
Abstract
PURPOSE:
To evaluate the diagnostic value of quantitative shear wave elastography (SWE) for the differential diagnosis of solid pancreatic tumors.
MATERIALS AND METHODS:
A total of 66 solid pancreatic masses were enrolled in this study and all the lesions underwent quantitative SWE. The stiffness of the masses was expressed in shear wave velocity (SWV, m/s). The receiver operating characteristic (ROC) curve was plotted to assess the diagnostic performance of quantitative SWE. The optimal cutoff value for SWV in the differentiation of benign from malignant masses was determined.
RESULTS:
The final diagnoses were 26 benign and 40 malignant masses. The SWVs were statistically higher for pancreatic malignant masses compared with those for benign masses (3.30±1.22 m/s versus 1.31±0.64 m/s; P < 0.001). The area under the curve (AUC, 0.93) was obtained. When the best cut-off point was 1.77 m/s, the accuracy, sensitivity, and specificity were 92.4%, 90.0%, and 96.2%, respectively.
CONCLUSIONS:
Quantitative SWE is a novel technique that can be considered as a quantitative and objective diagnostic tool for prediction of pancreas malignancy.
Introduction
Pancreatic cancer (PC) has turned out to be one of the top 5 causes of cancer mortality so far with pancreatic ductal adenocarcinoma (PDAC) being the most common type, and the global annual incidence rate of pancreatic cancer is approximately 8/100000 persons [1]. One year and five year survival rates are estimated at 24% and 4.3% respectively [2]. However, many other lesions (most primarily focal chronic pancreatitis) can imitate malignancy, thus the differentiation between pancreatic cancer and these lesions remains a challenge [3, 4]. Conventional ultrasound (US) can quickly provide images of the pancreas without radiation, which is considered as an initial imaging modality for the detection and diagnosis of focal pancreatic masses. Because of an overlap in conventional US imaging, it is sometimes difficult to differentiate an pancreatic inflammatory mass from pancreatic cancer [5]. This is supported by the fact that 5–10% of cases confirmed to be inflammatory mass by histological finding disguise as pancreatic carcinoma in large amount of pancreatic resections for carcinoma of pancreas [6, 7].
US elastography is a method for the evaluation of tissue stiffness, and several studies have shown the usefulness of conventional strain elastography in patients with pancreatic lesions [8–16]. Currently, the benefits of elastography in pancreatic lesion assessment are gaining increasing recognition. Acoustic radiation force impulse (ARFI) is a novel and promising ultrasound-based elasticity diagnostic technique to evaluate tissue stiffness of pancreatic solid masses, which consists of virtual touch tissue imaging (VTTI) (Siemens, Mountain View, CA, USA) and virtual touch tissue quantification (VTTQ) (Siemens, Mountain View, CA, USA). The VTTQ provides quantitative information about the tissue stiffness by calculating the transverse shear wave velocity (SWV, m/s) within the region of interest (ROI) excited by the acoustic push force from the transducer, which is defined as shear wave elastography (SWE). In a previous study from our group, this technique of SWE was used to quantify the stiffness of normal pancreas and acute pancreatitis [17]. Based on the previous experience, it was hypothesized that the quantitative SWE might be used for the differential diagnosis between malignant and benign pancreatic masses. Therefore, this retrospective study was performed to assess the usefulness of SWE as a diagnostic tool for differential diagnosis of solid pancreatic masses.
Materials and methods
Patientss
The study was in agreement with the ethical guidelines of the Helsinki Declaration and approved by the Ethics Review Board of the University Hospital (the approval number of the ethical committee: 2017 1191 A129. Informed consent was also obtained from each patient. From June 2014 to December 2017, a total of 66 patients were retrospectively included in the study, with solid-appearing pancreatic mass at conventional US. All the patients underwent quantitative p-SWE examination before enrollment. The exclusion criteria for the patients were as follows: (1) Cystic lesions with a predominant cystic component (n = 9). (2) Mass size less than 5 mm in diameter, because the size of the sampling region of interest (ROI) for the quantitative SWE is 10mm×5 mm (n = 2). (3) SWV value acquisition failure (n = 4). Informed consent was also obtained from each patient before the US and SWE examinations. Final diagnoses of pancreatic masses were confirmed according to the following reference methods: (1) histology of surgical specimens in case of undergoing surgery; (2) a definite cytological diagnosis obtained from endoscopic ultrasound-guided fine-needle aspiration (EUS–FNA) for malignancy, together with consistent results at computed tomography (CT) in some unresectable tumors; (3) a final diagnosis was verified by means of a minimum 6 months follow-up with several imaging modalities, such as contrast-enhanced ultrasound (CEUS), CT, magnetic resonance imaging (MRI), endoscopic retrograde cholangiopancreatography (ERCP), EUS–FNA, blood examinations, and medical history in other unresectable tumors.
