
Abstract
OBJECTIVE:
To investigate the association between ultrasound appearances and pathological features in small breast cancer.
MATERIALS AND METHODS:
A total of 186 small breast cancers in 186 patients were analyzed in this retrospective study from January 2015 to December 2019 according to pathological results. Forty-seven cases of axillary lymph node metastasis were found. All patients underwent radical axillary surgery following conventional ultrasound (US) and contrast-enhanced ultrasound (CEUS) examinations. The association between ultrasound appearances and pathological features was analyzed using univariate distributions and multivariate analysis. Then, a logistic regression model was established using the pathological diagnosis of lymph node metastasis and biochemical indicators as the dependent variable and the ultrasound appearances as independent variables.
RESULTS:
In small breast cancer, risk factors of axillary lymph node metastasis were crab claw-like enhancement on CEUS and abnormal axillary lymph nodes on US. The logistic regression model was established as follows: (axillary lymph node metastasis) = 1.100×(crab claw-like enhancement of CEUS) + 2.749×(abnormal axillary lymph nodes of US) –5.790. In addition, irregular shape on CEUS and posterior echo attenuation on US were risk factors for both positive estrogen receptor and progesterone receptor expression, whereas calcification on US was a risk factor for positive Her-2 expression. A specific relationship could be found using the following logistic models: (positive ER expression) = 1.367×(irregular shape of CEUS) + 1.441×(posterior echo attenuation of US) –5.668; (positive PR expression) = 1.265×(irregular shape of CEUS) + 1.136×(posterior echo attenuation of US) –4.320; (positive Her-2 expression) = 1.658×(calcification of US) –0.896.
CONCLUSION:
Logistic models were established to provide significant value for the prediction of pre-operative lymph node metastasis and positive biochemical indicators, which may guide clinical treatment.
Introduction
Mammography, ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) are procedures that are used to determine breast disease diagnosis. Mammography remains the most important diagnostic tool for women with low-density breast tissue and over 40 years old [1]. However, the use of ionizing radiation and uncomfortable examination limits the use of mammography for breast screening [2]. In contrast, ultrasonography is the most effective procedure for diagnosis of small tumors in women with dense breast tissue and for screening in young women. Furthermore, CT and MRI are not conventional diagnostic procedures and are mainly used for the screening of high-risk patients. Breast CT images have limited spatial resolution and cannot provide more details compared with MRI [3, 4].
Conventional ultrasound (US) is the most common method for diagnosing breast diseases [5], but its application in differentiating between benign and malignant breast lesions is limited. Previous studies have reported that US elastography reflects the stiffness of breast tissue and is used as a diagnostic procedure in breast cancer patients [6–8]. Contrast-enhanced ultrasound (CEUS) provides more information regarding the tumor blood supply, thus, it may be more helpful for the identification of breast diseases in combination with conventional US [9–11].
The progression of breast disease is generally based on histopathology and molecular biology, on which clinicians, pathologists and biologists are focused [12–15]. The clinical and imaging features are based on histological and molecular characteristics, thus the present study focused on pathological features. The high rate of axillary lymph node metastasis and high level of histologic grade indicated that prognosis was relatively poor. The positive expressions of the estrogen receptor (ER) and the progesterone receptor (PR) in patients with breast cancer can guide antihormonal therapy [16]. Human epidermal growth factor receptor-2 (Her-2) and Ki-67 are biomarkers that reflect the invasiveness and metastasis capacity of breast cancers [13, 18].
“Small breast cancer” indicates that the largest size of the lesion is ≤2 cm observed by conventional US [19]. Generally, the larger the size of the breast cancer, the worse the prognosis, including the pathological indicators related to proliferation and invasiveness. However, many studies have shown that the prognosis of some small breast cancer could be relatively poor [19–21].
Yu’s study declared that some ultrasound appearances of small breast cancer, including perforating vessels and maximum cortical thickness of lymph nodes > 3.0 mm, correlated with axillary lymph node metastasis [19]. However, the US features found in the study were not classical. We hypothesized that the application of CEUS might be more helpful and valuable in the identification and evaluation of small breast cancer. However, incomplete US elastography data restricted us from more systematic research. The purpose of our study was to investigate the association between conventional US and CEUS appearances and pathological features to guide diagnosis and treatment of small breast cancer.
