. Complete blood counts were performed on a Coulter LH 750 (Beckman Coulter, Fullerton, CA, USA) analyzer. Direct inspection of blood smears excluded platelet aggregation as an artifactual cause of thrombocytopenia in those patients with a MPV higher than 12 fl. Thrombocytopenia was defined as a platelet count <150×103 μL. As the MPV cut off value that predicts cardiovascular events in clinical practice remains unknown [23] we used, as a MPV cutoff value for CHD patients, the 95th percentile of the MPV value in the control group. The remaining analytical data such as serum apoferritin, serum creatinine, C reactive protein (CRP) and N-terminal pro B-type natriuretic peptide (NT-pro-BNP) levels were measured as previously reported [24]. A cut-off value of 125 pg/mL was used for NT-pro-BNP levels as it effectively rules out left ventricular dysfunction [25].
Statistical analysis
Characteristics were summarized by mean±standard deviation or median (interquartile range) for continuous measurements and by percentages for categorical measurements. Kolmogorov-Smirnov test was used to assess normality of distribution of continuous variables. Student’s t-test was used for the comparison of two means with normal distribution while the Mann-Whitney test was used in those cases without normal distribution. Pearson’s chi-squared test was applied to sets of categorical data. Multiple linear regression analysis was used to explain the relationship between one continuous dependent variable and two or more independent continuous or categorical variables. Binary logistic regression analysis was used to predict the relationship between a dependent binary variable and continuous or categorical independent variables after excluding high intercorrelations among the predictors. The results were expressed as odds ratios (ORs) with their 95 % confidence intervals (CIs). Kaplan-Meier survival curves for MACE, arterial thrombotic events and cardiac mortality, according to a cut-off MPV value of 11 fL, were compared by the log-rank test. A p values less than 0.05 was considered statically significant. Data analysis was carried out using SPSS 19.0 (SPSS, Chicago, IL).
Results
658 out of a total of 818 CHD patients were included in the analysis. Control population consisted of the 2092 patients matched for age, sex, arterial hypertension and diabetes mellitus to the CHD group. Table 1 shows CHD patients classification in relation to complexity. No significant differences were seen between MPV values and cardiac complexity (p = 0.308) nor between MPV values in the CHD and control groups (p = 0.911). Table 2 shows demographic, clinical and analytical data in CHD patients and the control population matched for age, sex, arterial hypertension and diabetes mellitus. Interestingly, CHD patients had significant lower platelet count and MPV levels than patients in the control group. Nonetheless, the 95th percentile of the MPV levels in the control and CHD patients was of 10.94 fL and 10.91 fL respectively.
Congenital cardiac classification system guided by the report of the 32nd Bethesda Conference [12] and Mean Platelet Volume above and below 11 fL
Congenital cardiac classification system guided by the report of the 32nd Bethesda Conference [12] and Mean Platelet Volume above and below 11 fL
The data are expressed as number of patients.
Demographic, clinical and analytical data in congenital heart disease patients and the control population
n: number of patients, CHD: congenital heart disease, MPV: mean platelet volume. Thrombocytopenia is defined as a platelet count below 150 103 μL. †Oral anticoagulation includes patients under Vitamin K Antagonists (e.g. Warfarin, Coumarins) and Non-VKA Oral Anticoagulants (NOACs). ††Diuretic treatment includes patients under loop-acting diuretics and/or thiazide diuretics. Data are expressed as median and quartiles (25–75) and as number and percentage. *Categorical variables are evaluated by the Pearson chi-square test and continuous data without normal distribution by the Mann-Whitney test.
Table 3 shows demographic, clinical and analytical data of CHD patients with MPV values above and below 11 fL. Descriptive analysis showed no significant differences in the parameters studied except for having atrial fibrillation or flutter, the percentage of lymphocytes, platelet count, thrombocytopenia and NT-pro-BNP levels according to heart failure diagnosis (above/below 125 pg/mL).
