
Abstract
During the last few years, dementia prevention based on modifiable lifestyle factors has gained increasing attention. Cohort studies with follow-ups extending up to decades have identified several risk and protective factors, and very recently new randomized controlled trials with multidomain approach have provided promising evidence by showing that modifying simultaneously several risk factors, it is possible to maintain and improve cognitive capacity among older at-risk persons. Several lifestyle-based multidomain trials are under preparation or ongoing and to facilitate international collaboration and effective worldwide dementia prevention, the World Wide FINGERS interdisciplinary network (http://wwfingers.com) was recently initiated. Additionally, several new implementation projects are taking the first steps from trial setting to real-life implementation of a dementia prevention program. This paper highlights the recent perspectives from the field of Alzheimer’s disease and reflects the implications and importance of current achievements. Finally, predictions for the future work especially in terms of global collaboration and implementation will be discussed.
INTRODUCTION
New predictions of the dramatic increase of dementia and Alzheimer’s disease (AD) rates worldwide are alarming [1]. There are currently no cure or disease modifying drugs available and recent drug trials have shown mainly negative results. Consequently, prevention has received increasing attention and has been highlighted as the key element in managing the dementia epidemic. During the last two decades, large prospective cohort studies have provided increasing evidence of risk and protective factors throughout the whole life-course which may contribute to the risk of dementia and AD. Lifestyle matters, since it has been estimated that about one third of AD cases could be attributable to modifiable risk factors [2, 3]. Based on these observational studies, new randomized controlled trials (RCT) have started to test whether changes in these modifiable risk factors could decrease the risk for dementia or slow down the progress of cognitive decline. The first randomized controlled trial, the Finnish Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), showed that modifying simultaneously several risk factors, cognitive capacity of older at-risk adults can be maintained and risk of cognitive decline reduced. Following the success of FINGER, several other countries all over the world are now planning FINGER-type interventions. This international collaboration has created a new World Wide FINGERS (WW-FINGERS) network, where large research groups are combining their forces to act against the increasing burden of dementia. Further, several implementation studies around the FINGER results are ongoing and general guidelines to dementia prevention are under preparation. This short overview describes the evidence that led to the FINGER trial, introduces the FINGER study and related ongoing activities, presents new results from implementation activities, and also discusses future directions mainly in terms of implementation.
LONG HISTORY OF OBSERVATIONAL STUDIES
We know today that cognitive impairment, dementia, and AD are multifactorial disorders, and evidence from observational studies shows that genetic, vascular, lifestyle-related, and other risk factors often co-occur in the same person, and interact across the lifespan to determine the overall risk of developing dementia and AD. Several large prospective cohort studies around the world have been able to identify a large amount of lifestyle-related risk and protective factors that have great influence on dementia incidence at a population level. The Finnish Cardiovascular Risk Factors, Aging and Dementia (CAIDE) study, which was started already in 1998, was among the first large population-based studies showing the importance of lifestyle related risk factors present already in midlife for dementia development. The CAIDE study linked midlife cardiovascular risk factors such as high blood pressure and cholesterol [4], smoking [5], physical inactivity [6, 7], alcohol consumption [8], poor diet [9, 10], and psychosocial factors [11–13] to increased risk of dementia and AD later in life. Within the CAIDE project, the CAIDE risk score, a simple method for the prediction of the risk of late-life dementia in people of middle age on the basis of their risk profiles, was developed [14] (Fig. 1).
