
Abstract
Cognitive control for the coordination of mental operations is essential in normal cognitive functioning of daily life. Although the decline of cognitive control in older adults with mild cognitive impairment (MCI) has been demonstrated, whether this decline is a core deficit in MCI remains unclear. In this study, we employed a perceptual decision-making task to estimate the capacity of cognitive control (CCC) in older adults with MCI (n = 55) and the age-, sex-, and education-matched healthy controls (HC, n = 55) selected based on a commonly used battery of ten neuropsychological tests in five cognitive domains. We found that the CCC was significantly correlated to the neuropsychological measures of the battery. The mean CCC was significantly lower in the MCI group (3.06 bps) than in the HC group (3.59 bps) and significantly lower in the amnestic MCI subgroup (2.90 bps) than in the nonamnestic MCI subgroup (3.22 bps). In detecting and classifying MCI using machine learning, the classifier with the CCC as the input feature outperformed the overall classification with neuropsychological measures in a single cognitive domain. The classification performance was significantly increased when the CCC was included as a feature in addition to measures in a single domain, and the CCC served as a key feature in optimal classifiers with inputs from multiple domains. These results support the hypothesis that the decline in cognitive control is a core deficit in MCI and suggest that the CCC may serve as a key index in the diagnosis of MCI.
INTRODUCTION
Mild cognitive impairment (MCI), an intermediate state between cognitive decline in normal aging and very early dementia or Alzheimer’s disease (AD), is a neurodegenerative disorder [1–3]. MCI is common in older populations and its prevalence increases with age [4]. The concept of MCI has evolved over time [2, 5]. In the early days, clinicians and researchers focused on memory declines [2, 6]. However, memory impairment is not necessarily a condition of MCI. Rather, individuals with MCI may show disorders in the single domain of memory (amnestic MCI), in any other single cognitive domain (nonamnestic MCI), or in multiple cognitive domains simultaneously [1–3]. However, it is still not well understood whether individuals with MCI have a core deficit that is associated with the cognitive decline in MCI.
Cognitive control refers to flexible allocation of mental resources to allow for important information to be processed according to current goals [7–11]. It is involved in all higher-level cognitive processes such as attention [11, 12], perception [13, 14], working memory [15–17], episodic memory [18–20], language [21, 22], thinking [23, 24], and decision making [13, 26]. Thus, cognitive control is conceptualized as a more abstract and higher-order construct for the coordination of information processing in goal-directed decision-making [8, 12], though with a limited capacity [11, 28]. Therefore, a deficit in cognitive control should impact other related cognitive processes. It has been shown that executive functioning, which is supported by cognitive control, declines with age [29–32] and the progression of neurodegenerative disorders [33–37]. A meta-analysis has demonstrated that the variance of daily functional abilities is mostly explained by functions related to cognitive control, such as executive functions (37%), attention (33%), and working memory (31%), while memory measures account for a comparatively lesser part (23%) of variance of functional outcomes [38]. The deficits in cognitive control are more severe in executive functions including processing speed, processing flexibility, inhibitory control, and working memory in amnestic MCIs compared to nonamnestic MCIs [39–42]. In most previous studies on cognitive control in MCI, the Stroop task [33, 43–45], the flanker task [37], the go/no-go task [36, 46], the attentional network test (ANT) [47], the Simon task [34, 49], and the trail making test (TMT) [35, 51] were used. These tasks share a common ground in that they elicit conflict processing, which is a special case with an increase in information uncertainty [8]. However, the impairment of cognitive control in MCI has not been examined in terms of capacity in previous studies.
The capacity of cognitive control (CCC) can be estimated under an information theory account of cognitive control, which argues that cognitive control is to coordinate mental operations under uncertainty, such as the effect elicited in conflict tasks [8]. According to information theory, the capacity of a channel is the maximum information transmission rate (in bits per second, bps) that can be achieved, i.e., the amount of information that can be processed within a unit of time with arbitrarily low error rate. If the rate of information inputs exceeds the capacity, the accuracy of information transmission will drop because of information loss. The CCC can be estimated based on the relationship between cognitive load (measured as information rate in bps) and response accuracy as demonstrated in recent studies [13, 52]. The backward masking majority function task (MFT-M, see Methods and Materials for details) is designed for the estimation, in which cognitive load is parametrically manipulated by varying both information amount and processing time, with the response accuracy as the outcome measure. Information rate in this task varies in a wide range (0 to about 20 bps), by which cognitive control can be challenged. The CCC of an individual can be estimated as the point of information rate at which response accuracy starts to drop. For healthy young adults, the CCC is about 3 to 4 bps [13, 53].
