
Abstract
BACKGROUND:
The first method of choice for gallbladder alteration detection is the conventional ultrasound. Due to some imaging limitations, contrast-enhanced ultrasound (CEUS) has been widely used in the last years. CEUS is an additional modality that is able to depict microvessels flow and elucidate suspicious findings.
OBJECTIVE:
The aim of this retrospective mono-center analysis study is to evaluate the performance of CEUS in gallbladder diseases and compare it to cross-sectional imaging modalities and histopathological results as gold standard.
METHODS:
The retrospective study analysed 37 patients with gallbladder diseases between 2009 and 2017. All patients underwent CEUS examinations and additional cross-sectional imaging was also performed: CT imaging on 24 (64.9%) patients, MRI imaging on 18 (48.6%) patients, CT and MRI imaging on (28.7%). CEUS images were performed and interpreted by a single physician.
RESULTS:
CEUS imaging results of the gallbladder showed a sensitivity and specificity of 100%, a positive predictive value (PPV) of 100% and a negative predictive value (NPV) of 100%. CT imaging of the gallbladder showed a sensitivity of 100%, specificity of 75%, PPV of 100%, and NPV of 95%. MR imaging of the gallbladder showed a sensitivity of 100%, specificity of 93%, PPV of 75%, and NPV of 100%.
CONCLUSION:
Ultrasound imaging plays an essential role in the evaluation of gallbladder disease. Due to additional features of contrast-enhanced ultrasound, it is possible to differentiate gallbladder pathologic alterations by depicting its micro and macrocirculation and display important malignant features that recommends prompt management. Patients with contraindications to other cross-sectional imaging modalities benefit from this safe technique.
Introduction
The gallbladder is a pear-shaped hollow organ that can be affected by several disorders causing specific or non-specific symptoms. The early detection of some alterations such as gallbladder carcinoma enables the improvement of a poor diagnosis [1]. Radiologic imaging not only detects pathologic alterations, but also determines its nature. The first tool of choice is the real-time ultrasonography due to its excellent temporal and spatial resolution, cost-effectiveness, easy manipulation and no radiation.
Due to the insufficiency of conventional ultrasound in some cases, contrast-enhanced ultrasound (CEUS) has been widely used in the last years. CEUS is a new modality that has already been established for the assessment of suspicious lesions in organs such as liver [2, 3], pancreas [4] and kidney [5, 6]. CEUS great advantage is that the additional contrast agent applied allows the depiction of small vessels and their blood flow. Moreover, it enables the visualization of vascularization pattern during 2 phases: arterial (10–20 seconds postinjection); and late phase (31–180 seconds after contrast agent injection) [2, 7–10]. As the gallbladder is perfused by the cystic artery only, its vascularization pattern differs from the liver perfusion.
Furthermore, it is a safe tool if compared to other imaging methods because the contrast agent administered has no cardiac or renal toxicity and can be used in patients with renal insufficiency and dysfunction of the thyroid glands [11, 12]. Additionally, severe allergic responses are very rare: 1 in 10.000 cases [12, 13].
However, cross-sectional imaging modalities such as magnetic resonance imaging (MRI) and computed tomography (CT) are likewise able to evaluate suspicious gallbladder alterations after ultrasound, displaying differential diagnosis such as xanthogranulomatous cholecystitis, inflammation, adenomyomatosis, hepatobiliary malignancies and metastatic disease. Unfortunately, cross-sectional imaging modalities use specific contrast agent that may be toxic for the kidney and cannot be used in patients with renal failure. Besides the radiation issue in CT imaging.
The aim of this retrospective mono-center analysis study is to evaluate the performance of CEUS in gallbladder diseases comparing to the cross-sectional imaging modalities and histopathological results.
Materials and methods
This study was approved by the local institutional ethical committee of the institutional review board. All authors respected the ethical guidelines for publication in Clinical Hemorheology and Microcirculation [14]. All exams and its potential causes were explained to the patients and patients gave their oral consent and signed a written informed consent prior each examination (CEUS, MRI and CT). All study documents supported the ethical principles expressed in the Declaration of Helsinki 2002.
