
Abstract
Background:
Many dementia and cardiovascular disease (CVD) cases in older adults are attributable to modifiable vascular and lifestyle-related risk factors, providing opportunities for prevention. In the Healthy Aging Through Internet Counselling in the Elderly (HATICE) randomized controlled trial, an internet-based multidomain intervention is being tested to improve the cardiovascular risk (CVR) profile of older adults.
Objective:
To design a multidomain intervention to improve CVR, based on the guidelines for CVR management, and administered through a coach-supported, interactive, platform to over 2500 community-dwellers aged 65+ in three European countries.
Methods:
A comparative analysis of national and European guidelines for primary and secondary CVD prevention was performed. Results were used to define the content of the intervention.
Results:
The intervention design focused on promoting awareness and self-management of hypertension, dyslipidemia, diabetes mellitus, and overweight, and supporting smoking cessation, physical activity, and healthy diet. Overall, available guidelines lacked specific recommendations for CVR management in older adults. The comparative analysis of the guidelines showed general consistency for lifestyle-related recommendations. Key differences, identified mostly in methods used to assess the overall CVR, did not hamper the intervention design. Minor country-specific adaptations were implemented to maximize the intervention feasibility in each country.
Conclusion:
Despite differences in CVR management within the countries considered, it was possible to design and implement the HATICE multidomain intervention. The study can help define preventative strategies for dementia and CVD that are applicable internationally.
Keywords
INTRODUCTION
Worldwide aging of populations is strongly associated with dementia [1], as well as linked to increased occurrence of cardiovascular disease (CVD) [2], with both disorders causing major health, economic, and social burdens [3, 4]. The management of CVD is still suboptimal in many countries, especially among older adults [2], and no cure is available for Alzheimer’s disease (AD), the main cause of dementia. Therefore, prevention could be crucial both in reducing the occurrence of CVD and halting the rapid increase in the prevalence of dementia, as some projection models suggested [5, 6]. Most CVDs are indeed attributable to modifiable risk factors— hypertension, hypercholesterolemia, diabetes mellitus (DM), obesity, smoking, physical inactivity, unhealthy diet— which have also been linked to dementia and AD [1– 4, 7], providing opportunities for prevention.
Prevention of dementia and CVDs in older adults is complex, as it requires a combination of primary and secondary prevention, and challenging, given the lack of evidence for this specific age group and individuals with existing comorbidity. Some cardiovascular risk factors (CVRFs, e.g., hypertension, hypercholesterolemia) are now labelled as actual diseases, even when they bear no symptoms [8], making the traditional distinction between primary and secondary prevention increasingly unclear and “more artificial than real” [9], from a public health perspective. Very limited data is available from clinical trials [10], thus robust scientific evidence to guide the treatment of CVRFs in older adults is lacking, making CVD prevention in this age group uncertain. Even less evidence is available within the field of dementia prevention. Due to the multi-factorial etiology of dementia, AD, and CVD, multidomain interventions simultaneously targeting several CVRFs seem most likely to be beneficial. However, evidence of the optimal target population and the most effective intervention is lacking [11], for strategies to manage CVRFs in this highly heterogeneous age group, in particular [12, 13]. Nevertheless, successful prevention trials for DM have highlighted the potential benefits of multidomain approaches [14, 15]. The prevention of dementia/AD is a relatively new research area, but national guidelines for the management of CVRFs allow the development of preventative strategies. Recently, three, large randomized controlled trials (RCTs) [16–18] on prevention of dementia have tested pioneering multidomain interventions in older adults and addressed key methodological issues for the successful delivery of such strategies.
The experience from these RCTs revealed the need for a wider, international approach, leading to the European Dementia Prevention Initiative (EDPI, http://www.edpi.org) and to the Healthy Aging Through Internet Counselling in the Elderly RCT (HATICE, trial registration number ISRCTN48151589) [19]. Within the HATICE project, an international, multidomain intervention RCT promoting vascular health through the internet is ongoing in Finland, France, and the Netherlands. The aim of HATICE is to optimize the self-management of CVRFs, improve the cardiovascular risk (CVR) profile, and reduce the risk of CVD, cognitive decline and dementia. For the RCT, a generic evidence-based prevention strategy was developed based on the comparative analysis of national and European guidelines for the management of CVRFs. Here we describe the groundwork carried out to compare and integrate national guidelines of the three countries, and to design the HATICE intervention.