Materials and methods
Patients
The present study was a retrospective analysis that included 186 patients with 186 pathologically confirmed small breast lesions from January 2015 to December 2019 at Shanghai General Hospital. The inclusion criteria were: a maximum tumor diameter of ≤2 cm observed by conventional US; patients underwent conventional US and CEUS examinations performed by the same sonographer using the same US machine as usual for patients with breast mass before surgery; and the pathologic results for each lesion was available after radical axillary surgery. The exclusion criteria included: incomplete, unsatisfactory or missing US images; previous treatment or interventional diagnosis before surgery; pregnant or breastfeeding. The most suspicious lesion was chosen in patients that had more than one lesion confirmed by pathology. Our retrospective study was approved by the institutional ethics committee of Shanghai General Hospital, and each patient signed informed consent before CEUS.
Conventional US and CEUS equipment
We used an APlio 500 (TOSHIBA Medical Systems, Minato Ward, Tokyo, Japan) to carry out conventional US and CEUS examinations. We used sulfur hexafluoride microbubbles (SonoVue®, Bracco Imaging S.p.A., Milan, Italy) as the contrast agent.
Conventional US and CEUS examination
Two sonographers with 3–20 years of experience in breast conventional US according to American Institute of Ultrasound Medicine guidelines and 2–6 years of experience in CEUS performed the US scanning. The sonographers have been uniformly trained, and videos and images were saved in strict accordance with storage standards for further analysis. All patients were positioned with fully exposed breasts. During the examination, the conventional US characteristics were noted, including lesion location, size, the ratio between length and width, margin, shape, internal echo, posterior echo, peripheral tissue distortion, calcification, blood flow and axillary lymph node status. Images were stored.
After conventional US, the same sonographer performed CEUS. The target section of CEUS was chosen based on the plane that consisted of the richest blood supply shown on conventional US images. We selected the most suspicious plane if the lesion lacked blood supply, such as the plane with the most irregular shape or maximal diameter. We performed the CEUS procedure in dual image mode to ensure the accuracy of results, and we set the mechanical index at 0.06. We injected 4.8 mL of sulfur hexafluoride microbubbles via the antecubital vein before injecting 5–10 mL of saline. Videos and images were recorded for further analysis.
Image analysis
Two skilled sonographers independently classified the conventional US and CEUS images in accordance with the Breast Imaging Reporting and Data System (BI-RADS). The sonographers had 3–20 years of experience in breast US diagnosis and 2–6 years of experience in CEUS; they were not the sonographers referred to above who performed the scans. Sonographers were blinded to other patient information and each other. Upon disagreement, the sonographers re-evaluated the lesion in company with each other and reached a consensus. The lesions were classified into categories 0, 1, 2, 3, 4a, 4b, 4c and 5 using BI-RADS lexicon. Categories 1, 2 and 3 were considered benign, whereas categories 4a, 4b, 4c and 5 were considered malignant. Suspicious sonographic features of malignancy were: irregular shape, unclear margins (speculated or angular), heterogeneity, calcifications, posterior echo attenuation, taller than wide, abundant blood flow, and abnormal axillary lymph nodes.
Results of CEUS were based on conventional US and the following were determined: enhancement intensity and time, enhancement direction, enhancement patterns (with or without ring and crab claw-like), internal homogeneity, perfusion defect, size, margin and shape. The CEUS BI-RADS scores were determined similar to the five-score system supposed by Luo [22].
Pathology
All patients underwent radical axillary surgery within 3 days after ultrasound examinations. The pathology results were considered as the reference standard. The lymph node metastasis and biochemical indicators, including positive or negative expression of ER, PR, Her-2, and Ki-67, were recorded according to pathological diagnosis. We considered immunohistochemistry staining with higher than 1%positive expression for ER and PR a positive result. Her-2 immunohistochemistry staining at “3+” or “2+” positive expression by fluorescence in situ hybridization was considered positive for Her-2. Ki-67 expression of more than 14%using immunohistochemistry was considered positive.
Statistical analysis
We used SPSS (version 26.0 for Windows; SPSS Inc., Chicago, IL, USA) to perform statistical analysis. The associations between ultrasound appearances and pathological features were analyzed using univariate distributions and multivariate analysis successively. We established a logistic regression model by taking the pathological diagnosis of lymph node metastasis and biochemical indicators as the dependent variable and the conventional US and CEUS appearances as independent variables. We used the forward method of maximum likelihood estimation to perform stepwise regression of the dependent variable, which ensured filtering the risk factors among independent variables that were related to lymph node metastasis and biochemical indicators. β refers to the regression coefficient. SE was standard error. OR was odds ratio. Wald χ2 testing was used for the regression coefficient. A P-value < 0.05 was considered statistically significant.