Clinical and analytical data in CHD patients with MPV values above and below 11 fL
CHD: congenital heart disease, MPV: mean platelet volume, n: number of patients, BMI: body mass index, NYHA: New York Heart Association, NT-pro-BNP: NT-pro-brain natriuretic peptide, ACE: angiotensin convertin enzyme, ARBs: angiotensin receptor blockers. †No patient under 18 years showed systemic arterial hypertension. ††Thrombocytopenia is defined as a platelet count < 150×103 μL. Data are expressed as mean±standard deviation, median and quartiles (25–75) and as number and percentage. *Categorical variables are evaluated by the Pearson chi-square test, continuous data with normal distribution are compared by Student’s t-test and continuous data without normal distribution by Mann-Whitney test.
Simple linear regression analysis in CHD patients showed a negative correlation between MPV levels and platelet count (partial correlation: – 0.095, p = 0.014) and a positive correlation between MPV levels and NT-pro-BNP concentration (partial correlation: 0.105, p = 0.045) and between MPV levels and being female (0.100, p = 0.011). In fact, median MPV values were significant higher in female than in male CHD patients [8.8 (7.2–10.8) vs. 8.5 (6.39–11), p = 0.003]. At the same time, the multiple linear regression model with the three predictors produced a R2 = 0.021, F (3.65), p = 0.013. On the other hand, age remained at the limit of the statistical significance (p = 0.052) while the rest of parameters exhibited in Table 3 did not reach statistical significance in the linear regression analysis.
Meanwhile, the binary logistic regression analysis (Table 4) determined that NT-pro-BNP levels above 125 pg/ml, thrombocytopenia and having atrial fibrillation/flutter were the only parameters that reached statistical significance as predictors of MPV levels above 11 fL in both crude and adjusted odds ratios (Table 4).
Results of the binary logistic regression analysis of congenital heart disease patients with MPV lower and higher than 11 fL
OR: odds ratio, CI: confidence interval, NT-pro-BNP: N-terminal proB-type natriuretic peptide. †Combination of patients with arterial hypertension, diabetes mellitus and/or dyslipidemia. ††Combination of patients with anticoagulation and/or antiplatelet treatment. γ Thrombocytopenia is defined as a platelet count below 150 103 μL.
MACE occurred in 52 patients during a median time follow-up of 6.7 (1.5–10.6) years. 4 patients with arterial thrombosis died during the follow up. Table 3 shows the distribution of arterial thrombosis, hemorrhage, cardiovascular death and MACE among CHD patients with MPV values above and below 11 fL. 26 patients had arterial thrombotic events: 20 patients had a stroke, 4 patients had myocardial infarction and 2 patients had peripheral arterial events. The Kaplan-Meier events free survival curves showed no statistical significance between MPV levels above or below 11 fL in relation to MACE (p = 0.358) (Fig. 1), cardiovascular mortality (p = 0.991) and thrombotic events (p = 0.265).
