
Abstract
Background:
Therapeutic research on Alzheimer’s disease (AD) has moved to intercepting the disease at the preclinical phase. Most drugs in late development have focused on the amyloid hypothesis.
Objective:
To understand the magnitude of amyloid-related functional decline and to identify the functional domains sensitive to decline in a preclinical AD population.
Methods:
Data were from the Religious Orders Study and the Rush Memory and Aging Project. Cognitive decline was measured by a modified version of the Alzheimer’s Disease Cooperative Study Preclinical Alzheimer Cognitive Composite. The trajectories of functional decline, as measured by the instrumental and basic activities of daily living, were longitudinally modeled in 484 participants without cognitive impairment at baseline and having both a final clinical and a postmortem neuropathology assessment of AD.
Results:
Individuals with different final clinical diagnoses had different trajectories of cognitive and functional decline. Individuals with AD dementia, minor cognitive impairment, and no cognitive impairment had the most, intermediate, and least declines. While individuals with pathologic AD had significantly more cognitive decline over time than those without, the magnitude of difference in functional decline between these two groups was small. Functional domains such as handling finance and handling medications were more sensitive to decline.
Conclusion:
Demonstrating the functional benefit of an amyloid-targeting drug represents a significant challenge as elderly people experience functional decline due to a wide range of reasons with limited manifestation attributable to AD neuropathology. More sensitive functional scales focusing on the functional domains sensitive to decline in preclinical AD are needed.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative disease characterized by progressive cognitive and functional decline. Most therapeutics in late development [1–3] focus on the amyloid-β (Aβ) hypothesis, which postulates extracellular Aβ deposits are the fundamental cause of AD [4–7]. The Aβ deposition usually starts years before the diagnosis of AD [8] and leads to the formation of neuritic plaques and neurofibrillary tangles. With failures of several phase III studies conducted in mild-to-moderate AD [1, 9], therapeutic research in AD has moved to intercepting the disease earlier. A recently published guideline has outlined a preclinical phase of AD in which patients have no obvious cognitive impairment but abnormal Aβ levels [10]. Treating people in this preclinical stage of AD with an Aβ-targeting intervention may prevent or slowdown the development of AD.
Sensitive cognitive measures have been derived for clinical trials conducted in preclinical AD to demonstrate drug efficacy on preventing or slowing down cognitive decline [11–13]. Using data from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) and the Australian Imaging, Biomarker & Lifestyle Study of Ageing, one study showed that individuals who were asymptomatic but had abnormal Aβ levels at baseline had more cognitive decline as measured by the Alzheimer’s Disease Cooperative Study Preclinical Alzheimer Cognitive Composite (ADCS-PACC) than individuals who had both normal cognition and normal Aβ levels at baseline [11]. The ADCS-PACC can be used as an endpoint in clinical trials conducted in preclinical AD to measure drug efficacy on cognition. The gap between the trajectories of Aβ+ and Aβ– groups can be deemed as the maximum benefit an Aβ-targeting intervention can achieve on slowing cognitive decline. A recent guideline from FDA states that while effect on a valid and reliable cognitive assessment may be sufficient for a marketing approval in trials conducted in preclinical AD, a long-term functional benefit is still required to support the approval (FDA Guidance ucm338287).
To derive a sensitive scale for tracking functional decline in preclinical AD, another study longitudinally modeled the trajectories of functional decline as measured by the Cognitive Function Instrument (CFI) between clinical progressors (Clinical Dementia Rating Scale (CDR) >0.5) and non-progressors (CDR remained 0) as well as between APOE ɛ4 carriers and non-carriers in 468 healthy older individuals enrolled in the ADCS Prevention Instrument study [14]. In this study, while APOE ɛ4 carriers had more decline in CFI over time than non-carriers, the difference in CFI decline between clinical progressors and non-progressors was much more significant. This indicates the magnitude of difference in functional decline between individuals with and without a risk biomarker can be quite different from between individuals who developed the clinical symptoms of AD and those who stayed healthy. By the same token, differences in functional decline observed between clinical progressors and non-progressors may not represent the difference between individuals with and without the Aβ pathology. Understanding the magnitude of Aβ-related decline in functional instruments and the subsequent temporal relationship with cognitive decline will help us understand the maximum functional benefit achievable by interventions conducted in target populations.