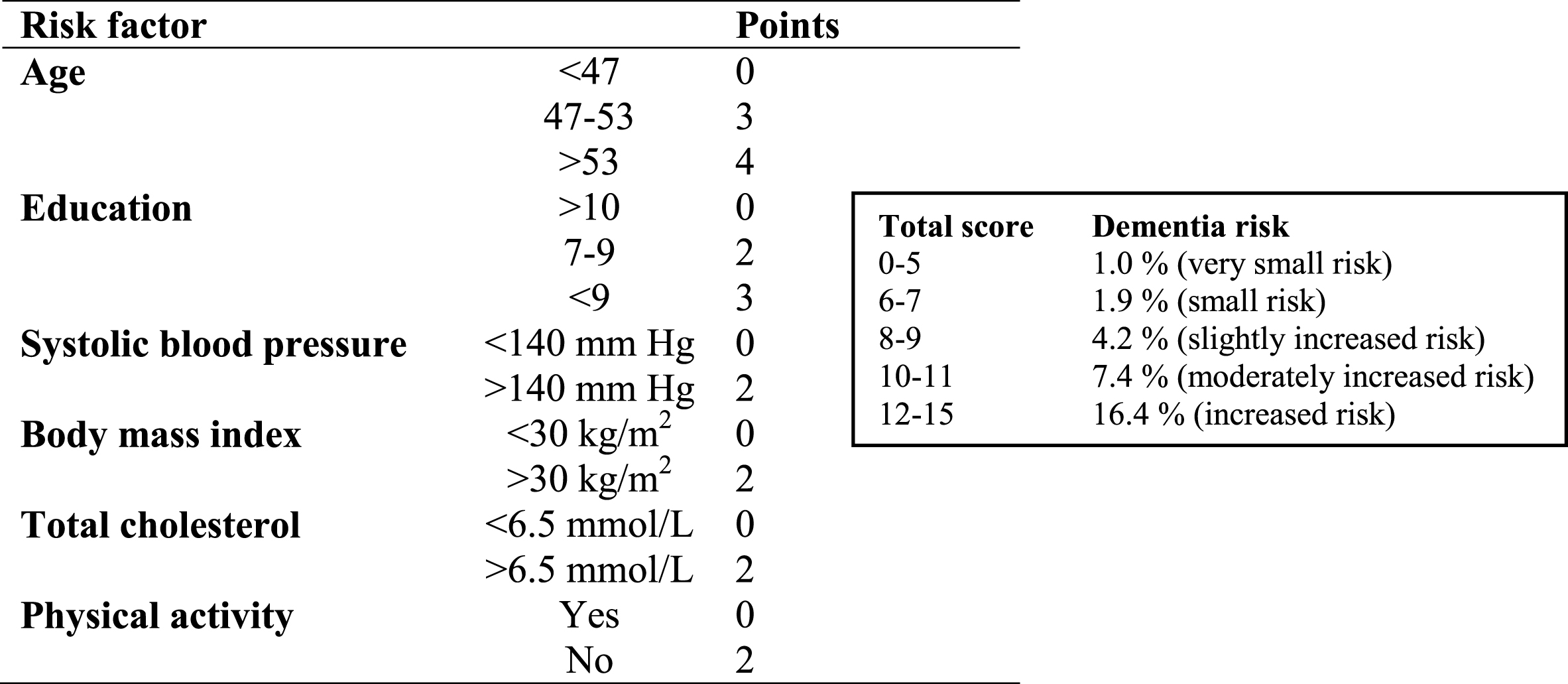
CAIDE risk score for the prediction of the risk of late-life dementia in people of middle age based on their risk profiles [14].
The CAIDE study is still ongoing and current activities include planning the extended follow-up, CAIDE 85+, which will provide opportunity to assess dementia incidence and risk factors among the oldest old, persons aged 90 and over using the follow-up period extending up to 40 years. The CAIDE study has significantly contributed to the current level of evidence on the modifiable risk factors. The risk factors have been a focus of intensive research in the past years, and currently the evidence is strong regarding many of the risk factors (e.g., midlife hypertension, midlife obesity, smoking, education, lack of physical activity), but still less consistent for some other factors, including depression, stress, and social factors. In addition, it is possible that age at the time of risk assessment modifies association between risk factor and outcome. Different risk factors may have critical time window at different time points and risk factors may change during the disease course (e.g., high blood pressure, obesity, cholesterol, and depression). The planned extended CAIDE follow-up study will provide additional evidence and new insights into life-course perspective on cognitive aging.
Technology and internet-based tools are important ways to carry out today’s health education and disease prevention. Recently based on CAIDE risk score, a new CAIDE risk score app was developed [15]. The CAIDE risk score app is the first evidence-based mobile app to predict the risk for dementia. Ongoing development will produce similar easily accessible risk assessment and prevention tools for different age and population groups. For example, the EU-funded project Healthy Aging Through Internet Counselling in the Elderly (HATICE) aims to develop an innovative, interactive internet intervention platform to optimize treatment of cardiovascular disease in the elderly and also to investigate whether cognitive decline can be prevented via internet counselling [16]. In the future, the aim is to make e-health risk assessments tools available around the globe, including in low- and middle-income countries and vulnerable populations.
