
Abstract
BACKGROUND:
Extractable nuclear antigen (ENA) and anti-double stranded DNA (anti-dsDNA) positivity and related diseases like systemic lupus erythematosus, Sjögren syndrome, and other autoimmune diseases are known to be associated with obstetrical complications and poor perinatal outcomes.
OBJECTIVE:
To demonstrate the importance of ENA, anti-dsDNA, antiphospholipid (APL), and anticardiolipin (ACL) antibody positivity on pregnancy outcomes.
METHODS:
Ninety one pregnant women with known ENA, anti-dsDNA, APL IgG and IgM, and ACL IgG and IgM antibody positivity were retrospectively compared with 91 randomly selected pregnant woman in terms of obstetrical complications and pregnancy outcomes. Beksac Obstetrics Index-pregnancy (BOIp), calculated as (number of children
RESULTS:
Significant differences were found in the median maternal age, gravidity, number of previous miscarriages, and BOIp between the groups (
CONCLUSION:
We evaluated the impact of anti-dsDNA, ENA, APL, and ACL antibody positivity, which may cause immunologic inflammation at placenta and thereby affect pregnancy outcomes.
Keywords
Introduction
Extractable nuclear antigen (ENA) and anti-double stranded DNA (anti-dsDNA) positivity and related diseases like systemic lupus erythematosus (SLE), Sjögren syndrome, and other autoimmune connective tissue diseases (CTDs) are known to be associated with obstetrical complications and poor perinatal outcomes [16]. Further, positivity to antiphospholipid (APL) and anticardiolipin (ACL) antibodies (with and without syndromic findings such as antiphospholipid syndrome (APS)) most probably causes placental inflammation and is associated with poor perinatal outcomes as it leads to vascular/thrombotic problems and obstetrical complications [9, 26].
ENA, anti-dsDNA, ACL, and APL antibodies are widely used to initially detect autoimmune problems [5, 15, 29]. Subsequently, various complex antibodies are used to identify and describe the exact autoimmune disorders [15, 29]. Obstetricians aim to detect “autoimmune events” and prevent “immunological inflammation of the placenta” (maternal-fetal interface; mainly cellular structures of intervillous space and endothelial tissues of spiral veins) in order to reduce perinatal morbidity and mortality [2, 3, 19, 20]. It has also been reported that low-molecular weight heparin (LMWH), low-dose salicylic acid, and low-dose corticosteroids can be used to successfully treat pregnancies complicated by autoimmune disorders or/and chronic inflammatory diseases along with thrombotic events and inflammatory events [2, 3, 19, 20].
In the present study, we examined the association between positivity to these four autoantibodies – ENA, anti-dsDNA, ACL, and APL – and poor perinatal outcome in pregnant women. We also studied the effects of LMWH, low-dose salicylic acid, and low-dose corticosteroids on pregnancy outcomes in these cases.
Materials and methods
This retrospective study included 91 randomly selected normal deliveries (control group) and 91 deliveries with known maternal positivity to ENA, anti-dsDNA, APL IgG and IgM, and ACL IgG and IgM, with or without active maternal disease (study group). Thirty-nine patients from the latter group (42.8%) were nulliparous, while the remaining 52 (57.2%) were multiparous. All study group patients had tested positive for antinuclear antibody before positivity to more specific autoantibodies was detected. The study group were also screened for other autoimmune antibodies (anti-parietal antibody, anti-smooth muscle antibody, and anti-mitochondrial antibody), hereditary thrombophilia, methylenetetrahydrofolate reductase polymorphisms, chronic inflammatory diseases, coagulation disorders, anemia, and infectious diseases. Women who had miscarried or delivered infants before the 23
The study group patients were registered to a special antenatal care program. Necessary laboratory tests such as complete blood count; clinical urine test; and tests for blood sugar, liver function, C-reactive protein, complement components 3 and 4, activated protein-C resistance, anti-thrombin III activity, protein-S activity, lupus anticoagulant, and von Willebrand factor antigen were also conducted during this program. Patients with clinical symptoms were all treated in collaboration with the rheumatology department (hydroxychloroquine and patient-specific treatment were provided as necessary).
