
Abstract
The goal of the present retrospective study was to focus on the potential influence of polypharmacy on the initiation of antidementia therapy in patients diagnosed with dementia in general practices in Germany. The current study sample included patients diagnosed with dementia in 1,217 general practices in Germany between 2014 and 2016 (index date). The primary outcome measure was the rate of prescription of anti-dementia drugs within one year following the index date. The explanatory variable was the number of different drugs prescribed at baseline per patient. Independent variables included age, sex, and type of dementia. Logistic regression analyses were conducted to study the impact of the number of different drugs prescribed at baseline per participant on the odds of receiving anti-dementia therapy (in all patients and in patients diagnosed with Alzheimer’s disease). The study included 21,888 patients with all-cause dementia. Mean age was 80.2 years (SD = 7.3 years) and 61.4% of the study population were women. Individuals receiving six drugs or more at baseline were significantly less likely to be prescribed anti-dementia treatment when compared to those without any drug at baseline (6– 9 drugs: odds ratio [OR] = 0.75;≥10 drugs: OR = 0.58). In the subgroup of patients with Alzheimer’s disease, the odds of being prescribed anti-dementia therapy were lower in individuals with four drugs or more, compared to patients who had not been prescribed any drugs at baseline (4– 5 drugs: OR = 0.60; 6– 9 drugs: OR = 0.49;≥10 drugs: OR = 0.36). There is a negative association between polypharmacy and antidementia therapy initiation in general practices in Germany.
INTRODUCTION
Dementia is a chronic condition which affects between 5% and 7% of people aged 60 years or over [1]. The number of dementia patients is expected to reach 66 million worldwide by 2030 and 115 million by 2050. In Germany, dementia is found in over one million individuals, highlighting the high prevalence of this condition in this country [2]. Since dementia is associated with poor quality of life [3] as well as psychiatric disorders (i.e., depression and anxiety) [4, 5], there is a need for better prevention, diagnosis, treatment, and management of this neurodegenerative disease.
Over the past decades, several crucial studies have shown the clinical benefits of receiving early treatment for dementia and, in particular, for Alzheimer’s disease [6, 7]. For example, in 2014, Cumbo and Ligori found, in a 12-month, randomized, open-label trial, that the prescription of several anti-dementia drugs (i.e., memantine, donepezil, rivastigmine, and galantamine) was associated with an improvement in the behavioral and psychological symptoms of Alzheimer’s disease [8]. That same year, Dysken et al. estimated, in 613 patients with mild to moderate Alzheimer’s disease, that vitamin E led to a significant reduction of the functional decline related to dementia [9]. Because of these arguments, early initiation of treatment with anti-dementia drugs is recommended in several national guidelines [10]. Nevertheless, anti-dementia drugs only have a limited effect on the long-term neurodegenerative process associated with dementia and display several side effects, such as weight loss, insomnia, and agitation [11].
Since the majority of dementia patients are 60 years or older [1], it is likely that most of them suffer from more than one chronic condition, and are therefore receiving several different drugs [12]. Thus, polypharmacy and inappropriate medication use (i.e., medications that should not be prescribed at all or should be prescribed at low dose in elderly patients) are very frequent in individuals diagnosed with dementia [13, 14]. For this reason, avoiding drug interactions that are potentially detrimental to the health of patients is an important challenge for general practitioners when prescribing anti-dementia drugs. To the best of our knowledge, there is no analysis focusing on the potential relationship between polypharmacy and the initiation of anti-dementia treatment. This is an important gap in the literature because primary care physicians may avoid prescribing these medications to elderly dementia patients who are already receiving several treatments. Therefore, the goal of this retrospective study was to examine the potential influence of polypharmacy on the initiation of anti-dementia therapy in patients diagnosed with dementia in general practices in Germany.
METHODS
Database
The present retrospective study was based on the nationwide Disease Analyzer database (IQVIA). This database contains demographic, clinical, and pharmaceutical variables anonymously obtained by IQVIA from a nationwide sample of general and specialist practices [15]. The quality of these data is assessed on a regular basis. Moreover, Becher and colleagues have shown that the Disease Analyzer database is representative of German practices [16]. Finally, several studies focusing on dementia have recently been conducted using this database [17–19].
Study population
The current study sample included patients with an initial documentation of all-cause dementia diagnosis (ICD-10 codes: F01, F03, G30) in 1,217 general practices in Germany between 2014 and 2016 (index date).
Study outcome and variables
The primary outcome measure was the rate of prescription of anti-dementia drugs (ATC: N07D incl. memantine, galantamine, donepezil, and rivastigmin) within one year after the index date. The explanatory variable was the number of different drugs prescribed at baseline per patient. Independent variables included age, sex, and type of dementia (Alzheimer’s disease [G30], vascular dementia [F01], and unspecified dementia [F03]).
