
Abstract
Biliary cystadenocarcinoma (BCAC) is an extremely rare intrahepatic cystic tumor. Patients usually present with nonspecific symptoms such as abdominal pain, abdominal distention, and abdominal mass. This tumor occurs most commonly in the left hemiliver and is thought to mainly develop from a benign biliary cystadenoma (BCA). At present, the disease is mainly diagnosed by ultrasound, CT, MR, and other imaging methods, and the main treatment is radical surgical resection. We reported a 75-year-old female with an unresectable huge BCAC (i.e., 161×145×122 mm in three orthogonal directions) and poor general condition (40 in Karnofsky Performance Status, KPS) who received sequential thermal ablation (i.e., cryoablation and microwave ablation) in combination with sclerotherapy using lauromacrogol. The diagnosis of intrahepatic BCAC was confirmed pathologically. Preablation grayscale US showed the BCAC with a clear boundary, regular shape, and cystic-solid mixed echogenicity, which appeared as a huge multilocular cystic lesions with thick internal sepatations. Preablation contrast-enhanced ultrasound (CEUS) showed honeycomb-like hyper-enhancement of the thick internal sepatations and cystic wall in the arterial and portal phase, and sustained enhancement of the thick internal sepatations and cystic wall in the late phase. 6-month postablation CEUS showed non-enhancement in most parts of the lesion in the arterial phase and 6-month postablation MRI showed the volume reduction ratio (VRR) was about 70%. The abdominal pain and abdominal distension were relieved remarkably, and her quality of life was greatly improved (70 in KPS). In conclusion, sequential thermal ablation in combination with sclerotherapy provides a successful translative therapy for this unresectable huge BCAC with a poor general condition, which makes subsequent curative surgery or ablation possible.
Introduction
Biliary cystadenocarcinoma (BCAC) is an extremely rare intrahepatic malignancy that occurs more frequently in females [1]. The existence of a transitional zone between normal cells and atypical cells in the cystic wall, as previously reported, proves that BCAC mainly develops from benign biliary cystadenoma (BCA) [2, 3]. Symptoms of BCAC are usually atypical and may include abdominal pain, bloating, nausea, vomiting, and an abdominal mass. Jaundice may or may not occur depending on the location of the tumor [4, 5]. BCA and BCAC are more common in the left lobe of the liver. This rare tumor is routinely treated with radical surgical resection, which previous studies have shown is associated with a low rate of recurrence and long survival [6].
If the tumor is too large to be removed, or the patient’s condition is not suitable for radical surgical resection, an alternative treatment strategy should be developed to destroy the tumor and alleviate the symptom. Ultrasound-guided interventional procedures such as ablation and sclerotherapy are both minimally invasive methods emerging with the development of technology. These methods have the advantages of minimal invasiveness, quick recovery, low cost, and ease to perform, and have been widely used in more and more fields such as liver, kidney, thyroid, breast, uterus, and so on [7, 8]. Ablation and sclerotherapy for BCAC have not been reported until the present. This article reports a case of US-guided sequential thermal ablation including cryoablation and microwave ablation (MWA), in combination with sclerotherapy, to treat a female patient with unresectable huge BCAC and poor general condition, which is proven to be a successful translative therapy for this patient and makes subsequent curative surgery or ablation possible. The Karnofsky Performance Status (KPS) was used to evaluate the overall status of the patient before and after the treatment, a score below 40 is considered as dependent while 0 is considered dead, 50–70 is considered semi-independent, above 80 is considered independent while 100 is considered perfect health.
Case report
Patient history
A 75-year-old female presented to our hospital with the chief complaint of a huge intrahepatic cyst, persistent abdominal distension, and low fever. The patient reported that a liver cyst was found in physical examination at the beginning of 2019, and no special treatment was taken. Subsequently, due to the continuous increase of the cyst volume during re-examination, she received 4 times ultrasound-guided liver cyst drainage in local hospitals from October 2019 to April 2021. A drainage tube was placed in the cyst for continuous drainage after the fourth treatment. Physical examination showed that the patient’s right upper abdomen was obviously protruding upward, and a mass of about 15 cm could be touched in the right upper abdomen. The mass was slightly soft with unclear boundaries, and there seemed to be a sense of fluctuation when pressed, without obvious tenderness or rebound pain. Outpatient ultrasound examination revealed a 145×117×160 mm cystic-solid mixed echoic lesion in the right lobe of the liver, which appeared as a huge multilocular cystic lesions with thick internal sepatations. Color Doppler flow imaging (CDFI) detected scarce blood flow signals inside the lesion (Fig. 1).