METHODS
Comparison and synthesis of the European, Dutch, Finnish, and French Guidelines for CVRF management
To support the European-wide setting and the evidence-based nature of the HATICE study, a comparative analysis of the guidelines for primary and secondary prevention of CVD was carried out. The latest guidelines for the management of CVRFs issued in the three participating countries at the time of the completion of the HATICE design (June 2014), as well as the guidelines by the European Society of Cardiology (ESC), were collected and examined [20–27]. The risk factors considered were: hypertension, dyslipidemia, DM, overweight, smoking, physical inactivity, and unhealthy diet. Although the French guidelines for the managements of dyslipidemia have been withdrawn since their publication in 2005, they have not been replaced with newer documents. Therefore, those used in this study remain the most up to date available recommendations. Since the management of CVRFs depends on the individual overall risk to develop CVD, the methods to quantify the CVR were also compared. Documents and recommendations addressing older adults were sought for and used, when available. A thorough English summary was prepared for each document that required translation.
Several parameters were extrapolated from each document: methods of assessment and normal range values of each risk factor; cut-off values to initiate lifestyle intervention and/or pharmacological treatment; content of the interventions; and specific recommendations for older adults. Main similarities and differences were identified across the countries, and data consistency examined to highlight potential difficulties in applying the intervention Europe-wide. The ESC guidelines [27] were used as an overall reference, when country-specific differences were not compatible with a uniform approach, or national guidelines lacked of specific recommendations.
Design of the intervention
HATICE is an international, multi-center, randomized, open-label, blinded end-point trial with an 18-month intervention and follow-up period [19]. 2,725 community dwellers aged 65+ with at least two CVRFs, and/or personal history of DM or CVD consented to participate in the trial [19], resulting in a study population with indications for either primary or secondary CVD prevention. Key aspects of the trial design are summarized in Table 1. The intervention is delivered through an interactive internet platform specifically designed for older adults; participants in the control arm access a simplified version of the platform, with only basic information and no interactive features [28]. Participants in the intervention arm have access to remote support of a lifestyle coach. The coach provides information, advice, and motivational support throughout the trial.
Summary of the key aspects of the HATICE trial design
BMI, body mass index; CAIDE, cardiovascular risk factors, aging, and incidence of dementia; CVD, cardiovascular disease; CVRF, cardiovascular risk factor; Fi, Finland; Fr, France; GP, general practitioner; LDL, low-density lipoproteins; MMSE, Mini-Mental State Examination; Nl, The Netherlands; PA, physical activity; SBP, systolic blood pressure.
The intervention was designed to promote self-management of seven CVRFs: hypertension, dyslipidemia, DM, overweight, smoking, physical inactivity, and unhealthy diet.
The results of the comparative analysis of the guidelines were used to define: the cut-off value for intervention, the content of the intervention platform, and recommendations provided by the coach. For all of the risk factors, cut-off values for lifestyle intervention were set to identify participants who were advised to act on a specific CVRF. Cut-off values for medical treatment were also set when applicable. However, as the HATICE intervention was not designed to have a pharmacological component, they were used to identify participants who were advised to seek medical assistance. When differences in cut-off values were identified among national guidelines, the value that maximized the number of participants eligible for intervention was chosen. The recommendations provided to the participants in the intervention arm were, when possible, specific for the age group (65+) and for the relevant level (primary or secondary) of prevention, and written to provide evidence-based, simple, reliable, and pragmatic advice that each individual could easily incorporate in his/her own unique lifestyle. The “Bandura’s theory for self-management and behavioral change” [29] was applied to define the conceptual structure of the intervention and the “Stages of Changes” [30, 31] model provided the basis for the motivational support delivered by the coaches.
Country-specific adjustments
The HATICE intervention was designed to not interfere with the healthcare services existing in each participating country, but rather complement them and facilitate CVRFs management in older adults. Therefore, it was crucial that the recommendations provided were always in keeping with national guidelines for CVRFs management and lifestyle habits. To ensure this, once the generic version of the intervention was finalized, minor country-specific adjustments were applied to both sections of the platform content and the coach protocol.
RESULTS
Guidelines’ comparative analysis: Similarities
Overall, the Dutch, Finnish, and French guidelines for the management of CVRFs were uniform and in keeping with the European ones. Similarities existed especially in lifestyle-related recommendations, and in the cut-off values that prompted interventions for specific risk factors.
