
Abstract
A risk factor relationship exists between periodontal disease and Alzheimer’s disease (AD) via tooth loss, and improved memory following dental intervention. This links the microbial contribution from indigenous oral periodontal pathogens to the manifestation of chronic conditions, such as AD. Here, we use Porphyromonas gingivalis infection to illustrate its effect on mental health. P. gingivalis infection, in its primary sub-gingival niche, can cause polymicrobial synergy and dysbiosis. Dysbiosis describes the residency of select commensals from the oral cavity following co-aggregation around the dominant keystone pathogen, such as P. gingivalis, to gain greater virulence. The initial process involves P. gingivalis disturbing neutrophil mediated innate immune responses in the healthy gingivae and then downregulating adaptive immune cell differentiation and development to invade, and subsequently, establish new dysbiotic bacterial communities. Immune responses affect the host in general and functionally via dietary adjustments caused by tooth loss. Studies from animals orally infected with P. gingivalis confirm this bacterium can transmigrate to distant organ sites (the brain) and contribute toward peripheral and intracerebral inflammation, and compromise vascular and microvascular integrity. In another study, P. gingivalis infection caused sleep pattern disturbances by altering glial cell light/dark molecular clock activity, and this, in turn, can affect the clearance of danger associated molecular patterns, such as amyloid-β, via the glymphatic system. Since P. gingivalis can transmigrate to the brain and modulate organ-specific inflammatory innate and adaptive immune responses, this paper explores whether better management of indigenous periodontal bacteria could delay/prevent the onset and/or progression of dementia.
MAKING A CASE FOR PERIODONTITIS AS A RISK FACTOR FOR ALZHEIMER’S DISEASE
Alzheimer’s disease (AD) is the most common example of dementia, constituting 60–80% of all dementias, and the healthcare costs associated with the management of individuals with this condition keeps rising [1]. Unfortunately, the pathogenesis of the disease remains an enigma. There is no adequate treatment or prophylaxis for the disease at present. The solution rests on prevention, or finding an effective treatment for AD.
To this end, Baumgart and colleagues [2] reported on the mission of the newly formed World Dementia Council and outlined the key challenges of tackling dementia. One key priority is to examine the modifiable risk factors that influence the development of dementia [2]. A risk factor relationship between periodontal pathogens/periodontal disease and AD exists, as previously discussed by Olsen and Singhrao [3]. Salient points are that periodontal disease is co-morbid with clinically demented subjects [4–7]. Tooth loss in early and mid-life has consequences for poor memory in later life [4, 7–12]. A prospective longitudinal study reported by Ide et al. [7] upholds the view that periodontitis is associated with a marked increase in cognitive decline, which is independent of baseline cognition, in men with a mild to moderate clinical diagnosis of dementia. A study following the impact of a dental intervention on patients with a clinical diagnosis of mild AD found over 50% of participants (who also suffered from gingivitis/periodontitis) showed improvements in their memory [6]. Oral bacteria and their virulence factors affect the central nervous system pathology [13, 14], and indiscriminate release of inflammatory mediators cause neuronal injury [5, 15–17]. The host’s humoral responses to periodontal pathogen infections are ineffective, but if combined with other tests, they may prove useful as predictive biomarkers of AD [18–20]. The failure of Baumgart et al. [2] to recognize these facts prompted a response in the form of a letter to the Editor by Kamer et al. [21]. We also lend our support to recognize periodontitis as a risk factor in the context for AD pathogenesis [21] and provide further laboratory based research evidence from rodent brains infected with Porphyromonas gingivalis(P. gingivalis).
While the aging process is associated with an increased likelihood of periodontitis [22] and dementia, their onset is by no means inevitable. Just as some individuals fail to progress beyond gingivitis [23], others retain cognitive functioning throughout their life [24, 25]. Individuals who retain cognitive functioning in later life also show a low lifetime risk for cancer, diabetes, cardiovascular disease(s) [26, 27], and possibly periodontitis. Oral bacteria are associated with diverse pathologies, which are often co-morbid with AD (Fig. 1) as described elsewhere [28]. As periodontitis is an easily manageable risk factor for a number of conditions, we argue that reducing the incidence of periodontal disease is a preventative measure for numerous health benefits in later life.