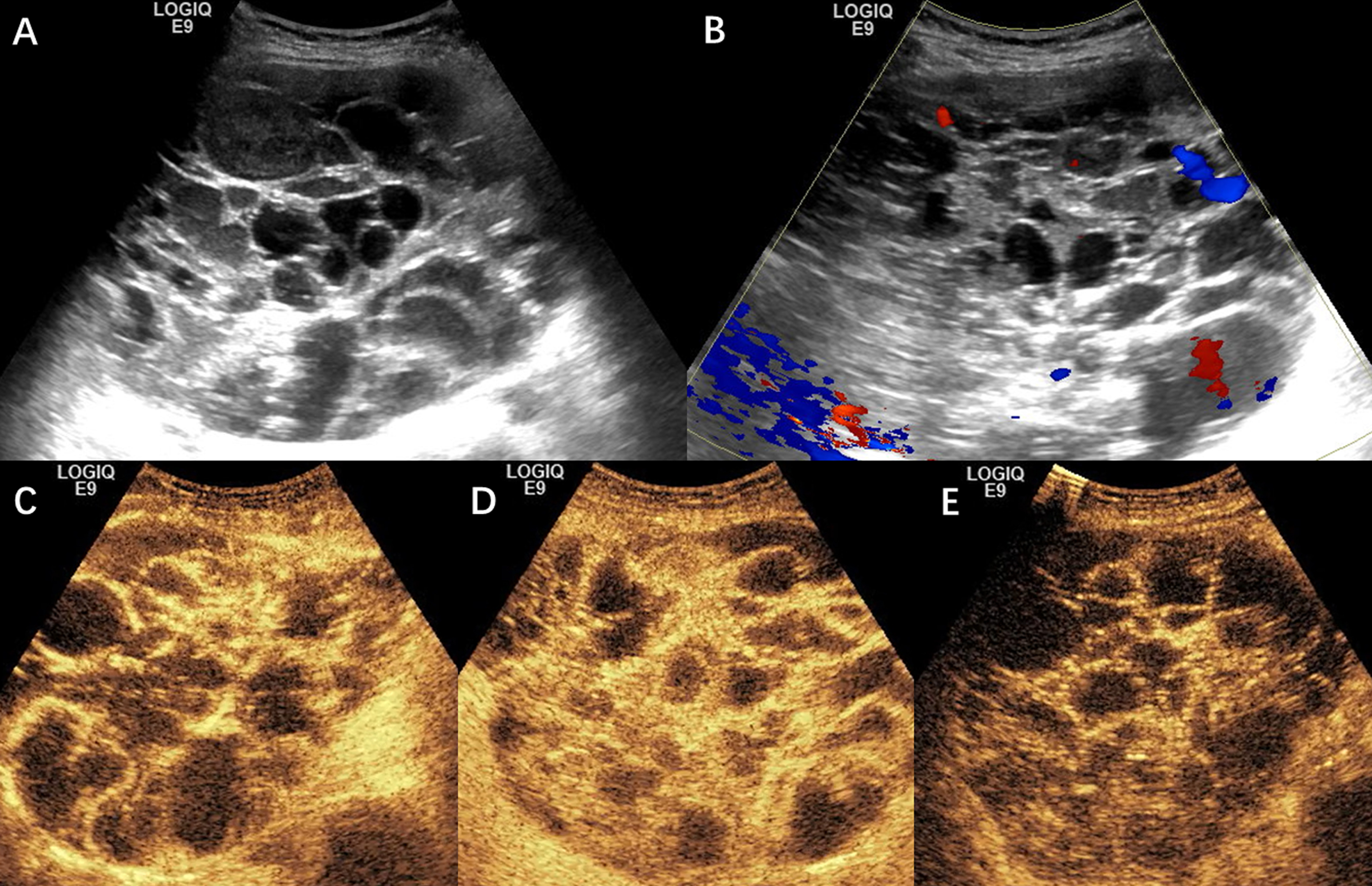
Preablation ultrasound examination of the 75-year-old female patient with a huge biliary cystadenocarcinoma. A. Preablation grayscale US shows the biliary cystadenocarcinoma (BCAC) with a clear boundary, regular shape, and cystic-solid mixed echogenicity, which appears as a large multilocular cystic lesions with thick internal sepatations. B. Preablation color Doppler flow imaging (CDFI) shows scarce blood flow signals inside the lesion. C. Preablation contrast-enhanced ultrasound (CEUS) shows honeycomb-like hyper-enhancement of the thick internal sepatations and cystic wall in the arterial phase (15 seconds after contrast agent injection). D. Preablation CEUS shows honeycomb-like hyper-enhancement of the thick internal sepatations and cystic wall in the portal phase (90 seconds after injection). E. Preablation CEUS shows sustained enhancement of the thick internal sepatations and cystic wall in the late phase (180 seconds after injection).
