
Abstract
Background:
Alzheimer’s disease (AD) is associated with several antibodies as well as signaling molecules and receptors. These may be detrimental in the presence of a disrupted blood-brain barrier (BBB).
Objective:
To investigate whether the levels of antibodies toward 33 signaling molecules involved in neurotransmitter, vascular, and immune functions were associated with AD and, within the AD group; cognitive function and mood.
Methods:
Antibodies in sera from patients with mild AD [(n = 91) defined as a Mini-Mental State Examination ≥ 20 or a Clinical Dementia Rating Scale≤1] and healthy controls (n = 102) were measured with enzyme-linked immunosorbent assays. Levels in AD and controls were compared by Mann-Whitney test. In the AD group, associations between antibodies and psychometric test scores were analyzed by robust regression. The false discovery threshold was set to 0.05.
Results:
Antibodies to serotonin receptors [5-HT2AR (effect size (r) = 0.21, p = 0.004), 5-HT2CR (r = 0.25, p = 0.0005) and 5-HT7R (r = 0.21, p = 0.003)], vascular endothelial growth factor receptor 1 [VEGFR1 (r = 0.29, p < 0.001)] and immune-receptors (Stabilin-1 (r = 0.23, p = 0.001) and C5aR1 (r = 0.21, p = 0.004) were higher in AD. Psychomotor speed was associated with D1R-abs (β 0.49, p < 0.001), depression with ETAR-abs (β 0.31, p < 0.001), and visuospatial function with 5-HT1AR-abs (β 0.27, p = 0.004) despite similar antibody levels compared to controls.
Conclusions:
Antibody levels to VEGFR1, serotonergic receptors, and receptors in the immune system were increased in AD. Antibodies at similar levels as in controls were associated cognitive dysfunction and depression in AD.
INTRODUCTION
Alzheimer’s disease (AD) is the most common form of dementia [1]. Neuropathological hallmarks of AD are accumulation of amyloid-β (Aβ) in plaques and tau proteins in tangles [2] causing extensive neuronal cell death [3], synapse loss [4], and microglial activation [5]. Naturally occurring antibodies (Nabs) of the IgG type are ubiquitous in human sera [6], including brain reactive antibodies [7]. Their physiological functions include clearance of apoptotic cells [8]. Under physiological conditions, the concentration of immunoglobulin G (IgG) inside the brain is extremely low and most Nabs do not cause disease. However, Nabs directed at proteins in the brain with pathogenic potential do exist at low frequencies in healthy populations [9]. Their pathogenic effect on the brain is likely dependent on damage to the blood-brain-barrier (BBB) [10]. Most AD patients have cerebral amyloid angiopathy and microvascular disease in the brain. Due to the BBB impairment seen in AD, IgG penetration to the brain might be increased [11].
AD has previously been associated with antibodies toward Aβ, tau, vascular-related molecules, lipid molecules, neurotransmitter receptors, glial markers, and cellular enzymes (reviewed in [12]). Antibodies directed to the angiotensin 2 type 1 receptor (AT1R-abs) [13], the α1- and β2-adrenoceptors, glutamate, serotonin, dopamine, and the N-methyl-d-aspartate glutamate receptors (NMDAR-abs) are found in AD sera [14–16]. Antibodies to receptors and signaling molecules may have pathogenic effects beyond the Fc-receptor mediated effects, by inducing signal-transduction mechanisms and as such they could act on receptors involved in neurotransmission under conditions with BBB impairment. In this explorative study, we aimed to comprehensively investigate antibodies to vascular, immune, serotonergic, dopaminergic, and muscarinic cholinergic receptors and signaling molecules to establish a) if they are increased in AD compared to healthy controls and b) if they are associated with cognitive functions and mood in AD.
MATERIAL AND METHODS
Subjects
Patients with mild dementia were recruited to a longitudinal cohort-study between 2005 and 2007 from three participating centers in Rogaland and Hordaland counties in Norway, the Dementia study in Western Norway (DemVest) [17]. From this larger cohort of 250 patients, 91 patients with AD and available blood samples were included in this study. Clinical data, psychometric test results, and measurements in sera from baseline constituted the main objects of study. Mild dementia was defined as a Mini-Mental State Examination (MMSE) test score ≥20 or a Clinical Dementia Rating scale = 1. AD was diagnosed according to the criteria from the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorder Association (NINCDS-ADRDA) [18]. A trained research clinician with long experience in geriatric psychiatry, neurology, or geriatric medicine conducted a detailed medical history and standardized clinical examination. Structural MRI was conducted for diagnostic purposes [19]. Patients were recruited for brain donation. Among the 91 cases included in this study, 19 patients underwent autopsy and 16 had a neuropathological diagnosis of AD (84.2%). Exclusion criteria were acute delirium or confusion, terminal illness, recently diagnosed major somatic illness, and previous bipolar or psychotic disorder. Patients were examined with neuropsychological tests (see below). The Cumulative Index Illness Rating Scale (CIRS, reviewed in: [20]) was registered for patients and controls. CIRS scores co-morbidity in 14 system domains by a severity score that can be added to give a total score (CIRS-total). ApoE genotyping [21] and routine blood tests were performed, including leukocyte count as a general marker of inflammation (see “Statistics” below). Further details of the clinical and biomarker assessment program are described elsewhere [17].