The retrospective study analysed 37 patients with gallbladder diseases between 2009 and 2017. All patients underwent CEUS examinations and had additional histopathological results to prove the diagnose. Additional cross-sectional imaging was also performed: CT imaging on 24 (64.9%) patients, MRI imaging on 18 (48.6%) patients, CT and MRI imaging on (28.7%). Moreover, 3 patients had CEUS, MRI and CT as well as additional histopathological results. Mean age of patients was 62 years old, ranging in age from 27 to 90 years, 37.8% were female and 62.2 % were male.
CT and MRI imaging were performed with standard scanning protocols and scanners used at the time of the examination. Histopathological analysis of a sample was achieved according to the valid methods, protocols and categorizations at the time of the examination.
All CEUS investigations used a high-end ultrasound system (Philips Ultrasound Siemens Acuson Sequoia, Siemens S2000 and EPIQ 7) with the latest specific protocols. The abdominal transducers used had a frequency ranged from 1.0 to 9.0 MHz, C4-1 and C6-1 HD for Siemens system and C9-2 for Philips system. A low mechanical index (always <0.2) was configured for each system in order to circumvent early microbubble-destruction. All CEUS studies were executed and interpreted by a single experienced physician with more than fifteen years of experience in CEUS.
All patients underwent fasting from 6–8 hours prior examination. At first, patient underwent a greyscale US investigation of the gallbladder and the adjacent liver. Then, a second-generation blood pool agent used in Europe (SonoVue®, Bracco, Milan, Italy) was applied; a dose of 1.5 to 2.4 mL SonoVue® was administered as a bolus injection by using a 20 or 22-gauge cannula positioned in the antecubital vein, a flush-injection of 5 to 10 ml of 0.9% NaCl followed the bolus. The contrast media applied contains phospholipid-stabilized shell microbubbles filled with sulfur hexafluoride gas. In the majority of cases, a single dose of contrast agent was sufficient. After contrast agent administration, cine loops of the examination were archived in the picture archiving and communication system (PACS) of our local institution. Mean study time ranged between 3–5 minutes. No severe adverse reaction was observed.
CEUS, CT, MRI images and histopathological results archived of all patients were retrieved from the data archiving system of our institution and CEUS performance was retrospectively analysed by testing specificity, sensitivity, positive predictive value (PPV) and negative predictive value (NPV).
Results
CEUS imaging results showed a sensitivity and specificity of 100%, a positive predictive value of 100% and a negative predictive value of 100%. CT imaging showed a sensitivity of 100% and specificity of 75%, a positive predictive value of 100% and a negative predictive value of 95%. MR imaging showed a sensitivity of 100% and specificity of 93%, a positive predictive value of 75% and a negative predictive value of 100%.
Out of 37 patients with gallbladder alterations, CEUS demonstrated three cases with a suspicious malignant gallbladder alteration. In two of those, the malignant appearance of the gallbladder was also presented in CT and histopathologically confirmed as adenocarcinoma (Fig. 1). In one case, the suspicious malignant gallbladder alteration demonstrated by CEUS was elucidated in the CT, MRI and in the pathologic results as an infiltration of a malignant liver mass.