The patient was first diagnosed with large intrahepatic cyst accompanied by repeated infections in other hospitals. Considering the difficulty of surgery caused by the huge lesion, the chronic kidney disease (CKD) history and poor general condition of the patient (40 in KPS), and the rejection to invasive surgery by her and her family, we admitted her to our hospital as huge intrahepatic cystic-solid lesion accompanied with infection for minimal invasive treatment to improve outcomes and quality of life.
The patient was admitted with a percutaneous drainage tube placed in the intrahepatic cyst. The drainage fluid was cloudy, yellow-brown purulent fluid with a daily flow rate of about 3 to 5 ml. Based on the previous examination data, we arranged for her to undergo upper abdominal magnetic resonance imaging (MRI), chest computed tomography (CT), contrast-enhanced ultrasound (CEUS), blood biochemical test, and other related examinations. At the same time, the drainage fluid was extracted for the culture of pathogenic microorganism examination and drug sensitivity test. She received a non-contrast chest CT protocol for assessment of intrathoracic condition. And T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), Diffusion-weighted imaging (DWI), post-contrast sequence, and magnetic resonance cholangiopancreatography (MRCP) were taken as MRI protocols for comprehensive evaluation of her intrahepatic lesion. Gadopentetate dimeglumine (Magnevist, Bayer Schering, Germany) was used as contrast-enhancing agent.
Upper abdomen MRI of the patient suggested a huge intrahepatic mass with a size of 161×145×122 mm, with mixed-signal, clear boundary, thick separation and cystic walls, significantly enhanced cystic walls, and solid components in enhanced MRI. The patient was diagnosed with intrahepatic BCA with MRI (Fig. 3). We performed a CEUS examination on the patient. In this exam, the mixed echoic structure of the right liver showed honeycomb-like hyperenhancement of the thick internal sepatations and cystic wall in the arterial and portal phase, and sustained enhancement in the late phase (Fig. 1). Ultrasound-guided puncture biopsy was performed on the solid parts of the lesion because the possibility of malignant tumor cannot be ignored considering the patient’s age, gender, general condition, etc. And pathological findings confirmed the diagnosis of BCAC.
In terms of biochemical examination, the patient’s liver function was normal except for the albumin (ALB), and the main abnormal indicators were carbohydrate antigen 199 (CA199) in tumor marker, creatinine (CRE), blood urea nitrogen (BUN), glomerular filtration rate (GFR) in renal function because of the CKD history, white blood cell (WBC), red blood cell (RBC), hemoglobin (Hb), platelet (PLT) in blood routine examination, and C-reactive protein (CRP) in the inflammatory index (Table 1).
Pre-treatment and post-treatment biochemical examination during follow-up
Pre-treatment and post-treatment biochemical examination during follow-up
CA199, carbohydrate antigen 199 (normal, <27 U/ml). CRP, C-reaction protein (normal, <8.2 mg/L). WBC, white blood cell (normal, 3.5–9.5×109/L). RBC, red blood cell (normal, 3.8–5.1×1012/L). Hb, hemoglobin (normal, 115–150 g/L). PLT, platelet (normal, 125–350×109/L). ALB, albumin (normal, 40–55 g/L). *The patient’s abnormal renal function was caused by chronic kidney disease (CKD), which was not listed in the table because there was no significant fluctuation during the whole treatment.