The recommendations for physical activity (derived from the WHO’s guidelines) [32], smoking, and diet, were strongly uniform across the national and European guidelines and only minor differences were identified (Table 2).
Summary of lifestyle-related recommendations in the Finnish, French and Dutch guidelines for the management of lifestyle-related cardiovascular risk factors (physical activity, smoking and diet) and minor differences
Fi, Finnish guidelines; Fr, French guidelines; Nl, Dutch guidelines.
Regarding risk factors assessed through biological or anthropometric measurements (hypertension, dyslipidemia, DM, overweight), eligibility for intervention depended on the overall CVR, which was assessed differently in the three countries. Nevertheless, it was possible to identify communal reference values for lifestyle interventions and/or pharmacological treatment (Table 3). In the French guidelines, initiation of pharmacological treatments was not based on specific cut-off values, but recommended when the therapeutic targets were not achieved following three months of lifestyle interventions.
Cut-off values to initiate lifestyle interventions or pharmacological treatments for four cardiovascular risk factors, based on the guidelines for the management of CVD published in Finland, France, the Netherlands, and by the ESC. For blood pressure, the cut-off values used for people at high risk of CVD are shown
BMI, body mass index; BP, blood pressure; DBP, diastolic blood pressure; EACPR, European association of cardiology prevention and rehabilitation; ESC, European society of cardiology; FINRISK, FINRISK risk calculator score that predicts 10-year risk for coronary heart disease and stroke incidence based on the national FINRISK study [36]; FPGT, fasting plasma glucose test; HbA1C, hemoglobin A1C; LDL, low density lipoproteins; LI, lifestyle intervention; OGTT, oral glucose tolerance test; RPG, random plasma glucose; SBP, systolic blood pressure. *ESC SCORE [27] (Systematic coronary risk evaluation) can also be used to assess overall cardiovascular risk. **Assessed with FINDRISC [67] score. ***Defined as: 1. 10-year risk of morbidity and mortality from CVD≥20% and/or LDL > 2.5 mmol/l, or 2. 10-year risk of morbidity and mortality from CVD = 10– 20% and/or LDL > 2.5 mmol/L and presence of other risk-increasing factors.
For hypertension, indications for a lifestyle intervention were well aligned for France (systolic blood pressure (SPB)≥140 mmHg and diastolic blood pressure (DPB)≥90 mmHg) and Finland (SPB≥130 mmHg and DPB≥85 mmHg, consistent with the European recommendations). The Dutch Guidelines recommended lifestyle changes for blood pressure (BP) management depending on the 10-year CVR and presence of other CVRFs. The cut-offs for pharmacological treatment of people without history of CVD nor relevant comorbidities were set at SBP≥160 mmHg and DBP≥100 by the Finnish and European Guidelines, and SBP≥180 mmHg or SBP≥140 mmHg and increased risk of CVD in the Dutch documents (Table 3). Since this analysis was carried out, new recommendations for the management of hypertension were published in Finland [33].
The low-density lipoprotein (LDL)-cholesterol cut-off values for the treatment of dyslipidemia were more complex to define and compare because different parameters were considered in each country (Table 3). In Finland, all the cut-off values were based on a combination of CVR and LDL level. In the other two countries, initiation of a pharmacological treatment depended on the LDL value alone, whereas lifestyle intervention was recommended based on LDL value (France) or presence of any other risk factors (the Netherlands).
To assess blood glucose and DM, the three countries recommended different diagnostic tests, but for common tests, cut-off values for interventions were generally consistent (Table 3), with only minor differences. The French cut-off depended on a sequential approach similar to that for hypertension. The HbA1C cut-off values used for medical treatment prompted lifestyle interventions in all the three countries, confirming that pharmacological management of DM goes hand in hand with lifestyle interventions. The Finnish guidelines deviated from this pattern by recommending lifestyle changes in the pre-diabetes group with Fasting Plasma Glucose Test (FPGT)>6 mmol/L or Oral Glucose Tolerance Test (OGTT)>7.8 mmol/L.
For overweight and obesity, cut-off values were uniform throughout all guidelines: lifestyle intervention was consistently recommended for body mass index (BMI)≥25. Recommendations for medical treatment were less uniform (Table 3).