One hundred and three healthy community-dwelling elderly controls were recruited from senior centers in Bergen, Hordaland, during 2014. The control group was frequency matched by design on age and gender compared to the AD group (see Table 1, results). Good physical and mental health and a MMSE test score ≥28 were inclusion criteria. A trained internist conducted a clinical interview and examination. Ongoing psychosis, delusions, depression, major medical illness, previous bipolar- or psychotic disorders were exclusion criteria. Cardiovascular risk factors, cardiovascular disease, cerebrovascular disease [transient ischemic attack or stroke (CBVD)], other known illnesses, CIRS, medication use, body mass index (BMI), and blood pressure were registered for both groups.
Characteristics of the study participants
M, mean; SD, standard deviation; Mdn, median; IQR, interquartile range; MMSE, Mini-Mental State Examination; BP, blood pressure; CIRS, Cumulative illness rating scale; MADRS, Montgomery Asberg Depression Rating Scale; VOSP, Visual Object and Space Perception Battery. aUnivariate statistical analysis by student T-test. bUnivariate statistical analysis by Pearson Chi-Square test. cUnivariate statistical analysis by Mann-Whitney U test. dCardiac disease = any of the following: known coronary heart disease, heart failure or atrial fibrillation. eCerebrovascular disease = previous stroke or transient ischemic attacks. fFrom the California Verbal Learning Test, Second Edition, part A. *Statistically significant difference <0.05, or **highly significant, <0.001.
Ethics
Ethical approval was granted from the Regional Ethics Committee (REK approval no.: 2010/633). Both patients and controls provided written consent to participate in the study after procedures had been explained in detail, and in case of patients with AD, also to a caregiver [13].
Antibody measurements
Sera from patients and controls were collected at baseline and stored at minus 80°C. Sample labels were blinded for the laboratory prior to analyses. Recombinant signaling molecules and receptors were expressed in Chinese hamster ovary (CHO) cells purified from membranes and used as antigens in subsequent enzyme-linked immunosorbant assays (ELISA) (CellTrend GmbH, Luckenwalde, Germany) [22]. A more detailed description of the ELISA procedure can be found in the Supplementary Material with coefficients of variation (Supplementary Table 2) and a list of abbreviations (Supplementary Table 4).
Mean storage time was 1 year for controls and 7 years for patients. Bias due to different storage times was investigated. First, by dividing the AD group into three subgroups based on mean years of storage time and comparing antibody levels in each of these subgroups (by year) to controls, a change in associations indicative of a temporal effect would indicate bias. Second, significant correlations between the levels of antibodies and storage time within the AD group would indicate bias.
Antigen selection
We selected antigens from a broad range of receptor and signaling systems expressed in the brain, vessels, immune system, lung, heart, and kidney that participate in key signal transduction pathways. We measured antibodies to three signaling molecules: vascular endothelial growth factor alpha (VEGFA); platelet derived growth factor (PDGF); and nerve growth factor (NGF); and twenty-two antibodies to receptors of the adrenergic-, dopaminergic-, serotonergic-, and cholinergic systems. Antibodies to the vascular receptors endothelin receptor type A (ETAR), protease-activated receptor 1 (PAR1), VEGF, VEGFR1, and VEGFR2 and antibodies to the innate immune system receptors [Stabilin-1 (Stab1) and Stabilin-2 (Stab2) and the complement component 5a receptor type 1 (C5aR1)] were also measured [23]. Finally, measurement of antibodies to nerve growth factor (NGF, linked to neuronal survival [24]) and the receptor for advanced glycation end-products (RAGE) that transport Aβ from the blood to the brain was performed [25].