Results
A total of 186 pathologically confirmed small breast lesions from 186 patients were included in the present study. A total of 180 (96.8%, 180/186) lesions were accurately diagnosed by conventional US (as shown in Fig. 1), whereas CEUS corrected three false lesions (as shown in Fig. 2). Three lesions were misdiagnosed benign breast cancer because they lacked typical ultrasound characteristics.
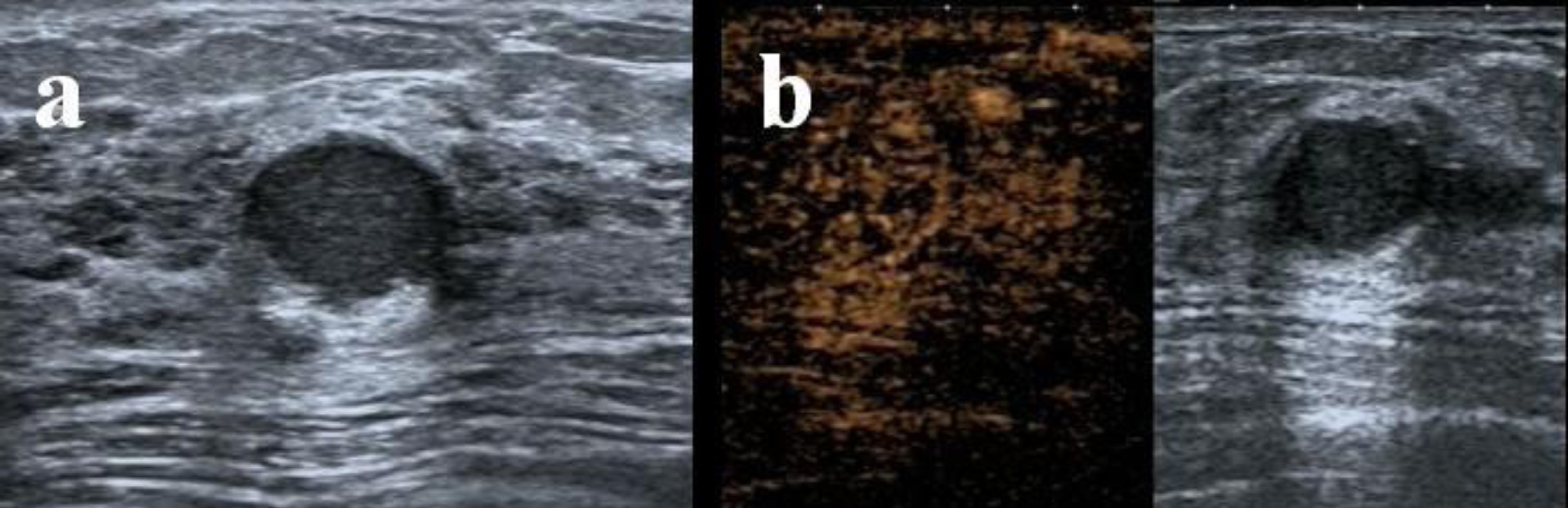
A 48-year-old patient with pathologically confirmed small breast cancer with a hypoechoic solid nodule located at 2 o’clock in the right breast with clear margins and regular shape is shown on conventional US (a), and shown on CEUS is equal enhancement, clear margins and regular shape (b), both indicating a benign lesion with a BI-RADS 3 score.

A 66-year-old patient with pathologically confirmed small breast cancer with a cystic solid nodule located at 9 o’clock in the right breast with clear margins, regular shape and scattered blood flow is shown on conventional US (c), which indicates a benign lesion with a BI-RADS 3 score. Signs shown on CEUS are early high enhancement, clear margins and irregular shape (d), indicating a malignant lesion with a BI-RADS 4c score.
The statistically significant conventional US and CEUS appearance of 186 small breast cancers, and the results of the univariate distributions are presented in Table 1. Our results showed that crab claw-like enhancements observed by CEUS and heterogeneous, calcification, abnormal axillary lymph nodes seen by US were significantly correlated with axillary lymph node metastasis. In addition, we found that irregular tumor shape shown by CEUS was closely related to advanced histological grade. Positive ER expression was correlated with crab claw-like enhancements and irregular tumor shapes observed with CEUS, as well as unclear margins, speculated or angular margins, and posterior echo attenuation observed with US. In addition, positive PR expression was correlated with appearances of crab claw-like enhancements and irregular tumor shapes observed with CEUS, as well as speculated or angular margins and posterior echo attenuation observed with US. Tumor heterogeneity and calcifications seen with US correlated with positive Her-2 expression. However, no tumor features correlated with Ki-67 expression.
