
Abstract
OBJECTIVE:
To assess diagnostic capabilities of a modern handheld ultrasound device (HUD) for portal vein (PV) evaluation in pediatric patients and to verify if age, body mass index (BMI) and object depth correlate to imagequality.
METHODS:
45 patients (3.9 months– 17.9 years; 10.3 years±5.4) were examined using a HUD and cart-based high-end ultrasound system (HEUS). The intra-and extrahepatic PV was scanned using B-Mode and Color-coded Doppler sonography (CCDS). A five-point Likert scale was applied to evaluate image quality. Results were interpreted by two readers in consensus. Scores were compared between the scanners and correlated to age, BMI and skin-to-portal-vein-distance (SPVD). The influence on image quality and the difference between the two devices were analyzed using ordinal and Bayesian logistic regression models.
RESULTS:
≥4 points (mild or no limitations) were achieved by the HUD in 60% for B-Mode and 56% for CCDS. There was a statistically significant negative correlation between the image quality achieved by the HUD and the SPVD for B-Mode and CCDS. The effect of BMI and SPVD on having≥4 points differed significantly between the HUD and HEUS for B-Mode and for CCDS.
CONCLUSIONS:
Sufficient to excellent image quality for portal vein assessment in pediatric patients was achieved by the HUD except for the most deep-lying structures. Compared to HEUS, diagnostic performance of the HUD is lower, based on a negative correlation with object depth.
Introduction
Over the recent years, rapid evolution of ultrasound technology and modern solutions for safe data storage and transfer have allowed the use of HUDs for high-quality Point-of-Care Ultrasound (POCUS), further boosted by the COVID 19-pandemic [1–3]. Due to improvements in image quality and usability, HUDs can be integrated in daily patient care and have been so especially by non-radiologists [4]. The overall examination time at the bedside can be considerably reduced if a portable device is used [5]. HUDs are increasingly used in resource-limited settings without access to high-end imaging, such as in low-income countries [6] or in out-of-hospital settings, for example in road or air ambulances [7–9]. They have also been utilized in teaching programs at several institutions [3, 10].
Due to their body habitus, children are particularly well suited for ultrasound examinations. The lack of necessity of patient transport and sedation and the lack of radiation exposure are major advantages compared to other diagnostic tools used in pediatric imaging [11]. Ultrasound is the first choice and highly sensitive imaging technique for vascular abdominal imaging in the majority of children [11–13]. HEUS offering multimodal imaging allow a detailed and extensive morphological and functional sonographic evaluation. They are, however, expensive and often only available at highly specialized hospital wards [14]. Considering the issues of hygiene, mobility and accessibility especially in critically ill patients or out-of-hospital settings, a wired connection of the probe to the ultrasound unit can potentially limit the availability of sonographic examinations [15]. The development of increasingly powerful HUDs can overcome these restrictions [16–19]. In the ultrasound center conducting the study, a portable, pocket-size, lightweight scanner, Vscan Air [20] was used. This device combines the linear and convex probe providing high resolution in a wireless transducer and enables digital image transmission, for example via Bluetooth or WLAN. To our prior experience, Vscan Air offers sufficient to excellent image quality in the assessment of superficial vascular structures [21]. Research of our study group gave rise to the question, whether handheld ultrasound imaging of deeper body parts might show significant restrictions due to limited penetration and depth blur. To evaluate the diagnostic potential and limitations of a modern HUD in the assessment of deep vascular structures in a routine clinical setting, the PV was chosen as exemplary major abdominal vessel.
Methods
This single-center, retrospective study was focusing on the applicability of a modern HUD in the assessment of abdominal vessels using the example of the PV in children and adolescents in the context of everyday clinical practice and its possible correlation with patient sex, age, calculated BMI and SPVD. Consent to search for and retrospectively analyze images obtained by Vscan Air and HEUS at the participating ultrasound center had been approved by the local ethics committee (University of Regensburg, Nr. 23-3347-104). All performed examinations were part of the out- and inpatient care provided and were already available at the start of the study.
Patients
A total of 45 children and adolescents were included. All patients had been referred to the pediatric radiology division at our hospital between January and May 2023 and underwent routine standardized sonographic examinations of the abdomen, including the liver. No patient had been sedated. Following anthropometric measurements were carried out routinely: age, weight, height and the calculation of the BMI (in kg/m2) and BMI-for-age-percentile using the BMI4kids-calculator of the German Obesity Society. A BMI-for-age-percentile of 10–90 is defined as normal weight, of > 90–97 as overweight, of > 97–99.5 as obesity and of > 99.5 as extreme obesity, whereas a child with a BMI-for age-percentile of < 10 is defined as underweight. For the two infants of the cohort, the calculator was also applied to estimate the BMI; both showed normal height and weight in their recorded somatograms.
Ultrasound examinations
All patients were examined by a board-certified pediatric radiologist with more than 15 years of experience in sonography. Conventional cart-based ultrasound was performed in a standardized procedure, followed by the examination using the HUD. A HEUS (Resona R9, Mindray, China, or LOGIQ E9, GE Healthcare, USA), equipped with two curved array multifrequency transducers, was used (1–6 MHz, additionally 2–9 MHz for smaller children). Solely non-contrast ultrasound was carried out. All patients received a scan of the whole abdomen. Images were stored digitally in the Picture Archiving and Communication System (PACS) of the University Hospital Regensburg.
Patients were examined in supine position, with the right arm elevated if possible. Warm transmission gel was used for patient comfort. The liver was imaged via the inter- and subcostal approach, and both lobes documented in sagittal and axial planes. Organ size and contour, parenchymal echogenicity, texture and homogeneity as well as the vascular architecture of the liver were noted. Vascular anatomical variants were ruled out. The hepatic artery, hepatic veins, inferior vena cava and the intra- and extrahepatic PV were imaged by B-Mode, CCDS and PW-Doppler. Color Doppler function was adapted to venous flow using optimized gain and adjusted pulse repetition frequency. Shape and diameter, wall thickness, echogenicity of lumen and respiratory variability were observed. Direction of flow of the portal, splenic and superior mesenteric veins were documented, as the size of the spleen and absence of ascites. When the child was cooperative, liver elastography was performed. Afterwards, the gall bladder and bile ducts, pancreas and spleen were scanned, followed by the rest of the standardized abdominal examination.