Shear wave elastography
All examinations were performed by an expert investigator using a Siemens Acuson S2000 ultrasound system (Siemens, Mountain View, CA, USA), equipped with 4C1 convex array probe (2.0–4.0 MHz). VTTQ is an integrated into conventional US system, so it could be performed during a standard examination. Conventional US scanning were performed on the patients in the supine position. The US characteristics and the size of masses were obtained. In the SWE procedure, SWV is shown superimposed on conventional US images which reflects tissue stiffness. When US scanners generate short-duration acoustic radiation forces (<1 ms), the tissue in a fixed size target ROI (10mm×5 mm) will be activated to induce an elastic shear wave tracked using detection pulses within milliseconds, which propagates in the lateral direction through the tissue. The propagation velocity of the shear wave is expressed in m/s. The patients were asked to hold their breath in SWE examination and the SWV value was shown in the screen. Whenever the measurement of the SWV is unsuccessful, the result displays X.XX m/s. There are several different explanations for the reason. The result of X.XX m/s may occur when the signal to noise ratio is poor, usually because of factors such as high shear wave attenuation or shear waves not being generated, and attenuation of the push pulse [18, 19]. The repeated measurements will finally receive an effective value if the reason is technical failure. Therefore, we had to perform two additional measurements while experiencing an unsuccessful attempt. The result of X.XX m/s which occurred in three consecutive measurements indicated that the SWV was too high and exceeded the upper limit of the possible measurement (5.00 m/s), and we would replace X.XX m/s by a value of 5.00 m/s, as previous studies [19]. In addition, to limit selection bias of ROI, SWV values were measured 7 times in the same depth in each patient; the median of all 7 measurements was considered as the final result. The stiffer the tissue through which the shear wave passes, the greater the shear velocity is [20].
Cytopathology or histopathology
Once EUS–FNA or surgery resection of the solid pancreatic mass were performed in patients, a senior pathologist, who had more than 15 years of experience in pancreatic disease diagnosis and was blind to the US and SWE findings, draw a finally cytological or histological evaluation after samples were appropriate processed.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (version 18.0; SPSS Inc, Chicago, IL, USA). The results were expressed as means±standard deviations (SD) for numerical variables together with the range. Comparison of the mean SWV between benign and malignant masses was analyzed using independent t-test. The diagnostic performance of quantitative SWE in predicting malignancy was calculated by receiver operating characteristic (ROC) curve analysis using the software of MedCalc 11, in which, the best cutoff points were achieved. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were also calculated for evaluation of the diagnostic ability of the quantitative p-SWE. A p-value < 0.05 was assumed statistically significant.
Results
Quantitative p-SWE was feasible in all 66 patients. There were 26 benign and 40 malignant solid pancreatic masses (male: female, 28:38), with a mean age of 62.7±14.30 years (range: 28 to 90). The mean size of solid pancreatic masses was 39.7±21.81 mm (range: 6 to 104) in maximum diameter. The patients were diagnosed as follows: 26 benign masses (mass-forming pancreatitis (MFP), 22; benign pancreatic neuroendocrine tumor, 2; pancreatic solid pseudopapillary tumor, 1; Fibrofatty tissue, 1) and 40 malignant masses (pancreatic cancer, 38; pancreatic metastasis from lung tumor and stomach cancer, 2) (Table 1). The mean SWVs of benign masses were 1.31±0.64 m/s (range: 0.75 to 4.20), while those of malignant masses were 3.30±1.22 m/s (range: 1.17 to 5.00, P < 0.001) (Table 2, Fig. 1, 2, 3).
Clinical characteristics
Clinical characteristics
Virtual touch tissue quantification (VTTQ) characteristics
Shear wave velocity (SWV).