Comparative analysis of guidelines: Differences
Main differences in guidelines were identified in only one key area: the assessment of the individual CVR. The CVR was classified as “low”, “moderate”, or “high”, and affected cut-off values for intervention on specific risk factors, and overall patient management. In the French guidelines, the CVR was defined by the sum of CVRFs, whereas in the other two countries it was calculated as the risk of developing CVD within 5 or 10 years. The Dutch CVR estimates derived from the ESC SCORE [27] and two Dutch cohorts [34, 35] for the assessment of the 10-year risk of fatal CVD, and included information on sex, age, smoking status, cholesterol values, and SBP. In Finland, the FINRISK calculator [36], a 10-year risk score for fatal and non-fatal myocardial infarction and stroke, which included also information on DM and family history of CVD, or the European SCORE [27] were recommended. All the listed risk assessment tools were developed for populations at different ages, and differences were identified in their upper age limit: 65 years for the European score, 70 for the Dutch, and 74 for FINRISK. The French guidelines attribute to each CVRF equal weight, whereas in other countries different CVRFs are given varying weights, making direct comparison impossible.
Differences were also identified in the recommendations for pharmacological treatment for some of the CVRFs. Approaches to intervention for hypertension and dyslipidemia included detailed indications based on age, comorbidities, and overall CVR in all the countries, but recommendations about drugs of choice, and how to proceed from mono- to combination-therapies varied greatly. Medical treatment targeting obesity was envisaged only in France and Finland. Finally, some differences existed in the protocols for the assessment of the CVRFs, in particular, in the number of blood pressure readings for hypertension and the type of tests used for DM.
Recommendation for old and oldest-old individuals
As HATICE targets individuals aged 65+, the assessment of specific guidelines for old and oldest-old (age 85+) adults was deemed germane for the design of the intervention, and a key aspect of the comparative analysis. Overall, the guidelines examined lacked specific information on the management of CVRFs in older adults. This applied for both the calculation of the CVR, 74 years being the highest age limit (FINRISK score), and recommendations for the management of individual CVRFs, which were not consistently available in any country. For hypertension, the ESC issued specific guidelines for individuals aged 80+, which set cut-off values for both lifestyle and pharmacological interventions to SBP > 160 mmHg and DBP > 100 mmHg [37]. The Dutch guidelines also provided advice for older adults and hypertension: pharmacological therapy was recommended for SPB > 140 mmHg if an initial lifestyle intervention did not result in an improvement, and SPB > 160 mmHg did not prompt immediately a pharmacological treatment for individual aged 80+, but lifestyle management was recommended first. The French guidelines had more lenient criteria for the pharmacological treatment of dyslipidemia in people aged 80+: initiation was not recommended, and continuation was advised only for patients with additional risk factors, lack of non-cardiovascular pathology and good treatment tolerance. Only the Finnish guidelines had age-specific recommendations for management of overweight/obesity in old individuals, for whom 25≤BMI < 30 was considered as a BMI in the normal range, and did not prompt a lifestyle intervention. In all three countries, the dietary guidelines had specific sections dedicated to older adults, and focused on ensuring sufficient nutrition among frail older adults with comorbidities. Among healthy older adults, the dietary recommendations for CVD prevention were similar to those of younger adults.
For physical activity, all guidelines adjusted the recommendations depending on the general health status, prevention level (primary or secondary), and presence of comorbidities, rather than age. Regular mobility and balance training was additionally recommended in Finland and France.
