
Abstract
Bilingualism is an independent component of cognitive reserve that permits to delay dementia onset up to 5 years. We describe a case of a bilingual Italian man affected by mild cognitive impairment with high cognitive reserve that, despite the presence of multiple risk factors (ApoE ɛ4/ɛ4 genotype, older age, untreated Obstructive Sleep Apnea Syndrome, AD-like biomarker alterations) did not convert to Alzheimer’s disease up to 5 years follow-up. The present case confirms the role of bilingualism as a strong protective factor for dementia, even in the occurrence of multiple risk factors.
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative disease that affects around 30 million people worldwide resulting in a relevant socio-economic burden for the society. Nowadays, a resolving therapy for this condition is lacking, and prevention is the only strategy to counteract dementia. Bilingualism is defined as the ability to communicate fluently in two languages, with regular use of both [1], and as a component of cognitive reserve (CR), it has been claimed to delay the onset of AD. The initial evidence for bilingualism as a CR component came from studies showing that lifelong bilinguals tend to develop clinical AD symptoms at an older age compared to monolinguals [2]. In healthy elderly, bilingualism may contribute to CR enhancing executive, attentive, and visual-spatial functions and has been associated with a more favorable biomarker profile [1]. On the other hand, sleep disturbances represent a risk factor for dementia and a strong relationship between sleep and cognitive decline is confirmed by recent evidence [3]. In particular, Obstructive Sleep Apnea Syndrome (OSAS) has been associated with an increased risk for all dementia subtypes [4]. Moreover, biomarker alterations in OSAS are in line with those described in AD [5, 6], supporting the hypothesis that OSAS may favor amyloid deposition leading to AD development. We describe a 77-year-old bilingual Italian man with high CR and with multiple risk factors for AD, affected by initial cognitive decline first documented in 2012, which did not meet the diagnostic criteria for dementia for over 5 years. Finally, after 6 years, the patient developed overt dementia.
MATERIALS AND METHODS
In December 2012, a 77-year-old right-handed, “late bilingual” Italian man (English as a second language) was admitted to the Neurology Unit because of initial difficulty in word-finding, especially in the English language and with a tendency to replace English words with Italian words. The patient and his wife both referred also difficulty in remembering people’s names and faces. Symptoms had started 2 years before, when he was still active as a literature professor. Despite his and his wife’s perception, he was still able to work in a satisfactory way in activities as writing, reading, and translating. There was no family history of dementia. Past medical history was significant for coronary artery disease with permanent pacemaker placement, hypercholesterolemia, and head injury. The patient underwent a neuropsychological assessment in the native language. Since a conventional head CT scan performed in 2011 was unremarkable, a [18F] FDG-PET scan was also performed in February 2013. In November 2013, the wife complained a progression in cognitive deficits, resulting in repetition of questions, misplacement of objects, difficulty in remembering appointments, reduction in sense of direction, and initial loss of interest in activities such as reading and writing. The patient referred to a memory clinic in the USA and according to available reports, a short neuropsychological assessment based on the English language was performed. Since the occurrence of daytime sleepiness, the tendency to fall asleep was investigated with the Epworth Sleepiness Scale (ESS) [7]. In May 2014, the patient again visited our memory clinic and supplemental investigations were planned: an amyloid PET, cerebrospinal fluid (CSF) analysis, and characterization of plasma apolipoprotein E (ApoE). Because of the discrepancy obtained in results between the evaluations performed in different languages (see results section), a neuropsychological assessment in the mother tongue was repeated. Moreover, since the wife referred snoring and excessive daytime sleepiness, a home-sleep apnea test was also performed. In the subsequent years, the patient continued his activities of reading, writing, and translating from English to Italian and vice versa; better performances on written tasks than on oral tasks were referred; he still performed these activities with satisfaction even though he needed more time than before to obtain the same results. In 2018, the wife referred a significant cognitive and functional impairment characterized by loss in sense of direction, inability to use a computer efficiently, loss of interests in activities such as reading and writing, and in maintaining social commitments. The connected speech was characterized by long word-finding pauses and was overall less fluent and informative, especially in the English language. The patient became dependent in medication taking and in financial management. In order to verify the progression of cognitive decline overtime, in March 2017, a [18F] FDG-PET scan was carried out together with a neuropsychological assessment, that was repeated in June 2018. In detail, four extensive neuropsychological assessments were conducted in the Italian language (in 2012, 2014, 2017, and 2018) with standard tests: Mini-Mental State Examination (MMSE) [8], Rey Auditory Verbal Learning Test [9], Story Recall Test [10], Digit Span and Spatial Span Forward and Backward [11], Trail Making Test A and B [12], Letter Fluency and Category Fluency tests [9, 13], Frontal Assessment Battery [14], Stroop Color and Word Test [15], Rey–Osterrieth Complex Figure Test [16], Activities of Daily Living Scale [17], and Instrumental Activities of Daily Leaving Scale (IADL) [18]. Language assessment was further performed with the naming subtests of an Italian battery for the assessment of semantic memory disorder (CaGi) [19] in 2012, 2014, and 2018, with the “Esame Neuropsicologico per l’Afasia” (ENPA) [20] in 2012 and 2018, with the “Screening for Aphasia in NeuroDegeneration” (SAND) test [21] in 2018 (the most important results of the language tests have been reported in Table 1). The neuropsychological assessment in the English language was performed in 2013 with some of the same and/or similar tests: MMSE, Neuropsychiatric Inventory (NPI) [22], 15 item-version of Boston naming test [23], Trail Making Test A and B [24], Luria Motor Task, Clinical Dementia Rating scale (CDR) [25]; verbal fluency was tested for animal category, long-term memory using Hopkins Verbal Learning Task [26], construction ability using Clock Drawing Test [27]. Standard cut-off values were used for both languages. Regarding imaging data, the [18F] FDG-PET scan was acquired 30 min after injection of the tracer; the amyloid PET scan was acquired 40 min after injection of [18F] Florbetapir. The PET data were analyzed by two experienced readers in a consensus reading based on visual assessment. The ApoE genotype was determined using standard procedures in the local laboratory. The CSF sample was analyzed for total-Tau, phospho-Tau, and Aβ1 - 42 by commercial enzyme-linked immunosorbent assay. Cut-off for normal values were for Aβ1 - 42 > 600 pg/ml, for total-Tau <300 pg/ml and for phospho-Tau <60 pg/ml.
Neuropsychological test results obtained in Italian language respectively in 2012, 2014, 2017, and 2018: raw values were shown in brackets, data corrected for age and education out of brackets. N.A., not applicable; err, number of errors
RESULTS
