
Abstract
Aims:
Anemia is common in the old and often observed in critically ill patients. Increased age is associated with higher mortality following a COVID-19 infection, making old patients prone to poor outcomes. We investigated whether anemia at admission to the ICU or the need for blood transfusion was associated with 90-day mortality in older, critically ill COVID-19 patients.
Methods:
In this prospective multicenter study, the 90-day mortality of COVID-19 patients≥70 years treated in 138 intensive care units (ICU) was analyzed. Associations between anemia (WHO definition) at admission and discharge from ICU and the use of red blood cell (RBC) transfusions with mortality were assessed. Hemoglobin thresholds of RBC transfusions in old, critically ill COVID-19 patients were recorded.
Results:
In 493 patients (350 anemic, 143 non-anemic), anemia (WHO definition) at the time of ICU admission was not associated with impaired overall survival. Transfusion and severe anemia (hemoglobin≤10 g/dL) at ICU discharge were independently associated with a higher risk of 90-day mortality.
Conclusion:
The need for red blood cell transfusions and severe anemia at ICU discharge, but not at the timepoint of admission, were independently associated with 90-day mortality in critically-ill old COVID-19 patients.
Introduction
The infection with SARS-CoV 2 can result in Coronarvirus disease 2019 (COVID-19), jeopardizing in particular the old [1], which are more prone to a severe course of illness [2]. Besides age, frailty and multimorbidity are both traits that are closely associated with mortality following COVID-19 [3–5]. Hence, the subpopulation of old, critically ill patients is particularly interesting in COVID-19-related studies [6, 7].
In an aging population, anemia (defined by WHO as Hb < 13.0 g/dL in male adults and < 12.0 g/dL in female adults) becomes increasingly prevalent, with over 10% of patients at 65 years of age or older [8, 9]. In critically ill patients admitted to intensive care units (ICU), anemia is distinctly common, occurring in nearly two-thirds of patients [10]. Due to the high prevalence, the management of anemia at admission, blood transfusion thresholds, and transfusion frequency are continuously under debate, as their use is associated with clinical outcomes [11–14]: several trials have investigated the implications of blood component substitutions, which were meant to counteract the negative clinical effects of anemia. In some settings, ICU patients receiving red blood cell (RBC) transfusions had higher mortality [15–17], whereas in other settings, a restrictive transfusion regimen proved to be non-inferior to a liberal regimen [10]. Therefore, current guidelines recommend a conservative blood transfusion regime. Of note, COVID-19 is associated with the activation of the endothelium [18] as well as plasmatic coagulation, which overall increases prothrombotic state [19, 20] and therefore may have an influence on transfusion regimens as well.
COVID-19 is associated with a high prevalence of anemia [21–23], and many patients with experience hematologic manifestations and side-effects [24, 25]. In hospitalized COVID-19 patients, reported RBC transfusion rates varied globally [26–28]; however, in some populations, RBC transfusions were given to more than 10% of patients [27, 28]. The impact of anemia on the outcome of COVID patients is uncertain and has led to divergent results [21–23]. In older patients (≥70 years old), due to the clustering of age, frailty, multimorbidity, and high prevalence of anemia, therapeutic algorithms for blood substitution products need to be developed to achieve the best possible outcome.
The current study aimed to assess the association of anemia at ICU admission and discharge as well as the use of RBC transfusions in relation to the mortality risk of old, critically ill COVID-19 patients.
Methods
COVIP study and population
The present work displays data from the prospective multicenter very old intensive care patients (VIP) project [3, 29]. The COVIP study (www.vipstudy.org) is supported and endorsed by the European Society of Intensive Care Medicine (ESICM), and it investigated in the first period COVID-19 patients≥70 years old admitted to 138 intensive care units (ICU) in 28 countries [3, 29–31]. Several coordinators supervised ICU recruitment, were responsible for obtaining local ethical permission, and supervised patient inclusion. Data presented in this work originates from subjects recruited from February 2022 until March 2023 with complete 90-day follow-up. Due to differences in legal and ethical regulations, several patients could be included in the study without informed consent. Additionally, patients in the current study were supported to enroll in further observational COVID-19 studies. Not enrolled but screened patients were not recorded. The study was registered on ClinicalTrials.gov (NCT04321265) and adhered to the European Union General Data Privacy Regulation (GDPR) directive, which is implemented in most participating countries. A detailed list of participating ICUs and the corresponding contacts are shown in SI Table 1.