Vscan Air CL (GE Healthcare, USA) is a battery-operated device consisting of a dual-headed probe. The integrated curved array transducer (2–5 MHz with center frequency of 3.3 MHz) was used. Additionally, the linear array probe (3–12 MHz with center frequency of 7.7 MHz) was applied in smaller children. The wireless scanner was WLAN-connected to a mobile iOS device, on which the corresponding function app had been installed. The battery of the HUD could be charged quickly on site using inductive charging. The obtained images were saved anonymously and password-protected on the used iOS device, in compliance with applicable data protection regulations. Using the HUD, the same examination procedure applying B-Mode and CCDS with adjusted Color flow for the PV was performed as described above. Spectral Doppler with quantitative measurements had not been available in Vscan Air at the time of the investigation. Elastography can currently not be performed by Vscan Air.
Rating score image quality
Image quality was assessed regarding detail and contrast resolution, penetration and clutter using a five-point Likert scale: 1 = no evaluation possible (e.g., in case of patient movement/crying or severe artifacts), 2 = major limitations of diagnostic evaluation (no reliable assessment), 3 = significant limitations of diagnostic evaluation but sufficient for a reliable assessment (e.g. due to significant depth blur), 4 = only mild limitations of diagnostic evaluation, 5 = excellent image quality without limitations. Obtained scores were documented in a proprietary Excel spreadsheet, also in compliance with the applicable data protection regulations.
Evaluation procedure
Data were evaluated and read in consensus off-line by two readers (one experienced with > 3000 examinations/year,>30 years of experience in sonography, DEGUM III Radiology; the other with > 500 examinations/year,>15 years of experience in sonography, board-certified pediatric radiologist) blinded to the examination date. Results gained of both scanners were compared. The skin-to-liver-capsule-distance (SLD in mm) and the longest distance from the skin to the main portal vein in the porta hepatis (SPVD in cm, as equivalent to object depth) were measured retrospectively in digitally stored images taken in the right intercostal plane.
Statistical analysis
Variables were summarized using absolute and relative frequencies, mean±standard deviation, median, range and interquartile range (IQR).
For comparison of the HUD and the HEUS, quality ratings were visualized with alluvial plots. For the comparison of different groups, we applied the non-parametric studentized permutation test by Neubert and Brunner [22]. Moreover, we fitted ordinal regression models with the ratings as dependent variables. Due to the small sample size, only two independent variables could be included in each model. We fitted Bayesian logistic regression models for only mild or no limitations (rating≥4) as dependent variable to analyze the influence of BMI, age and SPVD on the difference between the HUD and HEUS. To deal with quasi-complete separation, we used a weak normal prior (with standard deviation 3) on the fixed effects. The significance level was set to α= 5% for all statistical tests. Due to the exploratory nature of this study, no adjustment for multiple testing was applied. All analyses were performed with the statistical programming environment R (version 4.2.3; R Core Team (2023)) using the R packages ggalluvial (version 0.12.5) for alluvial plots, ggstatsplot (version 0.12.1) for box and bar plots, nparcomp (version 3.0; [24]) for the studentized permutation test, ordinal (version 2023.12.4) for ordinal regression models, blme (version 1.0.5) for Bayesian logistic regression models and ggeffects (version 1.3.4) for the visualization of the results of the Bayesian logistic regression models.
Results
45 patients were successfully examined. 20 were female (44.4%), 25 male (55.6%). Mean age was 10.3±5.4 years (0.3–17.9; IQR 5.9; 14.8). 39 had been diagnosed with hemato-oncological diseases, 6 with other diagnoses. No individual presented with status post liver transplantation and no primary or secondary liver tumors were noted. No hepatic vascular variants or anomalies including portal vein stenoses and portosystemic shunts were found. Patients had not been diagnosed with known or suspected liver cirrhosis. High-grade fibrosis was imaged in only one patient, a 7-year-old boy with clinically suspected Fontan-associated liver disease, presenting with severe parenchymal hyperechogenicity and F3-fibrosis stage using elastography. Mean SPVD was 8.34±1.50 cm (4.5–12.0 cm; IQR 7.5; 9.5) and mean SLD 12.4±4.1 mm (6.0–25.0 mm; IQR 10.0; 14.0). Mean BMI was 18.5±3.5 kg/m2 (14.0–29.4 kg/m2; IQR 16.2; 19.5). 33 patients were within the normal weight range, seven classified as underweight with a BMI-for-age percentile of < 10, four patients were overweight with a BMI-for-age percentile of > 90–97 and one obese with a BMI-for-age percentile of > 97. No patient was found to be extremely obese. Characteristics of the study population are presented in Table 1.
Demographic data of the study patients
Demographic data of the study patients
98% of examinations carried out with the high-end device were rated with ≥4 points using B-Mode and CCDS. Good to excellent image quality (≥4 points) was achieved by the HUD in 60% for B-Mode and 56% for CCDS; example images are depicted in Figs. 1–3. Significant limitations in image quality are illustrated in Fig. 4.