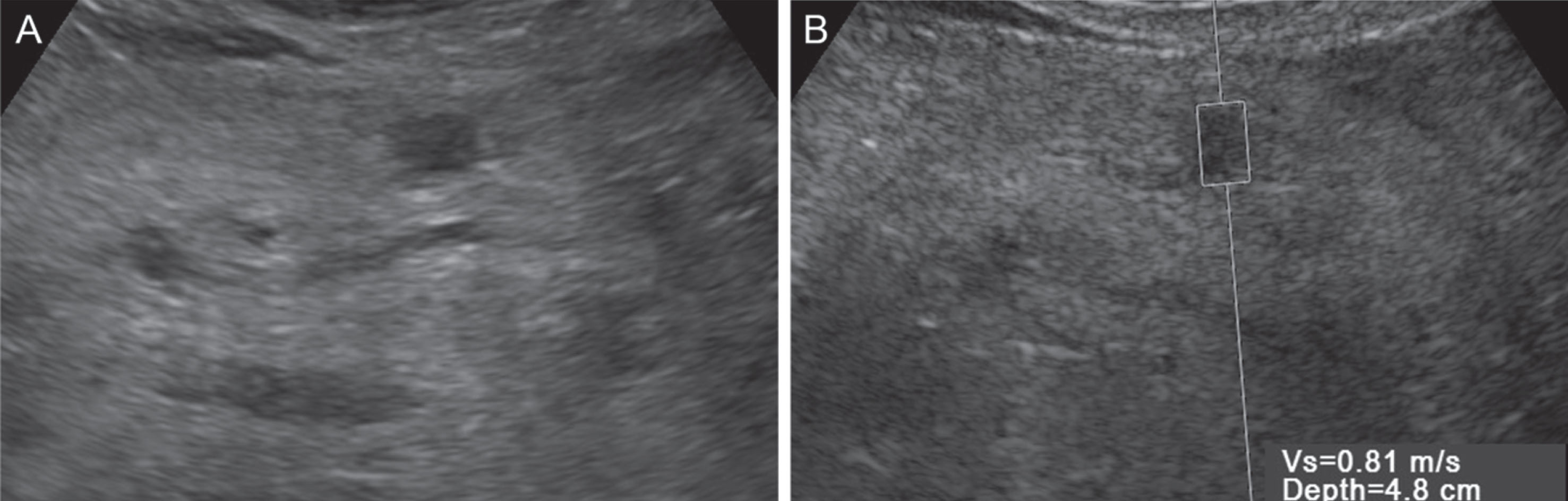
A 62 year old man with mass-forming pancreatitis. A. The lession shows a hypoechoic mass on conventional image. B. The shear wave velocity (SWV) of the lesion using virtual touch tissue quantification (VTTQ) is 0.81 m/s.
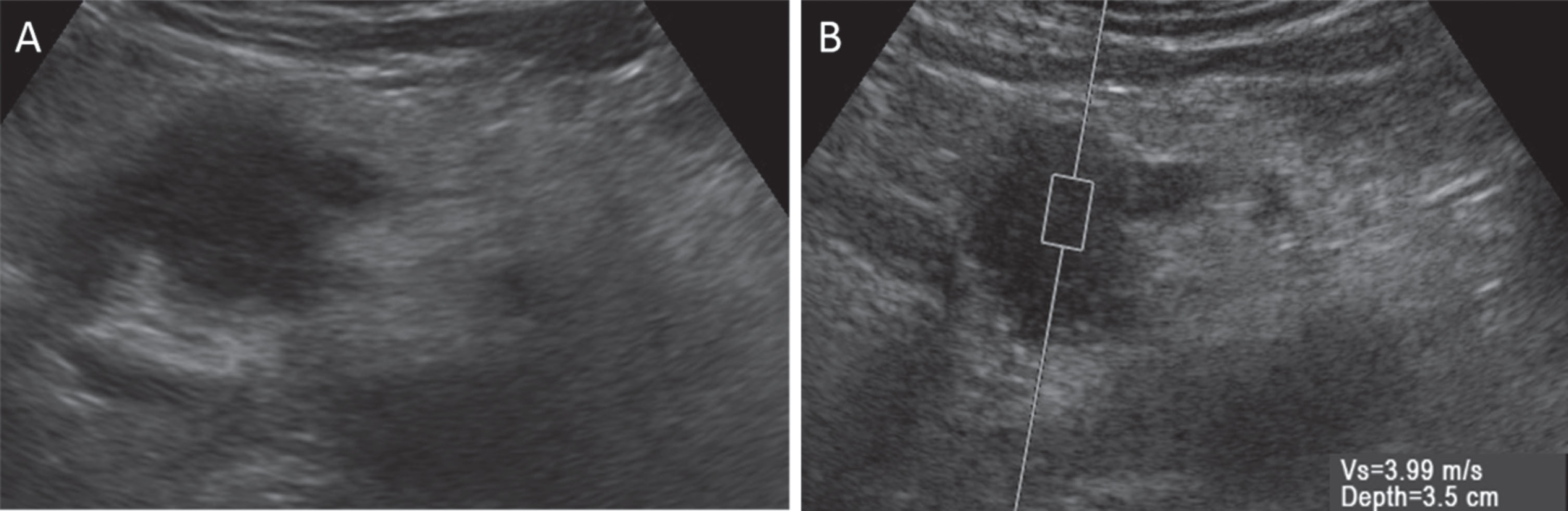
A 68 year old man with pancreatic cancer. A. The lession shows an irregular hypoechoic mass on conventional image. B. The shear wave velocity (SWV) of the lesion using virtual touch tissue quantification (VTTQ) is 3.99 m/s.