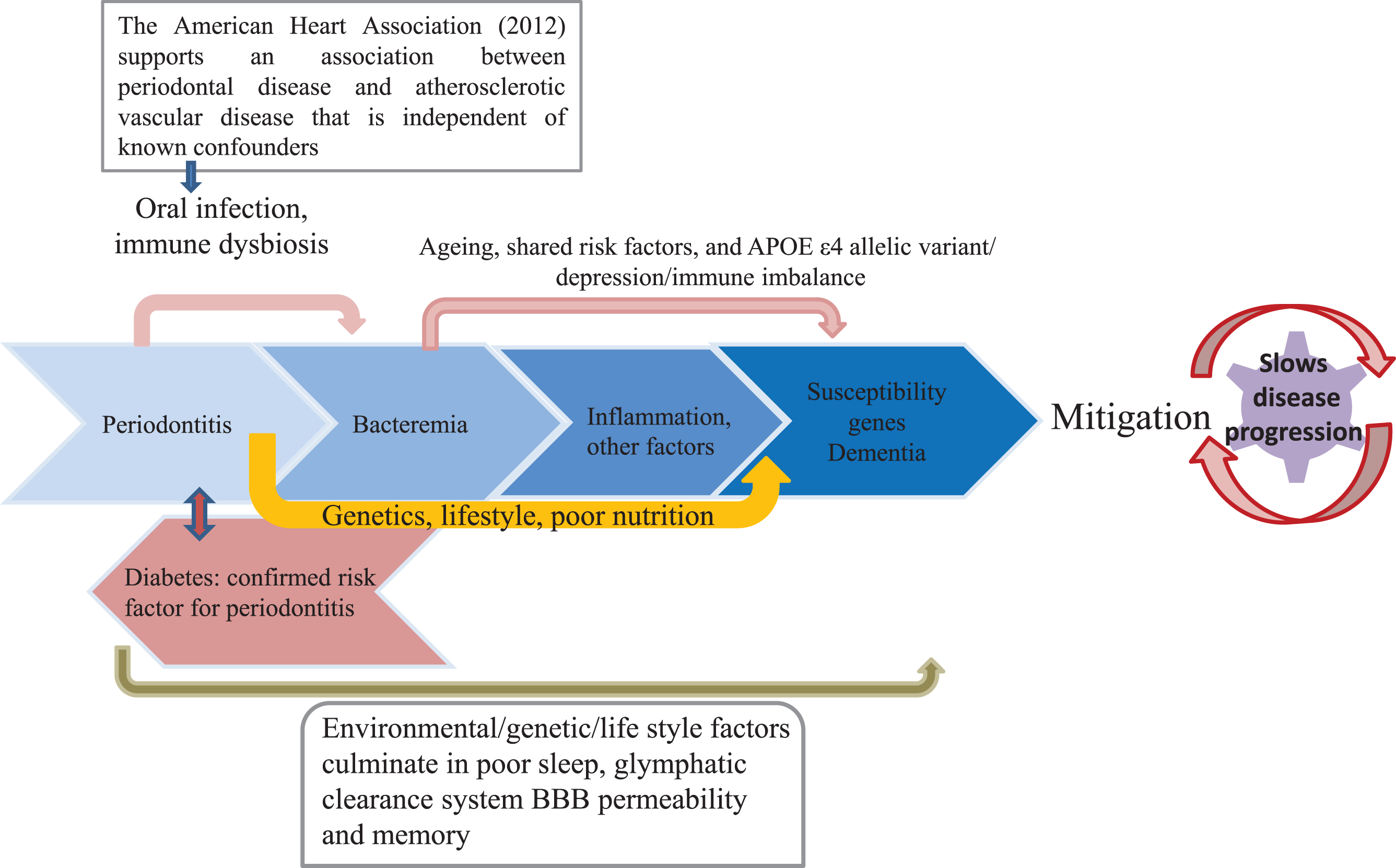
Schematic to show knock-on effect from an oral condition such as periodontitis to the development of mixed pathologies in the order of periodontal disease, cardiovascular, and AD with input from metabolic disorders like type 2 diabetes. The arrows point to major risk factors with plausible effect on each condition. Mitigation of poor lifestyles are modifiable with dental intervention potentially slowing down/preventing these related conditions.