FROM OBSERVATIONAL STUDIES TO GOLD-STANDARD CLINICAL TRIAL
FINGER [17, 18] is the first randomized controlled trial published showing that intensive lifestyle-based intervention targeting simultaneously to several modifiable risk factors has a beneficial effect on the cognitive capacity of older persons who are at increased risk for cognitive decline [17]. The FINGER trial is a 2-year multi-center RCT carried out in Finland and coordinated by the National Institute for Health and Welfare, Helsinki, and conducted in close collaboration with Universities of Eastern Finland, Oulu and Helsinki (Finland) and Karolinska Institutet (Sweden). The aim of the study is to test the effect of a multi-domain intervention in delaying cognitive impairment and disability in elderly at risk. FINGER enrolled 1,260 participants aged 60–77 years recruited from previous population-based survey cohorts in 2009. Inclusion criteria were: CAIDE Dementia Risk Score >6 points, indicating the presence of modifiable risk factors; and cognitive performance at the mean level or slightly lower than expected for age. Participants were randomized (1:1) into either the multidomain intervention group or the control group. The intervention included nutritional guidance, physical exercise, cognitive training and social activities, and management of vascular risk factors (Fig. 2). The control group received regular health advice.
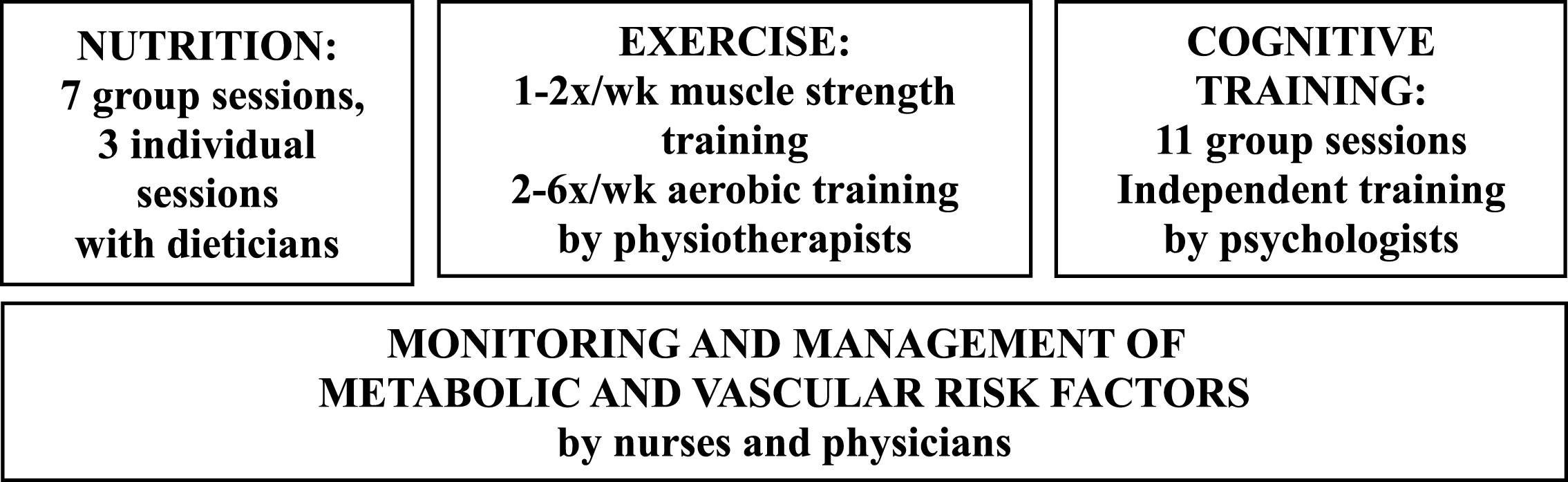
Intervention components in the FINGER trial.