Most functional scales used in AD and dementia focus on measuring the patients’ ability to live independently and to perform instrumental/basic activities of daily living (IADL/BADL) [15–19]. While impairments in the cognitive domains, especially in the memory domain, can be observed in very early stage of AD, impairments in the functional domains are typically observed during later stages. As outlined in the Functional Assessment Staging of Dementia [20], a scale that mirrors the characteristic progression of functional loss in AD to 7 stages from normal to very severe cognitive decline, AD patients typically lose their abilities to perform IADL (such as planning dinner for guest, handling finance, shopping) during stages 4 and 5 and their abilities to perform BADL (such as bathing, dressing, toileting, walking) during stages 6 and 7. Functional scales with signal in the earlier stages of AD are clearly needed. Identifying the functional domains that decline early in preclinical AD will provide valuable information for developing a sensitive functional scale to measure the short-term functional benefit of intervention.
The Religious Orders Study [21] and the Rush Memory and Aging Project [22] are two large, community-based, longitudinal clinical-pathological cohort studies of aging and AD. Although this population is relatively older than the preclinical AD population targeted by most clinical trials, it provides a unique opportunity to examine the relationship between AD neuropathology and functional decline in a large number of individuals. Using various modeling approaches, we previously showed that AD pathology is related to the trajectory of cognitive decline over multiple years prior to death stretching to the initial examination [23–25]. In this study, we extend our work to functional change. We longitudinally model cognitive and functional decline in individuals asymptomatic at baseline, based on their subsequent pathologic diagnosis of AD, to understand the potential magnitude of Aβ-related functional decline. We also model cognitive and functional decline based on final clinical diagnoses such as AD dementia, mild cognitive impairment (MCI), or no cognitive impairment (NCI) to understand whether neuropathology can account for all the symptomatic differences observed among individuals with different final clinical diagnoses. Finally, we model the trajectories of individual functional domains to identify the functional domains sensitive to decline in preclinical AD. These analyses will provide valuable information to designing a clinical study to demonstrate the functional benefit of intervention.
MATERIALS AND METHODS
Participants
Subjects included in the current analysis were from the Religious Orders Study (ROS) [21] and the Rush Memory and Aging Project (MAP) [22]. The participants of ROS were older Catholic nuns, priests, and brothers from more than 40 groups across the United States. The participants of MAP were older community-dwelling persons from ∼40 retirement communities and senior subsidized housing facilities across northeastern Illinois. All participants consented to annual detailed clinical evaluation and brain donation at the time of death. Both studies were approved by the Institutional Review Board of Rush University Medical Center. At the time of the analysis (11/11/2013), 2,822 had enrolled and fewer than 5% dropped out during a total of 19 years of the 2 studies; 1,300 had died and 1,049 autopsies were performed with an autopsy rate in excess of 80%. Although both studies primarily enrolled older persons without known dementia at baseline, persons with MCI or mild dementia were also enrolled. For current analysis, we focused on participants who had a clinical diagnosis of NCI at baseline and had both a final clinical diagnosis of AD, MCI, or NCI at the time of death and a postmortem assessment of AD neuropathology by CERAD. Twenty-two individuals had fairly low Mini-Mental State Evaluation (MMSE) [26] total scores (<25) at baseline despite a clinical diagnosis of NCI. These 22 individuals were excluded from analysis. For simplicity, individuals with causes of cognitive impairment other than AD based on the final clinical diagnosis were also excluded. The final analysis set included 484 individuals (see Supplementary Materials for details on sample size derivation). The maximum follow-up time was 15 years and the mean and median of follow-up time were 6.9 and 6.5 years, respectively, in the subset analyzed.