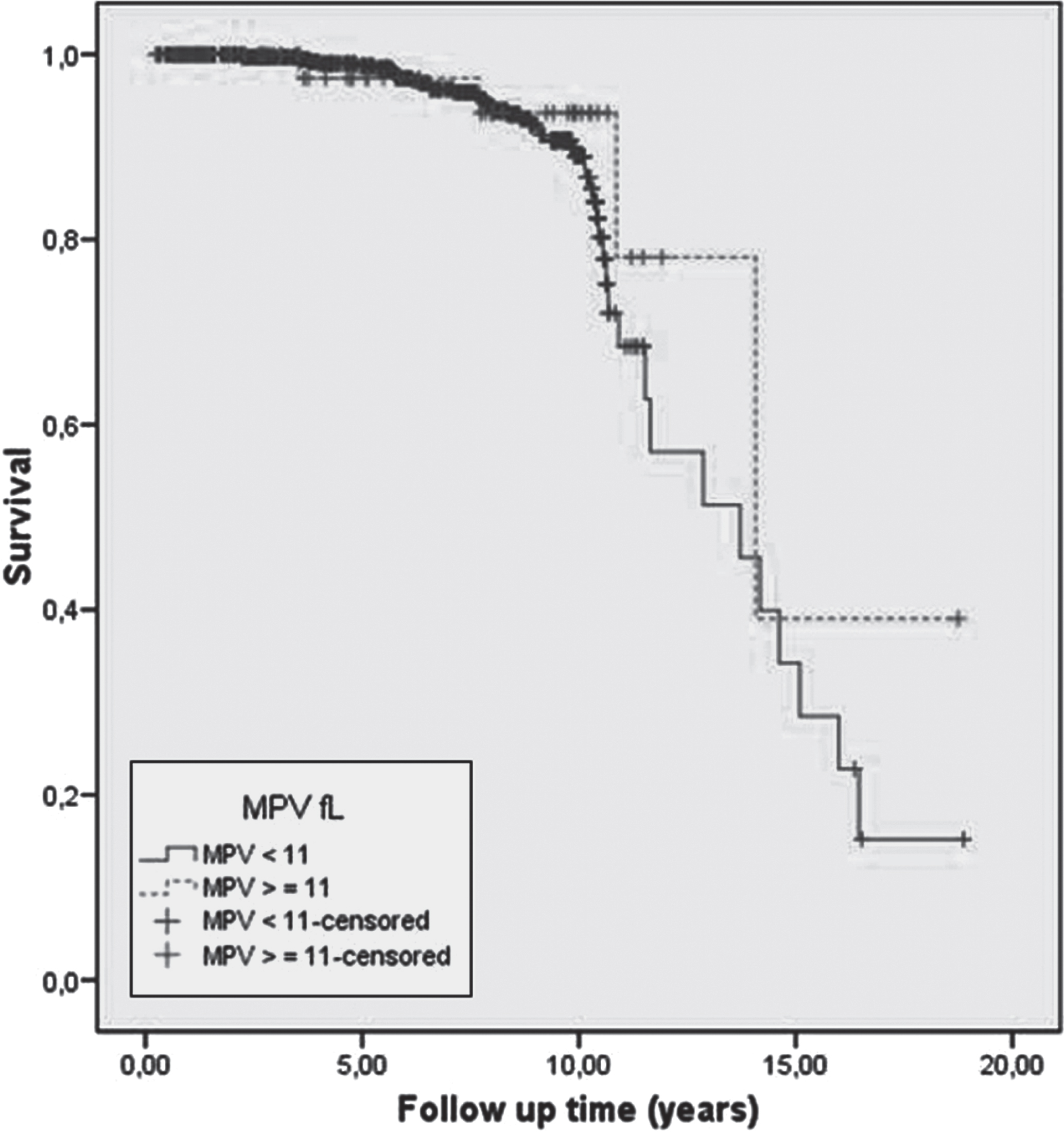
Kaplan-Meier survival curves in relation to Major Adverse Cardiovascular Event (MACE) and mean platelet volume (MPV) above and below 11 fL.
Thromboembolic events are a well-recognized source of morbidity and mortality in patients with CHD, with a prevalence of 10 to 100-fold higher than age matched controls [26]. Similar findings emerged from our study where the number of arterial thrombotic events among CHD patients, venous events were not included, was 8 times higher than in the control group. Additionally CHD patients had significantly more thrombocytopenia and a lower platelet count than patients in the control group. On the contrary, patients in the general population showed higher MPV levels than CHD patients what could be in relation to the greater percentage of smokers and dyslipidemic patients in the former [27, 28]. Nevertheless, neither the MPV 95th percentile nor the percentage of patients with a MPV level above 11 fL, 5% of the patients in the CHD and control groups, showed statistical significance between CHD and control patients.