Primary outcome after 2 years was cognitive performance measured by a comprehensive neuropsychological test battery (NTB) composite Z score. An extended follow-up (after 5 and 7 years) with an ongoing sustenance intervention aims to evaluate longer-term effects of the intervention on dementia and AD incidence, and secondary and exploratory outcomes including blood-based biomarkers and neuroimaging with MRI and PET. The 2-year intervention was finalized in February 2014. Already published main results showed that after 2 years, the NTB scores in the intervention group improved 25% more than in the control group. For some cognitive domains, including executive functioning and processing speed, the impact of the intervention was even larger [17]. Currently several secondary outcomes are being analyzed.
Most recent publications have shown that multidomain intervention improved important dimensions of quality of life [19]. Further, participants with shorter leukocyte telomere length had more pronounced benefits on cognition following the multidomain lifestyle intervention [20], which indicates that participants with shorter telomere length had more room for lifestyle improvements when they entered the study. Since shorter telomere length is associated with poor cognitive performance and dementia, the FINGER intervention may be especially beneficial among individuals with increased risk. New results also show that intake of several vitamins and minerals decreased in the control group but remained unchanged or increased in the intervention group during the 2 years [21]. The FINGER study is thus the first large RCT showing that it is possible to prevent cognitive decline using a multidomain intervention among older at-risk individuals. The results highlighted the value of the feasible and novel multidomain approach that is effective for several cognitive domains.
WHAT LIES BEHIND THE SUCCESSFUL FINGER INTERVENTION?
FINGER is currently the only largescale intervention study which has provided evidence of the benefits of the multidomain intervention. Now among the main interests are to find out the factors that influenced the success of this intervention. The ongoing analyses will show how shorter-term adherence to the FINGER intervention (overall adherence and per domain adherence) is related to longer-term adherence to healthy lifestyle changes. This will provide essential information about how to facilitate healthy lifestyle maintenance, and how to optimize the duration of a prevention program. Future analyses will include identifying facilitators and barriers to long-term adherence and identifying effects of adherence level on cognitive decline and dementia incidence. One goal is to tailor the intervention by taking into account how baseline risk level impacts FINGER intervention effects.
One of the main factors behind the success of FINGER intervention was most likely participants’ strong commitment for the study and willingness to lifestyle modifications. Detailed feedback regarding intensive intervention was gathered from all participants who received intervention and came at the 2-year follow-up visit (n = 555). Feedback was gathered using structured questionnaires and questions focused on the self-reported adherence, common experiences, benefits, and usefulness of the intervention. The results showed that participants perceived intensive 2-year FINGER multidomain lifestyle intervention useful, and most participants intended to continue healthy lifestyle after the intervention. The main feedback from the intensive intervention is summarized in Table 1.
Participants’ self-reported adherence, common experiences, perceived benefits and usefulness of the FINGER multidomain intervention (total n = 555)
Intensive FINGER intervention lasted for 2 years and required participation in physical and cognitive activities and dietary counselling as well as regular visits to study nurse and physician. The control group got regular health advice from the study nurse and physician. The study design was kept as double-blinded as possible and participants in the FINGER study were not actively told which group they belong to. After the intervention, participants were asked to report their own assumptions of their randomization. Interestingly, almost half of the participants in the intervention group (44%) did not see themselves taking part of intensive intervention, rather instead they thought they only got regular health advice. This gives positive sign that lifestyle modifications used in the FINGER trial were not perceived too stressful and this type of intervention was feasible among older adults at-risk of cognitive decline.
FINGER STUDY AS A MODEL FOR LIFESTYLE INTERVENTION TRIALS IN SEVERAL COUNTRIES
Following the success of FINGER, several other countries are now planning or already starting FINGER-type interventions to test the effect of the multidomain intervention in their own older populations. To facilitate this international collaboration, in July 2017, World Wide FINGERS interdisciplinary network (http://wwfingers.com) was initiated. This new network aims to share experiences, harmonize data, and plan joint international initiatives for the prevention of cognitive impairment and dementia (Fig. 3). The network is led by Professor Miia Kivipelto and the main goal is to generate robust evidence to define effective preventive approaches for various at-risk groups and settings. World Wide Fingers network makes it possible to test sustainable dementia prevention strategies for populations with different geographical, economic, and cultural settings. During the following years, the FINGER multidomain model will be tested in diverse settings in Europe, Singapore, USA, Australia, and China.