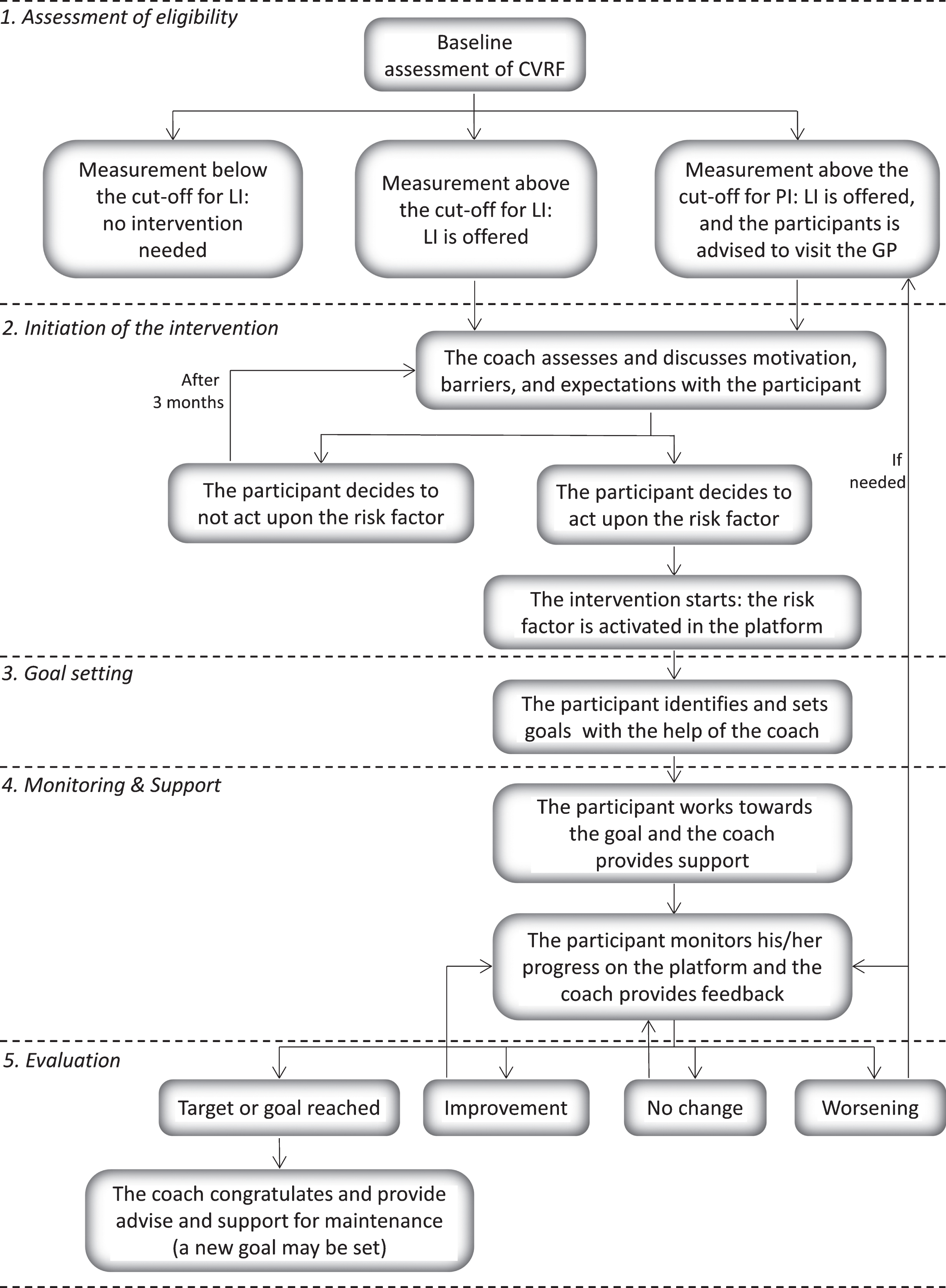
Generic algorithm of the multidomain intervention applied to all the risk factors considered. CVRF, cardiovascular risk factor; LI, lifestyle intervention; PI, pharmacological intervention; GP, general practitioner.
In conclusion, a consistent approach aimed toward elderly individuals could not be identified across the guidelines analyzed. This is in keeping with recent evidence [10], and constantly affects CVRFs management in older adults.
Design of the generic HATICE intervention
Self-determination, management of realistic expectations, assessment of barriers, and goal setting are the key underlying principles included in the HATICE intervention, to promote and maintain behavioral change. They were applied based on the “Bandura’s theory for self-management and behavioral change” [29], through a blended approach that combined the platform functionalities with the remote support of the coach.
A generic algorithm structured in five main phases was designed to define the multidomain intervention for all the CVRFs (Fig. 1):
Cut-off values that determine, for each cardiovascular risk factor, the recommendation to either initiate a lifestyle intervention or seek medical advice for the HATICE participants within the intervention arm
BMI, body mass index; CVD, cardiovascular disease; DBP, diastolic blood pressure; DM, diabetes mellitus; LDL, low-density lipoproteins; SBP, systolic blood pressure. * The values of blood glucose assessed with different tests and the related ranges are presented in Table 5. ** Nutrition score included qualitative and quantitative information in five diet components: fat, fibers, salt, sugar, and alcohol. Higher results in nutrition score indicate better diet quality.
Definition of eligibility; the participants who could benefit from a lifestyle intervention and/or medical treatment are identified based on cut-off values.