Statistical analyses
Descriptive analyses were obtained for age, sex, and type of dementia. Logistic regression analyses were conducted to study the impact of the number of different drugs prescribed at baseline per participant on the odds of receiving anti-dementia therapy (in all patients and in patients diagnosed with Alzheimer’s disease). The reason why logistic regression analyses were also conducted in the subgroup of patients affected by Alzheimer’s disease is that anti-dementia drugs were initially developed and launched for the treatment of this specific type of dementia. p-values of <0.05 were considered statistically significant. Analyses were carried out using SAS 9.4.
RESULTS
The study included 21,888 patients (Table 1). Mean age was 80.2 years (SD = 7.3 years) and 61.4% of the study population were women. Figure 1 shows the 10 most frequently prescribed drug classes within the three months prior to first dementia diagnosis (agents acting on the renin-angiotensin system: 62%; beta blocking agents: 49%; and antithrombotic agents: 43%). The results of the logistic regression analysis conducted in the all-cause dementia population are displayed in Table 2. Individuals receiving six drugs or more at baseline were less likely to be prescribed anti-dementia treatment when compared to those who had not been prescribed any drugs at baseline (6– 9 drugs: odds ratio [OR] = 0.75;≥10 drugs: OR = 0.58). In addition, patients aged 90 years or over (OR = 0.53), women (OR = 0.91), and participants with vascular dementia (OR = 0.70) had a lower chance of receiving a prescription for anti-dementia drugs when compared to those younger than 80 years, men, and those with unspecified dementia, respectively. By contrast, people with Alzheimer’s disease were more likely to be prescribed anti-dementia treatments than those with unspecified dementia (OR = 3.08). Table 3 shows the results of the logistic regression analysis conducted in patients with Alzheimer’s disease. The odds of being prescribed an anti-dementia drug were lower in individuals with four or more drugs at baseline than in those without any drug at baseline (4– 5 drugs: OR = 0.60; 6– 9 drugs: OR = 0.49;≥10 drugs: OR = 0.36). Moreover, people aged 90 years or over (OR = 0.44) and women (OR = 0.95) were less likely to receive these treatments when compared to people under 80 and men, respectively.
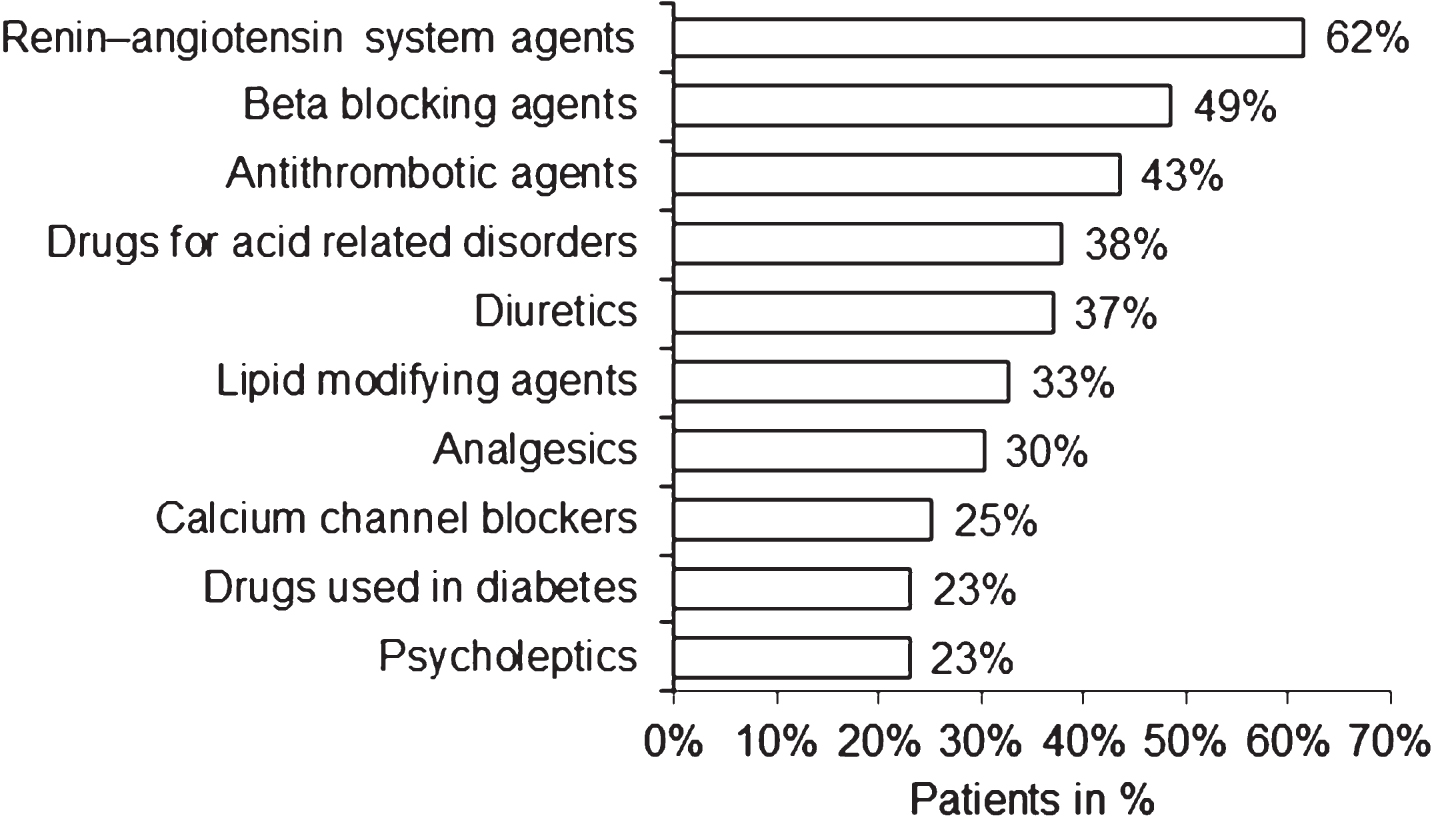
Ten most frequent drug classes prescribed within three months prior to first dementia diagnosis.