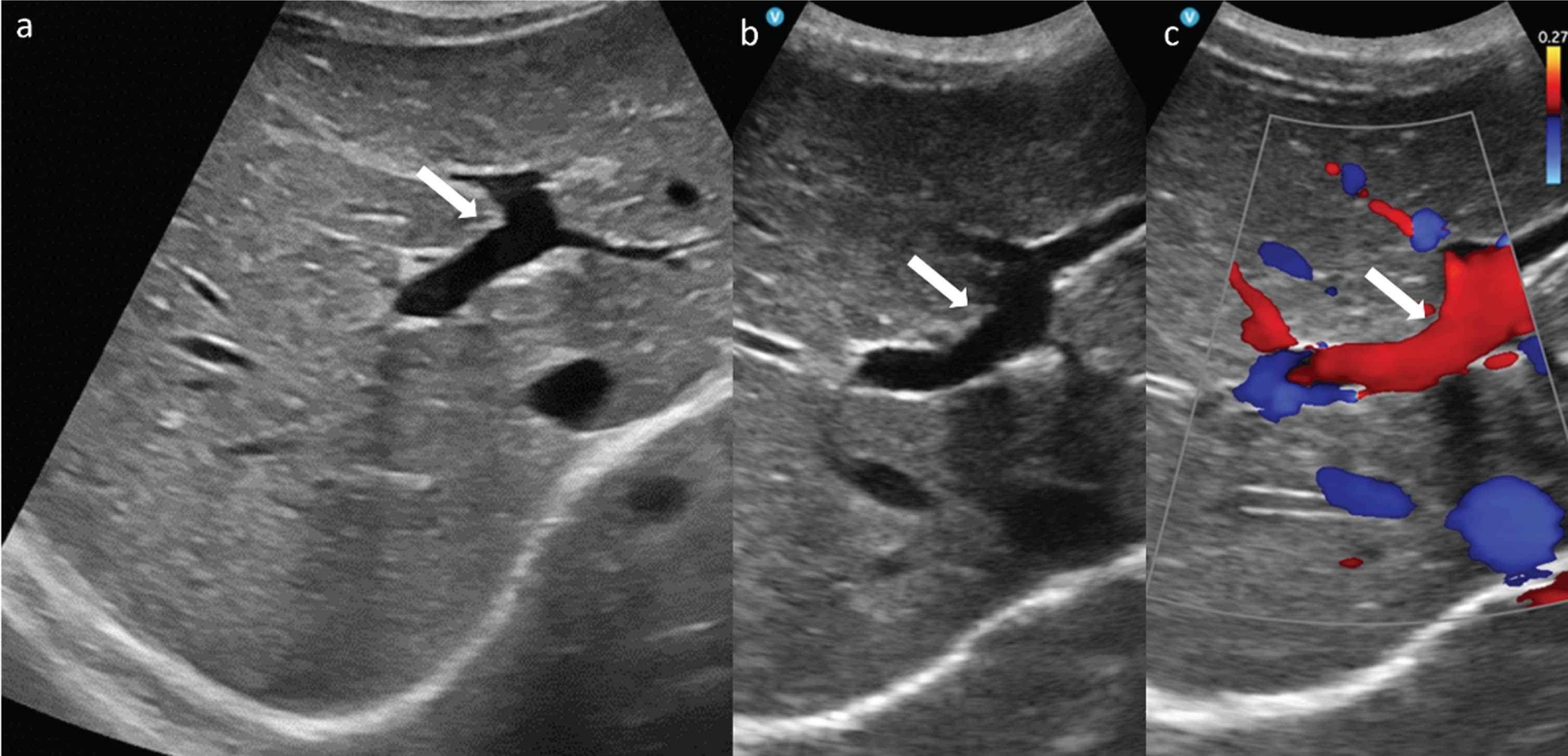
Intrahepatic PV (arrow) in 8-year-old boy depicted by the HEUS (a) and the HUD using B-Mode (b) and CCDS (c).
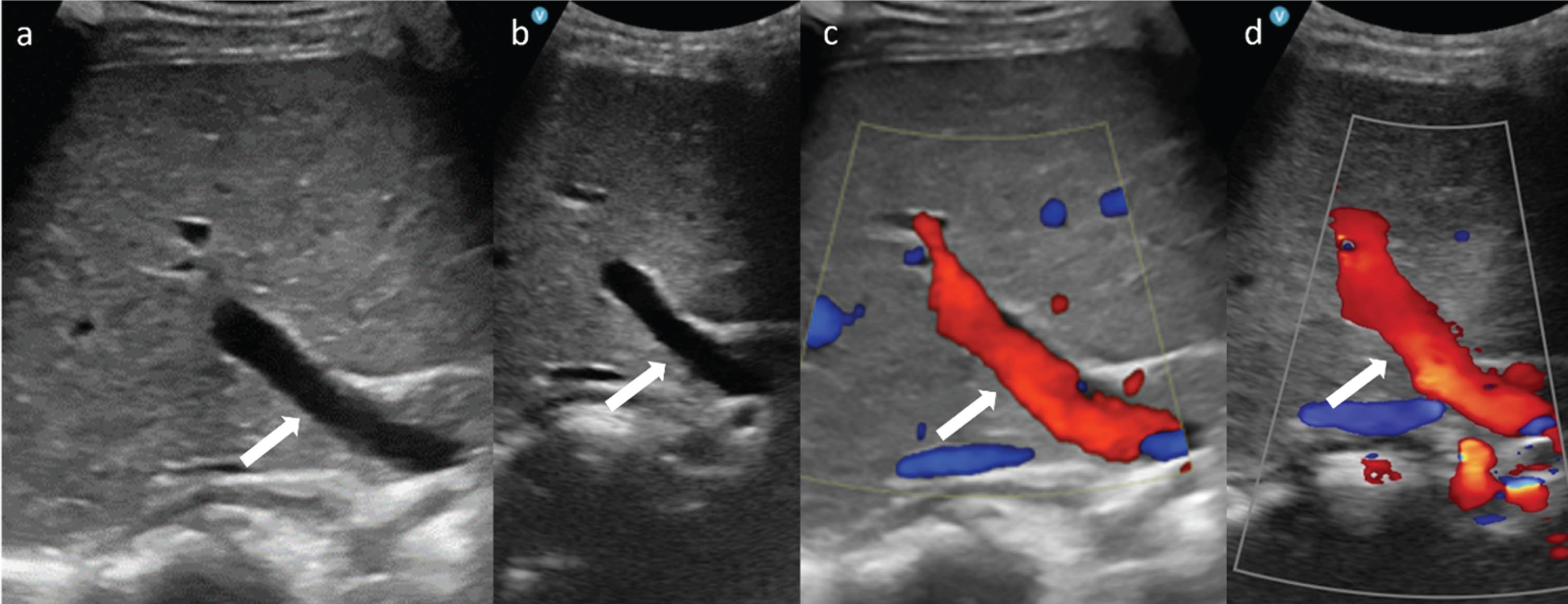
Main PV (arrow) in 5-year-old girl pictured by the HEUS using B-Mode (a) and CCDS (c) and by the HUD using B-Mode (b) and CCDS (d).