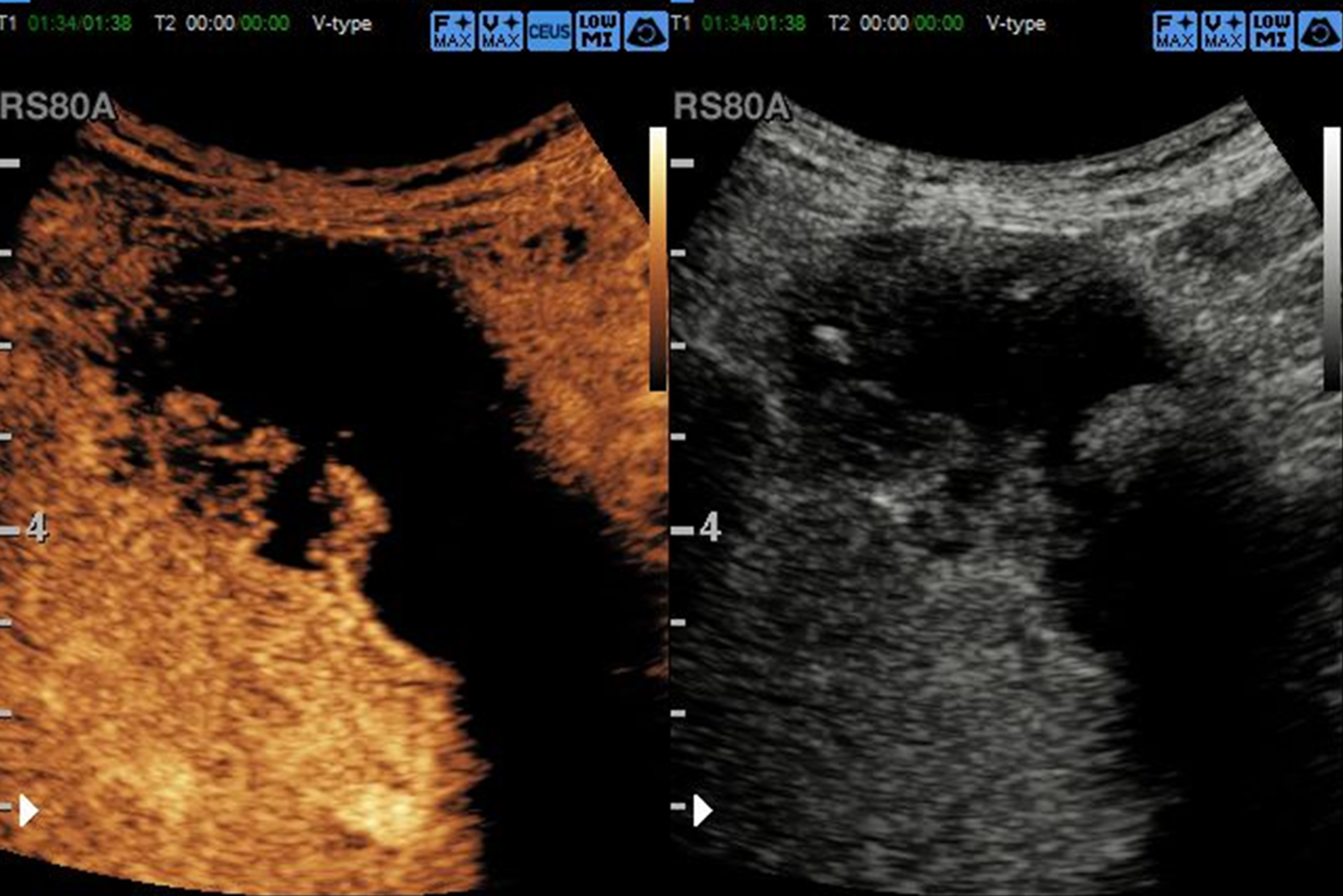
Gallbladder carcinoma in a 91-year old patient. CEUS shows an arterial focal hyperenhancement of the gallbladder wall and of a suspicious mass with irregularly shaped borders adjacent to the wall. In the venous phase of CEUS the mass displays a pathological wash-out.
Moreover, gallbladder polyposis was depicted by CEUS and confirmed by the histopathological findings in two patients. Adenomyomatosis pattern was depicted by CEUS and confirmed in CT and MRI as well as in the pathology in 2 other cases. Additionally, cholecystitis pattern was displayed by CEUS, demonstrated in the cross-sectional modality and was pathologically confirmed in 10 cases (Figs. 2– 6).