The statistically significant conventional US and CEUS appearance of 186 small breast cancers
The statistically significant conventional US and CEUS appearance of 186 small breast cancers
US: ultrasound; CEUS: contrast-enhanced ultrasound.
The logistic regression models were established between US appearance and pathological features, including axillary lymph node metastasis and biochemical indicators. However, the relationship between the index of histological grade and Ki-67 expression and US features showed no statistical significance. The correlations between US appearance and axillary lymph node metastasis, ER expression, PR expression and Her-2 expression in 186 small breast cancers were statistically analyzed (Table 2, 4 and 5). Table 2 shows that crab claw-like enhancement (using CEUS) and abnormal axillary lymph nodes (using US) were risk factors for lymph node metastasis in small breast cancer patients. Irregular tumor shape (observed by CEUS) and posterior echo attenuation (observed by US) were risk factors for positive ER and PR expression (Table 3 4). In Table 5, we show that the presence of calcification (seen by US) increased the risk of positive Her-2 expression.
Logistic regression analysis of the correlation between US appearances and axillary lymph node metastasis in 186 small breast cancers
Logistic regression analysis of the correlation between US appearances and axillary lymph node metastasis in 186 small breast cancers
US: ultrasound; CEUS: contrast-enhanced ultrasound; β: regression coefficient; SE: standard error; OR: odds ratio.
Logistic regression analysis of the correlation between US appearances and ER expression in 186 small breast cancers
US: ultrasound; CEUS: contrast-enhanced ultrasound; β: regression coefficient; SE: standard error; OR: odds ratio.
Logistic regression analysis of the correlation between US appearances and PR expression in 186 small breast cancers
US: ultrasound; CEUS: contrast-enhanced ultrasound; β: regression coefficient; SE: standard error; OR: odds ratio.
Logistic regression analysis of the correlation between US appearances and Her-2 expression in 186 small breast cancers
US: ultrasound; CEUS: contrast-enhanced ultrasound; β: regression coefficient; SE: standard error; OR: odds ratio.
The logistic models were as follows:
(axillary lymph node metastasis) = 1.100×(crab claw-like enhancement of CEUS) + 2.749×(abnormal axillary lymph nodes of US) –5.790;
(positive ER expression) = 1.367×(irregular shape of CEUS) + 1.441×(posterior echo attenuation of US) - 5.668;
(positive PR expression) = 1.265×(irregular shape of CEUS) + 1.136×(posterior echo attenuation of US) - 4.320;
(positive Her-2 expression) = 1.658×(calcification of US) –0.896.
Discussion
Early detection is crucial for small breast cancer due to diverse clinical features and possible poor prognosis. The sensitivity of mammography is greatly affected by the density of breast tissue. Previous studies have shown 80–98%sensitivity in women with fatty breast tissue versus 30–48%sensitivity in women with dense breast tissue [23, 24]. MRI has been proven to be the most sensitive modality for the detection of breast cancer, with a sensitivity of 95%. Furthermore, the addition of MRI to conventional techniques increases the sensitivity of detection [25, 26]. A study by Chen [27] evaluated the sensitivity of mammography, ultrasound, MRI, and combinations for the detection of small (≤2 cm) breast cancer and reported that mammography had limited diagnostic sensitivity, especially in dense breast tissue, and that ultrasound is more sensitive than mammography, regardless of breast density. The addition of MRI with mammography may increase sensitivity without increasing the rate of mastectomy. Our study aimed to investigate the diagnostic value of conventional US and CEUS in small breast cancer.
CEUS showed microcirculation perfusion in small breast cancer. The CEUS BI-RADS scores were obtained with the five-score system proposed by Luo [22] derived from enhancement features and the BI-RADS scores using conventional US. When CEUS scores are > 3, readers should upgrade the BI-RADS scores using conventional US to obtain the final CEUS BI-RADS scores (upgrade BI-RADS score 3 to 4a, 4a to 4b, 4b to 4c or 4c to 5). Readers were asked to downgrade the final CEUS BI-RADS scores when the CEUS scores were ≤3 (downgrade BI-RADS score 5 to 4c, 4c to 4b, 4b to 4a, or 4a to 3). In the present study, we evaluated tumor appearance, BI-RADS scores using conventional US and CEUS, and pathological features in patients with small breast cancer.