Neuropsychological testing and mood
Four specific cognitive domains were tested: verbal memory [List A, Short Delay Cued Recall, California Verbal Learning test-II (CVLT-II) subtest (CVLT-SDCR)], visuospatial function [Visual Object and Space Perception Battery – Silhouettes subtest (VOSP)], psychomotor speed [Trail Making A Test (TMT-A)], and executive function (Stroop color-word test). TMT-A is a measure of psychomotor speed [26]. The Stroop Color-Word test use interference to test the ability to shift attention (Stroop effect: Stroop-E) and it is a measure of executive function. Depression was assessed using the Montgomery and Aasberg Depression Rating Scale (MADRS), a clinical interview consisting of 10 items scored between 0 and 6 that has shown good test performance in AD [27]. An overview of central tendencies and dispersions of the psychometric scores can be found in Table 1, results.
Power analyses
We could not identify prior studies to identify effect sizes a priori. We therefore used small-to-moderate effect size for power analyses. Alpha levels of 0.01 were used as a crude adjustment to accommodate power loss due to adjustment for multiple testing (see Statistics). A sample size of 200 in equal groups was necessary to detect a moderate difference (R = 0.24) in antibody levels between the groups with a power of 0.8 [alpha = 0.01, Mann-Whitney U test (MWUT)]. The required sample size to detect an R2-increase of 0.13 from 1 predictor in multiple linear regression (regression with antibodies and psychometric test scores) with a power of 0.8 was 82 (alpha = 0.01, predictors = 5). Power to detect interactions in multivariate regression (not calculated) has been estimated to be 1/3 of the overall power, making our study underpowered to detect such effects [28], but multivariate analyses of confounding do not lead to a similar power loss [29]. Power analyses were conducted with G*Power 3.0 [29].
Statistics
p-values less than 0.05 were considered statistically significant and adjustment for multiple comparisons were made with false discovery rate set to 5% (Benjamini-Hochberg). Univariate tests were analyzed using non-parametric statistics and ROC analyses (evaluated at specificity and sensitivity of 0.7) due to skewed distributions of antibody levels. A clustered heatmap was made from Spearman correlations between antibody levels. In multivariate analyses, antibody levels were transformed to normality by the Rankit method (logistic regression) and Box-Cox transformations (linear regression). Cognitive test scores were log and square root transformed to normality and optionally inversed so that “higher is worse” was true for all.
Confounding effects due to differences between the AD and control groups were evaluated by comparing estimates of antibody association with AD by logistic regression. Estimates from a simple model with age and gender (model 1) was compared to estimates a model with age, gender, known hypertension, current systolic blood pressure >140 mmHg, diabetes, current smoking, cardiac disease, and CBVD as potential confounders (model 2). A 10% change in estimate [(Crude Odds Ratio (OR) – Adjusted OR) / Crude OR] was considered minor confounding and change to a non-significant p-value, major confounding. Finally, we compared antibody levels between participants with neuropathologically confirmed AD to those with a clinical diagnosisof AD.
Potential linear relationships between antibodies and psychometric test scores were analyzed by standardized robust regression by MM estimation [30] (package “mmregress”, STATA) due to the presence of influential outliers (criteria: Cooks distance > 4(N – k -1) and/or leverage >2p/N). Due to strong correlations between antibodies (illustrated in Fig. 3), the assumption of non-multicollinearity was broken. Each antibody was thus entered separately with covariates to identify the strongest associations. We addressed major confounding of the strongest associations from ApoE genotype, leukocytes, vascular risk factors or CBVD (10 cases missing for ApoE genotype and total cholesterol were deleted list-wise, as they were missing completely atrandom).
Analyses were performed using SPSS Statistics version 22.0 (SPSS Inc., Chicago, IL, USA), STATA 14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP), and Orange Data Miner (Orange, in collaboration with Open Source Community, Bioinformatics lab.,University of Ljubljana, Slovenia) [31].
RESULTS
Study participants
The AD and control groups were frequency matched by design on age and gender with a good match. They were also well matched on BMI, ever smoking, and CIRS, but there were significant differences between the groups in the prevalence of cardiovascular risk factors and disease (Table 1).
Differences in antibody levels between AD and controls
Eleven out of 33 antibodies measured were significantly different between the groups and six antibodies were discoveries, after multiple testing was adjusted for (Fig. 1). Antibody levels by groups can be found in Supplementary Table 1.