The patients were started on LMWH (enoxaparin; 2000 anti-Xa IU/0.2 ml), oral prednisone (4 mg methylprednisolone), and aspirin (100 mg acetylsalicylic acid) as early as possible after they were found to be pregnant. Pregnancy follow-up involved serial ultrasonography, aneuploidy screening (combined or triple test), fetal anatomy scanning at the 20–24
Obstetric and perinatal complications were analyzed in the study group. Preterm delivery was defined as spontaneous onset of labor before the 37
Autoantibody-positive patients were divided into two subgroups: (1) those that tested positive for only one and (2) those that tested positive for two or more antibodies. Maternal age, gravidity, parity, number of previous miscarriages, gestational age at birth, birthweight, APGAR scores, preterm delivery, IUGR, oligohydramnios, GDM, GHT, and stillbirth rates were compared between these subgroups.
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS, version 23). Data were presented as number, percentage, mean
Results
The demographic characteristics and clinical features were compared between all study patients (
Median, minimum, and maximum values of maternal age, gravidity, parity, number of miscarriages, number of living children, BOIp, obstetric outcomes and rates of some gestational risk factors and obstetric complications for the study and control groups along with p-values for comparisons between the study and control groups
Median, minimum, and maximum values of maternal age, gravidity, parity, number of miscarriages, number of living children, BOIp, obstetric outcomes and rates of some gestational risk factors and obstetric complications for the study and control groups along with p-values for comparisons between the study and control groups
Linear graph of the BOIp values for the study and control groups.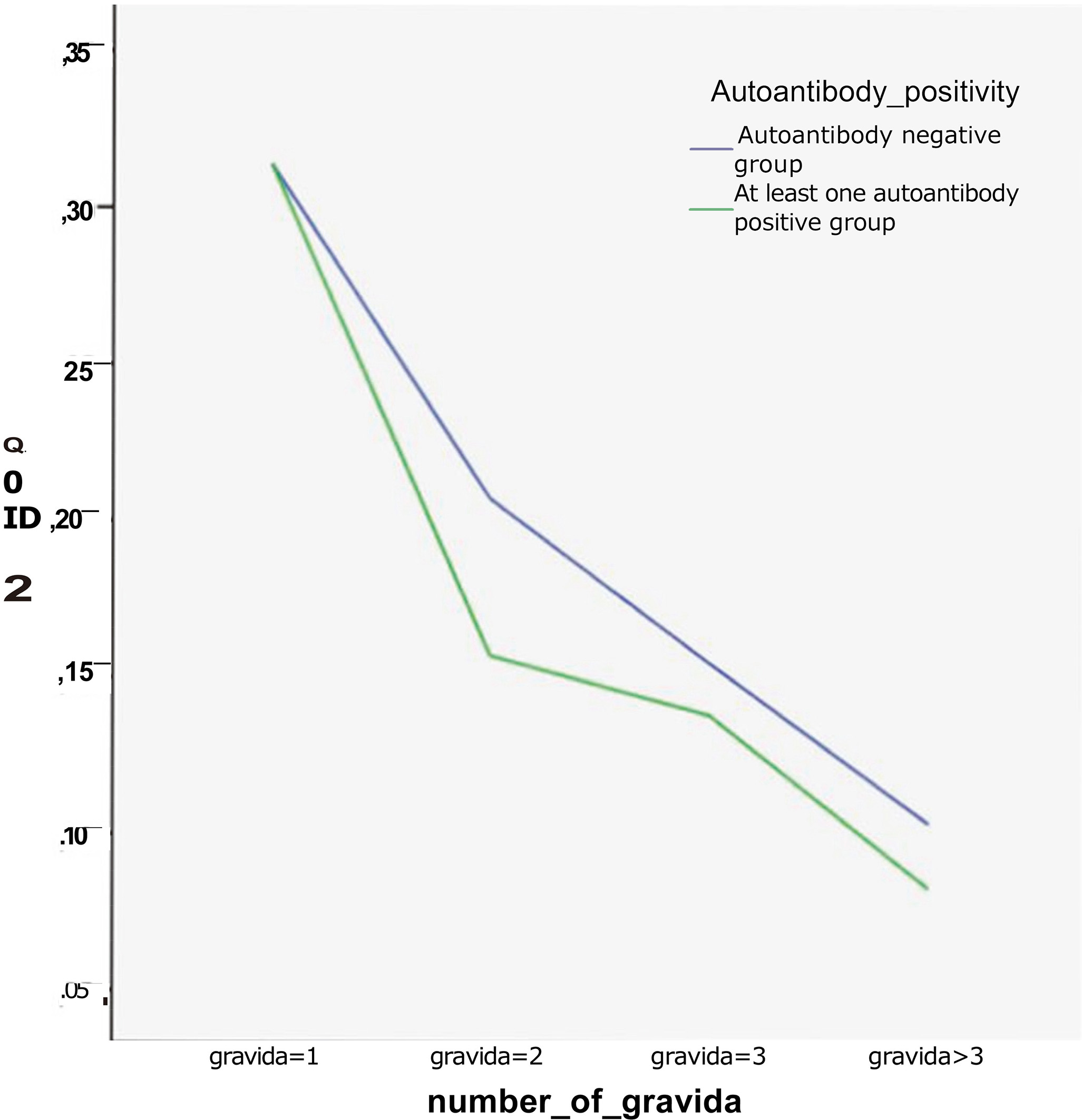
The median value of gestational age at birth for the study and control groups was 37 (27–39 weeks) and 38 weeks (32–41 weeks), respectively. Further, the median birth weight of the newborns was 2860 (800–3880 g) and 3270 (2010–4200 g), respectively, for the study and control groups. Finally, the median APGAR1 scores of the study and control groups were 9 (0–10) and 10 (5–10), respectively. Statistically significant differences were found between the groups in the median gestational age at birth, birth weight, and APGAR1 scores (