In December 2012, a neuropsychological assessment revealed an impairment in verbal short-term memory, difficulty in single-word retrieval in spontaneous speech, especially at the onset of conversation, without other language deficits. A reduction in the inhibitory control on motor stimulus was also detectable. MMSE total score was 30/30 and there was no functional impairment (Table 1). The clinical picture was compatible with “non-amnestic MCI”. The CT scan revealed a mild frontal atrophy with hippocampal sparing; white matter changes were also detectable (Fig. 1a). The [18F] FDG-PET performed in February 2013 showed preserved brain metabolism (Fig. 1b). In November 2013, the neuropsychological assessment carried out in the English language revealed a deficit in long-term memory and naming tests, in executive functions and construction; long-term memory performances improved with a cued recall. The CDR total score was 0.5, the NPI score was 5 for anxiety, apathy, irritability, appetite changes, and sleep fragmentation. The ESS score was 10, over the cut-off of normality. Overall the picture was indicative of mild cognitive impairment (MCI) of unclear etiology, with AD as a possible diagnosis and OSAS as a possible comorbid condition that could promote cognitive decline. Donepezil was then started. Given the discrepancy in memory and naming tests obtained performing evaluations in the two different languages, another neuropsychological assessment in the mother tongue was repeated. The discrepancy was confirmed (Table 2): in the native language, long-term memory performances were well preserved and the naming ability was within the normal range, whereas a slight impairment in executive functions was detectable in both languages. With regards to CSF biomarkers, Aβ1 - 42 was low (348 pg/ml), while total-Tau and phospho-Tau were within the normal range (222 pg/ml and 41 pg/ml). The value of total-Tau/Aβ1 - 42 ratio (0.64) was compatible with AD [28]. The genetic study revealed the presence of ApoE ɛ4/ɛ4 genotype, a condition strongly associated with the AD risk [29]. Significant amyloid tracer retention was found at Amyloid PET (Fig. 1c). A home sleep apnea test revealed an apnea/hypopnea index of 41.4, indicative of severe OSAS; despite this, the patient refused treatment with Continuous Positive Airway Pressure ventilation. In 2017, the result of the neuropsychological assessment was substantially stable compared to that obtained in 2014 (Table 1), whereas the [18F] FDG-PET scan showed a slight worsening of the metabolic activity in posterior cingulate and left parieto-temporal cortices (Fig. 1d). Hence, after 5 years follow-up, a diagnosis of “non-amnestic MCI in patient affected by severe untreated OSAS” was confirmed. Eventually, in 2018, according to the cognitive and functional worsening referred by the wife, the neuropsychological assessment revealed a progressive decline in executive functions and attention, whereas the long-term memory was still preserved. Regarding native language abilities, the connected speech was characterized by longer word-finding pauses, several anomias, semantic “conduites d’approches”; the patient was not more able to replace the Italian missing word with the corresponding English one. Naming skills progressively declined especially for the category “living things”, both for visual stimuli and in response to oral descriptions. A progressive decline was also evident in the verbal fluency tests total scores (from 2012 to 2018 a loss of 7 and 4 scores, respectively, in the Phonemic and in the Semantic tests). Taking into account individual items of these tests, pathological results in fluency were documentable for the letter “A” and for the category “objects”. Results of the SAND battery revealed a selective deficit in words comprehension for the category “living things” (Table 1). An initial dependence in IADL and a urinary urgency with occasional incontinence were also detectable; however, an expert urologist attributed the last symptom to a side effect of Donepezil.
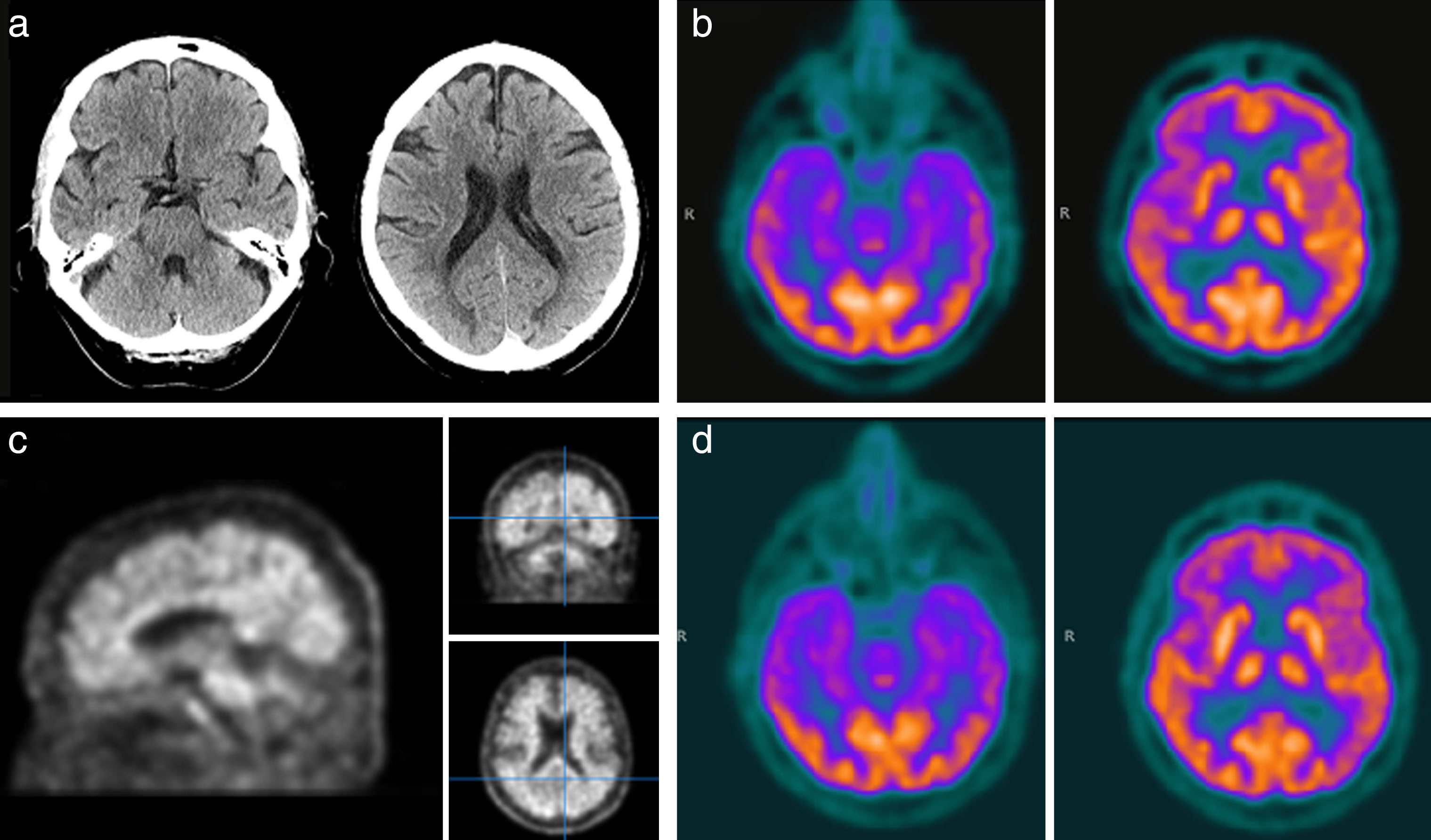