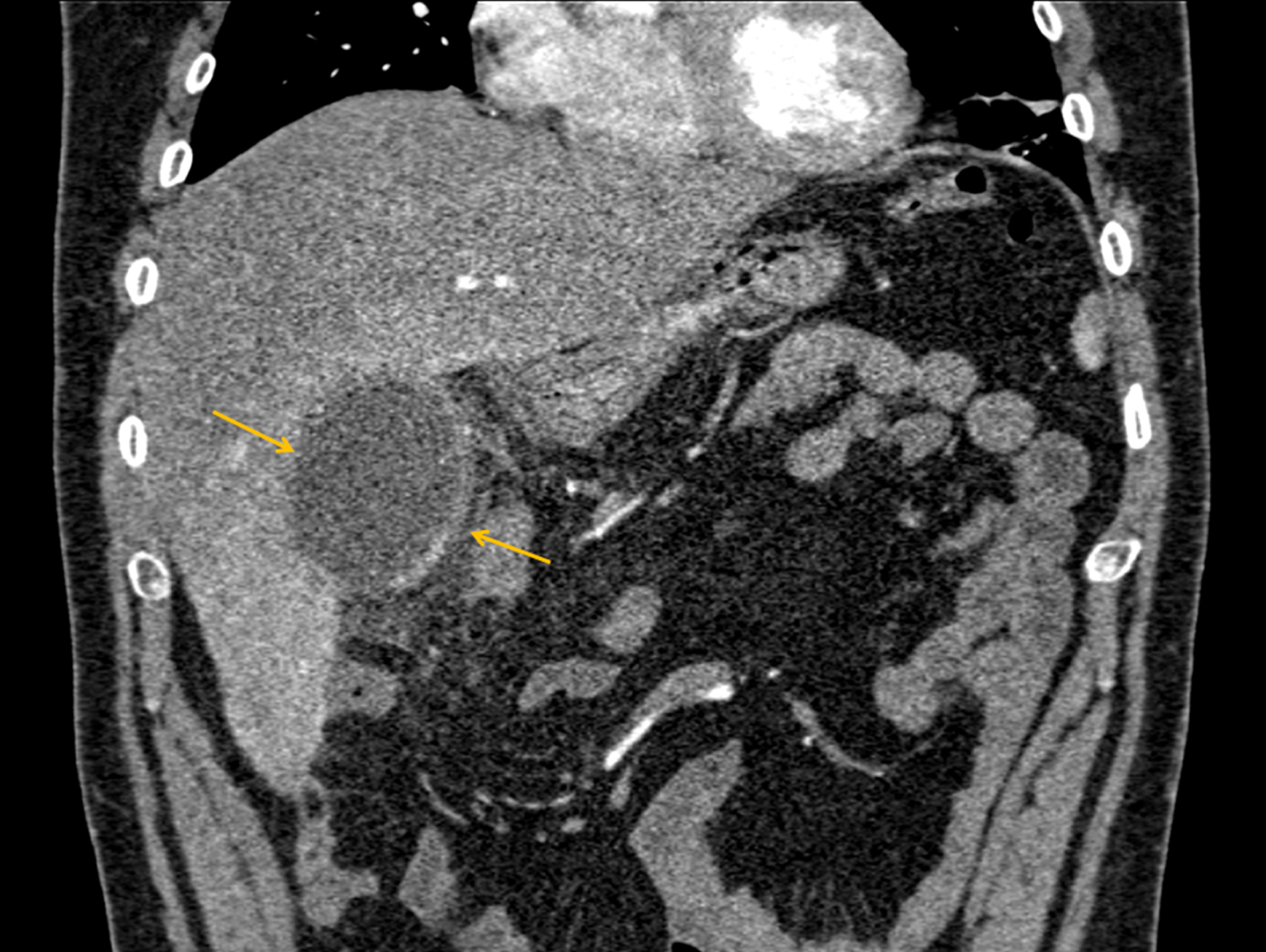
Coronal CT-reconstruction of a patient with abdominal pain showing a thickened gallbladder wall (yellow arrows).

Same patient as in Fig. 2. Axial CT-reconstruction showing a thickened wall of the gallbladder suggesting cholecystitis (yellow arrows).