The patient was diagnosed with intrahepatic BCAC. Considering the large tumor, elder age, and poor general condition, we planned to carry out treatments step by step under local anesthesia after careful communication with family members.
Step 1: Transcatheter hepatic artery embolization (TAE). Step 2: Ultrasound-guided cryoablation of solid parts in the tumor and fluid drainage of cystic parts of the tumor. Step 3: Ultrasound-guided sclerotherapy of the cystic parts of the tumor. Step 4: Ultrasound-guided MWA of solid parts in the tumor.
We expected to inactivate as many tumor tissues as possible through a combination of the above-mentioned multiple methods, and at the same time draining the cystic fluid to reduce the tumor volume to relieve the pain of abdominal distension and improve her life quality.
The main procedures of ultrasound-guided cryoablation and drainage were as follows:
Routine preablation ultrasound examination was performed to measure the size of the lesion and plan the puncture route of cryoablation. CDFI was used to display the vascularity of the lesion. Preablation CEUS was performed to evaluate the blood perfusion and SonoVue® (Bracco, Milan, Italy) was used as a contrast agent (Fig. 1). During the operation, intravenous sedation and analgesia combined with local anesthesia were used for anesthesia. The patient received an intravenous injection of 30 mg ketorolac tromethamine 30 minutes before the operation for intravenous analgesia. And 0.2 mg dexmedetomidine was mixed with 50 ml 0.9% sodium chloride for intravenous sedation, which was pumped into the patient with 15 ml/h from 15 minutes before operation and reduced to 5 ml/h 20 minutes after the operation beginning till the end of the operation. Under the guidance of real-time ultrasound, an 18G EV needle (Hakko, Nagano, Japan) was punctured into several large cystic cavities within the lesion, and a total of 180 ml of purulent, bloody, and other properties fluid was extracted. Under the guidance of real-time ultrasound, an 14G cryoablation probe (AccuTarget, Shanghai, China) was punctured into a predetermined solid part in the lesion, and the cryoablation instrument was turned on. Iceball was formed after cooling for 13–15 minutes and rewarmed for 3 minutes as a cycle. Two cycles of ablation were performed at each site under the guidance of the cryogenic treatment system. The ablation boundary was determined according to the size of the iceball formed. In the cryoablation, the lowest temperature was reduced to –165°C, and the rewarmed temperature was 40–50°C. The total cryoablation time was 70 min, and the total rewarmed temperature time was 30 min (Fig. 2). CEUS was performed to evaluate the local treatment response immediately after the ablation. And there was no enhancement in the ablated part. The patient was given abdominal compression bandaging to prevent bleeding after the operation.
The patient then received ultrasound-guided sclerotherapy for the cystic parts of the tumor 3 days after the cryoablation, about 125 ml purpuric brown fluid was extracted from the cysts. After repeated washing of each cyst cavity with 0.9% sodium chloride and metronidazole, 30 ml 1% lauromacrogol solution (i.e., polidocanol) was injected into the cystic cavities for repeated flushing. And 20 ml of lauromacrogol solution and 40 ml of lauromacrogol foam (solution: air = 1:3) were retained. The patient was well tolerated during and after the operation.
The patient received ultrasound-guided MWA for solid parts and drainage for cystic parts 7 days after the sclerotherapy, and the general procedures were similar to those before in cryoablation. During this treatment, a total of 370 ml brown fluid was extracted from the cystic parts of the tumor without sclerotherapy. The MWA was then performed at 60W power for 10 min 18s and 80W power for 62 min 26s. The total ablation time was 72 min 44s (Fig. 2).