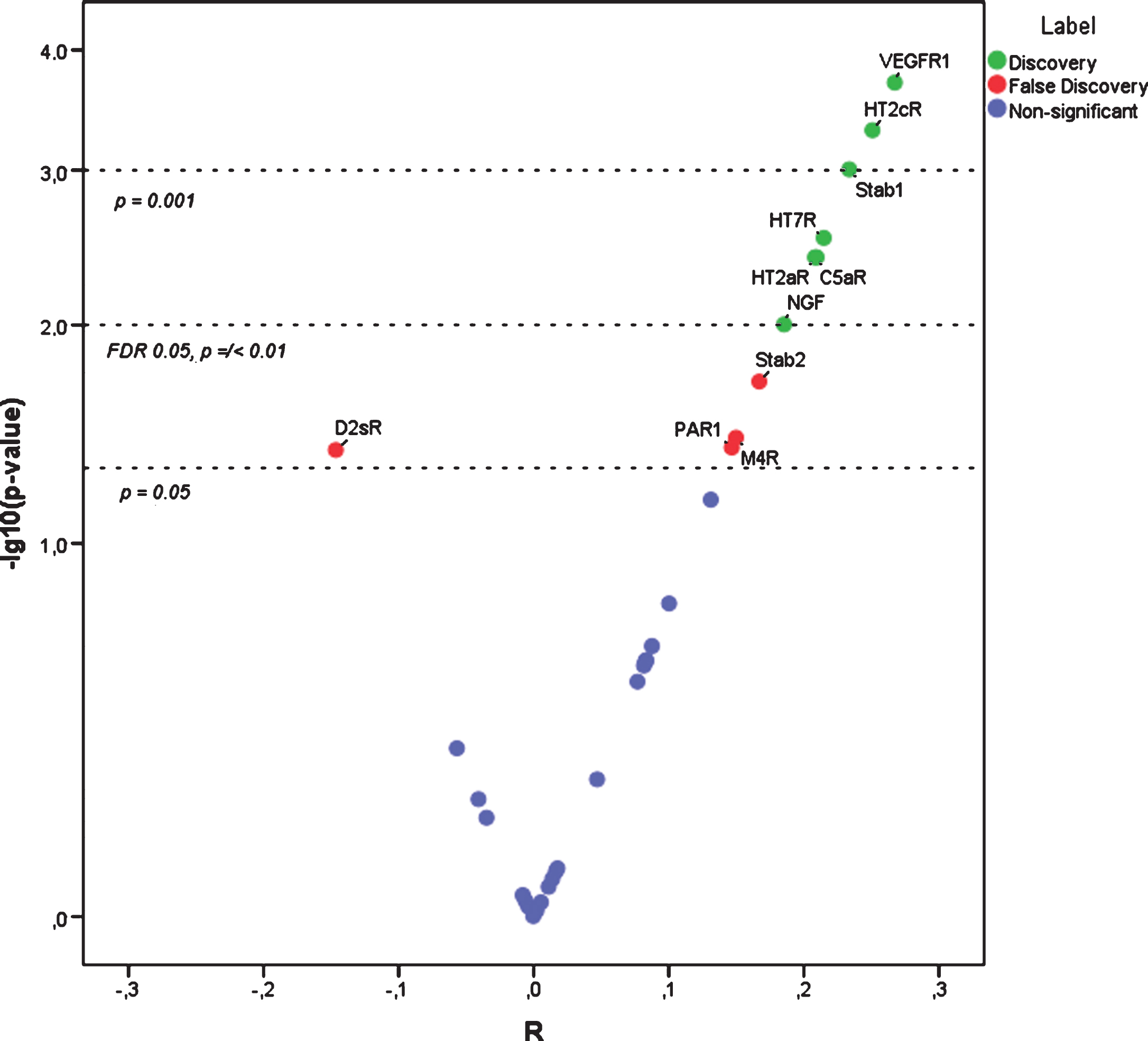
Antibodies in Alzheimer’s disease and healthy controls. *Non-parametric smile plot. The negative log of the p-value is on the y-axis (1 is p = 0.1, 2 is p = 0.01, 3 is p = 0.001) and R from Mann-Whitney U test (calculated as the test z-score/√N). Positive R indicates association with AD. p-values of 0.05 and 0.001 and p-value cut-off adjusted for multiple testing with the FDR 0.05 are indicated.
VEGFR1-abs was most associated with AD (r = 0.28, p = 0.0002) with 5-HT2AR-abs (r = 0.21, p = 0.004), 5-HT2CR-abs (r = 0.25, p = 0.0005), 5-HT7R-abs (r = 0.21, p = 0.003), Stab1-abs (r = 0.23, p = 0.001), C5aR1-abs (r = 0.21, p = 0.004), and NGF-abs (r = 0.19, p = 0.01) less so. The sensitivity and specificity of VEGFR1-abs to distinguish AD from controls was 0.58 and 0.52, respectively.