The prevalence of thrombosis in CHD patients is influenced by factors involved in hemodynamic or coagulation alterations. Increased venous pressure, hepatic dysfunction, stasis of flow, ventricular dysfunction, atrial shunts, metal prostheses, Fontan circulation, or Eisenmenger syndrome are some of the factors that may contribute to an increased risk of clot formation [5, 29]. Likewise, reduced protein C, protein S, coagulation factors or platelet dysfunction may increase the thrombotic risk in CHD patients [30]. In this context, larger platelets which are metabolically and enzymatically more active [31] may also have greater prothombotic potential [32]. In fact, elevated MPV values have been associated with cardiovascular diseases and a poor outcome following acute coronary events or coronary interventions [3]. Moreover, some authors have reported an association between MPV and traditional CV risk factors, such as arterial hypertension, impaired fasting glucose, diabetes mellitus, hypercholesterolemia and obesity, suggesting a possible mechanism in increasing cardiovascular risk [33]. However, in our series, we did not find an association between MPV levels, cardiovascular risk factors or thrombotic events in CHD patients.
Despite some authors have found an association between raised MPV levels and an increased risk of thrombotic events in Eisenmenger patients [11] these findings, that cannot be extended to the whole of CHD patients, may be in relation to heart failure. In fact, as the authors state in their limitation section, they did not include parameters of risk stratification, such as NT-pro-BNP levels or ventricular function, both of which are affected in patients with Eisenmenger syndrome. This may have resulted in a bias of their results according to our findings since patients with NT-pro-BNP levels >125 pg/mL and ventricular dysfunction, although the latter without reaching statistical significance, presented higher MPV levels. Moreover, chronic heart failure may predispose by itself to platelets abnormalities and an increased thrombotic risk through increased catecholamine release, hemodynamic changes, vascular factors, nitric oxide, cytokines and co-morbidity situations [34]. In this regard, some authors have correlated MPV levels and heart failure [35, 36] while others [37] have reported that patients with severe heart failure are more likely to have platelet activation. Also other factors may affect platelet count and MPV values in CHD patients as seen in our series: on the one hand the number of platelets as it is inversely related to MPV values [38, 39] in an attempt to maintain haemostasis by preserving a constant platelet mass [40] and on the other hand female sex as in women platelet count and the total volume of platelets is higher than in men, which seems to reflect different hormonal profiles or a compensatory mechanism associated with menstrual blood loss [41].
In relation to inflammation it may predispose to changes in MPV values as platelets not only mediate haemostasis but also modulate inflammation via the communication with other platelets as well as endothelial cells and leucocytes [4]. In fact, MPV has emerged as a relatively reliable marker of inflammation in patients with various diseases [7, 42] with high MPV associated with low-grade inflammation. However we found no association between MPV levels and CRP or leukocytes concentrations in our CHD patients probably because they were stable patients seen in outpatient clinic. On the contrary, we found a lower percentage of lymphocytes among CHD patients with higher MPV values. This is especially important as a low relative lymphocyte count, in both chronic and hospitalized heart failure patients, has consistently shown worse prognosis independently of traditional prognostic indicators [43, 44]. Similarly, and as reported by others we did not identify any associations between MPV levels and thyroid function [45] or between increased MPV levels and antiplatelet therapy [46, 47].
With respect to atrial fibrillation and flutter both of them are associated with an increased risk of thromboembolic complications playing platelets also a critical and precipitating role in the occurrence of these arrhythmias. In this context, some authors have found that MPV and white blood cell count is independently associated with chronic non-valvular atrial fibrillation [48] while others have found that MPV levels is significantly greater in atrial fibrillation patients compared to those who remained in sinus rhythms [49]. As atrial arrhythmias and congestive heart failure are common conditions which predispose each other [50] it is understood that in our series atrial fibrillation and flutter present high MPV levels (>11 fL). On the contrary platelet count was significantly lower in patients with atrial fibrillation [49].
In conclusion, despite our awareness of the study’s limitations because of the low number of cardiovascular deaths and thrombotic events in a young CHD population we may conclude that high MPV levels are not associated with cardiac death or thrombotic events in CHD patients.