Maternal demographics and neonatal outcomes in the subgroups that tested positive for only one antibody and two or more antibodies
In the study group, 65 women tested positive for one autoantibody (71.4%), while the remaining 26 women tested positive for two or more (two in 22 [24.1%], three in 1 [1.1%], and four in 3 women [3.4%]). Table 2 shows the maternal demographic characteristics and neonatal outcomes for these subgroups. No statistically significant differences were found between the subgroups in terms of maternal age, gravidity, parity, number of miscarriages, gestational age at birth, birthweight, and APGAR scores. No significant difference was found between subgroups in terms of various obstetrical complications (Table 3). Although the rates of preterm delivery, IUGR, oligohydramnios, and GHT were higher in the two or more autoantibody-positive group, although these findings were not significant. GDM was detected in 7 of the 65 women who tested positive for one antibody (10.8%), and there were three stillbirths in this group. However, this finding was also not significant compared to those obtained for the other group.
Gestational risk factors and obstetrical complications
The placenta plays a key role in the gestational biological processes, and balanced maternal-fetal interaction is necessary to have a normal pregnancy [22]. Thus, a stable ambience in the intervillous space (maternal-fetal interface) and sufficient fetal perfusion are necessary for normal fetal growth [17]. Various immunological, metabolic, infectious, and epigenetic factors can affect the cellular components of the intervillous space (syncytiotrophoblasts, endovascular trophoblasts covering the tip of the spiral arteries, superficial and glandular epithelial cells of the decidua, endothelial cells of the spiral veins, etc.) and may cause obstetrical complications [2, 3, 19, 20]. Entry of cell debris in maternal circulation triggers inflammatory processes (and stimulates the maternal innate and humeral immune systems), which are most probably the main reasons for impaired fetal perfusion and intrauterine hypoxia [1, 7]. Syncytiotrophoblasts and endovascular trophoblasts with paternal tissue characteristics are important triggers for the maternal immune system [10, 11].