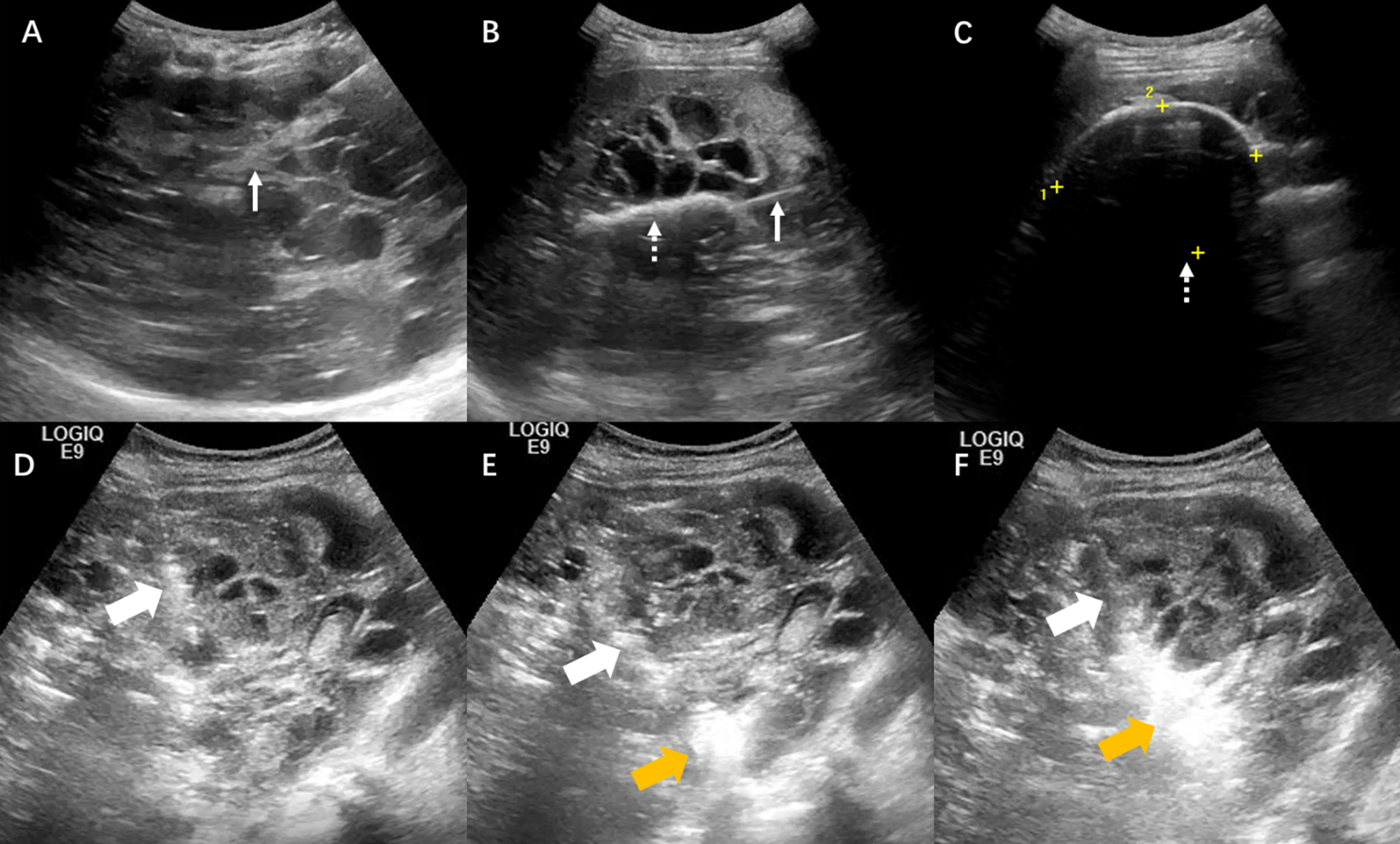
Ultrasound-guided percutaneous cryoablation and MWA ablation for the huge biliary cystadenocarcinoma. A. The cryoablation probe (solid arrow) is inserted into the solid portion of BCAC under ultrasound guidance. B. Remarkable hyperechoic iceball formation (dotted arrow) is observed around the probe throughout the ablation. C. Remarkable hyperechoic iceball formation (dotted arrow) with posterior acoustic shadowing is observed around the probe throughout the ablation. D. The microwave antenna (coarse arrow) is inserted into the solid portion of BCAC under ultrasound guidance. E. Remarkable hyperechoic gas formation (yellow coarse arrow) is observed around the antenna when the MWA is started. F. Remarkable hyperechoic gas formation (yellow coarse arrow) is observed around the antenna throughout the ablation and the range is expanding.