PERIODONTAL DISEASE
Periodontitis describes a chronic polymicrobial infection in which P. gingivalis represents a keystone pathogen [29] and initiates dysbiosis [30] for nutritional dependency and imparting greater immune armamentarium to sustain the newly developing microbial communities in the sub-gingival niche. Until recently, it was acceptable to relate P. gingivalis interactions with specific species of bacteria, for example, those belonging to the red complex (Treponema denticola and Tannerella forsythia) [31]. However, to explain periodontal disease pathology, Hajishengalis and Lamont [30] have revised this view into a polymicrobial synergy and dysbiosis model. Hajishengalis and Lamont [30] propose that several hundreds of bacteria identified from the oral cavity (the oral microbiome, http://www.homd.org) all have the potential to subvert immune defenses, and overcome protective host barriers by gaining greater virulence from the keystone pathogen in the susceptible host. This process is like a form of bacterial radicalization where seemingly inert species co-aggregate, while dwelling in the oral cavity. Co-aggregation of P. gingivalis with Streptococcus gordonii is a typical example of how synergy between local commensals and a keystone pathogen may be possible [32]. Taken together these newly armed, select communities of bacteria with greater virulence can impair the host’s immune surveillance, and tip the balance from homeostasis to dysbiosis [30].
Periodontitis consistently shows progressive destruction of gingival connective tissue and adjacent alveolar bone [3, 29]. The initial gingival epithelial cell breach is the result of P. gingivalis being able to infect and survive within neutrophils that normally survey the gingival health [33]. The transient disablement of inflammatory signaling pathways attenuate neutrophil recruiting chemokine, interleukin 8 (IL-8), and cause imbalance of T cell IL-17 levels [34]. These changes promote local dysbiosis and therefore increase local inflammation, which is beneficial for selection and survival of the most resilient inflammophilic dysbiotic species within that oral niche [33, 35]. The oral bacterial/virulence factor will then transmigrate to the AD brain, with neuroinflammation as an obvious outcome [14]. Already disturbed adaptive immune responses, as is apparent from the host suffering from periodontal disease [34], will give rise to oral pathology. Marsh et al. [36] have verified the role of adaptive immune cells in the immune-deficient transgenic AD mouse model (Rag-5xfAD). This report confirms that adaptive immune cells in an immune-sufficient host (control animals) help to restrain both neuroinflammation and accumulation of amyloid-β (Aβ) protein [36], suggesting organ specific hallmark pathology can develop in the immunosuppressed vulnerable host.