Immunological inflammation in the intervillous space structures due to autoimmune antibodies with or without related diseases/syndromes such as SLE, Sjögren’s syndrome, APS, Hashimoto’s thyroiditis, scleroderma, type-1 diabetes mellitus, rheumatoid arthritis, psoriasis, Addison’s disease, multiple sclerosis, inflammatory bowel disease, Graves’ disease, myasthenia gravis, vasculitis, celiac disease, and Behçet’s disease is associated with vascular/thrombotic disorders and obstetrical complications [2, 3, 19, 20]. Autoantibodies and/or disease-related inflammatory cytokines and cell debris (e.g., lysosomal enzymes) are most probably responsible for destruction of the cellular components of the intervillous space and the endothelial tissues of the vascular structures of the placenta (mainly, the spiral veins that supply blood to the intervillous space) [12, 16].
In the present study, we retrospectively evaluated pregnant women who had tested autoimmune antibody positive prior to becoming pregnant and who delivered at our hospital. We selected anti-dsDNA, ENA, APL, and ACL antibody-positive patients, which are widely used autoimmune markers of injury to endothelial cells of the vascular structures of the placenta and obstetrical complications [14, 18]. We focused on autoantibodies rather than specific autoimmune diseases, since these are better markers to demonstrate the association between immune system problems and pregnancy outcomes.
Anti-dsDNA antibody is the most commonly used antibody for the diagnosis of SLE [13, 23]. SLE is a disease affecting multiple organs with circulating autoantibodies of complex specificities [6, 30]. In contrast, tests for ENA antibodies establish a diagnosis of autoimmune CTDs in patients with indicative clinical features [8, 28]. Both these antibodies are disease specific and directed against nuclear or cytoplasmic antigens.
ENA and anti-dsDNA positivity and the related maternal diseases (SLE, Sjögren’s syndrome, and other CTDs) are known to be associated with obstetrical complications and poor perinatal outcomes [16, 21]. However, the generally reported sensitivities and specificities for the diseases associated with ENA and anti-dsDNA antibodies are based on a large body of literature that is difficult to interpret because the studies are heterogeneous in terms of design, subject population, and the methodology [8, 28].
APS is an another immunopathological condition that most probably causes placental inflammation and is associated with poor perinatal outcomes, vascular/thrombotic problems, and maternal complica-tions [9, 26]. APL screen IgG is an ELISA-based screening test for the quantitative determination of IgG antibodies against cardiolipin, phosphatidyl serine, phosphatidyl inositol, phosphatidic acid, and cofactor beta-2-glycoprotein I in human serum or plasma. This test is for the serological detection of primary and secondary APS [25, 27]. On the other hand, anti-phospholipid IgM antibodies against the same antigens also serve the same function [24, 25]. Similarly, IgG and IgM ACL antibodies are also used to diagnose or screen for APS and vascular thrombosis [24, 27].
In addition to its antithrombotic effects, LMWH also has anti-inflammatory effects and has successfully been used to manage high-risk pregnancies and autoimmune disorders [2, 3, 19, 20]. Low-dose corticosteroids are also used for immune disorders during pregnancy in order to prevent obstetrical complications and improve pregnancy outcomes [2, 3, 19, 20]. Salicylic acid is another therapeutic agent used in pregnancies to improve the outcomes, especially in women with autoimmune disorders [2, 3, 19, 20].
In this series, we evaluated the effect of LMWH and low-dose corticosteroids and salicylic acid on pregnant women with anti-dsDNA, ENA, APL, and ACL antibody positivity with or without active disease. All patients were enrolled in a special follow-up program prior to becoming pregnant, and we started them on LMWH (enoxaparin; 2000 anti-Xa IU/0.2 ml), oral prednisone (4 mg methylprednisolone), and aspirin (100 mg acetylsalicylic acid) as early as possible after they became pregnant. Although the study group was under treatment, statistically significant differences were found between this group and the control group in terms of the median gestational age at birth, birth weight, and APGAR1 scores (
In conclusion, we found that anti-dsDNA, ENA, APL, and ACL antibody positivity had unfavorable effects on pregnancy outcomes, despite treatment with LMWH and low-dose corticosteroids and salicylic acid.
Footnotes
Acknowledgments
Special thanks to all the perinatology division staff who work with devotion for the treatment of high-risk pregnancy patients.
Conflict of interest
All authors state that they have no conflict of interest in this study.