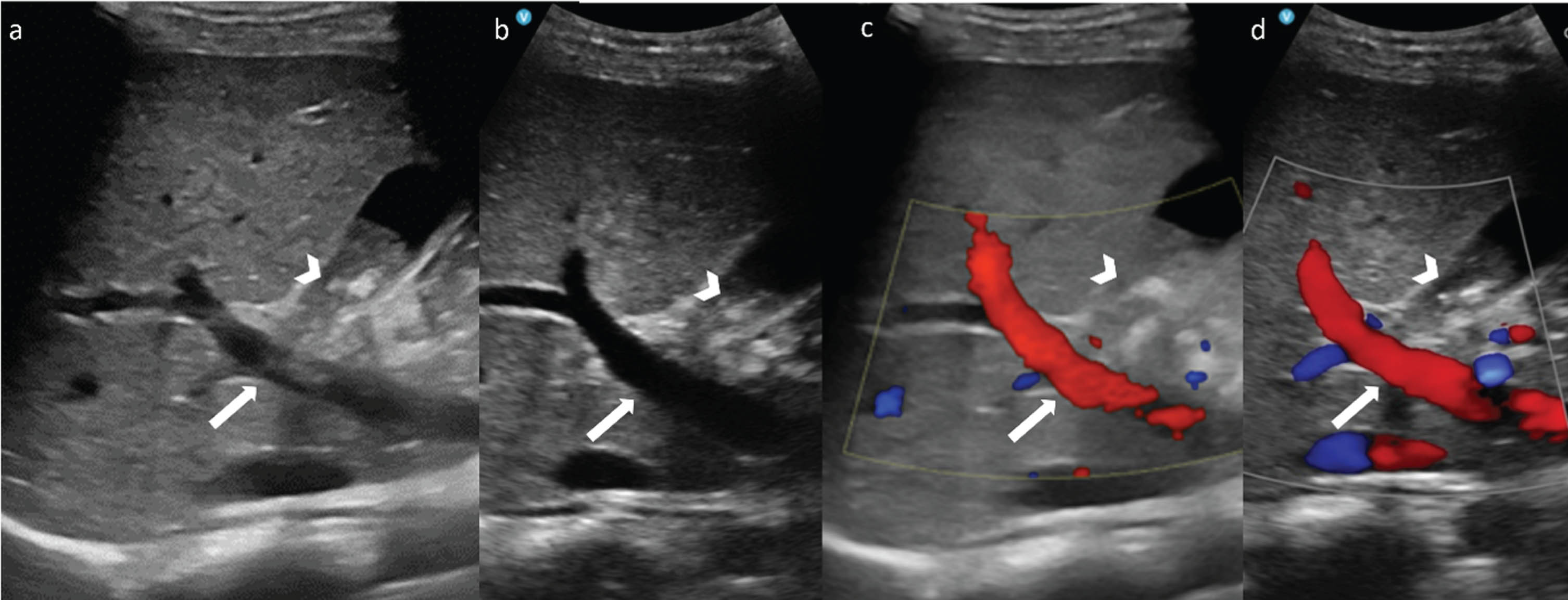
Main PV (arrow) in a 14-year-old boy with beta-thalassemia pictured by the HEUS (a + c) and by the HUD using B-Mode (b) and CCDS (d). Acoustic shadowing due to cholecystolithiasis (arrowhead), impeding assessability in the intercostal view.
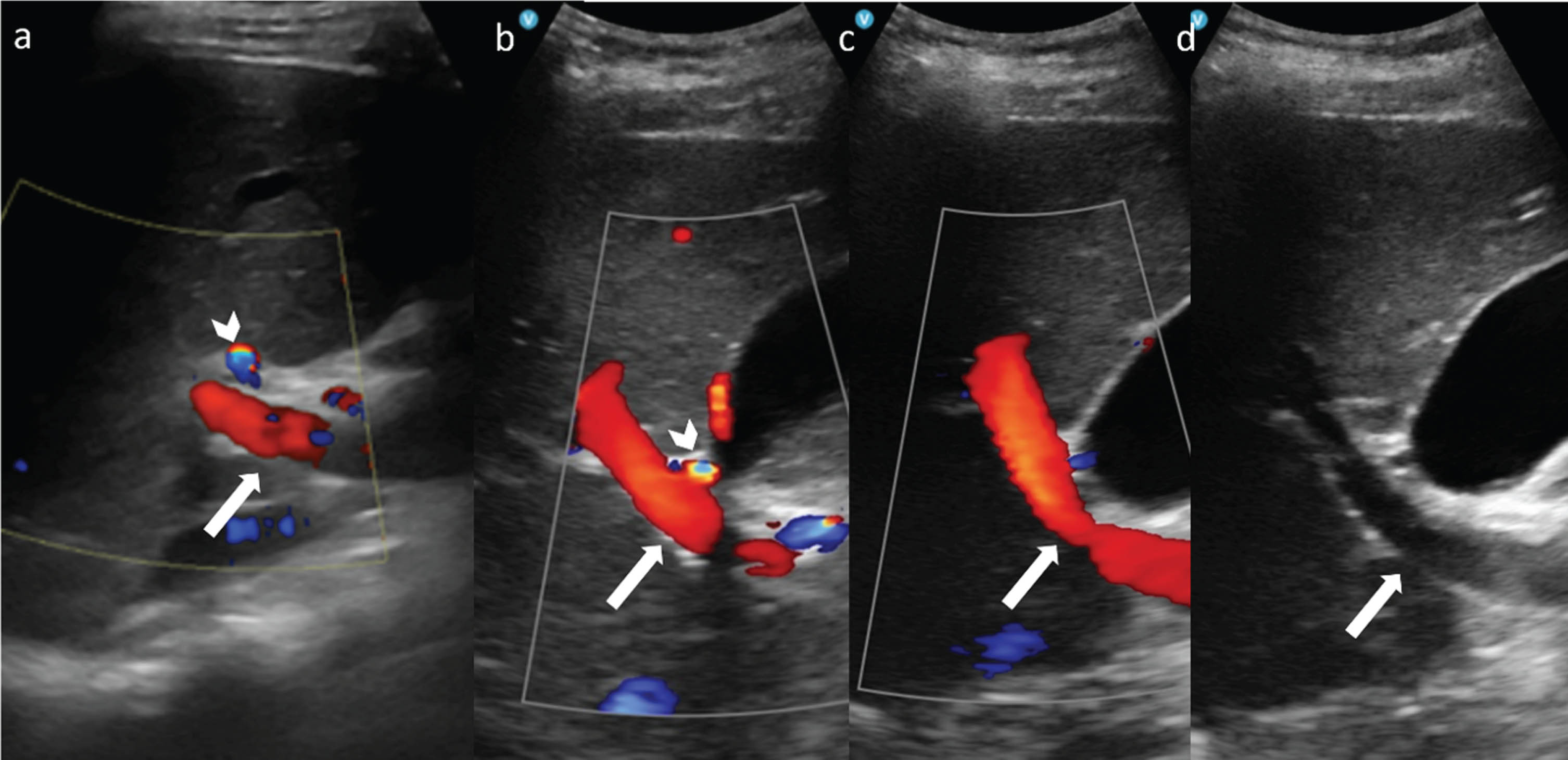
Restricted image quality in 17-year-old overweight adolescent. Main PV (arrow) pictured by the HEUS (a) and by the HUD using CCDS (b + c) and B-Mode (d). Note the hepatic artery (arrowhead).