The suggested association between periodontal disease and AD relies on several key observations. First, there are significant correlations between the rate of cognitive decline and measures of periodontal disease progression, such as pocket depth, alveolar bone loss, and tooth loss [37]. Currently, the relevance of newly identified risk factor, cognitive deficit for periodontitis [8], is more difficult to measure and pinpoint. We have suggested an explanation following our studies performed in the P. ginigivalis mono-infection model of periodontal disease in apolipoprotein E knockout (ApoE-/-) mice (see section on blood-brain barrier below). Future research will undoubtedly highlight a better understanding of the pathophysiology of poor memory development in relation to the human form of periodontitis.
ALZHEIMER’S DISEASE
AD is a neurodegenerative disease characterized clinically by generalized loss of numerous markers of social values. Of major interest here are irreversible memory loss and sleep pattern disturbances [38–41]. Pathologically, the presence of significant numbers of two specific microscopic lesions (extracellular Aβ deposits, and intracellular hyperphosphorylated tau protein coated neurofibrillary tangles) is critical to AD diagnosis. Major risk factors for AD include aging, and genetic susceptibilities [42]. Co-morbid states include cerebrovascular strokes [43–45] with and without diabetes [46, 47]. The salient environmental factors, which can increase AD onset, include physical injury and peripheral infections [48] (Fig. 2).
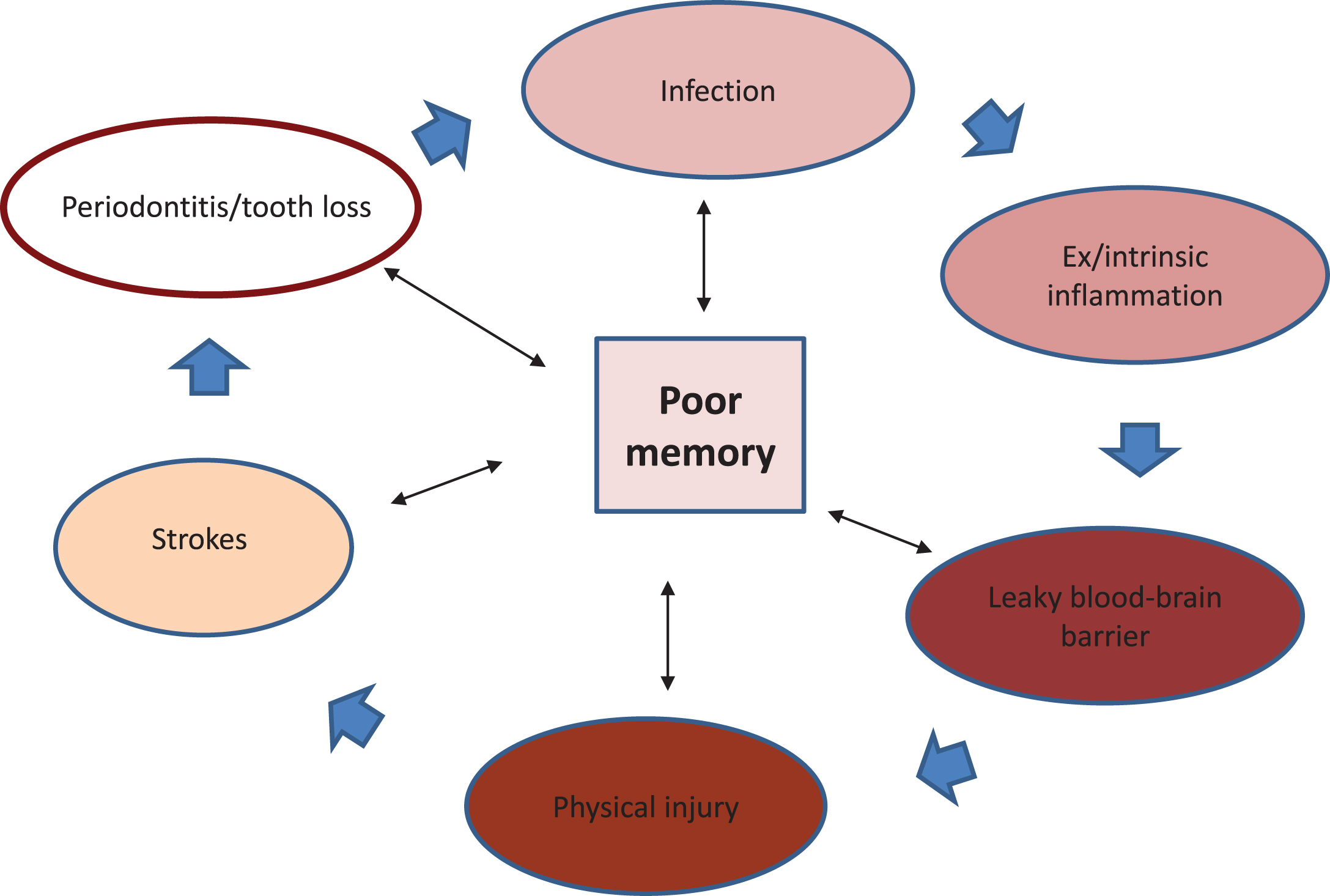
Schematic shows the relationship of various pathologies affecting memory. The single head arrows suggest a possible direction of disease progression with periodontitis as the initial condition. The double arrow heads point to known examples of diseases that negatively affect memory.
A diverse list of candidate microbes that appear to be associated with, and survive the highly inflammophilic environment of the AD brain, is given by Olsen and Singhrao [3]. However, there is a paucity of information as to whether there is synergy among multiple-species identified from AD brains, as is suggested, for example, in the oral biofilm bacteria [30]. Miklossy implicates oral and non-oral spirochaetal infections [13, 49] as dominant AD pathogens. However, microbes, such as Chlamydophila pneumoniae [50], Helicobacter pylori [51], Herpes simplex virus type 1 [52], and LPS from Gram-negative bacteria [14, 53], are documented as being identified in AD postmortem brain specimens. This hypothesis implies the existence of an AD specific, but yet incomplete microbiome, consisting of a consortium of inflammophilic pathogens indigenous to oral and remote body organs. Intensive research is underway with newer hypotheses incorporating Aβ senile plaques as by-products of bacterial biofilm matrices [54, 55], and determining the existence of synergy among multiple-microbial species. If this is the case, oral bacterial infections will reveal their potential to cause/modulate the late-onset AD with possible synergy with other spirochetes as suggested elsewhere [49, 56].