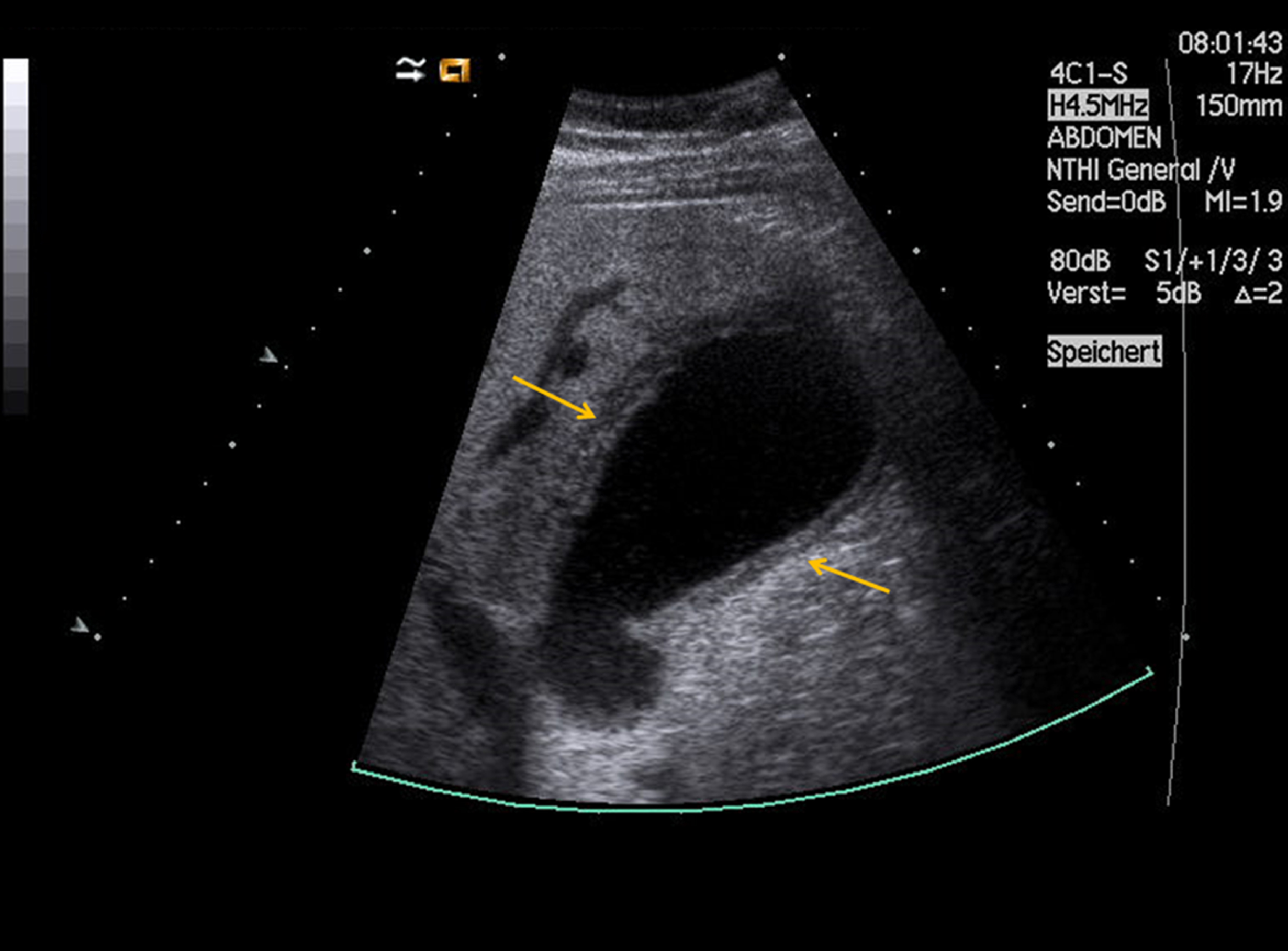
Native B-mode ultrasound of the same patient as in Figs. 2– 3. The native ultrasound shows a gallbladder with a three-layered thickened wall (yellow arrows).