Immune-assays for determining antibody levels: Coefficients of variation
Fourteen out of thirty-three antibodies measured had coefficients of variation <10% (good), fifteen below 20% (acceptable) and four were above 20% (poor). Of the antibodies increased in AD, 5-HT7R-abs had a coefficient of variation >20%. A full list of coefficients of variation can be found in Supplementary Table 2.
Confounding analysis of the difference between AD and controls
We found no influence of storage time on antibody levels (data not shown), consistent with previous studies [32]. To identify if the group differences in vascular risk and disease confounded the relationship between AD and antibodies, we compared multivariate models with and without these confounders (Table 2).
Multivariate analysis of Alzheimer’s disease versus healthy controls
OR, odds ratio; p, p-value; ΔOR = ((Crude OR – Adjusted OR)/Crude OR)). ΔOR > ±0.1 is minor confounding. aOutcome: AD versus controls, covariates: age, gender and antibody as listed (logistic regression). bOutcome: AD versus controls, covariates: age, gender, cardiac disease, diabetes, stroke, hypertension, BP > 140, current smoking and antibody as listed (logistic regressions). *Major confounding (change to non-significant p-value).
None of the antibodies met the 10% change in estimate (OR) criterion, but NGF-abs were majorly confounded. Antibody levels were not different between neuropathologically confirmed and clinically diagnose AD (p-values [0.37–0.86], MWUT).
Correlations between antibodies: Within-group analysis of patients with AD
The antibodies in AD (controls not shown) correlated (Spearman) with each other with weak, moderate, and strong correlation coefficients and formed hierarchical clusters (Fig. 3).
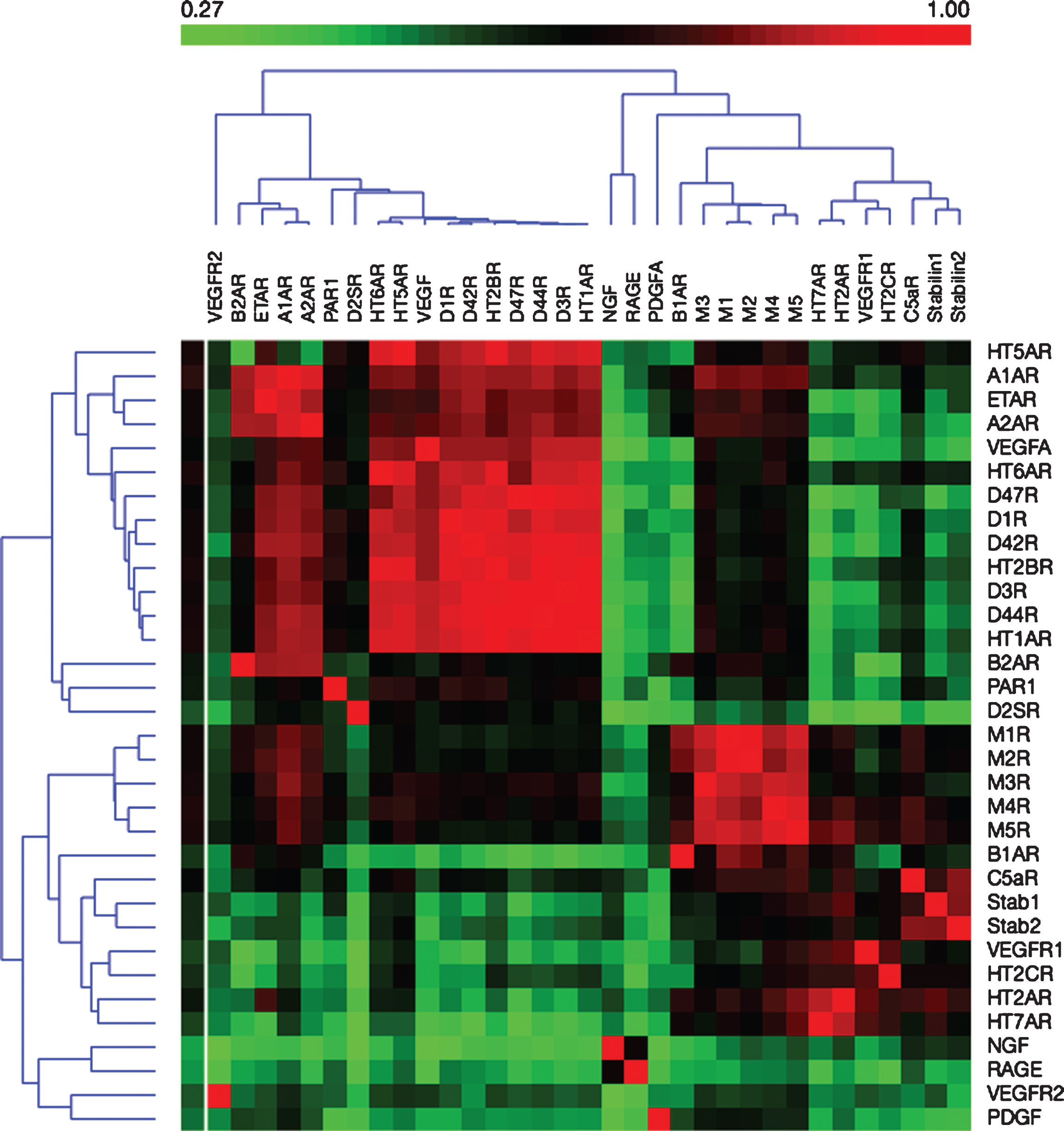
Antibodies are correlated and form hierarchical clusters (heatmap). *Antibodies in hierarchical clusters by their spearman correlation coefficient. Weak correlations are displayed in green, moderate in black and strong in red.