Baseline characteristics of patients with initial anemia (WHO definition) at admission to the ICU
Baseline characteristics of patients with initial anemia (WHO definition) at admission to the ICU
In recruiting ICUs, patients≥70 years old and treated for a COVID-19 infection were eligible. A nasopharyngeal swab confirmed the infection with a SARS-CoV-2 polymerase chain reaction. The major objectives of this study were to investigate if 1) the association of anemia at ICU admission and discharge and 2) the transfusion rate during the ICU stay was associated with 90-day mortality rates. Anemia at admission was defined according to the World Health Organization (WHO), at 13 g/dL for men and 12 g/dL for women. Patients were classified with severe anemia when the hemoglobin (Hb) level was ≤ 10 g/dL (for both sexes). Additionally, the Hb transfusion trigger was assessed (provided by the treating physicians).
Patient characteristics were collected either by hand or by the standardized electronic case report form in a prospective manner, as previously described [32, 33]. Extended laboratory parameters besides Hb (such as creatinine, C-reactive protein, leucocytes, ferritin, or lactate) were not collected to accommodate a slim workflow during a pandemic. In addition, data collection included intubation/ventilation therapies, steroids, and vasopressor use. The precise SOFA score assessed disease severity during the first day in the ICU. The frailty status of the patients was assessed by the clinical frailty score (CFS), as described previously [3]. The clinical informational system or a follow-up call procured 30-day and 90-day mortality.
Statistical analysis
Demographic data are presented as means±standard error of the mean (SEM). Differences between the groups are investigated by unpaired t-tests (normally distributed data, as indicated by the Kolmogorov-Smirnov test) or Mann-Whitney test (non-normal distributed data). Survival is compared by the Kaplan-Meier estimator using the Log-rank (Mantel-Cox) test to assess 90-day mortality. The independent associations between anemia at admission or discharge and the use of red blood cell transfusions with mortality were assessed by Hazard-Ratios (HR) in Cox regression analyses adjusted for age and gender. Significance was assumed if p < 0.05. The statistical analyses were performed in STATA.
Results
Study population
Overall, 493 patients were included in this analysis. Of these, 350 initially presented with anemia, whereas 143 were non-anemic. Age was similar between the two groups. A higher proportion of male patients were in the non-anemic group (70% vs. 56%, p = 0.003). The complete baseline characteristics of the population are shown in Table 1 2. Patients presenting with anemia at admission and those without anemia received similar respiratory and vasoactive therapy during intensive care treatment (Table 1 2). The proportion of intubated and ventilated (p = 0.79), high-flow nasal oxygen (p = 0.68), and non-invasive ventilation (p = 0.21) was comparable in both groups as well as the use of vasoactive (p = 0.64) and corticosteroids (p = 0.28).
Baseline characteristics of patients with severe anemia (Hb ≤ 10 g/dL) at admission to the ICU
Baseline characteristics of patients with severe anemia (Hb ≤ 10 g/dL) at admission to the ICU
COVID-19 patients with anemia at ICU admission had similar 30-day survival as compared to non-anemic patients (40% vs. 40%, p = 0.97, respectively). Moreover, both groups had comparable survival rates 90 days after ICU admission (Fig. 1A, p = 0.41). If the patient population was stratified by the presence of severe anemia (Hb≤10 mg/dL) at the time of ICU admission, patients with an Hb≤10 mg/dL showed a trend toward higher 90-day mortality (Fig. 1B, p = 0.06), which remained not significant. Cox regression analysis showed that anemia at ICU admission was not independently associated with a higher risk of mortality within the first 90 days (HR 1.11, 95% CI: 0.83 –1.48, p = 0.47), even after adjusting for age and sex (HR: 1.13, 95% CI: 0.84 –1.51, p = 0.409).
