
Abstract
Background:
There is a growing concern that general anesthesia could increase the risk of dementia. However, the relationship between anesthesia and subsequent dementia is still undetermined.
Objective:
To determine whether the risk of dementia increases after exposure to general anesthesia.
Methods:
A population-based prospective cohort study analyzing the Korean National Health Insurance Service-National Sample Cohort database was conducted of all persons aged over 50 years (n = 219,423) from 1 January 2003 and 31 December 2013.
Results:
44,956 in the general anesthesia group and 174,469 in the control group were followed for 12 years. The risk of dementia associated with previous exposure to general anesthesia was increased after adjusting for all covariates such as gender, age, health care visit frequency, and co-morbidities (Hazard ratio = 1.285, 95% confidence interval = 1.262–1.384, time-varying Cox hazard model). In addition, the number of anesthetic agents administered, the number of exposures to general anesthesia, the cumulative exposure time, and the organ category involved in surgery were associated with risk of dementia.
Conclusion:
In light of the increasing societal burden of dementia, careful surveillance for dementia and prevention guidelines for patients after general anesthesia are needed.
INTRODUCTION
Dementia is a progressive neurodegenerative disease. Dementia is among the leading causes of disability, decreased quality of life and burden to family and society [1, 2]. By 2050, it is estimated that approximately 100 million people will live with dementia worldwide [3]. Given the absence of any effective disease-modifying treatment, there has been growing interest in the identification of potentially modifiable risk factors for dementia [4].
A number of recent studies have indicated the possibility that there has been a decrease in the incidence of dementia, and it is believed that this may be due to better management of chronic disease and earlier intervention than had previously occurred [5]. Key modifiable risk factors for dementia have been identified in earlier work [6–8]. In addition, there is some concern that general anesthesia could increase the risk of dementia [9–11].
Anesthesia has been postulated to have some etiological contribution to postoperative cognitive dysfunction (POCD), a subtle impairment in cognition that has commonly been reported in the post-operative period following surgery [12]. Recent evidence suggests that anesthesia may have a crucial role in POCD by its neurotoxic effect on the brain [13, 14] or through a cortical oxidative stress process. These findings suggest that general anesthesia could also be included as a modifiable risk factor for neurodegenerative disease. Anesthesia and dementia have not been unequivocally linked to date, and investigation of this association is complicated. As it is not possible to conduct placebo controlled randomized trials, well designed observational studies are needed.
In this study, we analyzed a large population-based cohort that is representative of the South Korean population and that was followed for up to 12 years. We sought 1) to determine whether the risk of dementia increases after exposure to general anesthesia, and 2) to evaluate possible associations between the risk of dementia and anesthetic agents, cumulative exposure time, number of general anesthesia episodes and the organ system involved.
MATERIALS AND METHODS
Study population
Data were obtained from the South Korean National Health Insurance Service-National Sample Cohort (NHIS-NSC) database [15]. We extracted data from patient records on file between 1 January 2002 and 31 December 2013. Supplementary Methods and Supplementary Tables 1–4 show the details of the NHIS-NSC dataset and the structure of the data.
All individuals who were younger than 50 years at cohort inception in 2002 or who had a dementia diagnosis prior to undergoing the first recorded exposure to anesthesia in the time period were excluded from analysis. The primary outcome of incident dementia required an ICD-10 code of dementia (F00-F03, G30, and G31) and a documented history of dementia medication (donepezil, rivastigmine, or galantamine). Figure 1 shows the summary flow data for inclusions, exclusions, and outcomes. A total of 219,423 individuals were included in this study, with 44,954 individuals in the general anesthesia group and 174,469 unexposed individuals in the control group. Among them 45,697 individuals died in the follow-up period, and analysis as censored data. This study was approved by the ethics review board of Samsung Medical Center, which waived the requirement for participants’ informed consent. All data were anonymized to maintain confidentiality.