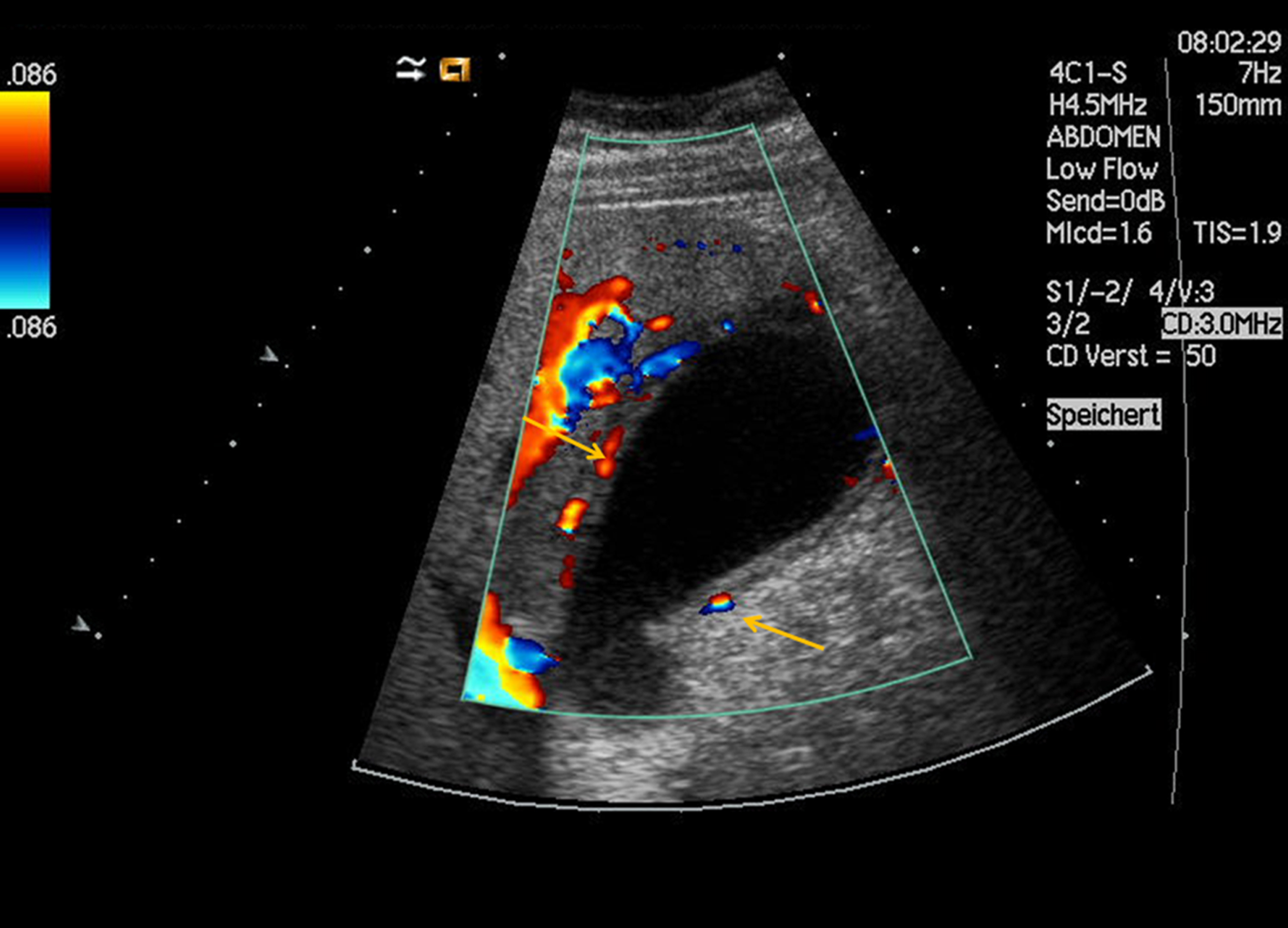
Same patient as in Figs. 2–4. Color Doppler shows the reactive inflammatory hypervascularization of the gallbladder wall (yellow arrows).
