
Abstract
OBJECTIVES:
To identify the associated factors for malignancy in partially cystic thyroid nodules (PCTNs) on ultrasound (US).
MATERIALS AND METHODS:
This is a retrospective study. 338 PCTNs confirmed by surgery was included in this study. The US features of the nodules were reviewed and their significance in differential diagnosis was analyzed.
RESULTS:
In the 338 PCTNs, 50 were malignant and 288 were benign. Univariate analyses revealed that a taller-than-wide shape and spiculated or microlobulated margin were significantly associated with malignancy while the spongy form, an ovoid to round shape and smooth margin were significantly associated with benign nature. In terms of the internal solid portion of the nodule, eccentric configuration, non-smooth margin, hypoechogenicity, and microcalcification were more frequently demonstrated in malignant nodules than in benign ones. In the multivariate logistic regression analysis, a taller than wide shape (OR: 13.357; 95% CIs: 3.457–28.797) was revealed to be the strongest independent predictor for malignancy, followed by microcalcification (OR: 11.578; 95% CIs: 3.142–29.563), spiculated or microlobulated margin (OR: 6.331; 95% CIs: 1.425–9.457), eccentric configuration (OR: 5.456; 95% CIs: 1.358–8.774), non-smooth rim of the internal solid portion (OR: 4.897; 95% CIs: 0.754–7.021), and hypoechogenicity of the internal solid portion (OR: 4.651; 95% CIs: 0.712–8.245).
CONCLUSIONS:
Understanding the ultrasound characteristics of malignant PCTNs is important to make a precise diagnosis of thyroid nodules.
Introduction
Partially cystic thyroid nodules are nodules that have both solid and cystic components, and they account for about 15–53.8% of all sonographically detected thyroid nodules [1, 2]. According to the past studies, most of the thyroid nodules were regarded as benign when cystic change occurred in the interior of the nodules [3]. However, thyroid carcinomas can also show a cystic change, and thus the PCTNs are often underestimated. Recently reports suggest the percentage of malignancy in PCTNs varies from about 2% to 18% [1, 5] and there is little information regarding US features associated with malignancy. The purpose of this study, therefore, was to search for US features predictive of malignancy as they relate to PCTNs.
Materials and methods
Patients
We reviewed the surgical thyroid excision data of Shanghai Ninth People’s Hospital from July 2012 to January 2017, and 338 PCTNs in 322 patients were enrolled by conforming to the following eligibility criteria: (1) Nodules should have both solid and cystic components; (2) Images were complete, and clinical information include age, gender, pathology result was available in the institute medical record system; (3) No treatment history. Nodules complied with any of the following cases were excluded from the study: (1) Accepted thyroid hormone therapy; (2) Nodules with incomplete ultrasound images, clinical information or pathological results. 50 nodules (33 women, 17 men; age range, 21-77 years; mean age, 54 ± 15.5 years) were confirmed as malignantwhile 288 nodules (183 women, 74 men; age range, 22-78 years; mean age, 50 ± 16.7 years) were confirmed as benign by surgery. The histological diagnosis of the malignant PCTNs was as follows: papillary thyroid carcinoma (n = 48), medullary thyroid carcinoma (n = 1) and follicular thyroid adenocarcinoma (n = 1). And the histological diagnosis of the benign PCTNs was as belows: nodular hyperplasia (n = 178), cystic degeneration of thyroid adenoma (n = 56), and cystic degeneration of nodular goiter (n = 49), thyroid adenoma with chronic inflammation (n = 5).
Thyroid US examination
All patients had been initially assessed by high-resolution grey-scale US and color Doppler using a 5–12 MHz linear array transducer (Philips iU22, Philips Healthcare, Bothell, Washington), performed by radiologists with 10–15 years’ experience. With optimized machine setting and sufficient gel applied, high quality images were acquired in patients’ supine position, including grey scale images and color Doppler images. During color Doppler examination, a low value of pulse repetition frequency (700 Hz) was used to evaluate the vascularity of PCTNs. US images on both transverse and longitudinal cross sections of each target nodule were obtained and stored in the internal hard disk for subsequent analyses.