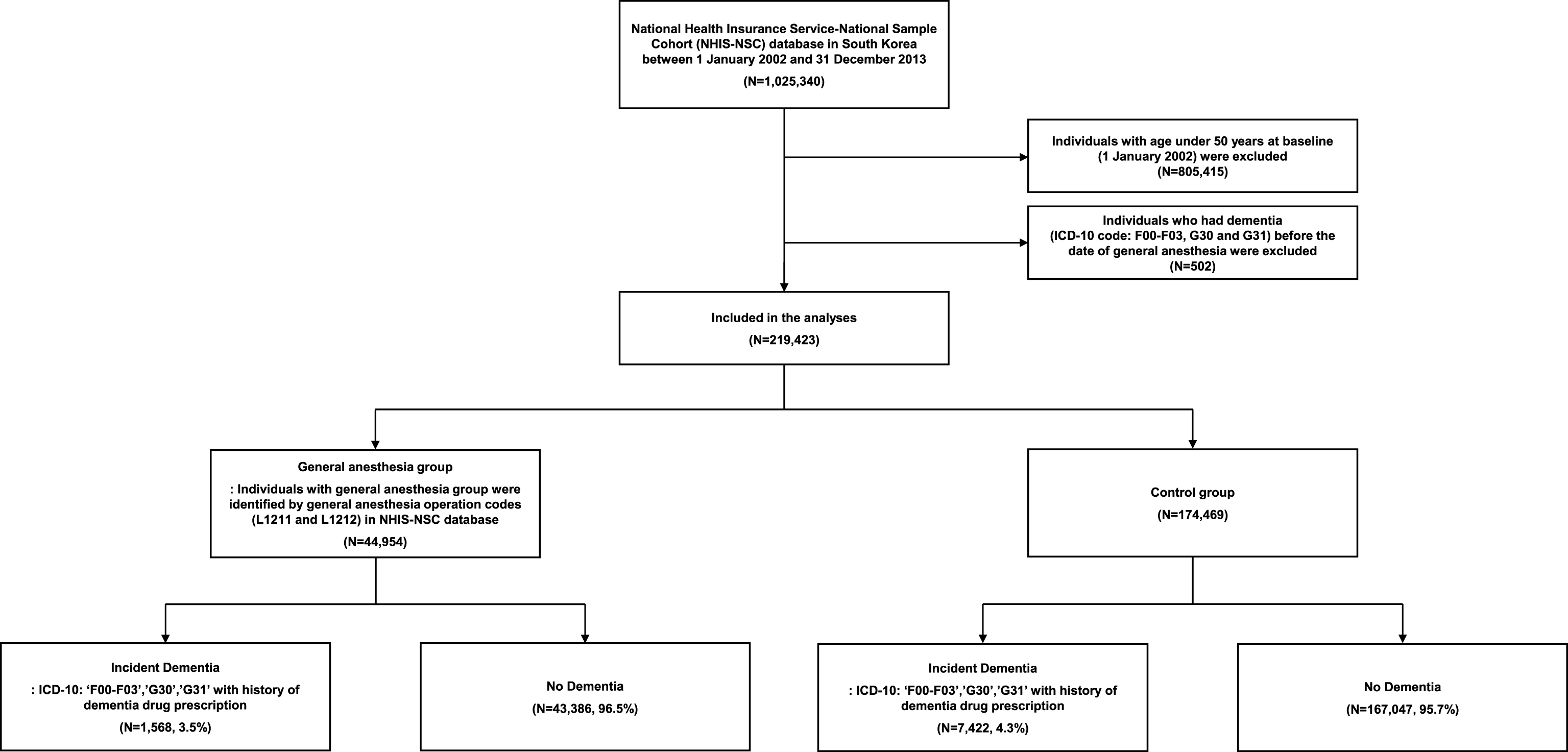
Study flow. From the total 1,025,340 individuals in the National Health Insurance Service-National Sample Cohort (NHIS-NSC) database from 1 January 2002 through 31 December 2013, 805,415 individuals were younger than 50 at baseline and 502 individuals had pre-existing dementia and were excluded from the analyses. Therefore, a total of 219,423 individuals were included in this study, with 44,954 individuals in the general anesthesia group and 174,469 individuals in the control group.