Demographic and clinical characteristics of dementia patients followed in 1,217 GP practices in Germany (2014– 2016)
Association between anti-dementia therapy initiation and pre-defined variables in all-cause dementia patients followed in 1,217 GP practices in Germany (2014– 2016) (N = 21,888)
Association between anti-dementia therapy initiation and pre-defined variables in Alzheimer’s disease patients followed in 1,217 GP practices in Germany (2014– 2016) (N = 2,144)
DISCUSSION
This is, to the best of our knowledge, the first study investigating the relationship between polypharmacy and anti-dementia therapy initiation. The study, including almost 22,000 dementia patients followed in over 1,200 general practices in Germany, showed that polypharmacy was associated with a significant decrease in the odds of initiating anti-dementia treatment. These odds were also lower in elderly patients, women, and patients with unspecified dementia than in younger participants, men, and patients with Alzheimer’s disease, respectively.
In recent years, there has been a growing interest in the relationship between dementia, polypharmacy and inappropriate medication use. Based on Beers criteria, there are several types of potentially inappropriate medication use such as medications that should be avoided in any elderly individuals, medications for which a specified dose should not be exceeded in any elderly individuals, and medications that should be avoided in certain elderly individuals displaying specific comorbidities [20, 21]. Several studies have suggested that polypharmacy might increase the risk of developing dementia [22, 23]. For example, Lai and colleagues found, in a sample of over 35,000 patients aged≥65 years, that there was a positive association between the number of drugs received and the risk of being diagnosed with dementia [22]. These findings were corroborated by Park et al., who reported in their study of more than 11,000 individuals that the risk of dementia gradually increased in proportion to the level of polypharmacy [23]. The major hypothesis in terms of the polypharmacy– dementia relationship is that the influence of polypharmacy on dementia is mediated by potentially inappropriate medication use. As a matter of fact, the use of several drugs in combination—such as anticholinergic drugs, benzodiazepines, or H2-receptor antagonists—is known to be a risk factor for cognitive decline and the development of dementia [24–27].
Other authors have focused on the prevalence of polypharmacy and potentially inappropriate medication use in dementia patients. In 2010, Lau and colleagues found, in 4,518 individuals aged≥65 years treated in Alzheimer’s Disease Centers but living at home, that the mean number of medications was higher in the group with dementia than in the group without dementia [20]. In addition, the number of medications was a risk factor for potentially inappropriate medication use in regression analyses, and the five drugs most frequently involved in this potential misuse were oral estrogens, muscle relaxants/antispasmodics, fluoxetine, short-acting nifedipine, and doxazosin. Later, in 2012, researchers from Italy reported a rate of inappropriate drug use close to 45% among 1,449 nursing home residents with severe cognitive impairment [28]. The drugs that were most frequently prescribed were lipid-lowering agents (9.9%), antiplatelet agents (9.9%), acetylcholinesterase inhibitors (7.2%), and antispasmodics (6.9%). In 2017, Clague et al. found, in a large population-based cross-sectional analysis of primary care data (N = 291,169), that comorbidity and polypharmacy were more common among participants with dementia than in those without this neurodegenerative condition (comorbidity: OR of 1.42 for≥5 physical conditions; polypharmacy: ORs of 1.46 and 2.01 for≥5 and≥10 repeat prescriptions, respectively) [29]. In addition, Balkhi and colleagues showed, in a retrospective cross-sectional study including 17,237 adults from a tertiary teaching hospital, that 46.5% of the study sample had been prescribed five medications or more, and that dementia was associated with a 5.6-fold increase in the risk of polypharmacy [30]. That same year, it was highlighted in a Danish study of 34,553 individuals with dementia that more than one out of four patients was prescribed at least two psychotropic drugs [31]. Interestingly, the most frequent combination of treatments was antidepressants and antipsychotics. Another work conducted in 448 community-dwelling primary care dementia patients from Germany reported a 22% rate of potentially inappropriate medication use in the study sample. This rate was particularly high for antidepressants, benzodiazepines, and analgesics [32].