The patient received a total of 4 treatments, all of which were routinely treated with oxygen inhalation, ECG monitoring, liver function protection, nutritional support, and continuous anti-infection therapy. Her post-treatment condition was stable and was discharged 7 days after the last treatment. The symptoms of abdominal pain and persistent low fever showed significant remission.
Follow-up
This patient was readmitted 1 month after the treatment with poor appetite, lethargy, mild swelling and pain in the liver region, and repeated low fever. It was considered to be a cystic infection in BCAC based on the examination. Then, the patient was arranged to receive ultrasound-guided drainage of the cystic parts of the tumor under local anesthesia applying antibiotics for anti-infection purpose. Some solid parts were still active in the tumor in CEUS reexamination during this hospitalization. After one month of recovery, ultrasound-guided sclerotherapy was performed for the cystic parts and ultrasound-guided MWA was performed for the remaining active solid parts of the tumor, and the total microwave ablation time was 10 min 38s. Postablation CEUS showed that the tumor was smaller than before with a size of about 130×78×97 mm and showed non-enhancement in most parts in the arterial phase, portal phase, and late phase, indicating necrosis (Fig. 3).
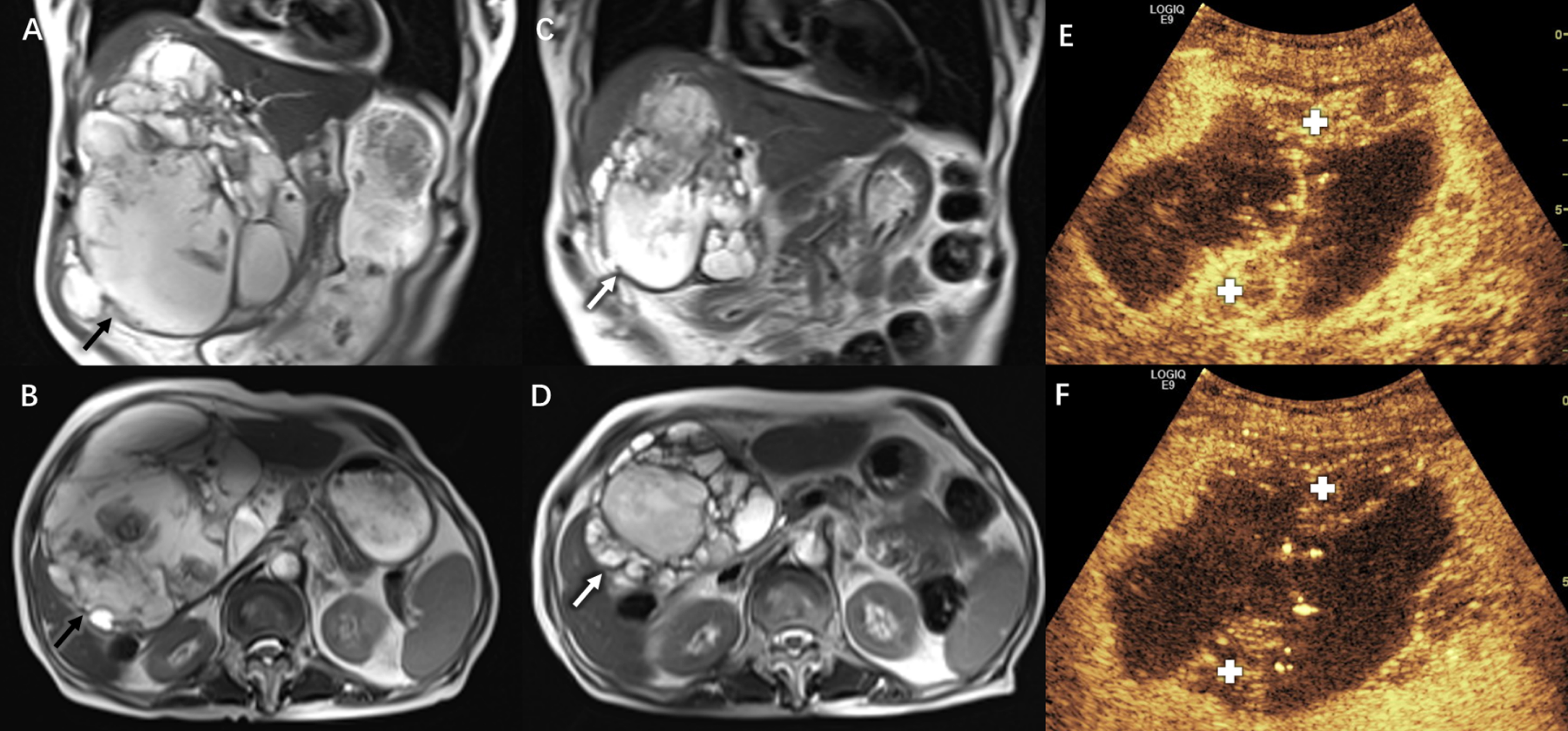
Pre-treatment MRI, post-treatment MRI, and post-treatment CEUS for the huge biliary cystadenocarcinoma. A. Coronal section of pre-treatment MRI in T2-weighted imaging (T2WI) shows the BCAC (black arrow) with mixed-signal, clear boundaries, thick sepatations, and cystic walls, which locates in the right liver. B. Cross section of pre-treatment MRI in T2WI. C. Coronal section of post-treatment (6-month after the first the operation) MRI in T2WI shows the volume of BCAC (white arrow) is significantly smaller than before the treatment (VRR was 70%). D. Cross section of post-treatment (6-month after the first operation) MRI in T2WI. E. 6-month post-treatment CEUS shows non-enhancement in most parts of the lesion in the arterial phase (15 seconds after injection), while viable tumor tissue (cross) is still observable which shows hyperenhancement. F. 6-month post-treatment CEUS shows non-enhancement in most parts in the portal phase (90 seconds after injection).