Cognitive performance tests
Twenty-one cognitive performance tests were administered annually in ROS and MAP with 19 tests in common. Current analysis focused on four cognitive tests needed to construct a modified version of the ADCS-PACC (mADCS-PACC) [11]: 1) the Word List Recall score from the CERAD Neuropsychological Assessment Battery [27], 2) the delayed recall score on the Logical Memory IIa subtest from the Wechsler Memory Scale [28, 29], 3) the Digit Symbol Substitution Test score from the Wechsler Adult Intelligence Scale Revised [30], and 4) the MMSE total score [26, 31]. Each of the four component scores was divided by the baseline sample standard deviation of that component to form a z-score. The z-scores were summed to form the mADCS-PACC (see Supplementary Materials for differences between mADCS-PACC and ADCS-PACC).
Functional performance measures
The individual’s ability to perform IADL and BADL was measured by self-report. The IADL were measured with 8 items, including telephone use, meal preparation, light housekeeping, heavy housekeeping, handling medications, handling finance, shopping, and travelling within the community. The BADL were measured with 6 items, including bathing, dressing, eating, toileting, walking across a small room, and transferring from bed to chair. Each item had 3 possible scores: 1 – no help; 2 – help; 3 – unable to do. In case a participant never had an opportunity to perform an activity, the participant was asked to answer the question based on whether (s)he thought (s)he was able to perform the activity. An IADL total score similar to the Lawton IADL total score [15] and a BADL total score similar to the Katz Index of Independence [16] were formed by counting the number of items the participant needed help, i.e., items with scores 2 or 3. The IADL and BADL total scores ranged from 0 to 8 and from 0 to 6, respectively, with higher scores indicating more disability. To understand whether functional decline can be measured more sensitively by measuring each item more quantitatively, an alternative IADL total score was formed by summing the 3-level individual item scores. This alternative IADL total score ranged from 8 (no disability) to 24 (100% disability).
Clinical diagnoses of AD, MCI, and NCI
Participants in both studies underwent structured, annual clinical evaluations. A decision tree was implemented to inform several clinical diagnoses, including AD dementia and MCI. Persons without dementia or MCI were labeled NCI [32]. It combined data reduction techniques for the cognitive performance tests with a series of discrete clinical judgments made by a neuropsychologist and an examining clinician. A final clinical diagnosis was rendered, blinded to all postmortem data, at the time of death by a neurologist with expertise in dementia after reviewing all available clinical data. Case conferences including one or more neurologists and a neuropsychologist were used for consensus on selected cases requiring adjudication.
Postmortem neuropathological diagnosis of AD
Brains of deceased subjects underwent complete macroscopic evaluation as described previously [33–37]. The diagnosis of pathologic AD was assigned by a board-certified neuropathologist blinded to all clinical data. It was based on semi-quantitative estimates of neuritic plaque density as recommended by CERAD [38] implemented without adjustment for age and clinical diagnosis [34], and Braak stage [39] to make a pathologic diagnosis by National Institute on Aging-Reagan criteria [40]. For current analysis, we used only the CERAD, which required moderate or frequent neuritic plaques in one or more neocortical regions as the pathologic criterion for AD as we were interested in the potential effects of an Aβ-targeting therapeutic.