US evaluation
The features of all the PCTNs were retrospectively evaluated by two board-certified radiologists in consensus, both of whom have more than 10 years of experience in thyroid US. The images were placed on a picture archiving and communication system workstation (Blue Technology, Shanghai, China), and were presented at random. Each nodule was evaluated for the following US findings of entire nodule: 1) composition (solid portion ≥50% vs. solid portion <50% vs. spongy form) (Figs. 1–3, the three cases of PCTNs were confirmed by surgery as papillary thyroid carcinoma, nodular goiter with cystic degeneration and cystic degeneration of thyroid adenoma, respectively), 2) shape (ovoid to round vs. taller-than-wide vs. irregular), 3) margin (smooth vs. spiculated or microlobulated vs. ill-defined), 4) nodule vascularity (peripheral vs. intranodular vs. avascular). US examination of internal solid portion included: 1) configuration (eccentric vs. non eccentric) (Fig. 4, confirmed by surgery as papillary thyroid carcinoma), 2) rim (smooth vs. non-smooth), 3) echogenicity (markedly hypoechoic vs. hypoechoic vs. isoechoic vs. hyperechoic) and 4) calcification (microcalcifications vs. macrocalcifications vs. mixed calcifications vs. none) of the solid portion of the nodules were also evaluated. Microcalcifications had tiny, punctuated hyperechoic foci ≤1 mm in diameter, either with or without acoustic shadows. Macrocalcifications exhibited hyperechoic foci >1 mm in diameter.
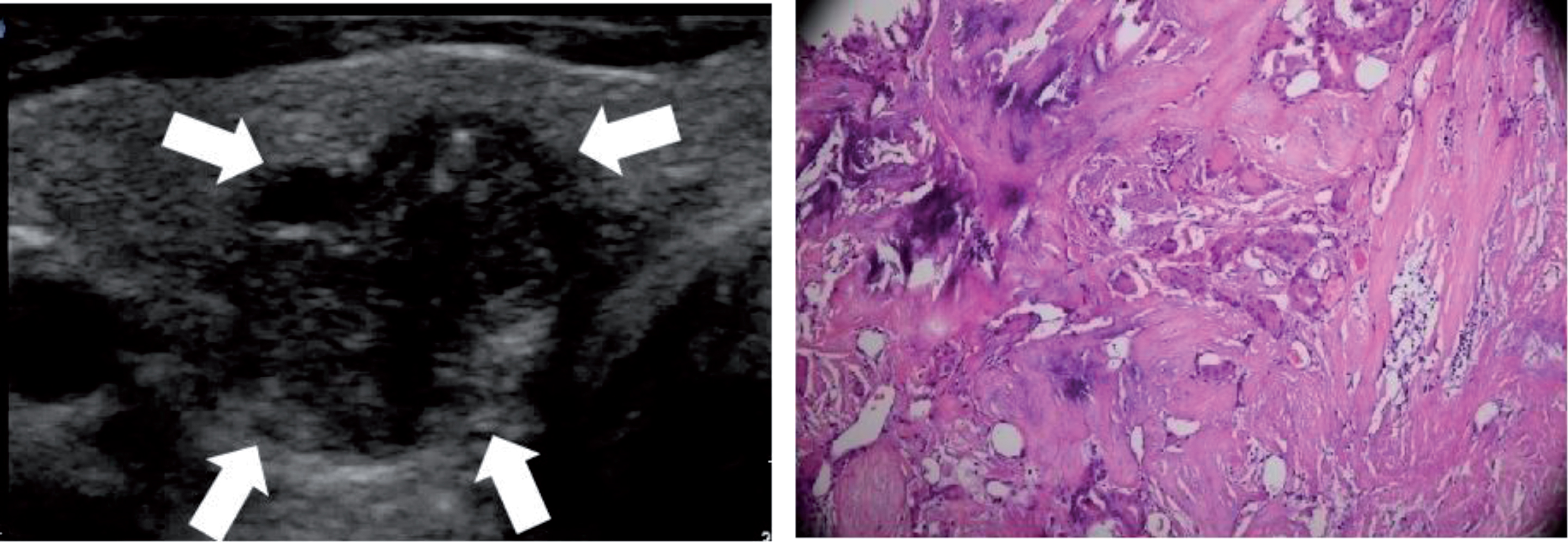
Transverse ultrasound image of papillary thyroid carcinoma in 29-year-old woman shows predominantly solid nodule. Entire nodule has a taller than wide shape and non-smooth margin. Internal solid position contains punctuated echogenic foci suggesting microcalcifications.