The application of the CCC measure in the study of MCI would enable us not only to quantitatively measure the decline in cognitive control in this population but also to examine the relationship between the CCC decline and the deficits in other cognitive domains. In this study, we used the MFT-M to estimate the CCC in older adults with MCI and the demographically matched (by age, sex, and years of education) healthy controls (HC) and tested the associations between the CCC and other cognitive domains of episodic memory, executive function, attention, language, and visuospatial ability. In addition, we employed support vector machines (SVMs) to examine the classification power of the CCC for MCI compared to the definitive cognitive measures of neuropsychological tests. It was predicted that older adult participants with MCI would show reduced CCC compared to the HC participants, and that there would be a more severe reduction in the CCC in amnestic than in nonamnestic MCI participants. The CCC would be correlated with the performance on the Mini-Mental State Examination (MMSE) and other neuropsychological tests. Importantly, if there were a core deficit of the CCC in MCI, the CCC would be a key feature in detecting and classifying MCI in machine learning.
METHODS AND MATERIALS
Participants
Older adult participants (50 years old and above, n = 310) were recruited from communities in Shenzhen city, China. Demographic information of the participants was collected using a questionnaire designed for this study. A Chinese version of the MMSE [54] and a combined version of the Physical Self-Maintenance Scale and the Instrumental Activities of Daily Living Scale [55] were administered. Participants with an MMSE score lower than 24, or impaired activities of daily living (ADLs), or instrumental activities of daily living (IADLs) were excluded from further testing in order to avoid the potential confounding of dementia or impaired ADLs/IADLs.
To identify individuals with MCI, ten neuropsychological tests were used for the following five cognitive domains: episodic memory, tested with the Auditory Verbal Learning Test (AVLT) [56] and the Rey-Osterrieth Complex Figure Recall Test (ROCFT Recall) [57]; executive function, tested with the Trail Making Test Part B (TMT-B) [58] and the Stroop Test (ST) [59]; attention, tested with the Trail Making Test Part A (TMT-A) [58] and the Symbol Digit Modalities Test (SDMT) [60]; language, tested with the Category Verbal Fluency Test (CVFT) [61] and the Boston Naming Test (BNT) [62]; and visuospatial ability, tested with the Rey-Osterrieth Complex Figure Copy Test (ROCFT Copy) [57] and the Clock Drawing Test (CDT) [63]. Dysfunction in a domain was defined if a participant’s scores on two or more measures in that domain were lower than the cut-off (1.5 SD lower than the grand mean of the norm [64]). According to Petersen’s criteria of MCI [65], an individual was identified as having MCI if this individual showed dysfunction in any of these five domains.
There were 78 (25%) MCI individuals identified among 310 participants. From these participants, 55 individuals with MCI (29 females and 26 males, mean age = 67.8 years, age range: 57.0–81.0 years, years of education = 8.9 years) and 55 individuals (who were not identified as having MCI) for the matched HC group (32 females and 23 males, mean age = 66.9 years, age range: 55.6–76.1 years, years of education = 9.7 years) were then tested using the MFT-M. There was no significant difference found in age, sex, and years of education between the MCI group and the HC group (p > 0.05) (Table 1). According to the performance on the memory tests (i.e., the AVLT and the ROCFT Recall), the MCI group was further divided into two subgroups: the amnestic MCI group (n = 27, mean age = 68.7 years, years of education = 8.9 years, 15 females) and the nonamnestic MCI group (n = 28, mean age = 67.0 years, years of education = 9.0 years, 14 females). There was no significant difference between the amnestic and nonamnestic MCI groups found in age, sex, and years of education (p > 0.05).
All participants were right-handed based on their statements and had normal or corrected-to-normal visual acuity. The protocol was approved by the Institutional Review Board (IRB) of Shenzhen University. Written informed consent was obtained from each participant.
Demographic data and performance on the neuropsychological tests in the MCI and the HC groups
Data are shown as mean (SD). MCI, mild cognitive impairment; HC, healthy control. a z value.