No statistically significant difference between the assessed image quality in female and male patients was found regarding all assessed parameters (median rating 4 in the HUD and median rating 5 in the HEUS for all combinations of sex and mode), with the smallest p-value being 0.305. There was a statistically significant negative correlation between the image quality achieved by the HUD and the SPVD and BMI for B-Mode, as illustrated in Table 2. For CCDS, an ordinal regression model with both SPVD and BMI as independent showed a significant association with image quality for SPVD only (Table 2).
Multivariable ordinal regression models for the quality ratings with BMI and SPVD as independent variables for all combinations of device and mode
1 OR = Odds Ratio, CI = Confidence Interval.
Although the age parameter initially showed a significant correlation (Fig. 6), this could no longer be proven in the subsequent investigation models and can therefore be best described as a spurious correlation. With increasing age, BMI and SPVD increased, and the effects on image quality are better explained by the correlation with SPVD (Table 3).
Multivariable ordinal regression models for the quality ratings with age and SPVD as independent variables for all combinations of device and mode
1 OR = Odds Ratio, CI = Confidence Interval.
Individuals with the same image quality rating for B-Mode in both scanners had a significantly lower BMI and SPVD than those with worse rating results for the HUD. For CCDS there was a significant result for SPVD (p = 0.050) and a trend for BMI (p = 0.095, Fig. 6). Note that only five individuals had the same rating for CCDS.
The HUD showed insufficient image quality (2 points) in 2% using B-Mode and 11% using CCDS. No examinations were rated with a score of 1 (Fig. 5).
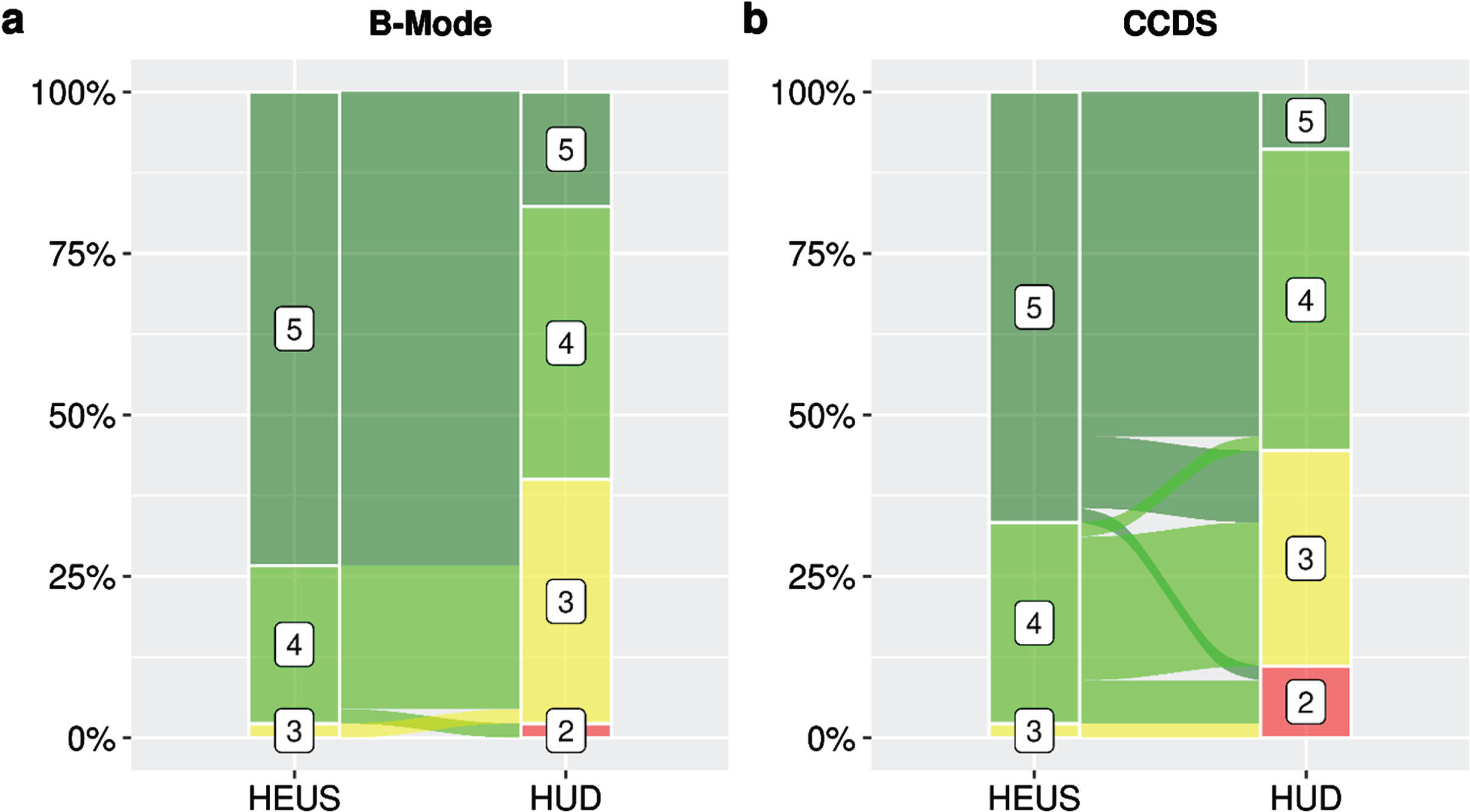
Alluvial plots for B-Mode (a) and CCDS (b) for the comparison of the quality ratings of the HUD and HEUS.