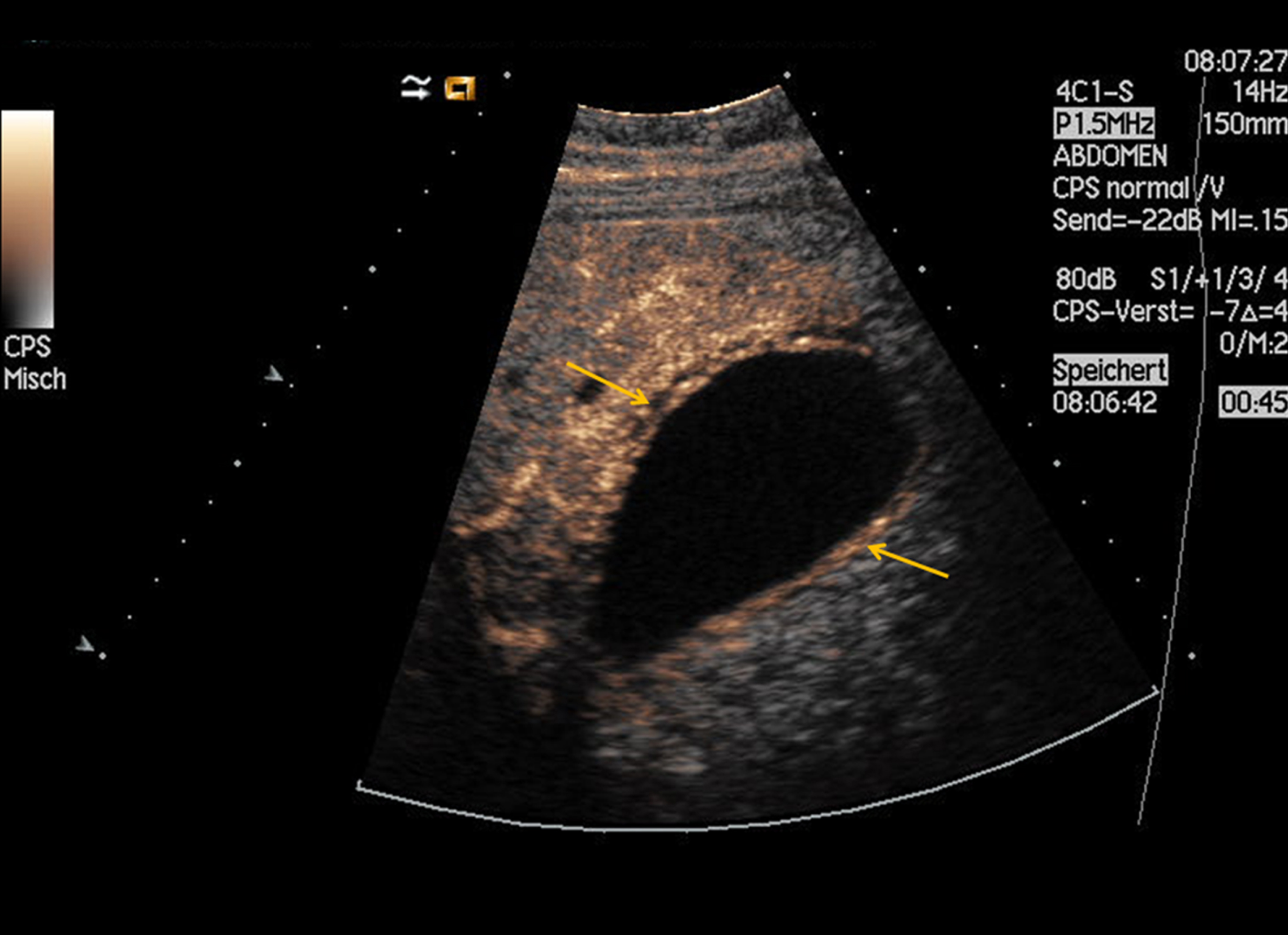
Same patient as in Figs. 2–5. CEUS can safely rule out malignancy by demonstrating the homogenous inflammatory vascularization pattern due to the cholecystitis (yellow arrows) with no signs of malignancy. The diagnosis was histopathologically confirmed after cholecystectomy.
Gallbladder carcinoma is the fifth most common malignant alteration of the gastrointestinal tract [15]. It affects older patients (>50–60 years of age), especially women (F:M = 4:1) [15]. The most usual carcinoma alteration is the adenocarcinoma (90%) [15]. As gallbladder carcinomas are normally asymptomatic until they are in an advanced stage, its early detection is crucial to avoid a potential poor diagnosis [1]. The accidental detection of risk factors such as chronic cholecystitis, gallstones, familial adenomatous polyposis syndrome, inflammatory bowel disease (IBD), porcelain gallbladder and gallbladder polyps (>1 cm that are sessile and solitary) enables the early therapy assessment [1, 15–17].