The impact of polypharmacy and potentially inappropriate medication use in dementia has been studied by only a few authors. In 2013, Onder et al. investigated polypharmacy and mortality among older adults with advanced cognitive impairment [33]. This analysis which included 822 participants showed that almost 14% of the population were prescribed 10 drugs or more and that polypharmacy was associated with a two-fold increase in the risk of mortality towards the end of an individual’s life. Later, Mueller and colleagues focused on the impact of polypharmacy on various health outcomes in 4,668 dementia patients [34]. The authors estimated that polypharmacy was significantly associated with emergency department visits, hospitalization, unplanned hospital admission, and death within two years. Interestingly, there was also a dose-response relationship between each additional drug at baseline, on the one hand, and emergency attendance (5%), hospitalization (3%), and mortality (5%), on the other. A recent German study conducted by Wucherer and colleagues also showed an association between the total number of drugs taken, the diagnosis of mental and behavioral disorders, and the risk of drug-related problems [35]. These studies suggest that polypharmacy and potentially inappropriate medication use have a negative impact on the health of dementia patients.
The negative relationship between polypharmacy and anti-dementia treatment initiation found in the present study is likely explained by the fact that general practitioners are worried about the potential interactions between anti-dementia drugs and drugs prescribed for other conditions (i.e., hypertension, diabetes, or depression). Interestingly, a recent study including 16 general practitioners highlighted the fact that the prescribing behavior of primary care practitioners when it comes to elderly patients was determined by several important factors such as “knowledge” and “skills” [36]. Participants acknowledged the importance of an adequate knowledge of pharmacology and drug interactions and reported the need for additional training in these domains. Finally, in this retrospective study, we showed that elderly patients, women, and patients with unspecified dementia were less likely to receive anti-dementia treatment compared to younger participants, men, and patients with Alzheimer’s disease, respectively. These findings are in line with the existing scientific literature on the topic [37, 38]. Regarding age, it is important to bear in mind that treatment strategies are similar between different age groups of elderly patients [39]. Nonetheless, as pharmacokinetics and pharmacodynamics change with age and are associated with major side effects [40], general practitioners usually prefer to start with a lower dose or sometimes even delay the initiation of anti-dementia treatment in very old patients. In addition, the average number of drugs is higher and drug interactions are more frequent in women compared to men [41]. Even though our regression analyses were adjusted for both age and polypharmacy, this could explain why women received anti-dementia prescriptions less frequently than men; however, this effect was not significant in patients with Alzheimer dementia. Finally, regarding the type of dementia, most anti-dementia drugs were initially developed and launched for the treatment of Alzheimer’s disease, and thus people with Alzheimer’s disease are more likely to receive these medications than those with unspecified dementia [42].
Although the results of this retrospective study are of great interest, there are several limitations that should be mentioned at this point. First, the diagnosis of dementia relied on ICD-10 codes only, and it was therefore not possible to investigate the potential impact of the severity of dementia symptoms on the odds of initiation of the anti-dementia treatment. Moreover, when no anti-dementia drugs were prescribed, we had no information about the reasons for this therapeutic strategy. There was no data regarding the potential existence of other chronic conditions, although these disorders might have been important factors in the practitioners’ decision to initiate anti-dementia therapy. In addition, since psychiatrists and neurologists are often involved in the diagnosis of dementia in Germany, it is possible that we may have overestimated the risk of non-initiation of anti-dementia treatment in this country. Of particular importance is the fact that we did not have information about the proportion of dementia patients for whom the diagnosis was done by a general practitioner. Finally, as there are health and prescription differences between Germany and other European countries and the US, our findings may not be extrapolated to these countries. The major strengths of this work are the number of patients and the number of general practices available for analysis, and the use of real-world data from general practices where diagnoses are continuously documented, allowing for unbiased exposure assessment (no recall bias).
Overall, there was a negative association between polypharmacy and anti-dementia therapy initiation in general practices in Germany. Patients’ sex, age, and type of dementia had an additional impact on the risk of non-initiation of anti-dementia treatment. Further research is needed to gain a better understanding of the prescription patterns of general practitioners and specialists (i.e., psychiatrists and neurologists) in relation to newly diagnosed dementia patients.