Primary independent variable, outcome of interest, and covariates
Our primary independent variable of interest was the use of general anesthesia. We identified individuals with general anesthesia operation codes (L1211 and L1212) in the NHIS-NSC database. The outcome was overall survival free of dementia. We defined patients with dementia as participants who had ICD-10 codes of all causes of dementia (F00-F03, G30 and G31) and a documented history of cognition-enhancing dementia medication (donepezil, rivastigmine, galantamine, or memantine) [16]. Detailed information on covariates is described in the Supplementary Methods and Supplementary Table 5.
Statistical analysis
For all patients, continuous variables and categorical variables were compared between the general anesthesia and control groups using the t-test and chi-square test, respectively. The first one year period (1 January 2002 and 31 December 2002) was used to exclude pre-existing dementia. The index date of follow-up was 1 January 2002 and the end of follow-up date was 31 December 2013.
We used a time-varying Cox hazard model, which avoids possible time-dependent bias [17]. Because the cohort design created immortal time bias [18], the outcome of dementia could not be assessed before general anesthesia had occurred, the actual observation time differed between the general anesthesia group and the control group (Fig. 2). For that reason, we used hazard ratios (HR, anesthesia group versus control group) rather than incidence data to assess the exposure effect. We used a time-varying Cox hazard model, which avoids possible time-dependent bias [17]. We conducted these analyses first in univariable mode and also in multivariable mode adjusting for gender, age group, health security system, health care visit frequency, and comorbidities (Tables 2 and 3). As can be seen in Results, the raw incidence data during follow-up did not necessarily match the adjusted HR data. In addition, we used the standard Cox hazard model to evaluate possible associations between the risk of dementia and anesthetic agents, cumulative exposure time, number of general anesthesia episodes and organ category of surgery, because time-dependent bias was not involved in these associations.
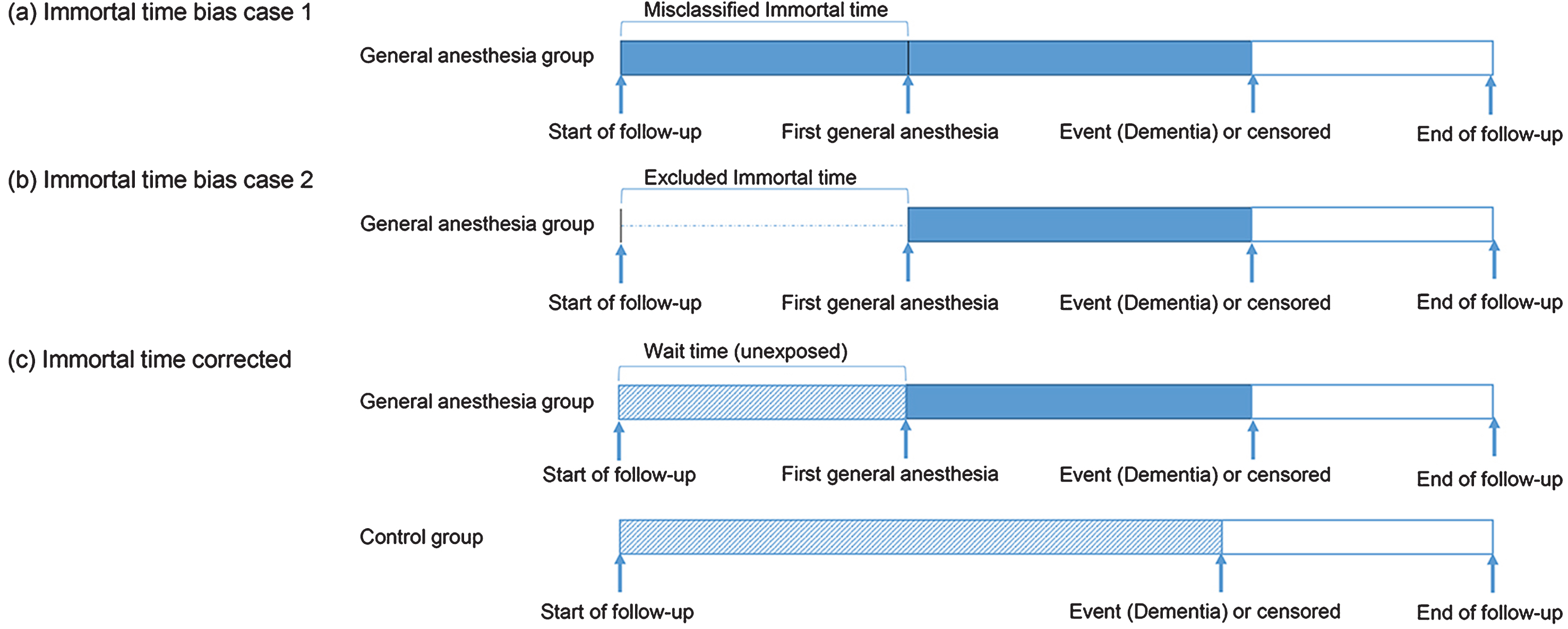
Misclassified immortal time. In observational studies, clinically relevant variables are often time dependent. These variables were often improperly managed in many medical studies using a time fixed survival analysis. Panels (a) and (b) show two typical inappropriate cases which misclassified and excluded follow-up time and treatment status in the study design. In our study, the exposure variable (general anesthesia) status can change during the follow-up period (
Time-varying Cox regression analyses of candidate risk factors at baseline for incidence of dementia
aadjusted for gender, age group, health security system, health care visit frequency, co-morbidities. bCharlson co-morbidity index was not entered as co-variate in multivariable analysis to avoid collinearity. cThe first quartile group had the highest frequency of medical visits.