Radiologic imaging has an important role in the detection of gallbladder alterations. The conventional ultrasound, MRI and CT are great modalities that are able to demonstrate the anatomy and morphological modifications of the gallbladder. However, the greyscale ultrasound is insufficient to distinguish a focal mass from a tumor, sludge or polyp; has limitations demonstrating malignant features such as gallbladder wall destruction or infiltration [16–19] and Color Doppler is not able to depict deeply located vessels. Moreover, other cross-sectional imaging methods such as CT and MRI cannot be performed in all patients because of renal failure, thyroid dysfunction, pacemaker and etc. [10, 20].
In order to overcome these limitations, CEUS has been used in the clinical routine as a suitable alternative method to evaluate pathological alteration of the gallbladder. The application of a contrast agent in real-time imaging has been recently increasingly recognized though some controversial statement in the literature [21–23].
The contrast media applied demonstrates the vascularization of a marked lesion presenting an organ enhancement in several phases (arterial and late parenchymal), increasing the diagnostic accuracy.
In this study, CEUS presented in 3 patients features of malignancy such as an asymmetrical, tortuous arterial enhancement that were also showed in other studies [7, 25]. Nevertheless, arterial contrast of a mass followed by its early washout is not a specific criterion for malignancy [19, 22–25]. The sum of other characteristics such as disrupted gallbladder wall, tortuous vascularity and patient age have also to be considered [18]. These modifications could also be seen in the cross-sectional images.
Histopathological results reported that 2 from 3 patients with the alterations cited above had an adenocarcinoma of the gallbladder with following pathological findings: glands lined by cuboidal or columnar cells that can be well, moderately, or poorly differentiated, depending on the degree of the gland configuration [26]. Moreover, others histologic variants such as papillary, intestinal, mucinous, signet-ring cell, and clear cell can also be recognized [26].
In the other patient that a malignant alteration was depicted by CEUS, an infiltration of a malignant hepatic mass was confirmed in the pathology. CEUS displayed a tortuous-type vascularity, disrupted gallbladder wall and arterial contrast [22–25]. Additional MRI and CT demonstrated the same modifications in the gallbladder and an additional hepatic mass. Pathological findings confirmed a hepatic mass with gallbladder infiltration.
Adenomyomatosis was also detected by CEUS and confirmed in CT and in the histopathological findings in 2 patients. However, MRI was only able to depict one of two adenomyomatosis. Adenomyomatosis is showed by CEUS as a focal, segmental, or diffuse benign hyperplasia of the gallbladder wall. The arterial phase displayed a “moth-eaten” contrast of the gallbladder wall. Sometimes, the gallbladder wall enhances homogeneously in an “hourglass” form [27, 28].
Other gallbladder alteration such as cholecystitis was also demonstrated by CEUS and validated in the pathology, MRI and/or CT in 10 patients. A gallbladder wall thickening, and edema was showed in the conventional ultrasound, additional CEUS imaging displayed a fast, homogeneous, and intense contrast of this thickened wall implying a gallbladder inflammation.
The last gallbladder modification depicted in this study was gallbladder polyp, which was depicted by CEUS in two cases as sessile projections of the wall into the lumen [29]. Histopathological results confirmed the diagnosis. Gallbladder polyps are normally incidentally findings that can be a potential risk factor for carcinomas [30]. Because of that they have a specific therapy management according to the radiologic findings: no further follow-up, follow-up and resectable (cholecystectomy).
Finally, the gallbladder alterations depicted by CEUS were all confirmed in other imaging modalities or in the histopathological findings showing its promising role in the future.
Conclusion
This study showed that CEUS, when compared to cross-sectional imaging modalities and histopathological findings, has a high sensitivity, specificity and PPV being feasible to differentiate gallbladder pathologic alterations by depicting its micro and macrocirculation, determine pathological modifications and display important malignant features that recommends prompt management.