Initiation of the intervention; the coach presents to the participants the results of the baseline assessment, provides feedback about their CVR profile and recommendations on how to improve it, and participants decide which CVRFs they want to act upon.
Goal setting; the participants set “specific, measurable, attainable, realistic, and time bound” (SMART) [38] goals to improve their lifestyle, with the guidance of the coach.
Monitoring and support; the participants record and follow their progress towards a goal or related to the status of a specific CVRF, by entering specific measurements (e.g., blood pressure values) and updates on the platform, and receive feedback and support from both the platform and the coach.
Evaluation of progress; the coach provides appropriate feedback based on what the participants record on the platform: further support, when improvements are not recorded, congratulations and recommendation on how to proceed, when goals are reached.
In order to define the eligibility for the intervention and the monitoring of each CVRF, adjustments were applied to this generic algorithm. Standardized criteria and cut-off values to identify participants eligible for both lifestyle and pharmacological intervention were defined (Table 4).
In the guidelines, the CVR level affected the cut-off values for lifestyle and pharmacological interventions, but it was not consistently assessed in the three countries. Since HATICE inclusion criteria required for an age of 65+ and at least two CVRFs and/or history of CVD or DM, it could be assumed that the majority of the recruited participants had a high CVR, using any of the assessment methods. Therefore, the cut-off values for interventions were set for individuals with high CVR (Table 4).
For DM, given that different tests or different cut-offs were used locally (Table 2), FPGT and HbA1C were selected because routinely available in each country. Three risk levels were then defined for both tests (Table 5). Participants with a blood glucose level beyond the “normal” range were recommended a lifestyle intervention, and were further advised to contact their general practitioner regarding potential pharmacological intervention if they had not discussed their blood glucose status with a doctor in the previous 6 months (Table 4).
Risk levels of diabetes mellitus based on ranges of blood glucose values assessed using different tests
FPGT, fasting glucose plasma test; HbA1C, hemoglobin A1C.
The cut-off value for lifestyle intervention of overweight/obesity was set at BMI≥30. The guidelines reviewed, except the Finnish ones, called for a lifestyle intervention already in overweight people (25≤BMI < 30), regardless of the age. However, an increasing body of evidence suggests that overweight older adults have an overall mortality risk equal or lower than those with normal BMI [39–43]. The increased risk of malnutrition in this age group is widely acknowledged [44–46], and it has been proposed that age-specific BMI cut-offs should be applied to more efficiently detect subjects at risk [47]. Since the broad ultimate scope of HATICE is to promote healthy aging, people with a BMI in the overweight range were, therefore, only recommended to monitor their weight.
Nutrition guidelines were not as standardized as for other CVRFs. Cut-offs were provided mostly for single nutrients but not for foods, except fish, fruits, and vegetables, and overall assessment of the diet requires a complex evaluation of many components. The nutrition questionnaire from an international study for the early prevention of DM complications [48] was adapted, for HATICE, by the consortium’s expert nutritionists, through a consensus process. The questionnaire accounted for all dietary components linked to the CVR profile and included a validated dietary assessment tool [49]. Cut-offs for specific nutrient groups (fat, fibers, sugar, salt, and alcohol), based on both their quality and quantity, were used to identify subjects who could benefit from changes in their diet.
Physical activity was assessed at baseline through the Community Healthy Activities Model Program for Seniors (CHAMPS) questionnaire [50], a thorough validated tool to record weekly levels of physical as well as social and recreational activities. Throughout the intervention, a simplified exercise diary allowed participants to record any relevant activity.
The recommendations provided throughout the intervention were based on the lifestyle components of the guidelines previously analyzed, and were delivered either via the platform or through the interaction with the coach. On the platform, recommendations were delivered through static and interactive education modules in form of text, videos, and pictures [28]. Information included: 1) background information on CVD, 2) recommendations for each individual CVRF, 3) practical tips aimed to translate recommendations in concrete actions that could fit in the person’s daily routine and individual lifestyle, 4) practical examples of “goals” to set during the intervention aimed to lifestyle improvement. To encourage participants to self-manage their risk factors, a tool to monitor personal data was included for each CVRF [28]. Participants were free to access the platform at their own convenience and decide their preferred frequency of use without any specific minimum or maximum requirement.