Hazard ratios of dementia in the anesthesia group in terms of anesthetic agents, cumulative exposure time and number of general anesthesia episodes (Cox regression analyses)
aAdjusted for gender, age group, health security system, Charlson comorbidity index, health care visit frequency and other anesthetic agents. bAdjusted for gender, age group, health security system, Charlson comorbidity index, health care visit frequency. cPatients who received ‘other drug’ were excluded due to lack of detailed information.
Clinically relevant covariates and variables that were statistically significant on univariable analysis were considered as candidate variables in the multivariable time-varying Cox hazard models. We also performed additional analyses in the general anesthesia group in terms of type of anesthetic agents, cumulative exposure time and number of general anesthesia events per patient and type of surgery. The potential collinearity was examined by using a variance inflation factor (VIF) score, and we did not detect any variable with collinearity (VIF >4) [19].
There were multiple differences on the observed baseline characteristics between the general anesthesia and control groups (Table 1). These differences generally favored the control group, except for age-group, and they could lead to biased estimates of anesthesia effect. To reduce the bias, we performed an additional sensitivity analysis by sampling the control group using the propensity score matching method. The propensity score matching method has been widely used to reduce the bias from observational studies through balancing the covariates in the different groups [20]. We estimated the propensity score using logistic regression. The variables with potential association with the anesthesia or the outcome were used in the models. Age group, sex, health security system, co-morbidities, health care visit frequency, and Charlson co-morbidity Index (with binary variable: <3 or ≥ 3) were used. The nearest neighbor matching methods and a 1:1 matching algorithm without replacement were used to identify matches for each individual. The propensity score matching was performed using ‘Matchit’ Packages in R (http://cran.r-project.org). Standardized mean difference and histogram of the distance measure were used to check the success of the propensity score matching.
All p values are 2-tailed, and p < 0.05 was considered significant. All statistical analyses were conducted using SAS (Version 9.3, SAS Institute, Inc., Cary, North Carolina, USA) and R version 3.3.2 for Windows (R Core Team, Vienna, Austria, 2016).
Results
Subject characteristics
The clinical and demographic characteristics of the participants at baseline are presented in Table 1. A total of 44,954 patients (20.5%) were included in the general anesthesia group and 174,469 (79.5%) in the control group. The study population consisted of 98,793 males (45.0%) and 120,630 female participants (55.0%). There were significant differences between groups for gender, age, health security system, co-morbidities, and health care visit frequency.
Clinical and demographic characteristicsa
aGroup comparisons by the chi-squared test. bThe first quartile group had the highest frequency of medical visits.
Risk factors for dementia: Univariable analyses
A total of 8,990 patients were newly diagnosed with dementia during the 12 years of follow-up (Fig. 1 and Supplementary Table 6). Most of them were diagnosed with Alzheimer dementia (76.5%), followed by vascular dementia (10.4%). The raw incidence of dementia was 3.5% in the general anesthesia group and 4.3% in the control group (Fig. 1). Thus, without correction for time of observation it might seem that general anesthesia did not increase the risk of dementia. In the time-varying Cox hazard analyses, however, anesthesia was associated with significantly increased risk of dementia (univariable HR = 1.195, 95% confidence interval [CI] = 1.131–1.262, p < 0.001, Table 2).