Reexamined MRI 6 months after the first treatment showed the huge tumor was significantly smaller than before, with a size of 91×85×112 mm and volume reduction rate (VRR) of about 70% (VRR = 1-current tumor volume/initial tumor volume). Biochemical tests in her reexaminations showed a marked improvement over the past 6 months (Table 1). Her psychological and physiological status improved significantly, scored 70 in KPS (Fig. 3).
The definition, clinical manifestation, and diagnosis of biliary cystadenocarcinoma
Intrahepatic BCA and BCAC are extremely rare cystic tumors originating from the intrahepatic bile duct, accounting for less than 5% of intrahepatic cystic masses [9]. According to previous studies, BCAC mainly develops as a benign lesion of BCA, which is usually more common in females [1]. The clinical manifestations of BCAC are similar to BCA and are usually associated with abdominal and digestive tract symptoms. Serum tumor markers such as CA19-9, CA12-5, carcinoembryonic antigen (CEA), and alpha-fetoprotein (AFP) may be elevated, while these markers lack specificity [10–14]. The diagnosis of BCAC usually depends on imaging examinations and usually presents as large multilocular cystic lesions with clear boundaries, internal sepatations, cystic wall nodules, and various properties of the cystic fluid [15–19].
Current treatment of biliary cystadenocarcinoma
Radical surgery is the most used treatment for BCAC at present, accounting for about 92.9% of all treatment methods. Other rarely used but reported treatment methods include fenestration, enucleation, marsupialization, liver transplantation, drainage, chemotherapy, and conservative treatment [6]. According to previous studies, the recurrence rate after resection is about 5.4% [9, 20–26]. Radical surgery to remove the tumor completely is the preferred method and is accepted by most patients. However, when the patient’s tumor is too large, the patient’s condition cannot tolerate traumatic surgery, and the patient seeks the least invasive treatment, appropriate methods other than conventional treatment to help them should be developed.