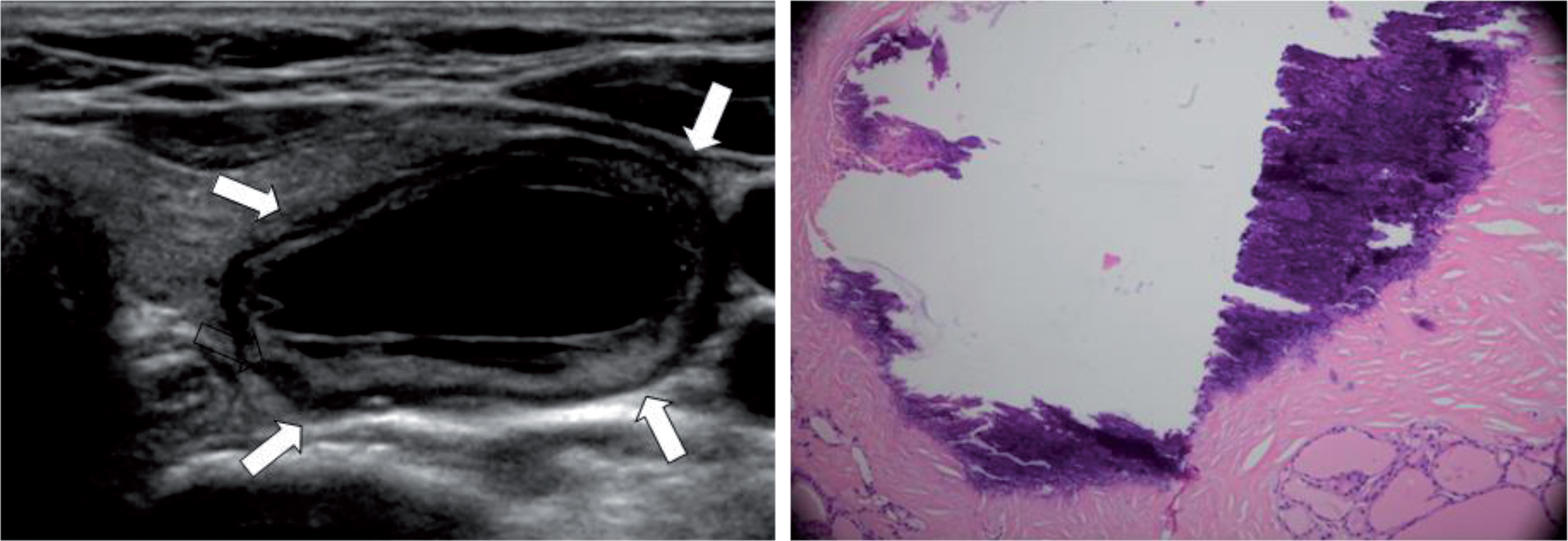
Example of PCTN with a solid portion <50%. Transverse US images show partially cystic nodule with isoechoic internal solid portion in 38-year-old woman. This lesion was surgically confirmed as nodular goiter with cystic degeneration.