The raw incidences of dementia were 0.9%, 4.8% and 9.6% in the age groups 50 to 59 years, 60 to 69 years, and older than 69 years, respectively. The age-stratified HRs in the univariable analyses were consistent with these raw incidences of dementia (Table 2). Dementia was also more likely to be observed in patients in the older age groups, especially in those aged>69 years, compared with those in the reference group aged 50–59 years. The mean duration from general anesthesia to onset of dementia was 9.40 years (standard deviation [SD]±2.09). The duration according to age group was similar (age groups 50 to 59 years [9.50±1.92], 60 to 69 years [9.53±1.97], and older than 69 years [9.14±2.30]).
Risk factors for dementia: Multivariable analyses
The multivariable survival analysis confirmed the main result of the univariable analysis. We observed an estimated 1.285-fold increased risk for developing dementia in the general anesthesia group compared to the control group (95% CI = 1.262–1.384, adjusted p < 0.001, Table 2). The risk of dementia associated with exposure to general anesthesia was increased similarly in males and females after adjusting for all other covariates (Supplementary Table 7). However, the effect of general anesthesia was more prominent in the younger age group than in older age groups (Supplementary Table 7). The interaction effect between age groups and general anesthesia on the risk of dementia was significant (adjusted p < 0.001).
We next conducted a sensitivity analysis by sampling from the control group for propensity matching. The differences between the general anesthesia group and the propensity score matched control group were substantially reduced, especially for gender and co-morbidities (Supplementary Table 8). Both univariable and multivariable analyses confirmed an increased risk of dementia after exposure to general anesthesia in these propensity score matched analyses (multivariable HR = 1.408, 95% CI = 1.314–1.508, adjusted p < 0.001, Supplementary Table 9). The increased risk of dementia after general anesthesia was also robust after the following subgroups were excluded: patients who developed dementia within 3 months after the first anesthesia, dementia other than AD, dementia due to AD and neoplasm related surgery in the first anesthesia. In addition, we found similar results after excluding patients who had undergone neurosurgery or had vascular diseases (Supplementary Table 10).
Anesthetic agents, frequency and cumulative time of exposure to general anesthesia, organ category of surgery and risk of dementia
The risk of dementia differed according to the anesthetic agents administered (Table 3). The hazard ratio of incident dementia was greater in patients who received the anesthetic agents, thiopental, desflurane and isoflurane. Sevoflurane was associated with lower risk of dementia. In addition, the combined use of intravenous anesthetic agents was associated with higher risk of dementia. The patients who received three or more anesthetic agents had a greater risk of dementia than those who received single anesthetic agents. Increasing number of exposures beyond 2 to general anesthesia also was associated with increased risk of dementia. The cumulative time of exposure to general anesthesia over the 12-year period was positively associated with higher risk of dementia. As anesthesia duration increased by one hour, the risk of dementia increased by 1.063-fold. The risk of dementia was prominent in neurosurgery when compared with surgery involving other organ systems.
Discussion
In this nationwide, population-based cohort study of more than 200,000 persons 50 years or older, exposure to general anesthesia was associated with an increased risk for dementia over 12 years. The increased risk of dementia was additional to the effects of age, gender, multiple co-morbidities and health care visit frequency. We found that the increased risk of dementia was prominent in younger persons, patients who received multiple anesthesia agents and who had multiple exposures to general anesthesia. In addition, we demonstrated that the risk of dementia varied according to the anesthetic agents used, the cumulative duration of general anesthesia and the organ systems for which surgery was performed.