Statistical analysis
Linear mixed effect models (LMEs) were applied to model the trajectories of cognitive and functional decline. Separate LMEs were fitted for the mADCS-PACC, the IADL total score, and the BADL total score to compare the trajectories of cognitive and functional decline among individuals with different final clinical diagnoses. Separate LMEs were also fitted for above scales and the 3-level individual IADL/BADL items to compare the trajectories of cognitive and functional decline between individuals with different pathologic diagnoses (see the Supplementary Materials for details). Briefly, for each cognitive or functional measure, the trajectories of individuals with different final clinical or pathologic diagnoses were modeled together in a single LME model as a function of follow-up year, age at baseline, gender, years of education, APOE status (ɛ4 carrier or non-carrier), study (ROS or MAP), and final clinical diagnosis (AD, MCI, or NCI) or pathologic diagnosis (AD or non-AD) (Supplementary Tables 2 and 3). Time (follow-up year) was treated as a continuous variable. Subject-level intercept and slope were included as random effects. Subject-level quadratic term of follow-up year was also included as a random effect as suggested by the likelihood ratio test comparing the models with and without the quadratic random effect. The null hypothesis of no quadratic random effect was rejected based on the usual asymptomatic distribution, which was conservative in protecting against the use of oversimplified covariance structures when the null hypothesis was at the boundary of the parameter space. For each cognitive and functional measure, separate trajectories and their associated 95% confidence intervals (CI) were estimated from the model for individuals with different final clinical or pathologic diagnoses. Welch’s approximate t-test [41] was used to determine whether two trajectories were different at each visit between individuals with different diagnoses (Supplementary Tables 4 and 5). A standardized difference was also derived at each visit to measure the magnitude of difference (effect size) between the two trajectories. The maximum standardized differences over time (d-Max) represented the maximum effect size over time. The effect sizes were also estimated using a different approach, mixed models for repeated measures, to ensure they were not drastically over or under-estimated by LMEs (see Supplementary Materials). All statistical analyses were performed using SAS 9.2 (http://www.sas.com).
RESULTS
Among the 484 participants, 279 (57.6%) had pathologic AD; 107 (22.1%), 125 (25.8%), and 252 (52.1%) had clinical diagnoses of AD dementia, MCI, and NCI, respectively (Table 1). Individuals with pathologic AD were older at baseline, more likely to be female and APOE ɛ4 carriers. Individuals with AD dementia were older, and with MCI intermediate in age. Individuals with AD dementia were more likely to be female. Individuals with AD dementia had the lowest mADCS-PACC and those with NCI the highest mADCS-PACC at baseline (p < 0.0001). No difference in the IADL or the BADL total score was observed by pathologic or final clinical diagnoses at baseline.
Demographics and baseline characteristics in individuals asymptomatic at baseline by neuropathological or final clinical diagnosis of AD
Data shown are Mean (SD) for continuous variables (age, education, mADCS-PACC, IADL total score, and BADL total score) and n (%) for categorical variables (sex, race, APOE status). p-values are from 1-way ANOVA tests for continuous variables and chi-square tests for categorical variables. AD, Alzheimer’s disease; MCI, mild cognitive impairment due to AD; NCI, no cognitive impairment; mADCS-PACC, modified version of Alzheimer’s Disease Cooperative Study Preclinical Alzheimer Cognitive Composite; IADL, instrumental activities of daily living; BADL, basic activities of daily living.
AD dementia was strongly associated with pathologic AD in this subset of ROS/MAP subjects (p-value = 1.2e-13, Table 2). Ninety-five (88.8%) out of the 107 individuals with AD dementia had pathologic AD. However, consistent with previous findings [32, 35], the majority of individuals with pathologic AD were not demented. Specifically, 113 (40.5%) and 71 (25.4%) out of the 279 individuals with pathologic AD had NCI and MCI, respectively, at the time of death.
Association between neuropathological and final clinical diagnoses of AD in individuals asymptomatic at baseline
The trajectories (and their 95% CI) of mADCS-PACC, the IADL total score, and the BADL total score in individuals with different final clinical or pathologic diagnoses are illustrated in Fig. 1. Individuals with different final clinical diagnoses had distinct trajectories of cognitive decline in mADCS-PACC over time (Supplementary Table 3). Individuals with NCI had the least decline, individuals with MCI had intermediate decline, and individuals with AD dementia had the most decline. This was expected because cognitive performance, among other variables, was used to operationalize the clinical diagnosis. Individuals with pathologic AD had more cognitive decline than individuals without. The magnitude of difference in cognitive decline between individuals with and without pathologic AD (d-Max = 0.62) was smaller than it between individuals with and without AD dementia (AD versus NCI: d-Max = 1.80; AD versus MCI: d-Max = 1.12; Table 3).