THE BLOOD-BRAIN BARRIER
Finding oral bacteria in postmortem AD brains is intriguing. To this end, our research in the P. gingivlais infected ApoE-/- periodontal disease mouse model [57] continues to search for scientifically relevant clues. Our research findings in chronic P. gingivalis infection of ApoE-/- mice suggest the integrity of the hippocampal blood-brain barrier (BBB) gradually erodes via an inflammation mediated physical injury of the cerebral parenchyma [58]. For the first time, P. gingivalis infection in mice has been associated with the loss of BBB integrity [58]. This is interesting, as the same pathological feature of the BBB exists during human aging [59] and in AD subjects with the APOE4 genetic phenotype [60]. AD subjects with the APOE4 susceptibility gene demonstrate a high proinflammatory cytokine (tumor necrosis factor-alpha or TNF-α, IL-6, and IL-1β) expression [61]. Since microbial infections promote interleukin class of cytokines (IL-6 and IL-1β) and TNF-α secretion via the inflammasome formation [62], it is plausible to suggest that individuals with APOE4 genotype are prone to harboring chronic infections and the cytokine burden is secondary to infections. For example, the genetically modified phenotype of ApoE-/- mice is predisposed to intrinsic stress in the form of higher burden of vascular inflammation, due to the constitutive expression of the pro-inflammatory cytokine TNF-α[63, 64]. Consequently, they are more sensitive to local and peripheral innate immune mediators (cytokines) released following daily bacteremia from experimental periodontitis [57]. This correlates with daily bacteremias that occur in humans due to periodontitis [65, 66]. A defective BBB [59, 60] would allow entry of pathogens and their immunogenic virulence factors and non-infection related molecules into the brain. Entry of bacteria and bacterial products will trigger oxidative stress followed by continually stimulating microglia to express inflammatory cytokines locally and generate neurodegeneration by mitigating protection of neurons from extrinsic insults.
There is little doubt that recurrent infections of the elderly increase the odds for developing AD [67]. The deteriorating BBB following P. gingivalis infection in mice [58] helps to explain the possible delirium post infections observed in elderly awaiting clinical AD diagnosis [67]. With regard specifically to periodontal disease, one longitudinal study has suggested a link between higher Aβ load in the hippocampus of elderly humans with mild forms of periodontitis [37]. Singhrao et al. [58] are suggesting the role of P. gingivalis in inflammation mediated injury with progressive deterioration of the hippocampal microvascular integrity in the very regions of the brain that demonstrate a high burden of neuropathological hallmarks of AD. These observations are similar to the effect of physical insults, such as traumatic brain injury and stroke, which also lead to cognitive deficit (Fig. 2), aggregated hallmark protein accumulation and eventually AD [45, 68]. Both infections and physical brain trauma show common inflammatory mediators in their eventual manifestation of dementia [17, 70].
Nutritional deficiency also correlates with cognitive decline [71], and fewer teeth may lead an individual reducing their intake of fresh foods, which in turn may decrease intake of B-vitamins and folic acid and other forms of nutrition [28]. Taken together, factors causing deterioration in cognition are multifactorial and complex with likely contribution from primary infection and nutritional deficiency due to loss of teeth. For example, depression can manifest from the generalized feeling of being unwell and can suppress appetite. Furthermore, AD is a depressive condition that can also lead to sufferers having reduced appetite.
Bacterial infections, specifically those that are involved in the onset of stroke, can also lead to AD in survivors [43–45]. Systemic hypoxia from co-morbid vascular states (atherosclerosis/stroke) [72, 73] and paucity of peripheral adaptive immune cells in the AD brain, and from Rag-5xfAD mice, demonstrates enhanced neuroinflammation and Aβ accumulation compared to control animals [36]. This research helps to explain Aβ deposition and abnormal tau phosphorylation post stroke. The chronic P. gingivalis infection of ApoE-/- mice show inflammation mediated physical damage that appears to be similar to that seen in traumatic brain injury or concussion cases with shared inflammatory biomarkers [58, 69]. These facts demonstrate how chronic infection of the brain with a keystone pathogen, such as P. gingivalis, can cause potentially serious consequences for the BBB and subsequent poor mental health. Future research should include AD transgenic mice with oral infections to support the preliminary findings of Singhrao et al. [58].
SLEEP
Sleep is a physiological process, which reduces responsiveness and induces immobility on a temporary basis [74] in order to rest the body and support several brain functions including mood, memory, and consciousness [75]. Two main biological drivers govern sleep. The first is the homeostatic pressure to sleep, which rises as the amount of time increases since the last sleep period [76]. The second driver is the body’s endogenous circadian timing mechanism, which controls the timing and organization of sleep and is located in the hypothalamic suprachiasmatic nuclei (SCN) [40, 77]. During sleep, changes in the brain’s electrical activity observed via cortical electroencephalogram (EEG) patterns define two different behavioral states. The first observable state is non-rapid eye movement sleep characterized by the presence of “theta waves” and “delta waves”. Second is rapid eye movement sleep characterized by EEG patterns similar to people who are awake but distinguished by the presence of phasic events (twitching limbs), and tonic phenomena (loss of muscle tone) [78].