Cognitive impairment, usually short-lived, is a well-known complication after general anesthesia; however, a link to other cognitive disorders such as dementia has not been made clearly [21]. Our findings suggest that general anesthesia can increase the risk of subsequent dementia, with persistent cognitive impairment, over the long term. To confirm that the association was not confounded with co-morbidities or short-term effects of surgery, we conducted additional sensitivity analyses with propensity score matching and with exclusion of patients who developed dementia within 3 months after the anesthesia. These analyses also showed robust results. Additionally, we adjusted for health care visit frequency in the survival analyses. By this adjustment, we could reduce the bias that patients who underwent general anesthesia were followed up more frequently, which could have allowed more chances for the dementia diagnosis [22]. Furthermore, we demonstrated dose-response effects of general anesthesia in terms of number of general anesthesia episodes and cumulative exposure time. Thus, our study, with a statistically rigorous design, provides evidence for a relationship between general anesthesia and dementia with a large nationwide population-based cohort study followed for up to 12 years.
Several pathophysiologic mechanisms for linkage between general anesthesia and dementia have been suggested, including amyloid-β protein (Aβ) accumulation, cell death pathways, growth factor signaling systems or neurotransmitter systems [13, 14]. Animal studies have shown that exposure to anesthetic agents can induce memory impairment [23], Aβ accumulation [24] and neuro-inflammation [25]. In addition, multiple anesthetic agents can also promote hyperphosphorylation of the microtubule-associated protein tau found in Alzheimer’s disease (AD) as neurofibrillary tangles [26–28]. These previous findings in animal studies and in in vitro studies are relevant to our observed significant association of general anesthesia with dementia. In our findings, the risk of dementia other than AD after general anesthesia was also increased (Supplementary Table 10). The effect of general anesthesia on brain vascular endothelial cells could be involved in the pathophysiologic mechanisms [29].
An extensive literature has reported the association between general anesthesia and dementia. However, there is no clear consensus for the association. A meta-analysis of case-control studies [30], and a large retrospective population-based nested case-control study [31] found lack of association between general anesthesia and dementia. In addition, a cohort study has reported no increased risk of dementia after general anesthesia [32]. However, these studies were limited by a case-control study design, small cohorts, and short follow-up duration. By contrast, a retrospective cohort study [10] in Taiwan, reported that patients undergoing anesthesia are at higher risk of developing dementia, and a case-control study [11] that analyzed identical cohort data in Taiwan found a significant association between anesthesia and dementia. However, the potential for substantial ascertainment bias due to differences of opportunity for dementia diagnosis according to surgery was raised as a problem [22]. Our study found a significant association between general anesthesia and dementia in an independent cohort in South Korea while controlling for ascertainment bias, and lends support to the increased risk of dementia after exposure to general anesthesia.
In agreement with previous studies, older age was the most significant risk factor for development of dementia (Table 2) [33–35]. As in the previous study in Taiwan [10], we found that the incidence of dementia after general anesthesia was higher in older than in younger age groups. However, the effect of general anesthesia on development of dementia was greater in the younger age group, and the interaction effect between general anesthesia and age group was significant (Supplementary Table 8). Our findings also are in line with a previous study that found a correlation between cumulative exposure to anesthesia and age of onset of dementia in a midlife group [36]. Elderly patients are recognized to be at high risk of POCD; however, our results suggest that clinicians should be concerned about the effects of general anesthesia on longer term cognitive function not only in the elderly but also in middle-aged patients. Whether exposure to general anesthesia at a young age is linked with cognitive disorder in later life has not been established [37]. Further studies with younger cases and a longer follow-up are needed.
A prospective randomized study found that patients who underwent general anesthesia with sevoflurane for lumbar spine surgery showed faster progression of MCI than those who received other anesthetic agents [38]. Furthermore, the effects on AD pathology, such as Aβ peptides and tau hyperphosphorylation differed according to inhalant anesthetic agents in in-vitro and in-vivo studies [39]. These studies imply that anesthetic agents may have a major role in the cognitive impairment after general anesthesia. However, very limited human data have been reported [37]. In our study, we found that thiopental, desflurane, and isoflurane have higher risks than other anesthetic agents. We also saw inconsistent evidence that combined use of anesthetic agents could be hazardous (Table 3). While careful interpretation is needed due to the relatively small subsample sizes and the observational study design, our results suggest a practical strategy for mitigating dementia associated with anesthesia by choosing the least provocative anesthetic agent and by avoiding use of multiple anesthetic agents [37]. Further studies need to be conducted to establish guidelines to select anesthetic agents for mitigation of dementia.