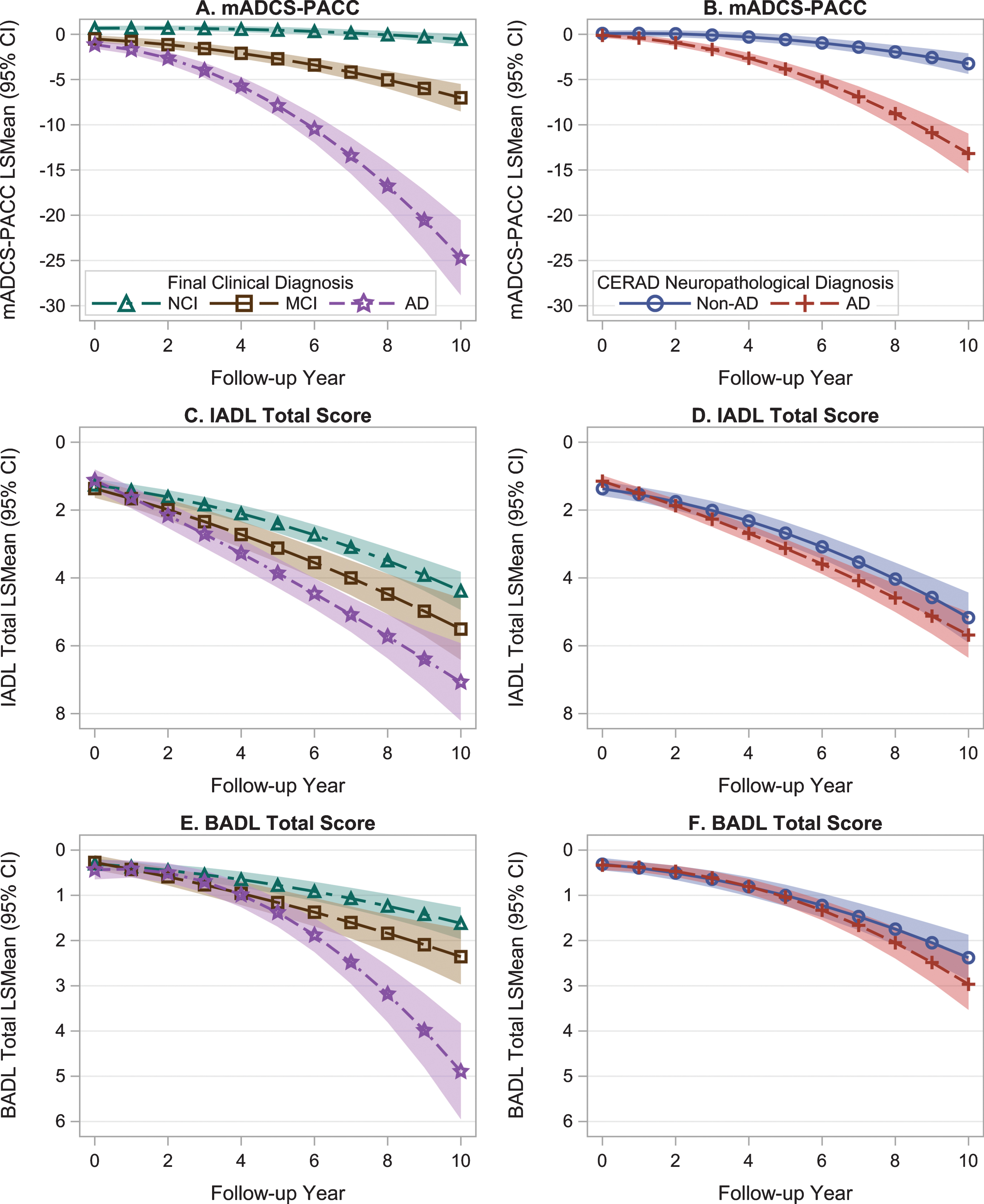
Trajectories of cognitive and functional decline by final clinical or neuropathological diagnosis of AD. Data shown are trajectories and their 95% confidence intervals (shaded regions) estimated from the linear mixed effect models. The y axes for the IADL and the BADL total scores are reversed so that a downward trend indicates deterioration on the corresponding scale. Panels A, C, E are trajectories of mADCS-PACC, the IADL total score, and the BADL total score by final clinical diagnosis. Panels B, D, F are trajectories of mADCS-PACC, the IADL total score, and the BADL total score by CERAD neuropathological diagnosis.