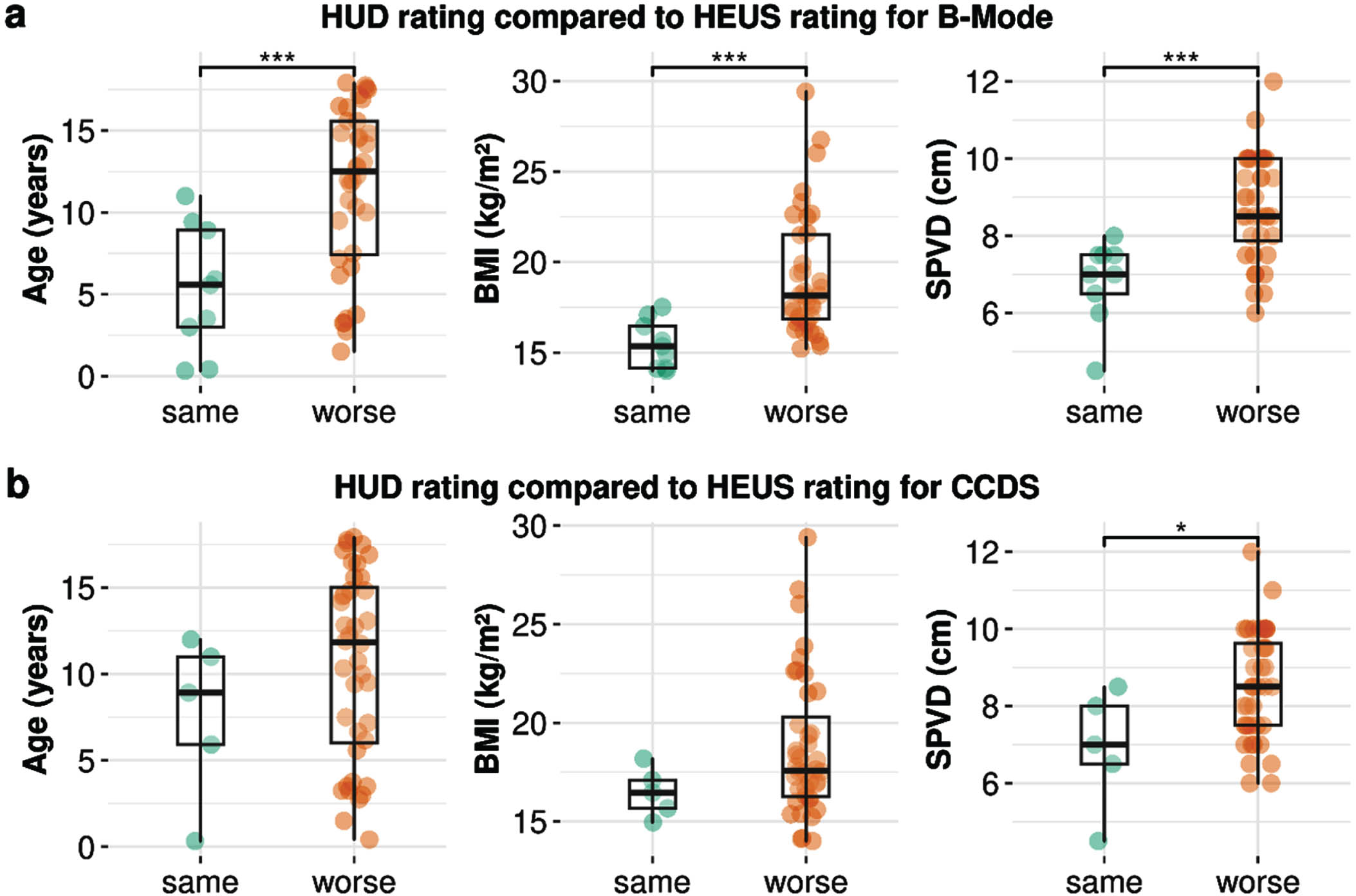
Boxplots for the comparison of age, BMI and SPVD between patients having the same rating in both scanners and patients with worse results for the HUD compared to the HEUS for B-Mode (a) and CCDS (b). *p≤0.05, ***p < 0.001.
The subgroup analysis for the comparison of quality ratings between patients having a lower or higher BMI than the median BMI and having a lower or higher SPVD than the median SPVD confirms the preceding analyses (Fig. 7).