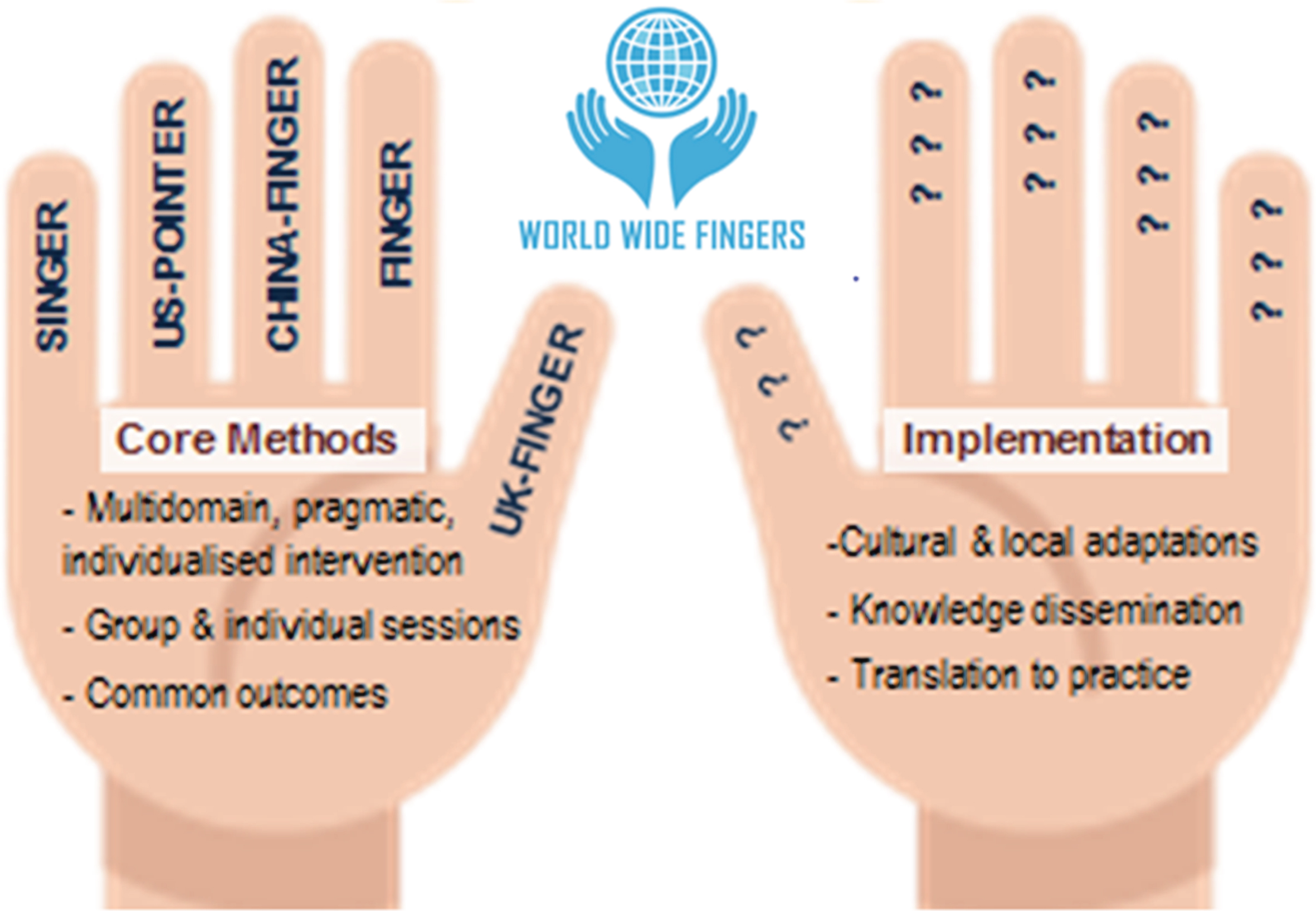
World Wide FINGERS network aims to share experiences, harmonize data, and plan joint international initiatives for the prevention of cognitive impairment and dementia.