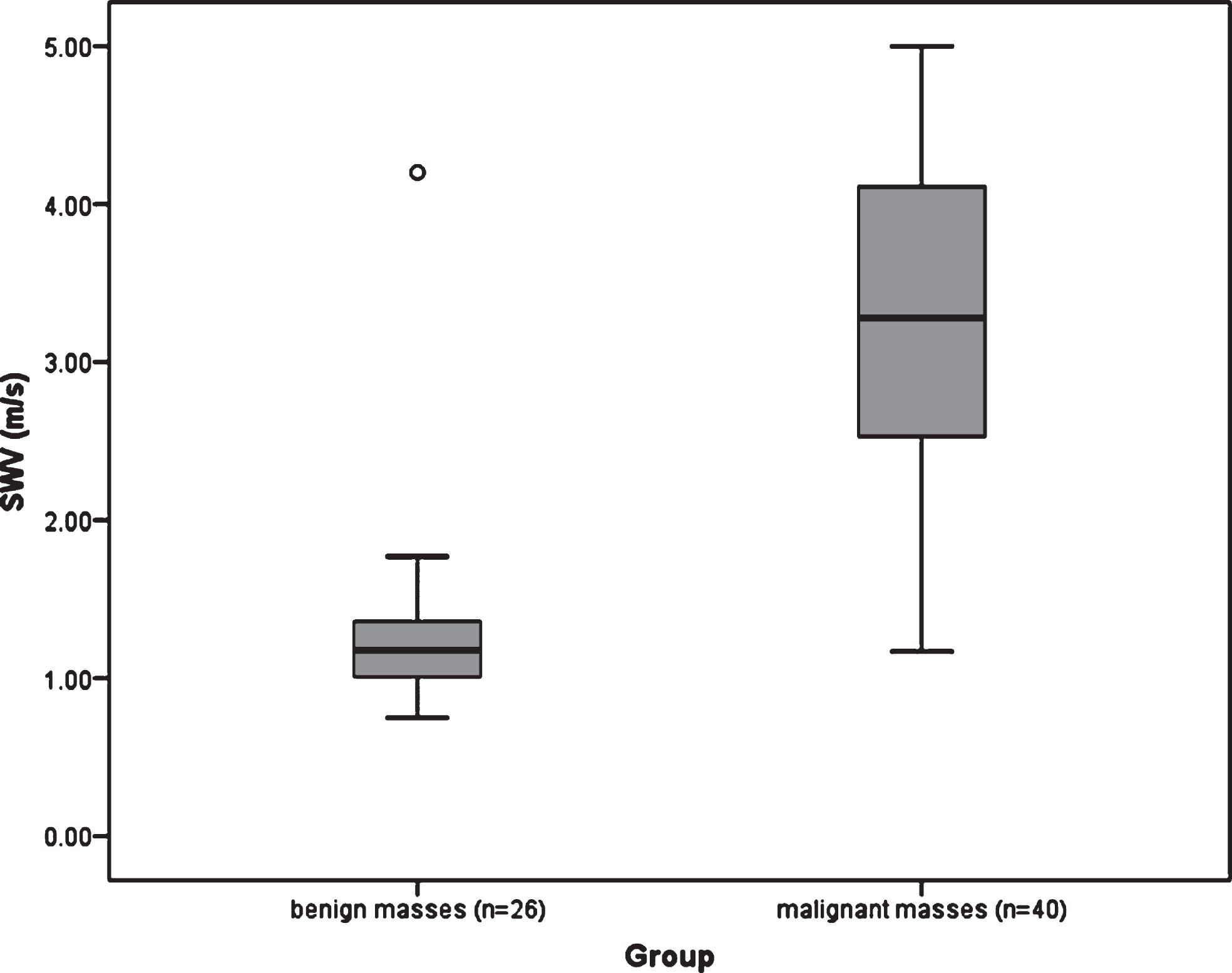
Box plots of the SWVs in benign and malignant pancreatic masses. The mean SWVs of benign and malignant masses were 1.31±0.64 m/s (range: 0.75 to 4.20) and 3.30±1.22 m/s (range: 1.17 to 5.00, P < 0.001).