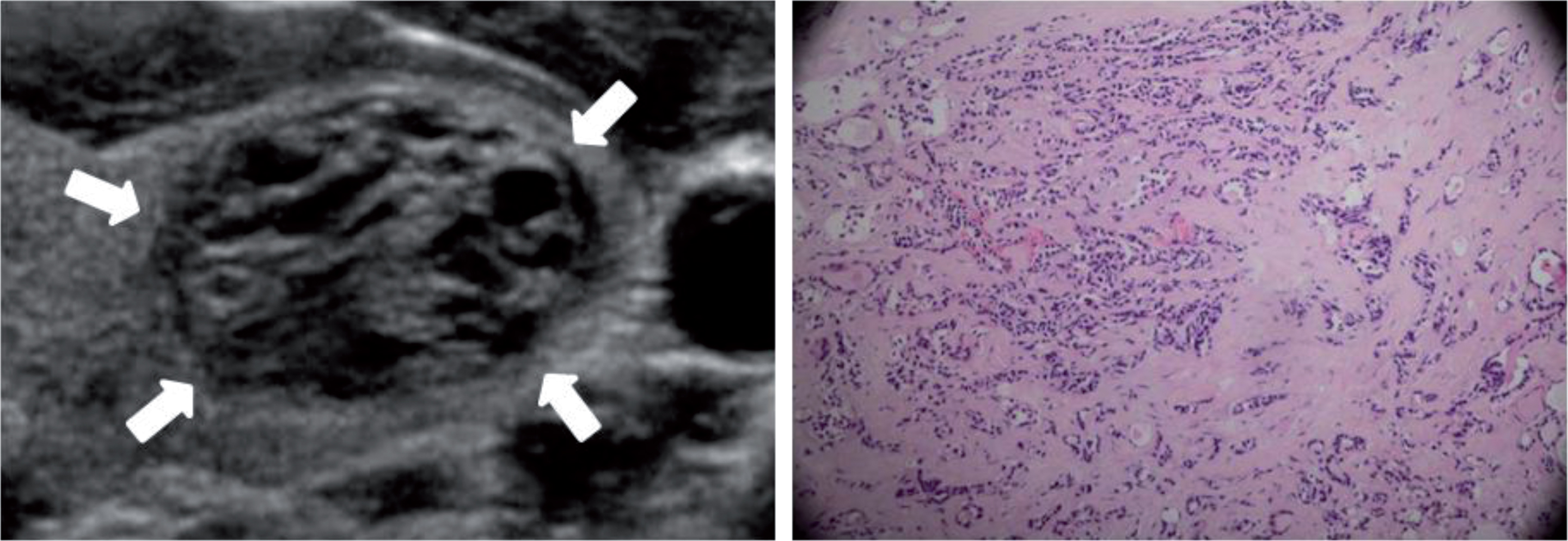
Example of PCTN with spongy form. Transverse US image shows a well-circumscribed, oval nodule with multiple microcystic components. This lesion was surgically confirmed as cystic degeneration of thyroid adenoma.
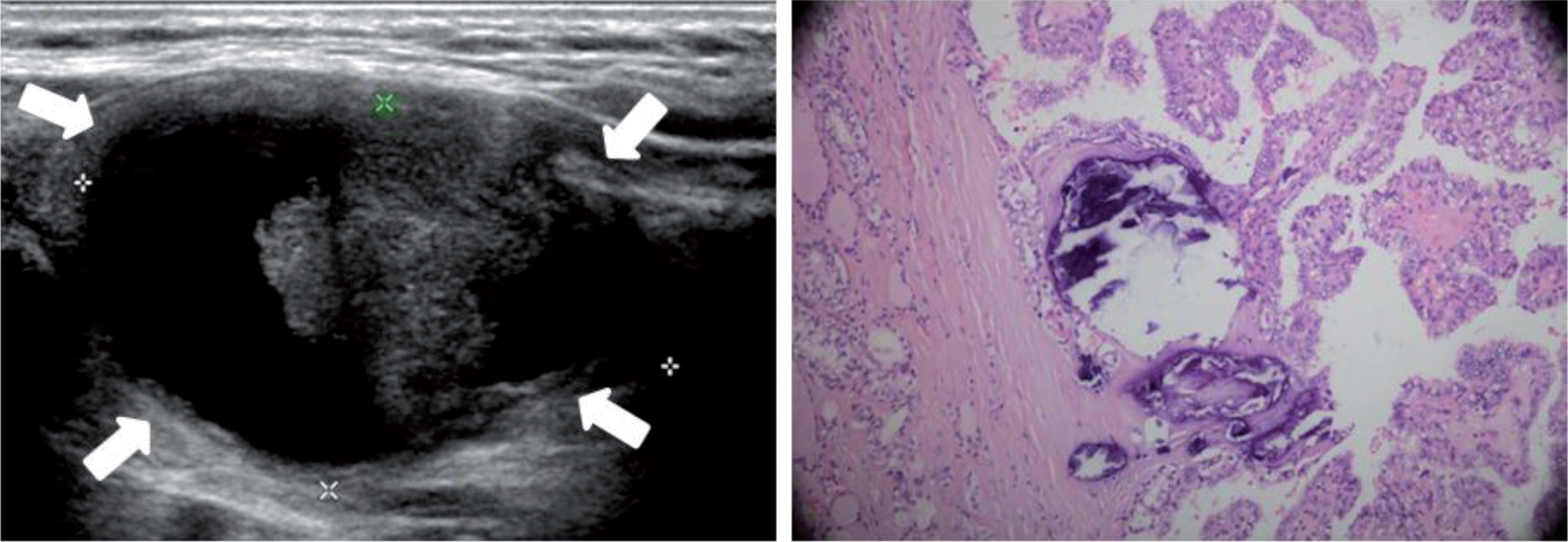
Longitudinal ultrasound image of papillary thyroid carcinoma in 46-year-old woman shows predominantly cystic nodule. Entire nodule has smooth margin while non-smooth of the internal protruding eccentric solid position.