Imaging performed over time: a) CT scan in 2011 showed slight frontal atrophy with hippocampal sparing, vascular encephalopathy; b) [18F] FDG-PET in February 2013 showed substantially preserved brain metabolism; c) amyloid-PET in May 2014 revealed the presence of high amyloid burden; d) [18F] FDG-PET in March 2017 showed slight hypometabolism in posterior cingulate and left parieto-temporal cortices.
Neuropsychological test results obtained in English language (November 2013) and in Italian language (May 2014): raw values were shown in brackets, data corrected for age and education out of brackets. Results’ interpretation in the last column. N.A., not applicable; err, number of errors
DISCUSSION
We described a case of a bilingual literature professor affected by MCI with a high CR and at high risk for AD conversion. Symptoms started in 2010 and despite the presence of major risk factors for AD conversion (ApoE ɛ4/ɛ4 genotype, older age, untreated OSAS, AD-like biomarker profile), the progression of cognitive decline was very low up to 2017. Starting from 2014, biomarkers suggested a neurodegenerative AD-like process as the cause of MCI, but repeated neuropsychological assessments did not show progression to dementia until 2018. Our findings confirm that bilingualism is associated with a delay in the AD onset up to 5 years [2, 30]. This phenomenon may be explained by the “brain plasticity bilingualism”, which allows greater resistance to cognitive decline and permits the delay of clinical symptoms of AD. In this regard, the “neural compensation” and the “neural reserve” are the two underlying mechanisms probably involved in the protective effect of bilingualism; indeed, both mechanisms seems to be induced by the cognitive load enhanced by bilingualism. Structural and functional neuroimaging studies into bilingualism confirm the neuroplastic effect of bilingualism on the brain and reveal that neuroplastic changes mainly take place in those structures related to executive control, language learning, and processing [31, 32]. At the time of symptoms onset, when the neuropsychological assessment was performed in the native language, the cognitive profile resulted preserved. Instead, in the English language, an emerging cognitive deficit was detectable. The discrepancy in results obtained in the two languages was evident, especially in the long-term memory and naming tests (Table 2), suggesting an initial impairment in English language abilities. Latency in single-word retrieval, detectable in spontaneous speech mostly at the onset of conversation, reflected probably the competition between the two languages. This represents an initial deficit in the executive functions, as confirmed by test results in both languages. Naming abilities were impaired more in the second language indeed, in case of “non-balanced bilingual” speaker, producing words in the “non-dominant language” requires greater executive control to overcome competition of the “dominant language” [33]. A deficit in executive functions together with frontal lobe atrophy [34] and other biomarker alterations outlined a profile also compatible with OSAS [5, 6]. Since the diagnosis of OSAS was confirmed by home-sleep apnea test result, our findings support the hypothesis that OSAS may precede and favor the AD onset. Eventually the patient developed dementia characterized by deficits in spatial orientation, attention, executive functions, and an initial impairment in semantic memory with a reduction in verbal fluency, whereas long-term memory was spared. In conclusion, for 5 years the present case was compatible with a diagnosis of “non-amnestic MCI with high CR and multiple risk factors for AD conversion”. For a long time, the bilingualism-dependent CR protected the patient from dementia development even in the presence of multiple risk factors. Beyond the bilingualism depletion, the patient developed an atypical form of AD. Our results suggest the importance of supporting bilingual education and preserving the second language among the elderly in order to delay dementia onset.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0736r1).