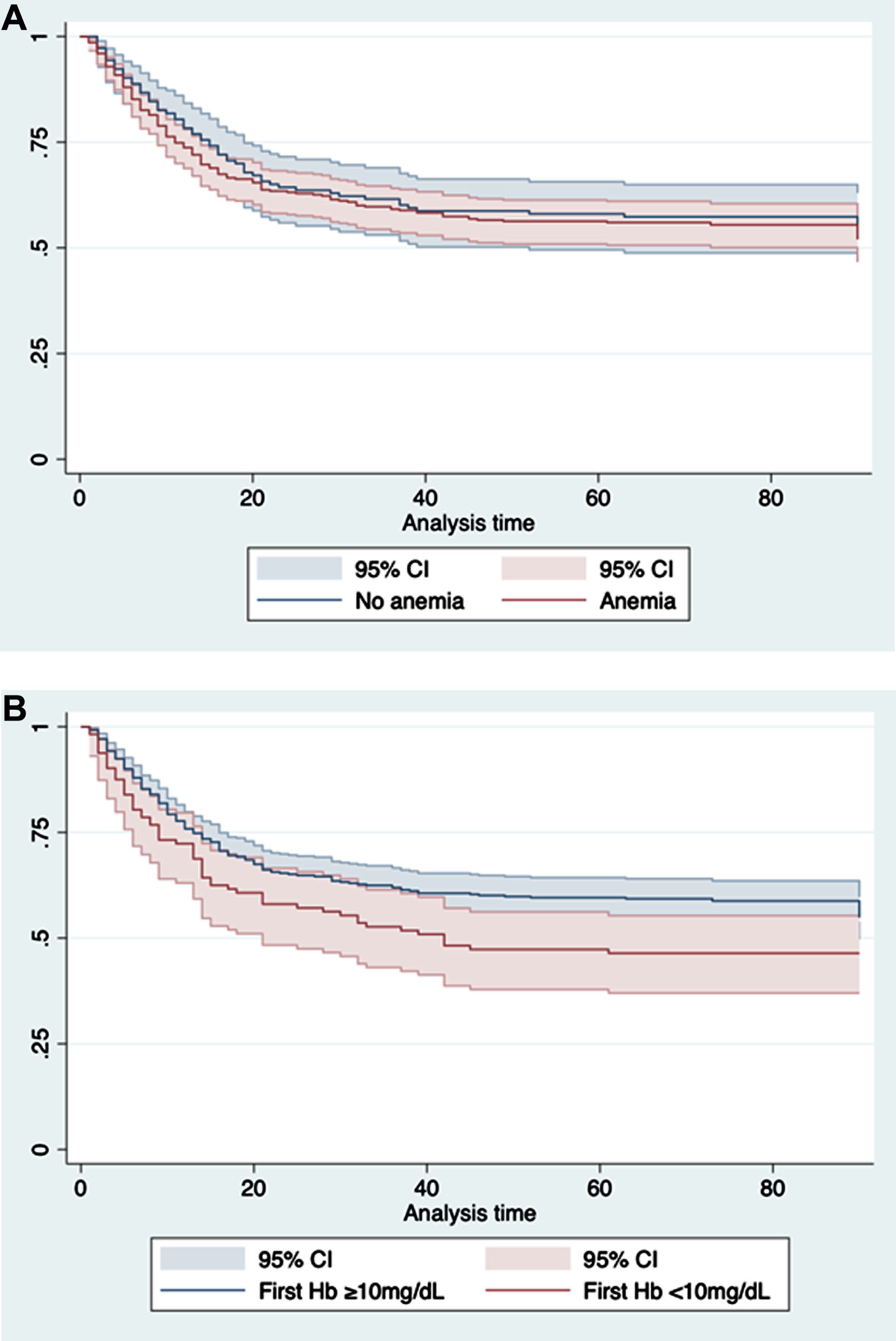
Anemia and severe anemia (Hb ≤ 10 g/dL) are not associated with a higher risk of mortality in elderly COVID-19 patients treated on the ICU. Kaplan-Meier curves representing 90-day survival of patients with initial anemia defined by the WHO classification (A) and severe anemia with a Hb≤10 g/dL (B). (A): Log-rank (Mantel-Cox) test p = 0.41; (B): Log-rank (Mantel-Cox) test p = 0.06.