In our study, a chi-square test for univariate distributions and logistic models established by multivariate analysis were used to determine the relationship between ultrasound appearances and pathological features of small breast cancer. Characteristics, such as crab claw-like enhancements observed by CEUS and abnormal axillary lymph nodes seen by US, were significantly correlated with axillary lymph node metastasis and were included in the logistic model. Regression coefficients for crab claw-like enhancement and lymph node metastasis were 1.100 and 2.749, respectively, and the ORs were 3.004 and 15.626, respectively. Therefore, compared with patients with no signs of crab claw-like enhancement, the presence of crab claw-like enhancement increased the risk of axillary lymph node metastasis by 3.004-fold. In addition, compared with patients demonstrating no signs of abnormal axillary lymph nodes observed by US, the presence of abnormal axillary lymph nodes increased the risk of metastasis by 15.626-fold. The abundant and disorganized blood flow in malignant tumors and infiltration into surrounding breast tissue led to the appearance of crab claw-like enhancements found using CEUS. The presence of axillary lymph nodes in US images may indicate a high tumor proliferation rate and can result in the disruption of the internal structure of lymph nodes and disappearance of the medulla. These results agreed with previous studies [28–30]. Because axillary lymph node metastasis was related to poor prognosis, our findings might be beneficial to clinical practice.
In previous studies [31–33], investigators have divided breast cancers into four subtypes by biochemical indicators, including luminal A or B subtype (luminal A/B), Her-2 over-expression subtype and triple negative subtype, and explored the value of ultrasound for the differential diagnosis of molecular subtypes in breast cancer. However, in our study, biochemical indicators were divided into two subtypes, including positive and negative expression, because of the low number of cases. According to the logistic models established by multivariate analysis, irregular tumor shape (shown with CEUS) and posterior echo attenuation (observed with US) were correlated with positive ER and PR expression. Abundant and disorganized blood vessels, especially around lesions and surrounding breast tissue, led to irregular tumor shapes observed on CEUS images. As a result of invasion of malignant tumors, fibrosis led to sound attenuation, which resulted in a posterior echo attenuation seen by US. Consistent with our findings, this ultrasound sign was found in a previous study [29]. Cancers that are positive for ER and PR expression are sensitive to antihormonal therapy; thus, our results may be valuable for preoperative prognostication.
We showed that calcification on US was a risk factor of Her-2 expression, with a regression coefficient of 1.658 and OR of 14.588. Hence, the presence of calcification seen by US increased the risk of Her-2 expression by 14.588-fold compared with patients with no calcification. These results suggested that positive Her-2 expression was correlated with the invasion of malignant tumors, suggesting rapid growth and active metabolism. When tumors lack nutrition and oxygen, ischemic necrosis and calcium deposition occur, resulting in calcification shown on US images. These findings were consistent with previous studies [28, 29]. Given that Her-2 expression indicates the invasiveness and metastasis capacity of breast cancers, calcification shown by US might guide clinical diagnosis.
Advanced histological grade is related to a high proliferation rate, and Ki-67 reflects the invasiveness and metastasis capacity in breast cancers. In our study in small breast cancer, no ultrasound features correlated with advanced histological grade or positive Ki-67 expression by multivariate analysis.
In the present study of small breast cancer, several classic ultrasonographic appearances were not found or involved in our prediction model because it was hard to observe classic malignant pathological and ultrasound features given the small tumor size. There were some other limitations of the study: the retrospective single-center study limited the number of cases and pathological types, and the study only included small breast cancer, thus, the results may not be applicable to other breast cancers. Further studies that are prospective and consecutive with a larger number of samples will be carried out to verify the findings.
Conclusion
Crab claw-like enhancement on CEUS and abnormal axillary lymph nodes on US were correlated with axillary lymph node metastasis in small breast cancer. In addition, positive ER and PR expressions were risk factors for both irregular tumor shape on CEUS and posterior echo attenuation on conventional US, whereas calcification on US was the only risk factor for positive Her-2 expression. Logistic models were proven to provide great benefit for the prediction of lymph node metastasis and positive biochemical indicators, guiding treatment for small breast cancer.
Footnotes
Acknowledgments
The current work was supported by the National Natural Science Foundation of China (Grant Nos. 82071931, 82130057), program for Shanghai Outstanding Medical Academic Leaders (2019LJ18), the interdisciplinary program of Shanghai Jiaotong University (ZH2018ZDA17), and the program from the Science and Technology Commission of Shanghai Municipality (No. 20Y11912400). The authors are grateful to Prof Rong Wu and Prof Yi-Jin Su for the valuable guidance in every stage of this article.