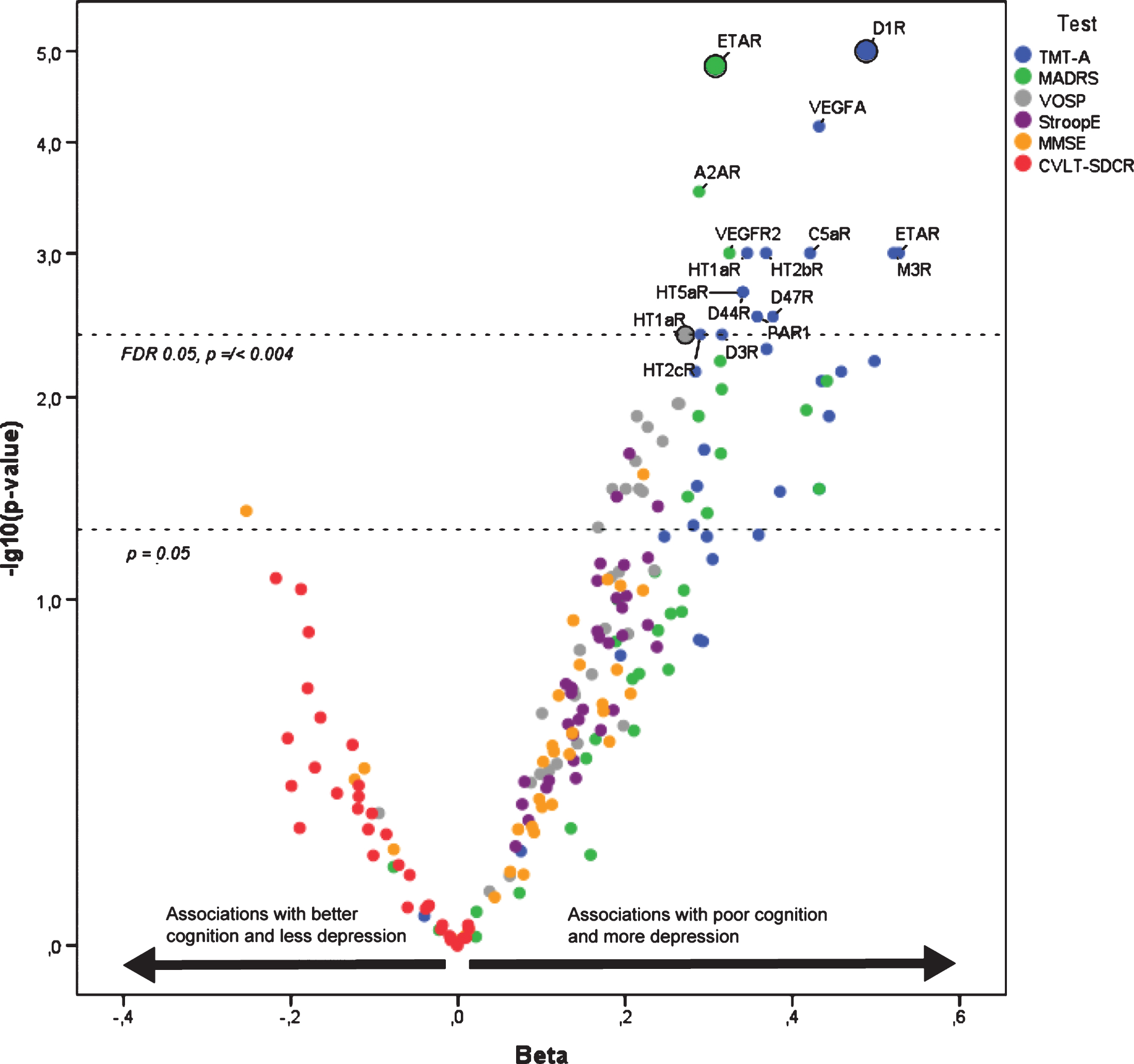
Antibodies, cognitive testing, and depression. *Smile plot of 196 robust regressions by MM estimation where each antibody is analyzed with covariates and the cognitive test (color coded) as the outcome. -log(p-value) on the Y axis generates a scale were (1 is p = 0.1), (2 is p = 0.01), (3 is p = 0.001), and (4 is p = 0.0001). Beta indicates standardized regression coefficients. Positive beta values indicate that antibodies are associated with poorer cognitive function and higher depression scores. The strongest associations with a particular cognitive test have larger dots. p = 0.05 and the FDR cutoff at FDR = 0.05 are marked by lines. All analyses are with age, gender, education, and CIRS in the equation. MMSE, Mini-Mental State Examination; CVLT-SDRC, CVLTA Short Delayed Cued Recall; Stroop E, Stroop effect; MADRS, Montgomery-Aasberg Depression Rating Scale; TMT-A, Trail Making A test. Three cases were missing for TMT-A, 1 for VOSP, and 3 for Stroop effect.
Many strong correlations between antibody levels will result in lack of statistical independence of all observations. This is likely due to sequence and/or structural homology in the extracellular sequences of the antigens targeted.
Antibodies, cognition, and mood: Within-group analysis of patients with AD
Age, gender, CIRS, and education (dichoto-mized >10 years) were included as covariates in all regressions. All cognitive test results were transformed so that a higher score is worse (Fig. 3).
Psychomotor speed (TMT-A) was most strongly associated with D1R-abs (β 0.49, p < 0.001), depression (MADRS) with ETAR-abs (β 0.31, p < 0.001), and visuospatial function (VOSP) with 5-HT1AR-abs (β 0.27, p = 0.004). There were no discoveries with MMSE, memory (CVLTA-SDCR), or executive function (Stroop-E).
We did not identify major confounding of these associations. Some confounders were themselves associated the outcomes. Current smoking (β 0.43, p = 0.03) and CBVD (β 0.68, p = 0.004) were associated with TMT-A and low BMI with VOSP (β -0.35, p = 0.03). The full confounding analysis can be found in Supplementary Table 3.
DISCUSSION