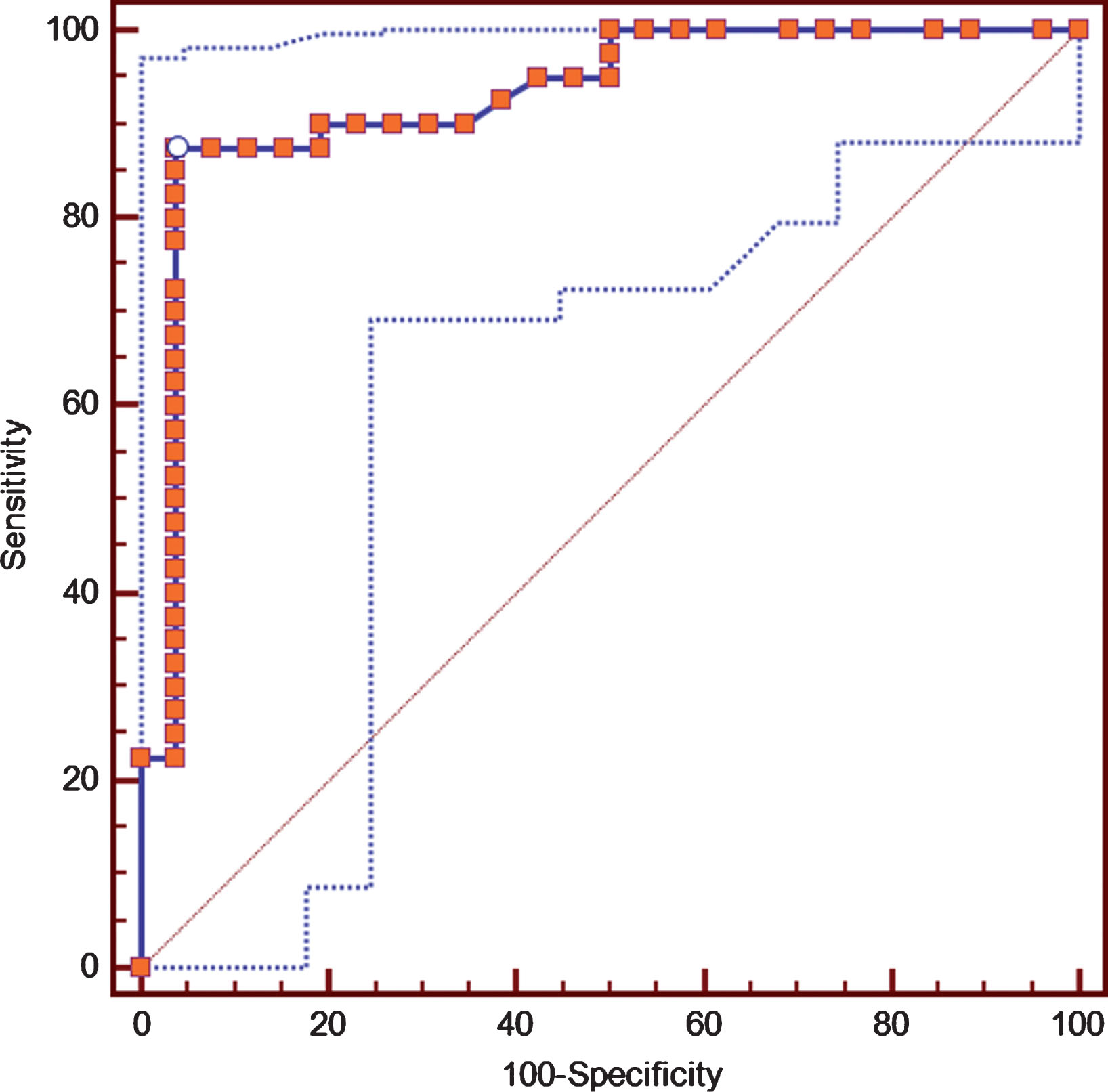
Receiver operating characteristic (ROC) curve of SWV in distinguishing malignant solid pancreatic masses. The area under the curve (AUC) of ROC curve was 0.93. The accuracy, sensitivity, and specificity were 92.4%, 90.0%, and 96.2%, respectively, when a best cutoff value of 1.77 m/s was applied.