The backward masking majority function task
The MFT-M, developed in a previous study [13], was used to estimate the CCC of each participant. In the current study, the materials of the MFT-M were identical to the previous study [53]. In this task, a set of five arrows pointing either left or right was displayed on the screen (top-right panel of Fig. 1) followed by a set of diamond shapes as the mask consisted of eight solid diamond shapes presented at the same eight positions at which the arrows could appear. There were two variables manipulated: the congruency of the arrow set (5:0, 4:1, or 3:2) and the exposure time (ET) of the arrow set (0.25, 0.5, 1, or 2 s). The majority was defined as the direction of the majority arrows (e.g., if there were three arrows pointing to the left and two arrows pointing to the right, the majority is left). The length of the arrow and the diameter of each diamond shape were 0.7° of the visual angle. The radius from the fixation cross to the center of an arrow subtended approximately 2.3° of the visual angle.
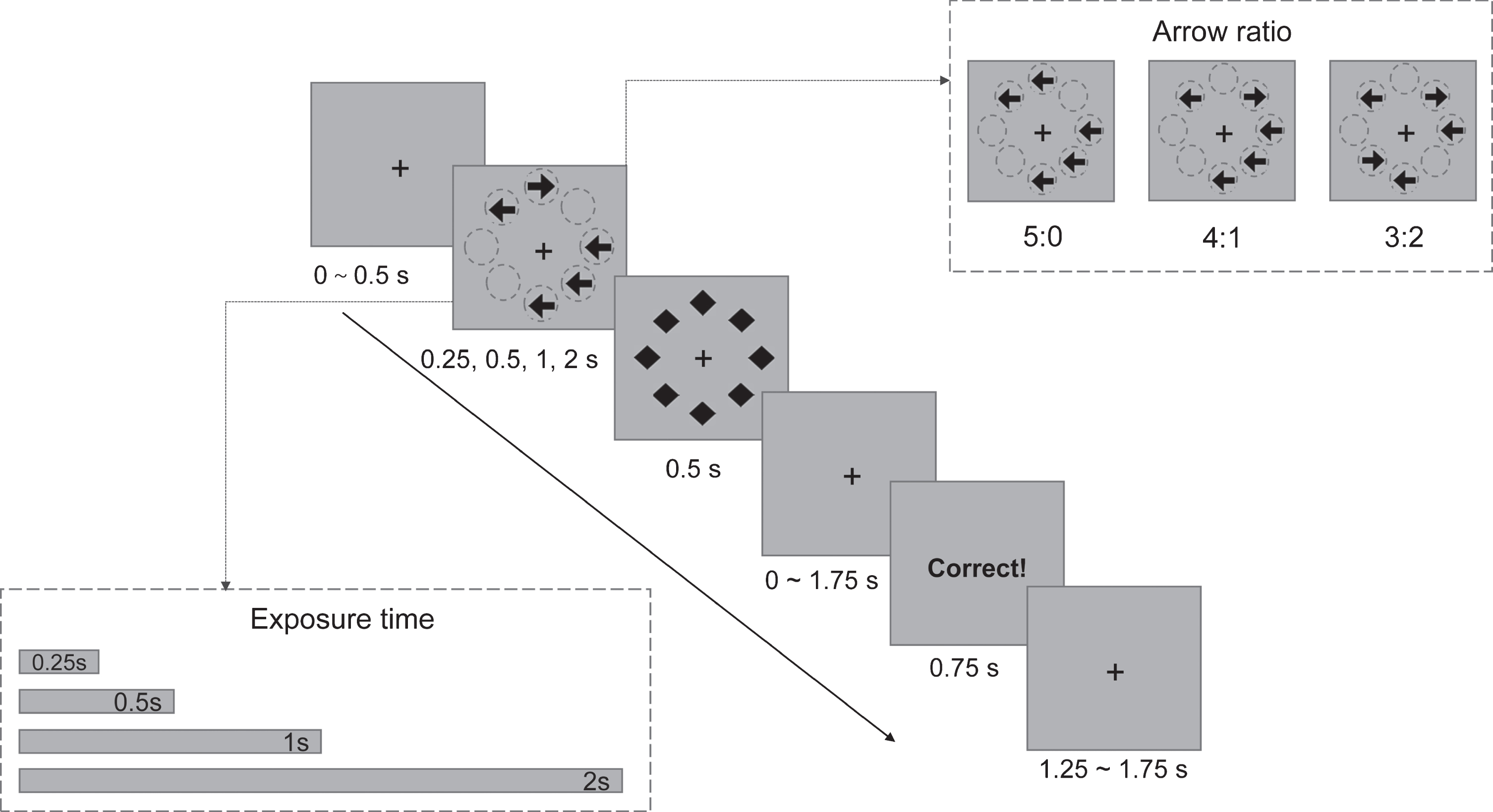
Schematic of the backward masking majority function task (MFT-M). Arrow ratio and exposure time manipulated in the MFT-M are shown in the top-right and bottom-left rectangles with dashed borders, respectively. A schematic description of a trial (4:1 condition) in the MFT-M is shown in the trial layout. Participants were instructed to indicate the majority direction of the arrows (left or right) within a 2.5 s response window.