About 20% of non-anemic and 14% of anemic patients received RBC transfusions during their ICU stay (Table 3). There was no significant difference in the proportion of anemic vs. non-anemic patients at admission receiving transfusions, however, their clinical outcome differed. Patients receiving RBC transfusions had a significantly higher 30-day mortality rate (76% vs. 55%, p < 0.001), which was consistent at 90-day follow-up (Fig. 2, p = 0.001). In the Cox regression model, RBC transfusions were associated with an HR of 1.67 (95% CI: 1.24 –2.25, p = 0.001), and after adjustment, aHR: 1.62 (95% CI: 1.2 –2.18, p = 0.001) with 90-day mortality.
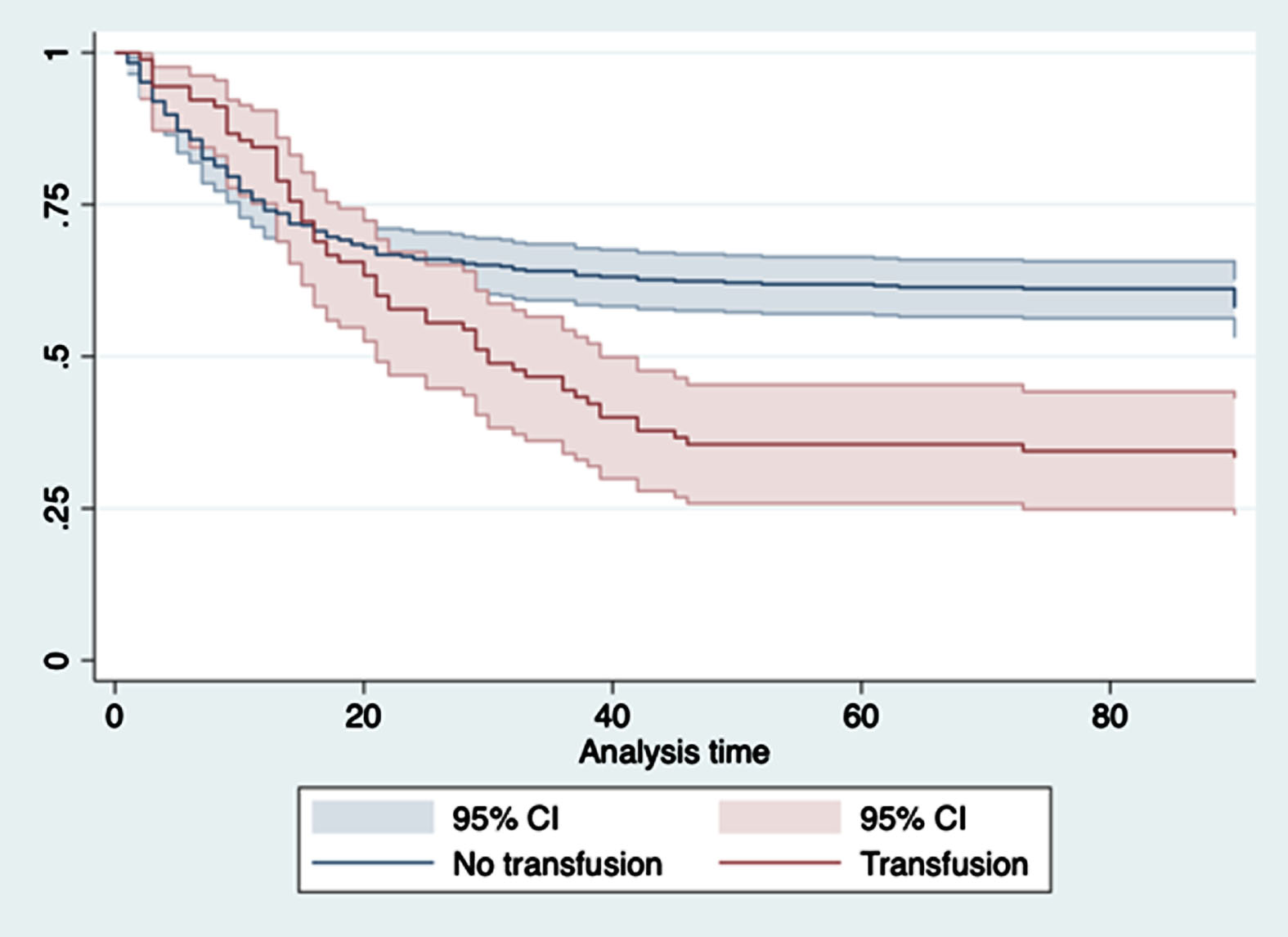
Red blood cell transfusions are associated with a higher 90-day risk of mortality. Kaplan-Meier curves representing 90-day survival of patients who received RBC transfusions vs. those who did not receive transfusions: Log-rank (Mantel-Cox) test p = 0.001.