AD was associated with a significant increase in the levels of six antibodies to receptors from the vasculature (VEGFR1-abs), immune (Stab1-abs, and C5aR1-abs), and serotonergic systems (5-HT2AR-abs, 5-HT2CR-abs and 5-HT7R-abs), after adjustment for multiple testing and differences in vascular co-morbidities. The difference in NGF-abs was confounded by group differences in vascular co-morbidities. Antibodies to VEGFR1 had the most significant association with AD. VEGFR1 is mainly expressed by the cerebral endothelium [33], but antibodies to other endothelial receptors were not increased. The main function of the innate immune system receptors C5aR1 and Stab1 are initiation of inflammation and scavenging, respectively [34, 35]. The serotonergic receptors that were targeted by antibodies have their highest level of expressions in the brain [36].
The physiological mechanisms that lead to the formation of auto-IgG Nabs, including brain antigens, are not firmly established. The level of Nabs can rise in response to apoptosis of cells and oxidation of proteins [37]. There is increased migration of immune cells to the brain in AD, including T-cells [38], monocytes [39], and neutrophils [40]. Expression of major histocompatibility protein 2, a key molecule for antigen-presentation, is increased in AD microglia [41]. This could generate an environment that favors autoantibody formation toward brain antigens. In line with this, antibodies to serotonergic receptors expressed mainly in the brain, were increased. Cholinergic neurons undergo extensive apoptosis in AD [42], but antibodies to muscarinic cholinergic receptors were not increased. Thus, we did not find convincing evidence to support AD-related cell-injury in the brain as a driver of antibody generation. More commonly, antibodies to brain antigens are initiated toward extra-cerebral antigens that are also expressed in the brain, or have shared epitopes with brain-antigens [43]. Apoptosis and oxidative stress also occur in the endothelial lining of brain [44, 45] and oxidative stress markers are generally increased in AD [46]. The antigens targeted are expressed at low to moderate levels in brain microvascular cells and immune-cells [36]. It is perhaps more likely that antibody formation is initiated due to AD-related cellular damage to cells outside the brain.