Research has pointed to a clear link between sleep duration and quality and physical health [79]. Short sleep durations (less than 6 h) and poor sleep quality can increase the likelihood of mortality [80, 81] and specifically increase susceptibility to illnesses, such as coronary heart disease [82] and Type 2 diabetes [83]. Indeed, lack of sleep and poor sleep quality appear to impact negatively on the body’s metabolic [84], endocrine, and immune functioning [85]. Furthermore, recent research has suggested that although healthy younger cohorts can compensate for the impact of sleep-deprivation or poor sleep quality, older adults and those with AD appear to suffer more markedly from disrupted sleep-wake cycles [86]. In addition, the process of aging can affect negatively on the mechanisms controlling sleep. In the elderly, the aging of the SCN can lead to a decrease in neuronal activity, which in turn can cause changes in the circadian regulation and secretion of the sleep hormone melatonin [76]. Furthermore, an older population may have more psychological [87] and physiological [88] risk factors for poor sleep.
Specifically, within the AD population, there are marked changes in sleep with increases in disturbed night sleep and increased daytime napping. It is therefore plausible to suggest that poor sleep (both duration and quality) could increase the risk of developing AD [89] in the elderly. However, once AD is established, deterioration in the circadian system that controls sleep-wake cycles [90] may be the direct or indirect result of disease processes that lead to increased sleep disturbances. Patients with AD who have been institutionalized (hospital setting), for example, show the marked disturbances in circadian patterns perhaps due to limited exercise and daylight exposure [91]. However, as AD progresses, the damage to the neuronal pathways that initiate and maintain sleep become more pronounced and lead to increased problems with sleep [89, 93]. For example, AD patients show increased theta activity during non-rapid eye movement sleep [94]. Such changes in sleep can destabilize both physiological processes, such as immune function, and impact on cognitive processes, such as memory (Fig. 3). As the impact of sleep appears to be bidirectional, it may be that stabilization of sleep patterns reduce thesymptoms [95].
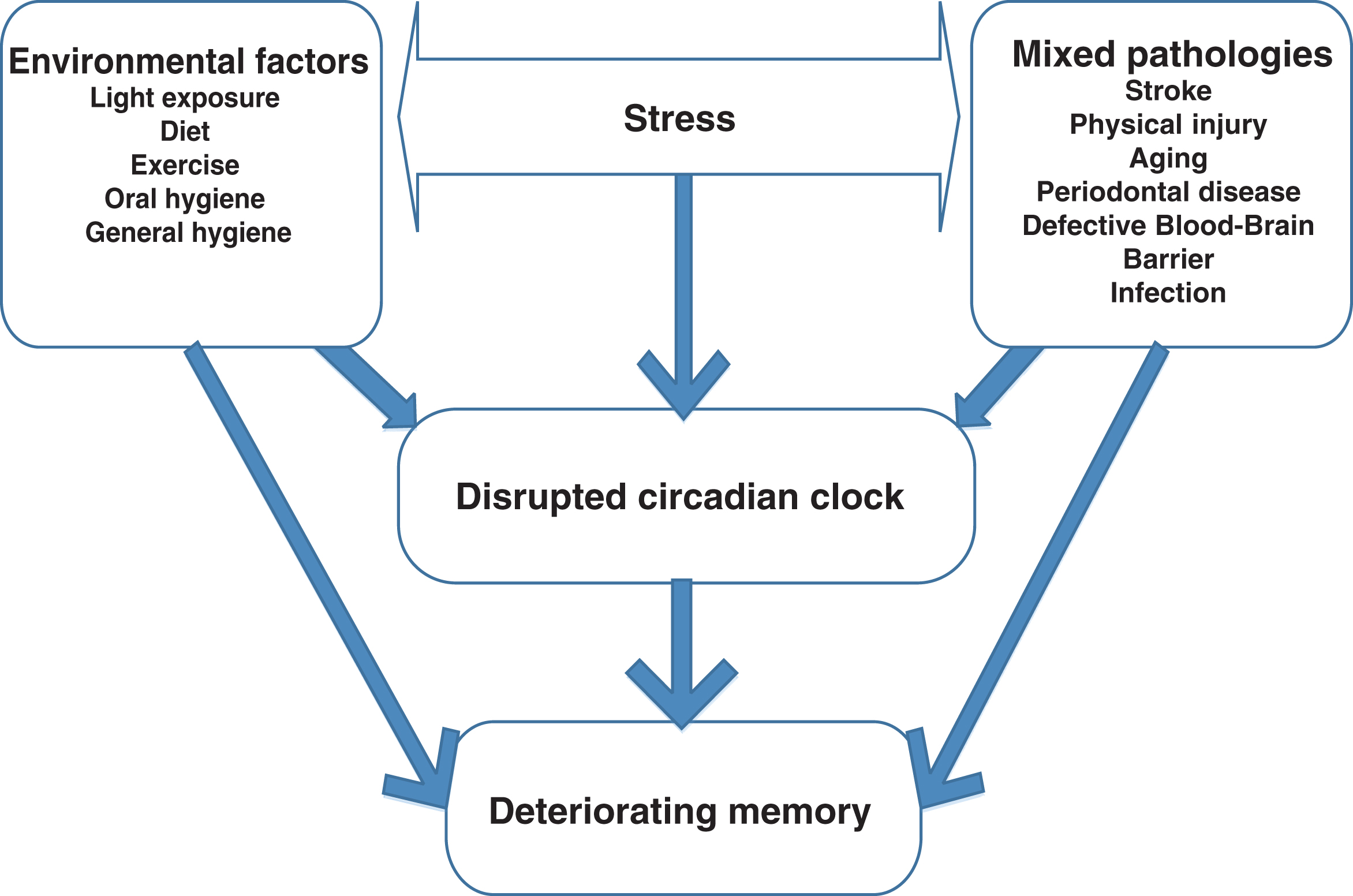
Schematic to show stress and the main risk factors influencing the circadian clock. All these factors, over time, lead to deterioration in memory. The arrows suggest a simplistic path for functional loss.