Laboratory values and number of transfusions
In general, anemic patients receiving RBC transfusions had a higher 30-day mortality rate (59% vs. 42%, p = 0.004), which was a consistent finding at 90 days following ICU admission (Fig. 3, p < 0.001). In the Cox regression analysis, severe anemia increased the HR for 90-day mortality of 2.11 (95% CI: 1.53 –2.91, p < 0.0001), and after adjusting for sex, age, SOFA and CFS an aHR of 1.59 (95% CI: 1.07 –2.37, p = 0.0022).
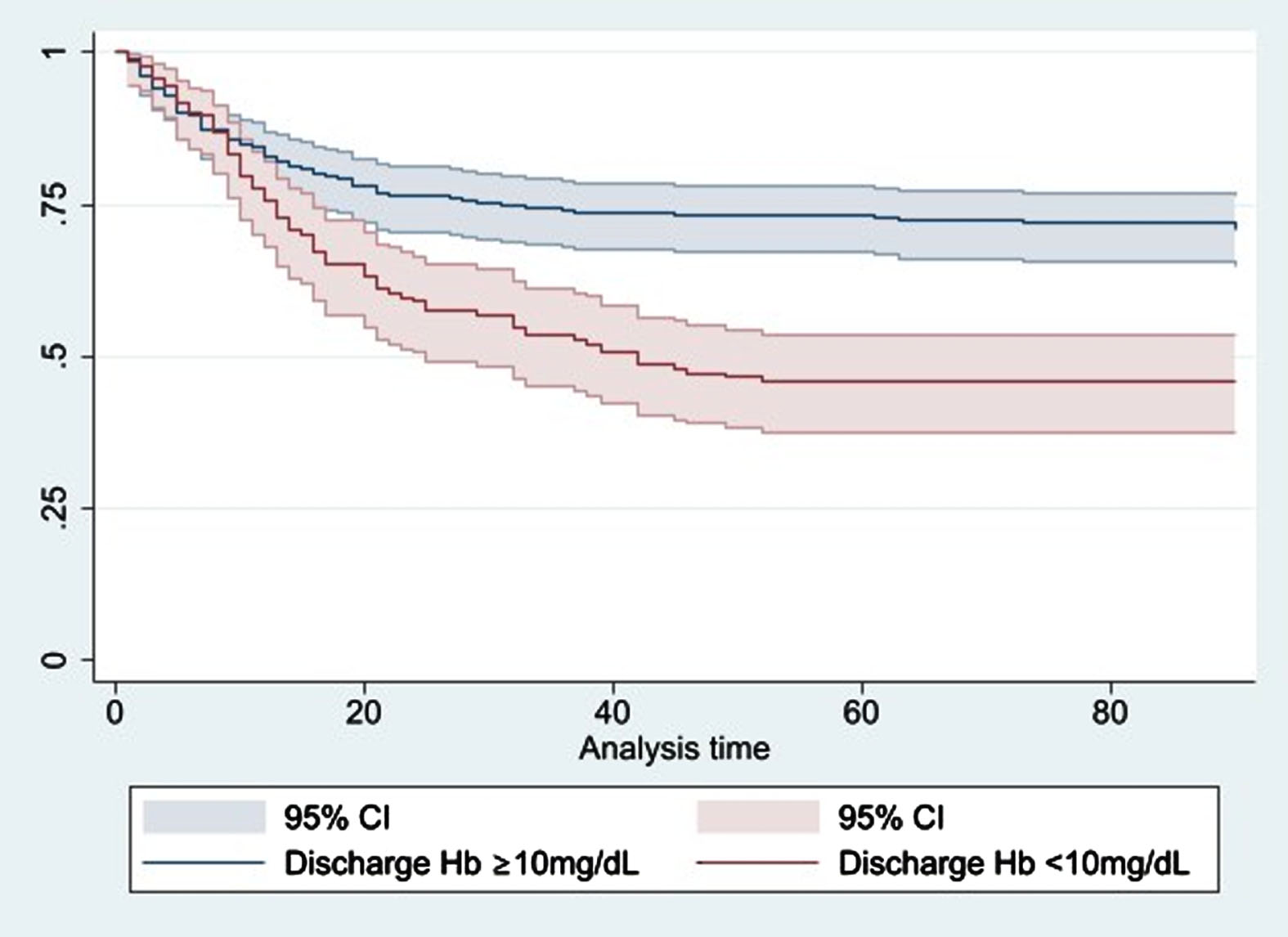
Severe anemia at discharge is associated with a higher risk of 90-day mortality. Kaplan-Meier curves representing 90-day survival of patients with severe anemia at discharge from ICU vs. those without severe anemia: Log-rank (Mantel-Cox) test p < 0.001.
The analysis of transfusion triggers set by intensivists in COVID-19 patients demonstrated a wide range of Hb thresholds. About one-quarter of transfusions were performed at Hb 6.9 –7 g/dL. The detailed list of transfusion triggers is presented in Table 4.
Hemoglobin thresholds considered triggers for RBC transfusion
Hemoglobin thresholds considered triggers for RBC transfusion
Cox regression analysis for the use of transfusions (model 1) and severe anemia at discharge (model 2) from ICU
Our study demonstrated a strong association between severe anemia at ICU discharge, and the use of RBC transfusions with 90-day mortality in old, critically ill COVID-19 patients. Interestingly, anemia at ICU admission was not associated with survival. Therefore, the interaction between anemia and COVID-19 in the context of increased age and multimorbidity is not well understood, which is reflected in a variety of Hb thresholds that were considered in our patients for red blood cell transfusion in the clinical setting.