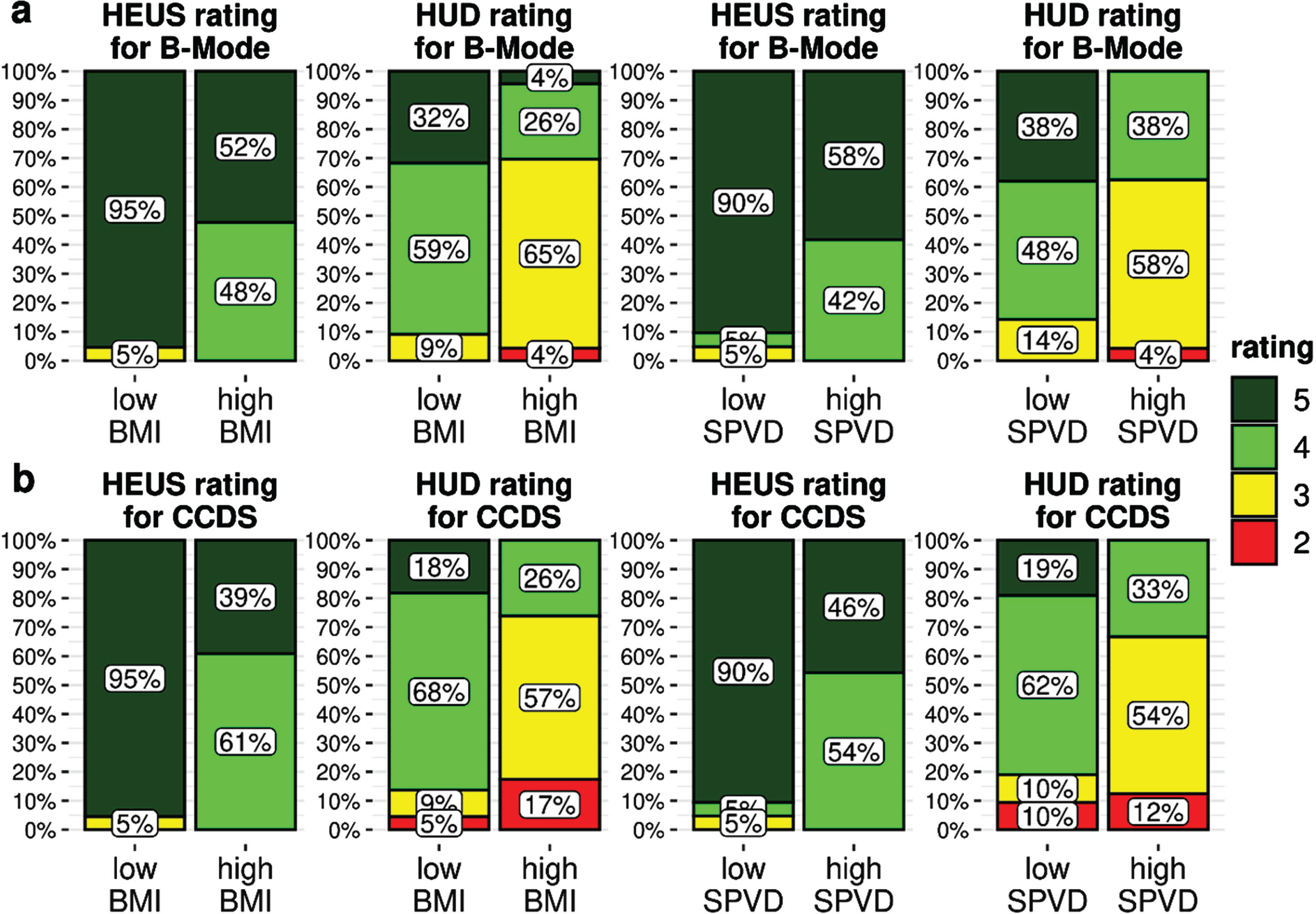
Bar plots for the comparison of quality ratings between patients having a BMI below or equal to (low BMI) or above (high BMI) the median (left-hand side) and between patients having a SPVD below or equal to (low SPVD) or above (high SPVD) the median (right-hand side), respectively, for B-Mode (a) and CCDS (b) and both scanner types.
Bayesian logistic regression models for B-Mode and CCDS showed that the chance of only mild or no limitations (rating≥4) is significantly lower for the HUD compared to the HEUS for patients having mean BMI (OR = 0.005, p < 0.001 and OR = 0.004, p < 0.001, respectively). The effect of BMI on having only mild or no limitations differed significantly between the HUD and HEUS (OR = 0.191, p = 0.005 and 0.209, p = 0.009, respectively). While there was no significant association between BMI and a rating≥4 for the HEUS: (OR = 1.004, p = 0.991, and OR = 1.045, p = 0.905, respectively), the chance of a rating≥4 using the HUD decreased considerably for a higher BMI. Predicted probabilities of B-Mode and CCDS rated≥4 for both devices are illustrated in Fig. 8 (Table S I). We obtained remarkably similar results for SPVD (Fig. 8, Table S II).