The statistical analyses of current study were addressed by SPSS software package(Version 19.0; SPSS Inc, Chicago, IL). Chi-square test or Fisher’s exact test was applied in categorical variables, while independent t test was applied in comparison of continuous variables. The malignancy risks for independent variables were calculated in univariate and multivariate analyses. Binary logistic regression analysis model testing was performed using the Forward: Likelihood Ratio (LR) approach for the simultaneous effects of multiple predictors. Candidate variables included those from the parameters that showed statistical significance in the univariate analysis. The corresponding odds ratio (OR) and the 95% confidence interval (95% CI) were reported for all categorical variables. Model performance was evaluated via the Hosmer-Lemeshow goodness of fit statistics. A Hosmer-Lemeshow P value greater than 0.05 indicated a good model fit. All reported P values were two-sided and considered statistically significant if they were less than 0.05.
Results
322 patients with 338 PCTNs included 50 malignant nodules and 288 benign ones. The prevalence of malignancy was 50 of 338 (14.8%). The percentage of malignant PCTNs that occurred in male patients (17.2%, 11/64) was higher than the percentage of malignant nodules that occurred in female patients (14.2%, 39/274). The average age of patients with malignant thyroid nodules and benign ones was 54.1 years and 50.7 years respectively. The mean malignant thyroid nodule size was 23.5±9.1 mm (range, 8.4–45.3 mm) while was 25.1±10.6 mm (range, 6.8–52.3 mm) in benign ones.
Univariate analyses of US features of the PCTNs were summarized in Table 1. A taller than wide shape was significantly associated with malignancy. The prevalence of malignancy was significantly higher in the nodules with spiculated or microlobulated margin. In addition, spongiform internal content was significantly associated with benignity. No significant difference was found between nodules with a solid portion ≥50% and with a solid portion <50%. Besides, there is also no significant difference between nodules with three different vascular patterns we divided. In terms of the internal solid portion of the nodule, an eccentric solid position, non-smooth rim, hypoechoic and microcalcifications were significantly associated with malignancy while non-eccentric solid position, smooth rim, isoechoic and none calcification with benignity. In addition, macrocalcifications (p = 0.072) and mixed calcifications (p = 0.059) were more frequently demonstrated in benign PCTNs, although the p value was not statistically significant.
US features of partially cystic thyroid nodules
US features of partially cystic thyroid nodules
Patients were regrouped, and the inherent correlation between the two suspicious ultrasound features—the solid portion ≥50% and eccentric solid portion of the nodule was revealed in Table 2. In the solid portion ≥50% group, an eccentric solid portion showed a statistically significant association with a malignant PCTN. Conversely, no significant difference was found in the solid portion <50% group.