It is clear that sleep can affect the development [89] and progression [96] of AD. However, the precise way in which deregulated sleep may influence AD is not clear. An interesting link between sleep and the host’s immune system is suggested [97], which links infections, inflammation, and disturbed sleep-wake cycles. However, until the recent discovery of the glymphatic system, it was not clear what processes could be mediating the link between poor sleep and AD. The glymphatic system was discovered using two-photon imaging of live mice via a closed cranial window [98]. The glymphatic system uses the glial water channels to perform a clearance function within the brain similar to that of the peripheral lymphatic system [99, 100]. Therefore, the glymphatic system is important for the removal of danger associated molecular patterns such as microbial debris, interstitial solutes and Aβ plaques from the brain [101]. Interestingly, the glymphatic system appears to be “turned on” during normal sleep and reduces in function during the awake state [101]. Therefore, if individuals are suffering from sleep abnormalities then the reduced functioning of the glymphatic system could increase levels of Aβ plaque formation and hyperphosphorylated tau neurofibrillary tangles. This may explain why poor sleep duration and quality can lead to the development of, and accelerate the progression of AD [102, 103]. Therefore, the down regulation of the glymphatic system because of aging and mixed pathological factors and intrinsic stress due to infections, which affect sleep quality and duration, may interact to influence AD development and progression (Fig. 3).
Impairments to the glymphatic system may specifically reduce the brains ability to clear microbes such as P. gingivalis. Direct infiltration of the brain by microbes such as P. gingivalis can directly lead to neuroinflammation through activation of cortical microglia and contribute to local immuneresponses [104]. Paolicelli and colleagues [105] reported that microglia play a key role in scavenging and pruning normal neuronal network connections for brain development, and this activity is greater when the animal is asleep. Takayama et al. [106] noted that P. gingivalis infection of mice brains caused sleep pattern disturbances by altering glial cell light/dark molecular clock activity. P. gingivalis, therefore, can subvert the host’s microglial cell phagocytic activity by disrupting the circadian system that controls sleep-wake cycles. Consequently, the glymphatic system appears less efficient. This important and original finding by Takayama et al. [106] links the keystone periodontal pathogen,P. gingivalis, to sleep disturbances and subversion of microglial cell function, and paves the way for aggregated protein build-up. This report has crucial relevance to sleep pattern disturbances in AD and supports how poor oral hygiene and the associated rising levels of intrinsic and extrinsic sources of cytokines may act as crucial early modifiers of neurodegeneration and disease severity leading to deteriorating memory, sleep and ultimately the development of pathology.