At the beginning of each trial, there was a variable fixation period of 0 to 0.5 s. After this fixation period, an arrow set was presented with a variable ET followed by a mask for 0.5 s. After the offset of the mask, there was a variable poststimulus fixation period of 0 to 1.75 s to make the total duration of the arrow set, mask, and poststimulus fixation together 2.5 s. Figure 1 illustrates the stimuli and the sequence of the events in a trial. Participants were instructed to respond as accurately and quickly as possible to indicate the direction of the majority by pressing a button (left or right). Responses had to be made within 2.5 s from the onset of the target. Participants were instructed to guess when they failed to find the majority direction and to respond in all trials. Feedback was then presented for 0.75 s to inform participants whether their response in the current trial was correct. At the end of each trial, there was a variable postfeedback fixation period of 1.25 to 1.75 s to make the total duration of each trial 5 s.
The task consisted of 12 blocks with 36 trials in each block. The ET was varied between blocks but not trial-by-trial. Blocks were presented in a random order. Trials within each block were also presented in a random order. Within each block, the number of trials in each congruency condition was identical (with an equal number of majority directions of left and right): 12 trials under 3:2, 12 trials under 4:1, and 12 trials under 5:0 conditions. The task consisted of 432 trials in total and lasted approximately 45 minutes.
The task was run on a PC using E-Prime software (Psychology Software Tools, Pittsburgh, PA). The experimenter first explained the task to the participants verbally. Once an understanding of the task was demonstrated, the participants performed a practice session before performing the actual test. The practice session consisted of 4 blocks with 18 trials in each block.
Data analysis
For the performance on the neuropsychological tests, independent samples t-tests (one-tailed) were performed with the prediction of better performance in HCs than in MCIs. In addition, the potential difference between the amnestic and the nonamnestic MCI subgroups was examined with independent samples t-tests (two-tailed).
For the MFT-M, means and standard deviations (SD) of accuracy and reaction time (RT) for each condition were calculated. Trials with no response within the response window were treated as invalid trials and were excluded from the RT analysis. Trials with RT exceeding±3 SD of the mean RT in each condition were considered as outliers and were removed from further analysis of the RT. The mean and SD of RT under each condition were then recalculated based on the remaining trials for each participant. Accuracy for each condition was computed as the percentage of trials with correct responses. Two separate 2 (Group: MCI versus HC)×3 (Ratio: 5:0, 4:1, 3:2)×4 (ET: 0.25, 0.5, 1, 2 s) repeated measures analysis of variance (ANOVA) tests were performed for accuracy and RT, with Group as a between-subject factor, ET and Ratio as within-subject factors. Greenhouse-Geisser correction was used for nonsphericity, and Bonferroni correction was used to correct for multiple comparison.
The CCC of each participant was estimated using the algorithm developed in a previous study [13]. One-tailed t-tests were performed to test whether the CCC of the MCI group was significantly lower than that of the HC group and whether the CCC of the amnestic MCI group was significantly lower than that of the nonamnestic MCI group. Correlation analyses were performed to test the associations between the CCC and neuropsychological measures in the MCI and HC groups separately, with the predictions that the CCC would be positively correlated with the performance in terms of test scores in the neuropsychological tests and negatively correlated with the performance in terms of completion time.
We applied SVMs to test the CCC’s power in the classification of MCI versus HC and amnestic versus nonamnestic MCI, in contrast to and in combination with other neuropsychological measures. Machine learning algorithms learned from the sample data (e.g., learned participants’ class labels of “MCI” or “HC” by using their CCC and neuropsychological test scores as the input features) and built a classifier that distinguishes between two classes. An SVM could be a line in a two-dimensional space (Fig. 2), a plane in a three-dimensional space, and a “hyperplane” in higher dimensional space. An optimal SVM should have a high classification accuracy, a large margin (the distance defined by classifier between two classes), and a small amount of support vectors (data points “supporting” the decision surface, such as dots surrounded by squares in Fig. 2).