The effect of the surgery itself on risk of dementia was not established. In our study, the risk of dementia after general anesthesia differed according to the organ category involved (Table 3). The most prominent increased risk of dementia was observed in patients who underwent neurosurgery. Additionally, the risk of dementia in patients with digestive organ surgery and ear, nose or throat surgery was lower than for other types of surgery. These results suggest that the surgical procedure also has an independent effect on the development of dementia. In an animal study, adult rats that underwent surgery combined with anesthesia showed more impaired cognitive function compared with rats that were anesthetized without surgery [25]. A speculation is that neuroinflammation triggered by surgical procedures might be involved in cognitive impairment after surgery [40]. Further studies are needed to clarify this issue.
Our study has several strengths. We followed up a nationwide cohort with limited losses, and limited nonresponse bias. The information on co-morbidities was collected prospectively and did not rely on patient reports, therefore, we could reduce recall bias. A previous study applied a time-fixed definition to an exposure which may lead to immortal time bias [10, 18]. Immortal time refers to a period of follow-up during which the study outcome cannot occur by study design (Fig. 2). In our study, the period between enrollment and general anesthesia (a wait period) was considered immortal time by study design, because the patients with general anesthesia have to be free from dementia until the general anesthesia was conducted. Thus, the observational time period in which dementia could develop differed between the two groups. For this reason, direct comparison of the raw, 12-year incident dementia rates (3.5% in the general anesthesia group versus 4.3% in the control group, Fig. 1) could lead to an erroneous conclusion. The results would be substantially biased if the date of first anesthesia exposure was used as the index date in the general anesthesia group, and the first date of follow-up (1 January 2003) was used as the index date in the control group because of mismatch in assignment of the index dates [22]. In this study, we considered time-varying exposure in our study design. Thus, our study results reduce such bias [17].
An important limitation of our study was the lack of data on possible confounding factors such as years of education, occupational attainment, and health-risk lifestyle [41]. We also had no data on general anesthesia episodes before 2002. Another limitation is that the increased risk of dementia development after exposure to general anesthesia could be attributable to intraoperative events or perioperative events including hemodynamic instability, ischemic damage in the brain or metabolic disturbance [10, 42]. Lastly, it is possible that some people with dementia were not diagnosed because they were not given the drugs approved for enhancing cognition in dementia. The NHIS-NSC database is a nationwide medical claims database, and the results of standardized neuropsychological tests or neuroimaging tests are not included in this database. However, any variability in diagnosis of dementia would be similar in both the anesthesia and the control groups. In addition, we included prescription information in the operational criteria for dementia to improve the accuracy of the diagnosis. In South Korea, clinicians are required to document from the medical record the clinical diagnosis of dementia as well as rating scale scores, such as Mini-Mental State Examination [43], Clinical Dementia Rating [44] or Global Deterioration Scale [45], in order to prescribe the medications named in the inclusion criteria of our study. These strict operational criteria compared to previous studies could have increased diagnostic accuracy.
In conclusion, we found that general anesthesia was associated with an increased risk of dementia in a nationwide population-based cohort. Additionally, our results suggest the possibility of modifiable factors including selection of anesthetic agents, and avoiding prolonged anesthesia or combined use of anesthetic agents. In light of the increasing societal burden of cognitive disorder, further research is needed to elucidate the pathophysiologic mechanisms linking general anesthesia and dementia, and to develop guidelines aimed at mitigating cognitive decline as a delayed complication of general anesthesia.
Footnotes
ACKNOWLEDGMENTS
The ethics review board of Samsung Medical Center approved our access to anonymized data sets for these analyses. This research was supported by the Global Research Lab (#K21004000001-10A0500-00710; H Kim) through the National Research Foundation of Korea funded by the Ministry of Science, ICT and future planning, and Basic Science Research Program through the National Research Foundation (NRF) of Korea funded by the Ministry of Education (NRF-2017R1A2A1A17069653; DK Kim, NRF-2017R1D1A1B03029342 and NRF-2018R1C1B6001708; W Myung). This work was also supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2012S1A6A3A01033504; Clara T Kim). This study was also funded by Eisai Inc. The funding source was not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.