Standardized differences in trajectories of cognitive and functional decline between individuals with different final clinical or neuropathological diagnoses of AD.
Negative numbers indicate individuals without pathologic AD had more decline than individuals with pathologic AD.
Individuals with different final clinical diagnoses also had significantly different trajectories of functional decline over time (Supplementary Table 3). Individuals with AD dementia, MCI and NCI had the most, intermediate, and least declines, respectively. Different from the pattern of cognitive decline in these three groups, individuals’ functional performance declined over time across groups with different final clinical diagnoses. Individuals with NCI had little cognitive decline but substantial functional decline in the IADL and BADL total scores. Individuals with MCI or AD dementia had both substantial cognitive and functional decline. The magnitude of difference in functional decline between individuals with and without AD dementia (AD versus NCI: d-Max = 0.62/0.67 for IADL/BADL; AD versus MCI: d-Max = 0.27/0.47 for IADL/BADL) was smaller than the difference in cognitive decline between the corresponding groups (AD versus NCI: d-Max = 1.80; AD versus MCI: d-Max = 1.12; Table 3). The magnitude of difference in functional decline between individuals with and without pathologic AD was small (d-Max = 0.13/0.12 for IADL/BADL) compared to the difference in cognitive decline between these 2 groups (d-Max = 0.62) and compared to the difference in functional decline between individuals with and without AD dementia (Table 3).
LME was also fitted for the alternative IADL total score calculated by summing the 3-level individual item scores. The magnitude of difference in the trajectories of this alternative IADL total score between individuals with and without pathologic AD was greater than the difference in the trajectories of the IADL total score counting the number of items the participant needed help (Table 3).
The trajectories (and their 95% CI) of individual IADL/BADL items in individuals with and without pathologic AD are illustrated in Fig. 2. The CIs of the trajectories overlapped between the 2 groups across time for most IADL/BADL items except for handling finance and handling medications. The magnitudes of difference in trajectories of these 2 IADL items (d-Max = 0.28 for handling finance and 0.27 for handling medications) were greater than the difference in the alternative IADL total score calculated by summing the 3-level individual scores of all IADL items (d-Max = 0.18, Table 3). A prototype composite was formed by summing the 3-level scores of these two items together. The magnitude of difference in the trajectories of this new composite between individuals with and without pathologic AD was greater than the difference in the trajectories of either item (Table 3).
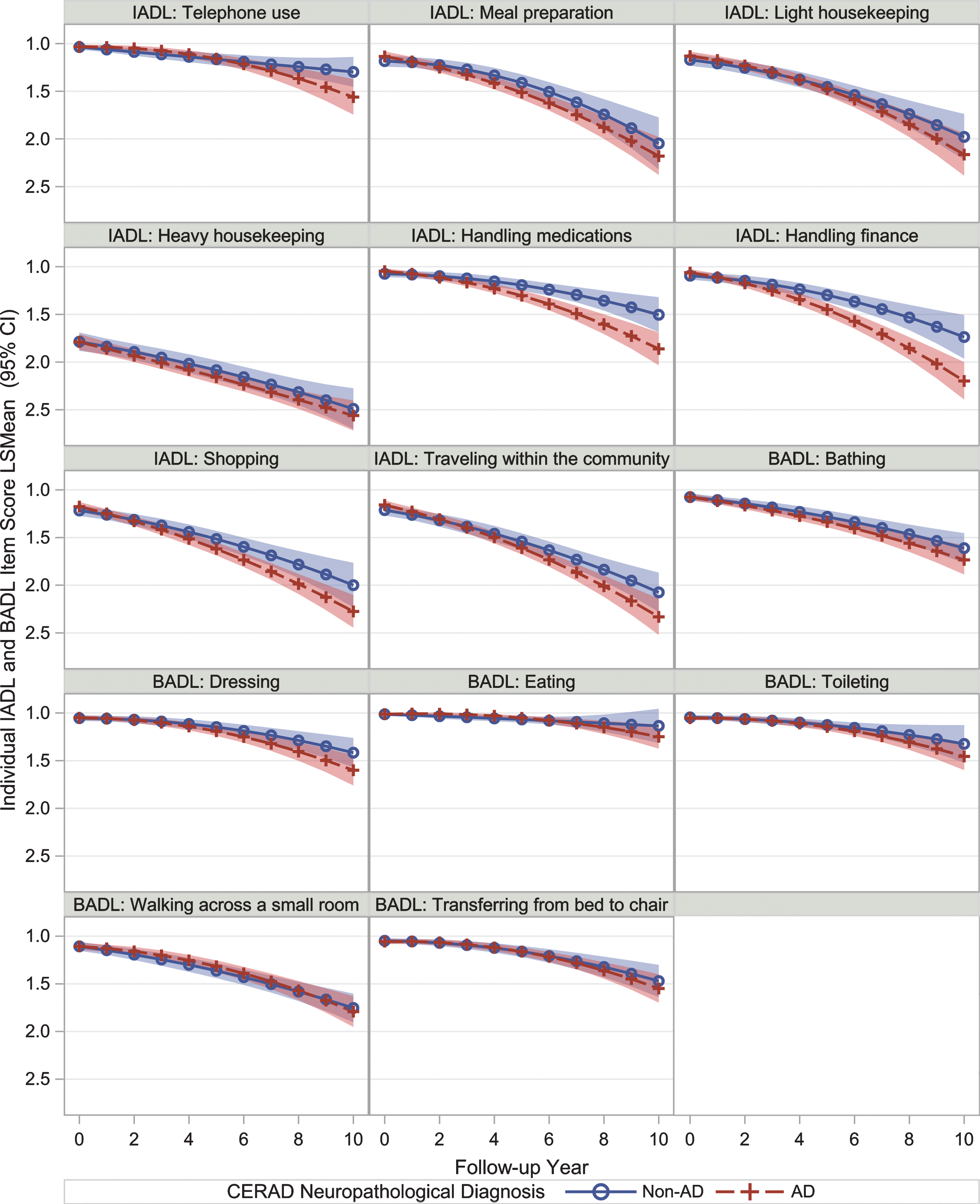
Trajectories of individual IADL/BADL items over time by neuropathological diagnosis of AD. Data shown are trajectories and their 95% confidence intervals (shaded regions) estimated from linear mixed effect models. All y axes are reversed so that a downward trend indicates deterioration on the corresponding scale.