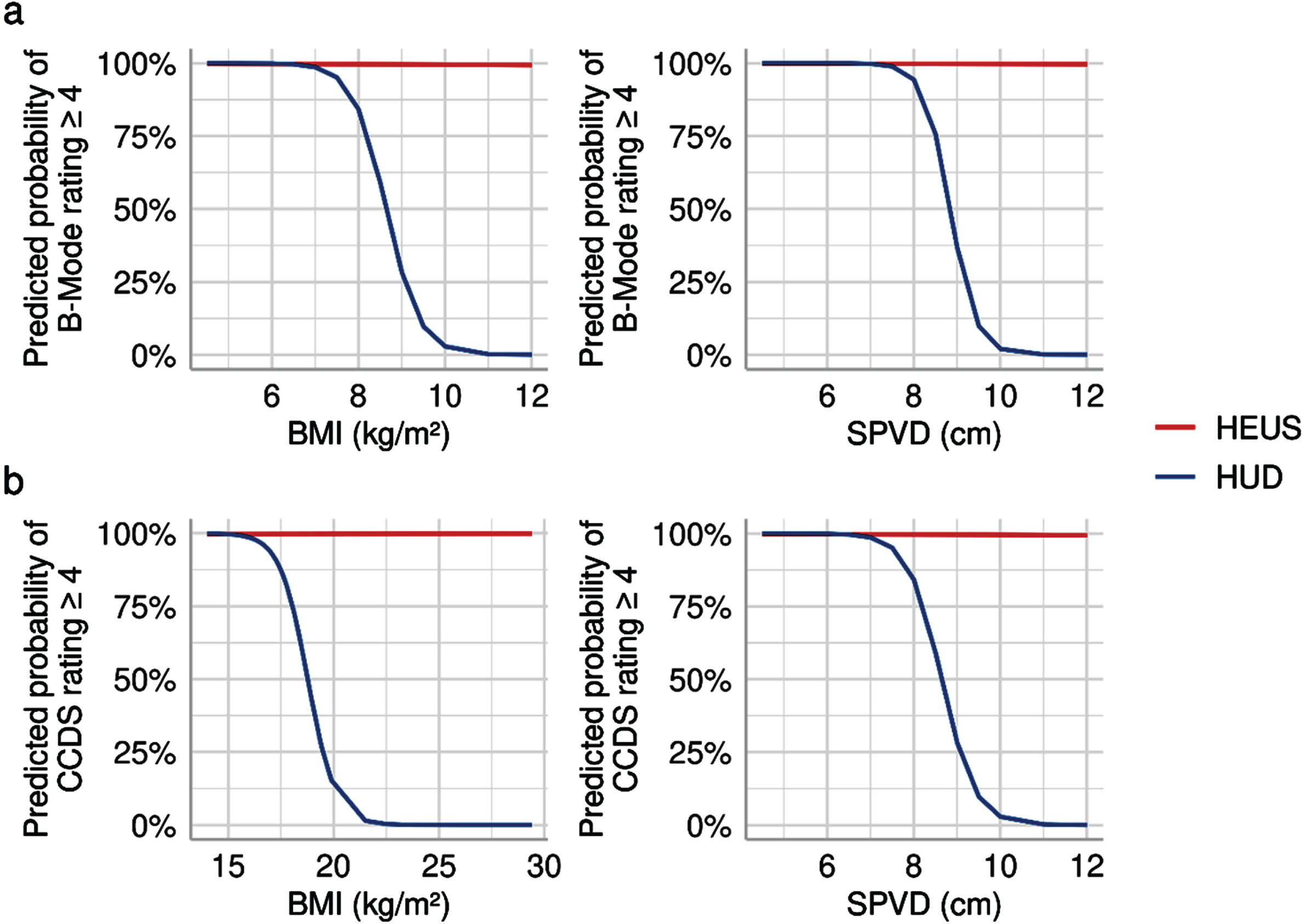
Visualization of the Bayesian logistic regression model from SI and SII (Supplement). The graphs show predicted probabilities of a quality rating≥4, i.e. only mild or no limitations, depending on the BMI (left-hand side) and the SPVD (right-hand side), respectively, for the HEUS (red) and HUD (blue) applying B-Mode (a) and CCDS (b).
Significant advances in mobile ultrasound technology have made HUDs versatile tools for POCUS across various fields including pediatric medicine and are being seen as future adjunct to physical examination [24, 25]. The problem of limited probe options, usually an important restriction on the use of mobile ultrasound technology in pediatric imaging, is being addressed by the dual probe design of Vscan Air, which was rated highest in a recent comparison of eight different types of HUDs regarding B-Scan quality and clinical significance [26]. Modern HUDs are equipped with more powerful batteries and offer improved frequency ranges and screen resolution compared to previous models. However spatial and temporal resolution are still lower compared to HEUS and in order to be of clinical value and to prevent ethical and juridical consequences for the user, HUDs need to reliably deliver diagnostic image quality. Relevant pediatric-specific data on the image quality provided by modern HUDs are scarce, and adequate quality assessment for pediatric POCUS is still lacking in many areas [27, 28]. To provide guidance and define possible limitations, several societies have issued recommendations on the use of HUDs for pediatric POCUS [1, 29–31].
To the best of our knowledge, this is the first study to evaluate diagnostic capabilities of handheld ultrasound for the assessment of the PV in pediatric patients. Reliable data on the maximum depth of the PV obtained by ultrasound in children and adolescents are missing. In our cohort the mean SPVD was 8.34±1.50 cm in the intercostal view. Our data show a significant influence of object depth, here expressed in the SPVD, on the image quality obtained by the HUD due to restrictions in penetration. Especially in depths of 9 cm and more, the probability of a low or insufficient image quality achieved by the HUD is higher than for the HEUS, as had been described before in adult patients [32]. Diagnostic capabilities of Vscan Air seem to be restricted in the evaluation of abdominal deep-lying vascular objects such as the portal vein in pediatric patients with greater body diameters.
Besides image quality, another prerequisite for the unrestricted use of HUDs in clinical routine is a secure image and video documentation. According to our experience, data transfer to and storage in PACS are central issues that still need to be resolved, in order for the devices to be used as adequate diagnostic imaging tools like cart-based systems.
This monocentric study is limited by the rather small number of patients and its retrospective design. Our results may not be generalizable to all pediatric patients. The correlation between the diagnostic performance of the HUD and liver fibrosis, a possible limiting factor in hepatic vascular imaging, has not been investigated; only one patient of our cohort presented with high-grade fibrosis. Furthermore, only one model of HUDs was used for this study, which at the time of investigation did not provide PW-Doppler and had offered only a small range of pediatric-specific presets. Very recently HUDs issued by various manufacturers have been updated with this important technique, extending the possibilities of mobile vascular ultrasound. Future directions of handheld ultrasound include the use of artificial intelligence to provide real-time coaching of image generation and interpretation[19, 33].
While the potential benefits of a modern HUD are undeniable in many areas of pediatric imaging, continuous and careful evaluation of possible limitations is necessary. Further studies on handheld vascular abdominal ultrasound with a larger number of subjects are needed.
Conclusions
Compared to HEUS, diagnostic performance provided by the HUD in portal vein assessment in children and adolescents is lower, based on a negative correlation with object depth and BMI. While the results are promising under adequate ultrasound conditions, dependence on object depth might potentially limit the use of handheld ultrasound for abdominal vascular POCUS in children and adolescents with greater body diameters.
Conflict of interest
The authors do not declare any existing conflicts of interest.
Author contributions
UK and BG wrote the original manuscript. FK carries out the statistical analyses. CS and EMJ reviewed the manuscript and supervised.
Funding
None.