Ultrasound technique enables visualization of the normal and pathological changes of organs and tissues, which can be easily used for diagnosis, real-time operation guidance, and provide treatment of diseases. Ultrasound-guided ablative therapy and drug sclerotherapy can accurately destroy lesions without damaging surrounding organ structures under the guidance of real-time ultrasound. The commonly used ultrasound-guided ablation methods include radiofrequency ablation (RFA), MWA, cryoablation, laser ablation (LA), and chemical ablation, all of which have advantages and disadvantages and have been widely used [27–29]. The cryoablation applied in this case refers to the method of in situ inactivation of the tissue by rapidly cooling the diseased tissue with low-temperature technology to destroy the cells and cause cell necrosis or apoptosis. This method has no heat stimulation and has the advantages of lower discomfort and pain for patients during the operation [30, 31]. And MWA is a method to generate high temperature on the diseased tissue by using the thermal effect of microwave, which denatures the proteins, dehydrates the cell, and finally achieves tissue coagulation necrosis. It has the advantages of high power, high temperature, and high efficiency as thermal ablation [32–35]. Ultrasound-guided sclerotherapy of cysts also plays an important role in clinical practice. The main principle is that drugs act on endothelial cells such as cysts, leading to protein degeneration and endothelial cell death. Lauromarogol or absolute ethanol is generally used in the liver cyst, kidney cyst, ovarian cyst, lower limb varicose vein, hemangioma, and other diseases [36–38].
In this case, the patient was initially considered to be a liver cyst in the local hospital and futilely treated multiple times without a definite diagnosis. Firstly, she was diagnosed with BCA, while the possibility of malignant tumor should be considered based on her age, gender, imaging data (especially CEUS), tumor markers, etc. The result of the pathological biopsy also confirmed our suspicion that the patient was diagnosed with BCAC.
Considering the difficulty in curative surgery, the patient’s poor general condition (40 in KPS), and the requirement of minimal trauma, we chose sequential, multi-step, and minimally invasive methods for combined treatment of her disease. A total of once TAE, once cryotherapy, twice MWA, and multiple times cystic partial drainage and sclerotherapy were performed. Sclerification of lauromacrogol and fluid drainage resulting in a rapid reduction of intratumor and peritoneal pressure and prevent the production of cystic fluid, significant relief the abdominal distention of this patient. The ablation of the solid parts of the tumor inhibits the growth of the BCAC and makes it shrink continuously after the treatment. The combination of intra-cyst and intravenous antibiotics usage effectively treated the long-term repeated infection of the patient, greatly improved her psychological and physiological state, and significantly improved her life quality (70 in KPS). CEUS plays an important role in diagnosis, real-time assessment of ablation scope and post-treatment effect evaluation follow-up during the whole process as described in previous literature [7, 39].
We successfully reduced the huge BCAC tumor volume to 30% of its original size with various minimally invasive treatment methods in this case, which alleviated the patient’s pain and improved her general condition (scored from 40 to 70 in KPS). Radical surgery was still the first choice for the next treatment. After consultation, the hepatobiliary surgeon concluded that the patient was generally in good condition and could be treated with surgery after more detailed examinations. Considering their rejection of trauma surgery, we are communicating with her and her family and hope that she can undergo radical surgery.
This long-term sequential treatment is a bold attempt and is the first experience in the minimal invasive translative therapy of huge, unresectable BCAC. The combination of different treatment methods maximizes the therapeutic effect while minimizing the patient’s pain compared with TAE, MWA, or cryoablation alone. The key to the safety, success, and effectiveness of this combined treatment is to accurately evaluate the patient’s lesion and specific systemic condition before and after treatment, pay attention to symptomatic support treatment and apply various minimally invasive treatment methods. CEUS and enhanced MRI can clearly show the details of the blood supply of the lesion and play an important role in diagnosis, curative effect evaluation, and long-term follow-up.
In conclusion, progressive sequential thermal ablation in combination with sclerotherapy after a detailed evaluation is a new and successful translative therapy for this unresectable huge BCAC and poor general condition, making subsequent radical surgery or ablation possible.
Footnotes
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (Grant 81725008), Fundamental Research Funds for the Central Universities (Grant 22120190213), Shanghai Municipal Health Commission (Grants 2019LJ21 and SHSLCZDZK03502), and the Science and Technology Commission of Shanghai Municipality (Grant 19DZ2251100).
Conflicts of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.