WAYS TO MITIGATE RISK FACTORS
Oral hygiene
From an oral hygiene aspect, even having teeth (being dentate) but not maintaining daily oral hygiene appears to increase the risk (22–65%) of dementia compared to those who brush their teeth daily [107]. A healthy oral cavity has a normal microbiome, consisting largely of non-pathogenic commensal bacteria. These adhere to oral surfaces in the form of a biofilm. Any disruption of their environmental equilibrium can lead to polymicrobial synergistic dysbiosis resulting in periodontitis. For good gingival health and protection against periodontal disease, effective tooth brushing techniques (twice a day) for 2 minutes using toothpaste with fluoride (containing a minimum of 1350 parts per million fluoride) is recommended. Combining brushing with interdental cleansing (e.g., interdental brushing once before bedtime) will aid physical removal of plaque from in between teeth and help to control host’s inflammatory response to plaque. Individuals should be encouraged to visit the dentist regularly to improve their oral health no matter what their predisposition in health. For example, patients with clinical AD are less able to perform a recommended daily oral hygieneroutine mainly due to ongoing cognitive impairment, and their dental check-ups are reliant on the freedom of their caregiver. As periodontitis is treatable, it offers the potential to reduce AD progression, if managed correctly (Fig. 1). Therefore, the dental intervention for AD patients should be high on the priority scale. Ultimately, the caregivers will need to take on-board the advice from dental professionals and change personal lifestyle and habits to minimize the severity of disease.
Diet
Poor diet combined with a non-active lifestyle leads to nutritional deficiencies and development of metabolic abnormalities. These include increases in the following: insulin resistance and chronic inflammation, oxidative stress-induced proteins, lipids, DNA damage, and alterations in neuroendocrine systems [108–113]. Calorie reduction, resulting in a body mass index of a healthy range of 19–23 is beneficial for bone density [114]. Moderate exercise leads to improved glucose tolerance and insulin action, and reduction in cardiovascular disease risk factors including plasma low-density lipoproteins-cholesterol concentration [115, 116]. Excessive exercise may increase the subjects’ metabolic rate, which in turn can act as a disease-based risk factor. Individuals prone to recurrent microbial infections show increased TNF-α level despite consuming a healthy diet suggesting the oxidative stress from infections is of a higher magnitude than the host can manage. Alternatively, aging and AD processes also lead to a gradual accumulation of oxidative stress and molecular damage suggesting existence of incomplete efficiency in anti-oxidative and repair mechanisms in the host [117].
Certain foods have a beneficial impact on health. Plant foods contain a range of phytochemicals and vitamins, which are associated with reduced oxidative stress and inflammation. These natural anti-oxidants help to prevent cardiovascular disease and cancer [118, 119]. A diet high in foods containing phytochemicals such as onion, garlic, wild blueberries, tea, cabbage, carrot, celery, and soya may reduce oxidative stress and inflammation [120], while some grain-based foods may destabilize blood glucose levels. In addition, oily fish high in omega-3 and omega-6 polyunsaturated fatty acids can positively affect the regulation of inflammation by increasing levels of eicosanoids [121]. Therefore, a healthy diet could reduce metabolic abnormalities, oxidative stress, and inflammation, which in turn, can control the progression of periodontitis and subsequently slow down AD progression.
CONCLUSIONS
Periodontitis constitutes a peripheral oral infection, the pathogenic components of which may result in infecting the brain and/or exposing the brain to immunogenic virulence factors and inflammatory mediators implicated in the pathogenesis of AD.A prospective interventional study has shown that effectively treating periodontitis can lead to improvements in cognition. A chronic oral infection with P. gingivalis in ApoE-/- mice demonstrated peripheral and intracerebral inflammation is capable of compromising BBB integrity. A dysfunctional BBB can lead to many neurological diseases, including stroke, traumatic brain injury and AD. This demonstrates some relevance of a chronic infection of the brain with a keystone pathogen such as P. gingivalis, causing potentially serious consequences for the BBB and subsequent mental health. Others have shown that P. gingivalis infection can alter the microglial cell light/dark molecular clock activity, resulting in defective phagocytosis. This increases the prevalence of danger associated molecular patterns, which prevent normal functioning of neuronal networks as does a periodontal dysbiotic microbial community in subverting hosts innate and adaptive immune responses. Thus, risk factors for AD should also include periodontitis in addition to the more accepted factors, such as aging, genetic susceptibilities, stroke, and traumatic brain injury.
Diet
The dietary regime should include foods that offer long-term protection from developing mixed pathologies (Figs. 1–3). The diet should include high intake of green leafy vegetables and blueberries, and oily fish because they appear to have anti-oxidant and anti-inflammatory properties as well as lowering cholesterol.
Sleep
Good quality sleep appears to be critical for the glymphatic system to function. Glymphatic processes appear to have the potential to prevent and slow AD progression. Health practitioners should highlight the importance of good sleep alongside guidance on diet and physical activity. Other potential non-medical interventions include focusing on a diet high in foods that promote sleep and the use of light therapy.
All of the above everyday activities (hygiene, dietary intake, and sleep) are changeable by the host’s indigenous microbiome if their balance is disturbed.