FROM RESEARCH TO IMPLEMENTATION: CREATING DEMENTIA PREVENTION TOOLKIT FOR PRIMARY CARE
The FINGER study is considered as a proof of concept trial. It has shown evidence that a multidomain lifestyle intervention results in clear health benefits, and therefore also health care professionals, leaders, and policy makers have shown increasing interest to implement the results into primary care. In close collaboration with key stakeholders, including policy makers, health care managers and other health and social care professionals, the first FINGER-based implementation project called MUISTIKKO began in autumn 2016 in Finland. The purpose of the project is to take the first steps from trial setting to real-life implementation of a dementia prevention program. This project provides detailed information on facilitators and barriers to implementation in primary care. Focus will be on communication and education activities, focus groups, and workshops to discuss with multiple stakeholders the practical details needed for future implementation of the FINGER-based operational model in an integrated dementia prevention program. The aim is to establish links between a dementia prevention model and cardiovascular and diabetes prevention models. Close collaboration with stakeholders and health care professionals provides the possibility to gather important information for preparing an implementation toolkit and guidelines for integrated dementia prevention in primary care. The project will lead to proposed operational model (Fig. 4) which will consist of provision of evidence-based means for early identification of at-risk individuals and provision of evidence-based, sustainable intervention strategies for preventing cognitive impairment, dementia, and disability. Also links between the dementia and cardiovascular and diabetes prevention models will be established.
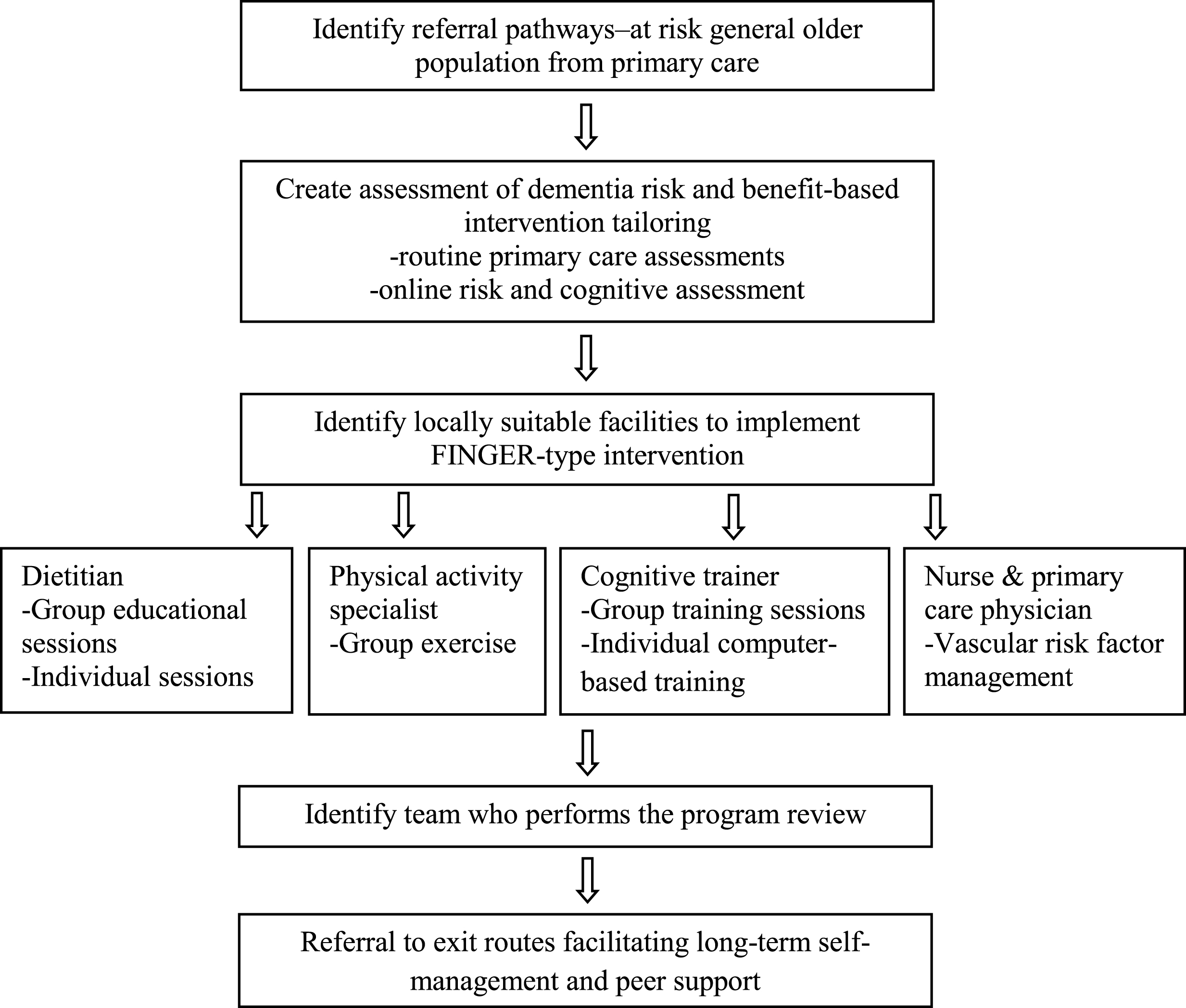
Proposed operational model for preventing dementia and disability.
As a result, this first FINGER-based implementation project will provide primary care physicians and nurses with guidelines on how to use available risk assessment tools for making better intervention-related decisions, and for establishing links between the dementia prevention model and cardiovascular and diabetes prevention models. Using information gathered from communication activities and results from focus groups, the aim is to prepare an easy-to-use implementation toolkit and guidelines for integrated dementia prevention in primary care.
SUMMARY AND FUTURE DIRECTIONS