Anemia in COVID-19 patients has been previously investigated in multiple studies [21–23]. Apart from its prevalence, anemias’ link to the outcome of COVID-19 patients remains uncertain, as some studies indicated an association of lower Hb levels with a higher risk of mortality [22, 23], while others did not come to the same conclusion [21]. A recent meta-analysis demonstrated that anemia was independently associated with a higher mortality risk in COVID-19 patients [34]. Nevertheless, the study included COVID-19 patients of all age groups, did not differentiate between anemia over course of time and did not consider specific risk groups. By contrast, our data showed that severe anemia at ICU discharge was associated with higher mortality in critically ill, elderly patients with COVID-19 (Fig. 4). While admission Hb values showed no direct relationship with clinical outcomes in our patients (Fig. 1), the inconsistent association of anemia during the ICU stay and at ICU discharge with mortality suggests complex, not yet fully understood interplay of COVID-19 hematologic manifestations and their consecutive role in patients’ survival. Interestingly, within this cohort, our data suggest that severe anemia at discharge from ICU has a more significant impact on 90-day mortality than frailty at admission. However, we and others have already demonstrated the prognostic relevant effects of frailty in elderly ICU patients [3, 35]. Furthermore, some studies suggests a relevant impact of immunesenescense on the presence and severity of anemia, which also might have an influence in old ICU patients [36]. Therefore, additional research is needed to understand the interplay of these conditions on individuals’ risk of mortality.