The area under the curve (AUC) achieved a best value of 0.926 (95% confidence interval, 0.834–0.976) in ROC curve analysis, and the best cut-off SWV value was 1.77 m/s for malignancy (Fig. 4). When the pancreatic masses of SWVs less than 1.77 m/s were designated as benign lesion and those with SWVs of higher than 1.77 m/s were assigned as malignancy, the sensitivity of the differentiation reached 90% (36/40), and the specificity, PPV, NPV, and accuracy were 96.2% (25/26), 97.2% (35/36), 86.2% (25/30), and 92.4% (60/66) (Table 3). With this cut-off value, 36 malignant masses were classified correctly, whereas one inflammatory mass was erroneously considered as malignant.
The diagnostic performance of SWV in differentiating malignant pancreatic masses
Positive predict value (PPV), negative predictive value (NPV).
With the introduction of elastography by Ophir et al. [21], endoscopic ultrasound (EUS) elastography has assumed an increasing role in the differential diagnosis of pancreatic lesions [8–14]. As a retroperitoneal organ, the pancreas is located deeply in the body, and the transcutaneous elastography in the assessment of pancreatic lesions is limited [15, 16]. The results of these conventional elastographic evaluation were defined according to the color map (the predominant color and the homogeneity or heterogeneity of color distribution) or semi-quantification elasticity of focal pancreatic lesions. In the study published by Itokawa et al. [12], using conventional strain elastography, the mean strain ratio (SR) of the pancreatic cancer (39.08±20.54) was significantly higher than that of mass-forming pancreatitis (23.66±12.65). A result was also reported by Iglesias-Garcia et al. [13] that inflammatory pancreatic masses had a higher mean strain ratio (3.28) than healthy pancreas (1.68) (P < 0.001), but lower than pancreatic adenocarcinoma (8.12) (P < 0.001), with the highest mean strain ratio (52.34) of endocrine tumors group.
However, the conventional strain elastography is a qualitative or semi-quantitative method for evaluation of tissue stiffness. In addition, an intrinsic limitation of qualitative elastography is that the diagnostic result is relatively subjective. The technical limitation of conventional strain elastography is manual control of the compression to probe in ROI. The elasticity map obtained is highly dependent on the compressibility limits under stress of the organ and on the extent of the tissue compression applied. On the other hand, EUS is invasive requiring sedation, and it is not suitable for all patients [22].
The ARFI-induced SWE, a recently developed US-based modality, is a promising diagnostic tool that is able to provide information about the physical properties of the tissues to estimate elasticity in an efficient and easy method, which could complement conventional US examination. With this technique, external compression and decompression of the tissue are not required while using an internal acoustic push pulse activated by the conventional US embedded software, so elasticity results are less affected by the operator experience and are more reproducible compared with conventional strain elastography [23, 24]. The generated SWV in SWE provides quantitative measurement of tissue elasticity, depending on the interactions with the transducer. As a diagnosis method, it is relatively objective [25, 26].
The quantitative SWE has been generally used for clinical diagnosis in various tissues, such as breast, thyroid, and liver, and so on [18–20, 27–30], However, relatively few studies focused on pancreatic lesions. In our previous study, for the normal pancreas, the mean SWVs were 1.18±0.23 m/s in pancreatic head and 1.21±0.20 m/s in pancreatic body; and were 1.18±0.20 m/s and 1.25±0.19 m/s in acute pancreatitis [17]. There was no statistical difference in SWV between normal pancreas and acute pancreatitis. In this present study, the mean SWV of malignant pancreatic masses (3.30 m/s) was higher than 1.31 m/s of benign masses.