Stratified analysis between composition and eccentric solid position or not
All variables from Table 1 with p values less than 0.10 were considered as candidate factors in a binary logistic regression analysis model. The shape and margin of the entire thyroid nodule, the configuration, rim and echogenicity of the internal solid portion, and calcification were identified as candidate factors. In the multivariate logistic regression analysis, a taller than wide shape (OR: 13.357; 95% CIs: 3.457–28.797) was revealed to be the strongest independent predictor for malignancy, followed by microcalcification (OR: 11.578; 95% CIs: 3.142–29.563), spiculated or microlobulated margin (OR: 6.331; 95% CIs: 1.425–9.457), eccentric configuration (OR: 5.456; 95% CIs: 1.358–8.774), non-smooth rim of the internal solid portion (OR: 4.897; 95% CIs: 0.754–7.021), and hypoechogenicity of the internal solid portion (OR:4.651; 95% CIs: 0.712–8.245) (Table 3).
Result of multivariate logistic regression analysis for tlie characteristics of partially cystic thyroid nodules
β, regression coefficient; SE, standard error; OR, odds ratio; CIs, Confidence intervals.
The diagnostic index of malignant US features of PCTNs was summarized in Table 4. A taller than wide shape showed a high specificity and positive predictive value (PPV) (both was 100%), whereas the sensitivity was poor (24.0%). Microcalcification showed a high specificity and PPV (99.0% and 91.7%, respectively) whereas the sensitivity was relatively poor (66.0%) which was significantly higher than that of a taller than wide shape showed. In addition, microcalcification reached a high diagnostic accuracy (94.1%), followed by non-smooth rim (92.6%), eccentric configuration (89.6%), taller than wide shape (88.8%), spiculated or microlobulated margin (87.3%) and hypoechogenicity (71.0%).
The diagnostic performance of US features for malignancy prediction
PPV, positive predictive value; NPV, negative predictive value.
PCTNs are common findings in thyroid imaging and most of them are regarded as benign as the past studies suggest that the cystic change in the nodules is the result of a degenerative process, arising from underlying benign lesions, such as nodular hyperplasia. However, recent reports revealed that the percentage of malignancy of PCTNs was gradually increased. The risk of malignancy in PCTNs has variably been reported from approximately 2% to 18%. In a review of 927 consecutive aspirations, García-Pascual et al. reported an 11.1% (4/36) malignancy rate among PCTNs with nondiagnostic fine-needle aspiration cytology (FNAC).Patients with echographic PCTNs and nondiagnostic FNAC who underwent surgery were included in that study [6]. In a study of 119 PCTNs which underwent US-FNA biopsy and subsequently thyroidectomy, Bellantone observed carcinoma in 21 patients (17.6%) [2]. However, the malignancy rate may be affected by false positive and negative results in the aforementioned studies. In our study, the PCTNs with FNAC results were excluded and a 14.8% (50/338) malignancy rate was revealed which was significantly higher than a total 5% malignancy rate in thyroid nodules reported in several past studies. In addition, the percentage of malignant PCTNs that occurred in male patients (17.2%, 11/64) was higher than the percentage of malignant nodules that occurred in female patients (14.2%, 39/274).
There were few reports which compared the US findings between malignant and benign PCTNs. This retrospective study was notable for analyzing the US findings of both the entire nodule and its internal solid portion so as to seek for the difference between the malignant and benign PCTNs. The results suggested that a taller-than-wide shape and spiculated or microlobulated margin were significantly associated with malignancy while an ovoid to round shape, smooth margin were significantly associated with benign nature. In terms of internal solid portion of the nodule, eccentric configuration, non-smooth margin, hypoechogenicity and microcalcification were more frequently demonstrated in malignant PCTNs than benign ones. These findings do not differ greatly from the previously suggested US criteria [7], indicating those criteria that are applicable to PCTNs. However, the solid portion ≥50% was not significantly associated with malignant nature in our study while it was in another two reports [8, 9]. In other words, the proportion of solid components of PCTNs cannot predict a malignancy. Thus, radiologists should not overlook predominantly cystic nodules. Interestingly, when patients were regrouped as showed in Tab 2, we found that an eccentric solid portion showed a statistically significant association with a malignant PCTN in the solid portion ≥50% group. Conversely, no significant difference was found in the solid portion <50% group. Thus, we come to the conclusion that only in the solid portion ≥50% nodules is eccentric positioning of the solid component significantly associated with malignancy.