As illustrated in Fig. 2, we observed high correlations between the antibodies. Immunization studies have found the immune-assays applied here to be specific when animals are immunized to a linear epitope [47]. Nabs do not have the same high affinity binding to antigens as antibodies raised by immunization and are typically polyreactive. We propose that the observed correlations represent polyreactivity with linear and/or conformational epitopes. In support of this, the highest correlations between antibodies were between different dopaminergic antibodies (r > 0.9), which do have high structural similarity [48]. This suggests that the antibodies measured are Nabs, a physiological part of the innate immune system.
Poor cognitive performance and higher depression scores were associated with levels of antibodies that were not significantly increased in AD compared to controls. The strongest associations were between slower psychomotor speed (TMT-A) and D1R-abs (moderate effect), more depression (MADRS) and ETAR-abs (moderate effect) and finally worse visuospatial function (VOSP) and 5-HT1AR-abs (small effect). These three associations were not confounded by the ApoE4 genotype, leukocyte levels, BMI, or vascular risk factors or disease. AD patients that were current smokers or had CBVD also had slower psychomotor speed, while a high BMI was associated with better visuospatial function (Supplementary Table 3).
D1R, 5-HT1AR and ETAR have moderate to high expression in the brain [49–51]. Brain-reactive antibodies are found in healthy individuals and the antibodies observed against D1R and 5-HT1AR could represent brain-reactive antibodies at physiological levels [52]. Decreased D1-receptor expression is associated with cognitive slowing [53] and 5-HT1A-receptors are involved in spatial learning and memory [54]. ETAR does not have an established role in depression, but ETAR antagonists had a beneficial effect on depression in an animal model by influencing cytokine secretion [55].
The association of antibodies at physiological levels with poor cognitive function and depression may indicate that AD-patients could have an underlying frailty to antibodies directed at certain receptors, though we do not know if similar associations were present among the controls. It has been suggested that healthy elderly individuals have NMDAR-abs with pathogenic potential and that this pathogenic potential can become realized when there is BBB breakdown [9]. Alternatively, our findings could be related to an increase in Nabs due to a pro-inflammatory state. BBB damage could lead to more brain-immune interactions in AD than occurs under physiological conditions [56]. Levels of CRP are linked to both psychomotor speed and depression [57, 58]. In AD, neuropsychiatric symptoms are linked to levels of cytokines [59], despite no increase in levels of most cytokines in AD [60]. Our findings need to be investigated in future studies for validation and exploration of any potential mechanisms underlying the associations between serum-antibodies, cognitive function, and mood in AD. Our study lacked neuropsychological tests for the healthy controls so we could not estimate any associations between Nabs and cognitive function and depression in healthy individuals. While coefficients of variations were acceptable for the antibodies associated with AD and cognitive tests, 5-HT7R was an exception with an inter-assay variability >20% and this finding should thus be interpreted with caution. Further studies are necessary to identify antibody targets and the functional consequences of antibody binding. To adequately address any effect modification of underlying BBB impairment, the degree of BBB compromise and intra-thecal antibody levels needs to be measured. Our study had adequate power to test all the primary hypotheses and conduct confounding analyses, but was underpowered to test for effect modification. Strengths in our study include the standardized clinical and biomarker assessments of the AD patients and autopsy diagnosis in a subset. The overall diagnostic accuracy is thus likely to be high.
In summary, AD was associated with increased levels of Nabs targeting receptors of the innate immune system (Stabilin-1and C5aR1), of brain microvascular cells (VEGFR1) and serotonergic receptors (5-HT2AR, 5-HT2CR, and 5-HT7R), though effect sizes were small. Nabs at physiological levels were associated with cognition and mood in the AD group: ETAR-abs with depression (MADRS, moderate effect), D1R-abs with psychomotor speed (TMT-A, moderate effect), and 5-HT1AR-abs with visuospatial function (VOSP, smalleffect).
Footnotes
ACKNOWLEDGMENTS
We want to thank the Kavli Trust and Haraldsplass Deaconess Hospital for making this study possible and our collaborators, as well as employees, at Celltrend GmbH for their kind and competent collaboration. We want to thank patients, relatives, and research personnel in the DemVest Study for their contributions. The study received funding from the Kavli Trust and Haraldsplass Deaconess Hospital. The Kavli Trust donates funds for a wide spectrum of dementia research and funded most of the study. Haraldsplass Deaconess Hospital contributed 50% salary to the first author. Celltrend GmbH contributed financially by measuring antibodies without charge. None of the sources of funding contributed to design or statistical analysis.