The coach provided the participants in the intervention arm with advice on their overall CVR and the relevant CVRFs, during both the baseline face-to-face meeting and the trial, and whenever in contact with the participants. Specific events triggered the coach feedback, including when participants set, edited, or updated the progress for a goal; recorded a measurement of a CVRF; or did not use the platform for more than three weeks. Overall, the role of the coach throughout the intervention was to offer motivational support, ensure that goals and expectations were realistic, encourage during the monitoring process, and promote long-term changes integrated in the overall lifestyle of each individual (Table 1). The motivational role of the coach was designed based on the “Stages of changes” model [30, 31], which provides a framework to understand the mental processes involved in behavior change. The model is structured on five distinct stages: pre-contemplative; contemplative; preparation; action; and maintenance. Training on this theoretical model, and related motivational interviewing techniques, was provided to all the coaches prior to the trial. The workload in each country was shared among several coaches from diverse backgrounds. To optimize the consistency in the delivery of the intervention, a detailed coach protocol, which defined and standardized all the actions of the coach during the trial was prepared, regular meetings were organized among the coaches in each country, and once at an international level.
Finally, the intervention delivered through the platform was supported by other interactive features including lifestyle groups (e.g., exercise groups), to promote peer support, and a computer-based cognitive training tool, adapted from a previous trial [51] and aimed to improve cognitive domains more vulnerable to aging (episodic memory, executive function, mental speed, and working memory).
Country-specific adaptations
The intervention was built on a number of key principles, which were kept constant to ensure a uniform approach in the participating countries: the intervention algorithm; the cut-off for eligibility; the functionality of the platform; and the overall components of the information and recommendations provided. However, once the generic intervention was designed, each country implemented minor changes to the coach protocol and platform informative content. Such adaptations accounted for country-specific cultural contexts, aimed to facilitate implementation and sustainability of the intervention and did not modify its substance or the way it was administered. Each country adapted their nutrition recommendations to suggest food items nutritionally equivalent to those mentioned in the generic intervention, but more consistent with local food habits and availability. Advice related to items deemed more relevant in specific countries, because of their high levels of consumption (e.g., liquorice in the Netherlands, and alcohol in Finland), were also added. Different examples of physical activities and exercise were suggested to account for geographical and climate differences. Other adjustments ensured that the intervention complemented with the existing healthcare. For example, Dutch primary care nurses have extensive experience in supporting smoking cessation. Therefore, as not to interfere with primary care policies, the Dutch coaches referred participants to primary care nurses for information on any type of medication aimed to support smoking cessation. Additionally, advice on non-supervised use of nicotine replacement therapy was removed from the Dutch platform. Finally, minor adaptations of the coach protocol and the platform were implemented to account for ethnic differences in countries with more heterogeneous populations.
DISCUSSION
Current evidence suggests that CVRFs are not optimally controlled in a significant proportion of older adults [3, 52], which offers opportunities for intervention. At the same time, international experts and the WHO have called upon governments, world-wide, to make prevention of dementia one of their key health priorities [53–56]. Although the clear nature of the relationship between CVD and dementia is yet to be unraveled, the two conditions share several risk factors, therefore it is plausible to suppose that acting on lifestyle and CVRFs could help prevent not only CVD but also cognitive impairment [57–59]. Findings from recent RCTs [16–18] support beneficial effects of multidomain strategies, but robust evidence is lacking on how and to what extent older adults can benefit from lifestyle changes. The aim of the study was to develop a generic, evidence-based multidomain intervention administered through the internet, and supported by a coach, to improve the CVR profile of older adults. Although several medical-related risk factors were considered in the RCT, HATICE was not designed to compete with regular healthcare, but rather complement it; this was achieved by placing lifestyle management and improvement at the core of the intervention. The intervention had to be easily and consistently applicable in Northern, Central and Southern European settings. As a result, a balance was required between standardization of its design and compliance with national guidelines for CVRFs management, which were the backbone of the HATICE intervention, together with the ESC guidelines. National recommendations were used to define cut-off values for the included CVRFs as well as for the lifestyle advice provided throughout the intervention, while the ESC guidelines were the overarching reference when discrepancies among the national documents were identified. To ease and optimize the implementation of the intervention, minor country-specific modifications were also made to account for differences in culture, geography/climate as well as healthcare systems.
Extensive similarities among the guidelines allowed the definition of a uniform intervention for most of the risk factors by directly integrating the national guidelines, with only few exceptions. For DM risk categories linked to specific cut-offs were created to facilitate the use of different country-specific routine tests. For diet, as no assessment tool standardized for all the countries was identified, a short nutritional questionnaire, with validated elements to assess dietary components relevant for CVD prevention, was selected and adjusted to meet cross-cultural requirements. For BMI, the intervention accounted for recent scientific evidence of the role played by age.