DISCUSSION
Modulation of Aβ turnover represents a promising therapeutic strategy for preclinical AD [3]. The differences in trajectories of cognitive and functional decline between individuals with and without pathologic AD may be considered the maximum clinical benefit that can be achieved by interventions that explicitly target this pathology. Using data from ROS and MAP, we longitudinally modeled the pathologic AD-related cognitive and functional decline in individuals asymptomatic at baseline to understand the magnitude of these differences. Consistent with previous findings [11], individuals with pathologic AD had significantly more cognitive decline over time than individuals without pathologic AD, providing further support that a PACC-like cognitive composite could be used to measure the efficacy of an intervention on slowing down the cognitive decline associated with AD in a preclinical population. However, our findings also indicated that demonstrating short-term functional benefit of intervention may be challenging. Functional performance declined with aging regardless of the AD status in the data. Individuals with a final clinical diagnosis of NCI had very little cognitive decline in mADCS-PACC but significant functional decline in the IADL/BADL total scores over time. The average baseline age of the individuals with postmortem neuropathological data was ∼80 years old, which was older than the typical preclinical AD populations targeted by clinical trials. In this aging population, functional decline may rise from non-Alzheimer neuropathological processes as well as non-neurological comorbidities that produce frailty. As a result, functional scales may be less specific in measuring AD disease progression than cognitive scales that are weighted for episodic memory. This makes it more difficult to show the short-term functional benefit of intervention with commonly used strategies. In our data, the magnitudes of difference in functional decline between individuals with different final clinical or pathologic diagnoses were smaller than the magnitudes of difference in cognitive decline between the corresponding groups. Although a pathologic diagnosis of AD predicted a final clinical diagnosis of AD with high sensitivity, AD neuropathology was often found in subjects with no or mild cognitive impairment. Consistent with previous reports [32, 35], 40.5% and 25.4% of the individuals with pathologic AD had final clinical diagnoses of NCI and MCI, respectively, in our data (Table 2). As a result, the differences in trajectories of cognitive and functional decline between individuals with and without pathologic AD were smaller than them between individuals with and without AD dementia, respectively (Fig. 1). If the maximum functional benefit of intervention is the difference in functional decline between individuals with and without pathologic AD, a fairly large sample size may be required to demonstrate the functional benefit using either the IADL or the BADL total score considering the long follow-up period needed to reach the effect sizes and the high attrition rate in older populations.