We found that COVID-19 patients receiving blood transfusions had a higher mortality risk during the first 90 days following ICU admission. A previous study reported that about 8% of all hospitalized COVID-19 patients received RBC transfusions, a rate which increased significantly (up to 48%) in the subpopulation treated in the ICU [37]. Since our comparison of transfused and non-transfused COVID-19 patients included only patients admitted to an ICU, we did not attribute the association of RBC transfusion with a higher mortality risk to a more severe disease course. However, considering the influence of anemia and RBC transfusions from a rheological point of view, an anemic state may have an advantage in morbid ICU patients with atherosclerosis, as a decrease in blood viscosity facilitates the regulation of blood flow [38, 39] and organ perfusion. RBC transfusions, with a sudden increase in blood volume and blood viscosity in poststenotic atherosclerotic regions, vascular areas may lead to a decreased oxygenation, possibly promoting infarcts, insults and thus adverse outcome [40].
Similarly, not only frailty but also age might play a role in the need for transfusions. A Korean study showed an overall transfusion rate of 8% in hospitalized patients. However, the rate doubled in COVID-19 patients older than 65 years [26]. In our cohort, the average age at admission was similar in transfused and non-transfused patients, and the Cox regression analysis was adjusted for age.
The prospective design of the present study facilitated the collection of transfusion triggers during the ICU course. Surprisingly, only approx. 25% of the transfusions were administered at a threshold value of Hb of 6.9 –7 g/dL, as recommended by current guidelines [41]. However, even the european society of intensive care medicine does not provide a recommendation for transfusion strategy in the elderly critically ill patients [42]. In this study, divergent Hb thresholds, augmented by the association between the use of transfusions and higher mortality, may reflect clinical uncertainties in the treatment algorithms of ICU physicians. Of note, we could not stratify between patients with and without hemodynamic alterations receiving blood transfusions, which might affect the need/decision-making for transfusion initiation. Since our data showed an association between severe anemia at ICU discharge and higher mortality, the question should be asked which of these patients should be subjected to a liberal transfusion regime. Future studies should expand our existing knowledge and, in particularly, investigate the entire clinical treatment course for the best possible care for patients.
The major advantage of our study was the patient’s cohort: among the whole spectrum of COVID-19 patients, critically ill and old patients are those with the suspected worst prognosis [3, 5], which makes the generation of evidence for appropriate treatment decisions in these patients of particular interest. The study did not target a specific risk group, but reflects an international diverse cohort, which increases the validity of our data [3].
Limitations
Several limitations must be mentioned: First, we did not differentiate between forms of anemia. Second, we did not record hemodynamic parameters. Hemodynamic alterations have affected the RBC transfusion trigger threshold. Third, while we investigated the quantitative association, no statement about the survivors’ quality of life could be assessed. This is due to our tight data entry, i.e. time-efficient data entry during the treatment period in order not to further stress the already overburdened resources of colleagues. Fourth, in our Cox regression analyses, we did not include additional variables (besides age and sex), which, however, might have affected the HR.
Conclusion
RBC transfusions and severe anemia at ICU discharge were associated with higher mortality rates in old, critically ill COVID-19 patients. Further studies should address the interaction between anemia (at several time points), RBC transfusion, and COVID-19 in the context of critical illness, particularly in the vulnerable subpopulation of old, frail COVID-19 patients.
Footnotes
Disclosures
SJS received grants and non-financial support from Reactive Robotics GmbH (Munich, Germany), ASP GmbH (Attendorn, Germany), STIMIT AG (Biel, Switzerland), ESICM (Geneva, Switzerland), grants, personal fees and non-financial support from Fresenius Kabi Deutschland GmbH (Bad Homburg, Germany), grants from the Innovationsfond of The Federal Joint Committee (G-BA), personal fees from Springer Verlag GmbH (Vienna, Austria) for educational purposes and Advanz Pharma GmbH (Bielefeld, Germany), non-financial support from national and international societies (and their congress organizers) in the field of anesthesiology and intensive care medicine, outside the submitted work. Dr. Schaller holds stocks in small amounts from Alphabeth Inc., Bayer AG and Siemens AG; these holdings have not affected any decisions regarding his research or this study.