Histologically, PDAC is characterized by an obvious desmoplastic reaction and fibrous tissue infiltrating [31, 32], and MFP is also characterized by various degrees of peri-lobular fibrosis with noticeably lower collagen content than pancreatic carcinoma [32, 33], which indicates that the stiffness of PDAC could be greater than that of MFP. PC and MFP accounted for most of pancreatic malignant and benign tumors in this study, respectively, so malignant tumors should have higher stiffness compared with benign tumors, as shown in our study and previous magnetic resonance elastography (MRE) study [34]. It was not consistent with the results of previous VTTQ studies, which indicated that there were no statistical differences in the mean SWV between benign (2.4±1.1 m/s) and malignant (3.3±1.0 m/s) solid pancretic lesions (P = 0.101) [22], and the median SWV of ductal adenocarcinoma and non-ductal adenocarcinoma in solid pancreatic lesions were 2.74 m/s (1.36–3.96 m/s) and 2.80 m/s(1.80–3.00 m/s) [35]. But the greatest insufficiency may be small sample cases (27 pancreatic lesions) in former study, the latter having only 7 non ductal adenocarcinoma case in solid pancreatic masses. In quantitative SWE, 4 malignant masses were not classified correctly, and one benign mass was erroneously considered as malignant using the cut-off point 1.77 m/s. Some malignant tumors (mucinous or cystic adenocarcinomas with extensive necrosis) are very soft [13], which could be shown low SWV values. The benign mass with high SWV value may be contains plenty fibrous tissue in pathology. These results indicate that in pancreatic disease, hard lesions may not always be malignant, while soft lesions may not always be benign. Meanwhile, the elasticity value of SWV could vary according to stiffness differences in the different stage of same disease, which may relate to intratumoral fibrosis. Therefore, there may be some possibility that quantitative SWE could be used to evaluate the progress and degree of pancreatic lesions.
The accuracy of quantitative SWE for the diagnosis of malignancy was, by a SWV 1.77 m/s as a cut-off value, 90.9%, sensitivity was 87.5%, specificity was 96.2%, PPV was 97.2%, NPV was 83.3%. In previous qualitative elastography by Iglesias-Garcia et al. [11], the sensitivity, specificity, PPV and NPV, and overall accuracy in detecting pancreatic malignancy were 100%, 85.5%, 90.7%, 100%, and 94.0%, respectively. With this qualitative elastography, among the MFP, AIP, and PC cases, the sensitivity for diagnosis of malignancy was 98.6% (71/72), specificity was 64.3% (9/14), PPV was 93.4% (71/76), NPV was 90.0% (9/10), and the accuracy was 93.0% (80/86) in Itokawa et al. [12] studies. Recently, Săftoiu et al. [14] reported a semiquantitative method based on performing computer-enhanced dynamic analysis using a hue histogram in a multicenter study. Based on a cut-off value of 175 in focal pancreatic masses, they reported that the results for the differential diagnosis between benign and malignant lesions were sensitivity of 93.4%, specificity of 66.0%, and overall accuracy of 85.4%. Iglesias-Garcia et al. [13] pointed out that the sensitivity, specificity, and accuracy for detecting pancreatic malignancy were 100%, 92.9%, and 97.7%, respectively (AUC, 0.98), when a strain ratio of 6.04 was used to as a cut-off value. However, CEUS (according to the Guidelines of the European Federation of Societies for Ultrasound in Medicine and Biology, EFSUMB) and MRI with special contrast agent can be applied to evaluate the macro- and micro-vascularization of pancreatic solid masses for decisions to operative treatment [36, 37], with VTTQ can’t doing this. But VTTQ is potentially able to differentiate more complex (mucinous) from simple (serous) content in pancreatic cystic lesions study [38].
This study had some limitations. Firstly, VTTQ is not an always available US technique. The small tumors (diameter < 5 mm) are not enrolled in this study, which could be diagnosed using EUS and CEUS. Secondly, the SWV measurements are affected by different degrees of artificial compression applied to pancreatic masses to get image high resolution [15], since the pancreas is seated in the deep body. Furthermore, pancreas is near a large blood vessel, and quantitative SWE is a static image that is sensitive to motion during measurement, so in some way the elasticity value is not perfectly accurate. Finally, not all pancreatic masses have been confirmed by pathological results.
In conclusion, based on the study of sufficient consecutive patients, the present quantitative SWE technique appears to be a useful tool with a high accuracy for the differential diagnosis of pancreatic solid masses. In quantitative SWE procedures, the optimal cut off value may be obtained, which show an excellent sensitivity and specificity in detecting pancreatic malignancy. Future investigations are needed to confirm these results in multicenter studies.