Our findings also suggested a few improvements can be made to current functional scales to increase the power to demonstrate the functional benefit of intervention. First, two IADL items, handling finance and handling medications, were more sensitive to decline in individuals who were asymptomatic at baseline and later developed the Aβ neuropathology of AD. The composite combining these two domains had a bigger effect size compared to each individual item as well as the alternative IADL total score derived by summing the 3-level individual item scores, suggesting using a functional composite that focuses on the functional domains sensitive to decline in preclinical AD can increase the power. A performance-based functional assessment, the Financial Capacity Instrument–Short Form, has been used in practice to detect functional impairment in preclinical AD [42]. This instrument has also been incorporated by ADNI-3 [43]. Second, the alternative IADL total score derived by summing the 3-level individual item scores had a bigger effect size than the IADL total score derived by counting the number of items patients needed help, suggesting that measuring each individual functional domain more quantitatively can also increase the power. In practice, performance-based assessments can provide finely grained quantitative measurement using performance scores and task completion time variables, thus increasing the sensitivity of detecting subtle changes in functional abilities [42].
There are a few limitations to the current study. First, the AD pathology status was based on postmortem neuropathology data because brain Aβ burden was not assessed at baseline. Although it may take decades to develop the AD neuropathology, it is still possible some of the individuals with pathologic AD may not have an abnormal Aβ level assessed by a biomarker at baseline. Therefore, the functional decline observed in individuals with pathologic AD at time of death may be slower than the actual functional decline in individuals with an abnormal Aβ level at baseline. Further studies of functional decline in individuals with a biomarker of brain Aβ deposition determined at baseline are needed to give more accurate estimate of the effect size of functional decline. Second, functional performance was by self-report in this study. It has been reported that individuals with cognitive impairment may underestimate their disabilities in performing daily activities [44]. Although we observed significant differences between the trajectories of functional decline between individuals with and without AD dementia, the effect sizes of functional decline associated with clinical or pathologic diagnosis of AD may have been underestimated. It has been shown care-givers may assesse the functional performance of MCI or AD patients more accurately [14, 46]. Alternatively, objective measures collected by performance-based tests or digital devices to track a patient’s ability to perform the daily activities of living, such as the patient’s capability to use computer in daily life and whether the patient is taking medications according to prescribed schedule, may give more accurate and quantitative measures of the patient’s functional performance. Third, our sample was predominantly Caucasian and was from two communities with specific socioeconomic backgrounds. In individuals from different ethnic groups or different socioeconomic environments, different functional measures may emerge as sensitive measures of functional decline in preclinical AD.
In summary, the magnitude of Aβ-related functional decline may be small due to the variability in causes of functional decline in aging populations and the inconsistencies between neuropathology and clinical symptoms of AD. Short-term functional scales that are more quantitative and objective and which focus on the functional domains most sensitive to decline in preclinical AD are needed in clinical trials for demonstrating the functional benefit of potential interventions.
Footnotes
ACKNOWLEDGMENTS
The authors thank the participants and the investigators of the studies reported herein, without whom the studies would never have been accomplished.
The authors acknowledge Drs. Mahesh N. Samtani and Nandini Raghavan (of Janssen Research & Development LLC) for helpful comments.