Compared with two recent studies [10, 11] regarding PCTNs, we confirmed that the eccentric configuration and microcalcifications of internal solid portion in PCTNs were significantly more frequent in malignant thyroid nodules. That is to say, malignant PCTNs are more likely to be an intracystic mass, protruding from the wall than the diffuse lesion, which is circumferentially located within the cystic wall that would result in a concentric configuration.
US diagnosis of microcalcifications in thyroid gland has been controversial and the conventional two-dimensional ultrasonic image exist artifacts which are inevitable. One notable difference in our study is that all the calcifications in the PCTNs were confirmed by pathology. In the present study, the presence of microcalcifications inside the solid components of PCTNs was associated with a high prevalence of malignancy. 33 of 36 PCTNs demonstrated with microcalcifications were confirmed as papillary thyroid carcinoma in our study. In addition, in this study macrocalcifications and mixed calcifications tended to be more frequently demonstrated in benign PCTNs, although no significant difference was reached.
It is worth mentioning that Color Doppler US has been evaluated as a diagnostic tool for predicting malignant PCTNs in this study. The results of relevant studies are mixed, with some reporting that Doppler US is helpful [12, 13] and others reporting that Doppler US did not improve diagnostic accuracy [14]. In our study, no significant difference was found between nodules with three different vascular patterns we divided.
Little related multivariate logistic regression analysis was reported to predict the significance of multiple ultrasonographic features in the differential diagnosis of PCTNs. In our study, the logistic regression model was developed to assess malignancy prediction of multiple ultrasonographic variables which has higher accuracy than single feature prediction. In order to make the model stable and easy to be explained, independent variables with significant regression effect were included in the model and those with no significant regression effect were excluded. In our study, the shape and margin of the entire thyroid nodule, the configuration, rim and echogenicity of the internal solid portion, and calcification were identified as candidate factors by forward stepwise analysis. A taller than wide shape other than microcalcification was revealed to be the strongest independent predictor for malignancy in PCTNs in the current study. In other words, a taller than wide shape was associated with an approximately13.5-fold increase in cancer risk when other independent variables were completely identical in PCTNs. Nevertheless, it was controversial to the recognized view that microcalcification was the most specific feature of malignant thyroid tumors [15]. Kim et al. [16], who initially described the taller-than-wide sign which was also known as anteroposterior–transverse ratio (A/T) >1, postulated that benign nodules grow parallel to normal thyroid tissue planes while malignant nodules (taller than wide) grow across normal thyroid tissue planes, which was similar to those previously reported in breast US studies. A number of investigators had documented that the taller-than-wide sign of the thyroid mass, as the sole criterion or in combination with other US features, was useful for differentiating malignant from benign masses [17, 18]. Besides, the American Association of Clinical Endocrinologists (AACE) and the American Thyroid Association (ATA) consider that US features with the highest specificities (median >90%) for thyroid cancer are microcalcifications, irregular margins, and a taller than wide shape [19, 20]. To our knowledge, this is the first paper that reported a taller than wide shape as the most specific feature of malignant PCTNs. In this study, all the 12 malignant PCTNs demonstrated with a taller than wide shape was confirmed by surgery as papillary thyroid carcinoma. However, the sensitivity of a taller than wide shape was significantly poorer than that of microcalcification showed in the present study.
Several limitations in our study cannot be ignored. First of all, the malignancy rate in our study may have been affected by some degree of selection bias. In our study, the PCTNs with FNAC results were excluded which would probably tend to cause us to underestimate the incidence of cancer in PCTNs. Second, the number of malignant cases is relatively small due to the small proportion of malignant PCTNs in thyroid cancer. Finally, this study was performed by a radiologist who had experience with thyroid US; therefore, it does not represent general operators with less experience in thyroid US or trainees.
In conclusion, the current study demonstrated that a taller-than-wide shape and spiculated or microlobulated margin were significantly associated with malignancy in PCTNs. An eccentric configuration, non-smooth rim, hypoechogenicity, and microcalcification were the US findings of the internal solid portion, which could suggest malignancy. These findings are useful for accurate differential diagnosis of malignant PCTNs. Prospective studies are needed to determine if the application of these findings in clinical decision making would be useful.