The current evidence suggests that about 30% of all dementia cases are attributable to modifiable lifestyle related risk factors. Lately, some studies have indeed indicated that age-adjusted prevalence of dementia has been decreasing and the main hypothesis behind the change is that the lifestyle has been improved [22–24]. The FINGER trial has shown that especially when targeting lifestyle intervention simultaneously to several modifiable risk factors and to a high-risk group of older people, the cognitive capacity of older adults could be maintained. Now FINGER serves as a model to other large scale randomized controlled trials all over the world. FINGER intervention is now being replicated in the United States, Europe, Singapore, and Australia and the trials will include populations from a variety of geographical and cultural backgrounds. This worldwide effort, WW-FINGERS, supports a collaborative network of trials and experienced investigators to facilitate harmonization of research methods, and sharing of experiences and data for maximum global scientific impact. During the following years, new results from cohort and intervention studies around the world will provide additional information to improve dementia prevention models. WW-FINGERS network will show how multidomain lifestyle interventions can be replicated worldwide. This global joint effort also provides opportunity for rapid knowledge dissemination and implementation. Lifestyle matters and now it is time for global action and effective implementation.
Footnotes
ACKNOWLEDGMENTS
FINGER study is financially supported by Academy of Finland’s Responding to Public Health Challenges Research Programme (SALVE) and Academy of Finland grant 278457 (MK), Academy of Finland Key Project Funding 305810 (Muistikko), La Carita Foundation, Alzheimer Association grant (HAT-10-173121), Juho Vainio Foundation, Finnish Medical Foundation (TN), Novo Nordisk Foundation, Finnish Social Insurance Institution, Ministry of Education and Culture Research Grant (MK, JK), EVO/VTR grants of University Hospitals of Kuopio, Oulu and Turku, Seinäjoki Central hospital and Oulu City Hospital, Yrjö Jahnsson Foundation, Finnish Cultural Foundation, South Ostrobothnia Regional fund, Swedish Research Council, Alzheimer’s Research & Prevention Foundation USA, AXA Research Fund, Knut and Alice Wallenberg Foundation Sweden, Center for Innovative Medicine (CIMED) at Karolinska Institutet Sweden, Stiftelsen Stockholms sjukhem Sweden, Konung Gustaf V:s och Drottning Victorias Frimurarstiftelse Sweden, af Jochnick Foundation Sweden and The Stockholms Sjukhem foundation. We thank all members of the FINGER study group for their cooperation in data collection and management.