Overall, national and European guidelines lacked comprehensive and consistent recommendation for the management of CVRFs in older adults, which meant that the HATICE intervention strategy could not always be fully tailored to the target population. This reflects both the complexity of prevention in advanced age, where primary and secondary prevention can coexist, for example when considering individual risk factors as actual diseases, and the paucity of RCT-derived knowledge of optimal treatment thresholds and therapeutic targets in older adults. Significant differences existed among the guidelines analyzed in the assessment of the overall CVR. However, they did not impact the intervention design, as the recruited population was specifically selected to be at high risk of CVD. Differences were also apparent in the recommendations for pharmacological treatment, reflecting ongoing debates about optimal therapeutic targets for CVRFs for older adults. For instance, although the ESC guidelines for hypertension suggest higher BP values for individuals aged 80+, whether to control BP more or less strictly in older adults is still open to debate. Almost a decade ago, one of the few trials conducted still to date on very old adults (80+ years) [60] supported antihypertensive treatment for SBP≥160 mmHg, and therapeutic targets set at SBP < 150 mmHg and DBP < 80 mmHg. Recently, a trial aiming to compare intensive (<120 mmHg) versus standard (<140 mmHg) SBP targets reported that a more intensive BP control in individuals aged 75+ was beneficial for cardiovascular morbidity and mortality [61]. However, a significant proportion of its participants experienced orthostatic hypotension, which has been shown to increase the risk of dementia [62]. Similar issues exist for dyslipidemia [63, 64]. Recommendations to initiate or modify pharmacological treatments were used in HATICE only to identify subjects who should be referred to primary healthcare, therefore differences on pharmacological recommendations did not affect the design of the intervention. As change in medication use is recorded during the HATICE trial, the analysis of these data might contribute to better understand the role of pharmacotherapy in older adults.
E-health solutions with interactive features could provide a simple, cost-effective, and widely accessible tool to increase awareness, educate, and promote self-management of CVRFs through improvement of lifestyle and adherence to pharmacological treatments, all relevant issues when planning public-health programs. The HATICE platform was successfully tested in a pilot study, and the full trial, which has included more than 2,500 participants, is now ongoing [19]. If shown to be efficacious, it will be crucial to see if and to what extent such internet-based approaches can reach different populations, including assessment of the potential to increase inequalities.
In conclusion, despite existing differences in the management of CVRFs, healthcare organization, and lifestyle habits within HATICE participating countries, a generic multidomain intervention could be designed and implemented uniformly. The design of the intervention was approached pragmatically, taking into account existing guidelines and recent scientific evidence from studies in older adults. A certain degree of flexibility was allowed in each country for the implementation of intervention, and minor adjustments were made locally to ensure adherence to the national guidelines. Given the constant evolution of the recommendations for the management of CVRFs, this adaptability could be of great help in future and larger applications. The HATICE trial can contribute to refine the knowledge on affordable strategies to manage CVRFs in older adults, and help to define Europe-wide applicable preventative programs for CVD and dementia.
ACKNOWLEDGMENTS
The research leading to these results has received funding from the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement n° 305374. The study has also been funded by the “Multimodal preventive trials for Alzheimer’s Disease: towards multinational strategies-programme: MIND-AD”, Academy of Finland (291803) and VTR, Kuopio University Hospital (5772815), Swedish Research Council (529-2014-7503), The Stockholms Sjukhem foundation, the Netherlands Organization for Health Research and Development, (733051041), and the French National Research Agency (ANR-14-JPPS-0001-02). The authors thank Lindsay Allen, and Jenni Lehtisalo, for the help provided with the design of the intervention; and Stéphanie Savy for the support with the implementation of the trial.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/17-0858r1).
Full list of the members of the HATICE study group:
Sandrine Andrieu, Mariagnese Barbera, Cathrien Beishuizen, Carol Brayne, Nicola Coley, Juliette Guillemont, Marieke Hoevenaar-Blom, Susan Jongstra, Miia Kivipelto, Francesca Mangialasche, Yannick Meiller, Eric P Moll van Charante, Tiia Ngandu, Edo Richard, Hilkka Soininen, Bram van de Groep, Willem A van Gool, Tessa van Middelaar, Lennard van Wanrooij.