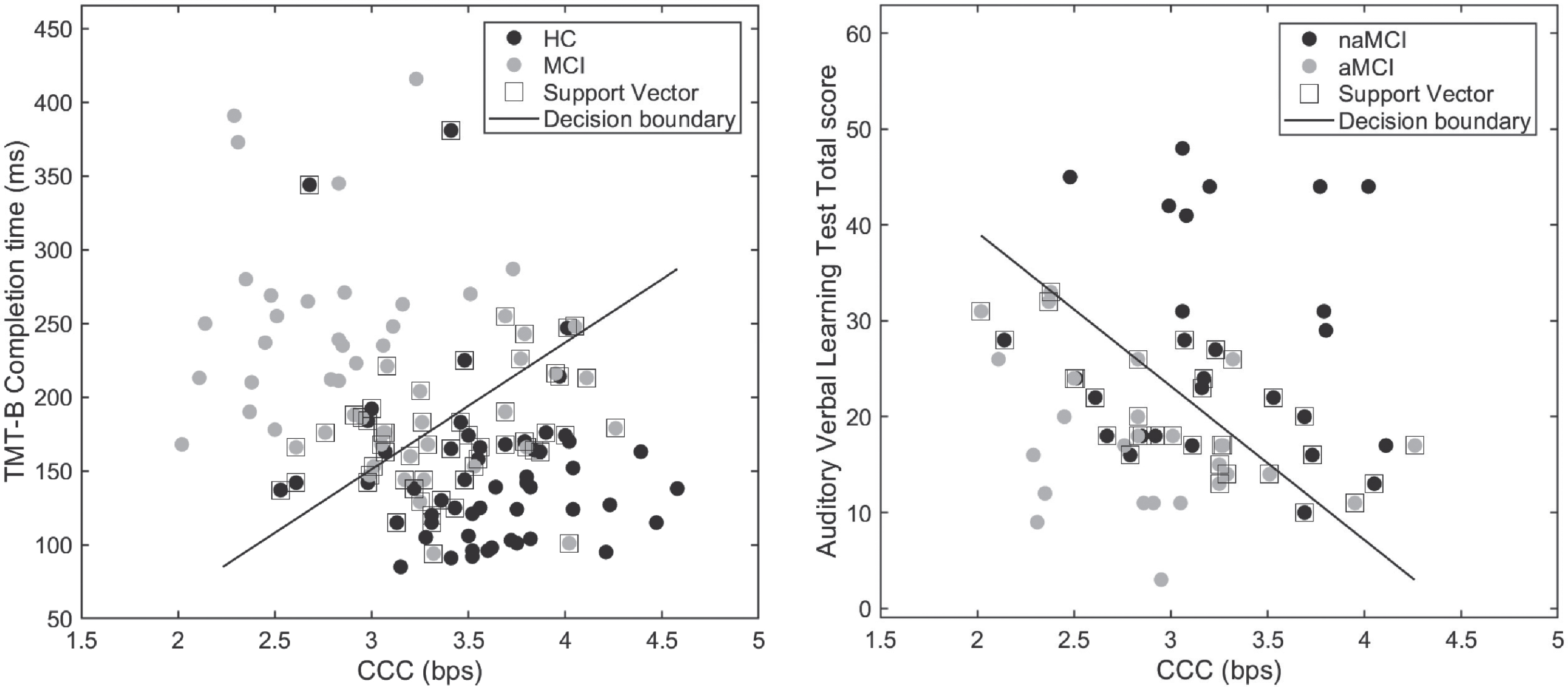
Scatter plots illustrating two optimal bivariate SVMs with the CCC as one of the two input features in the classification of MCIs versus HCs (left panel) and of amnestic MCIs (aMCI) versus nonamnestic MCIs (naMCI) (right panel).
We first trained six classifiers, using the CCC and the neuropsychological measures in each of the five cognitive domains (i.e., episodic memory, executive function, attention, language, and visuospatial ability) as the input features respectively, to classify participants with and without MCI (MCIs versus HCs) and to differentiate between amnestic MCIs and nonamnestic MCIs. If the classifier with the CCC as an input feature showed classification performance comparable to or higher than the classifiers with the criterion neuropsychological measures as the input features, it would suggest that the CCC catched the core deficits reflected by these neuropsychological tests defining MCI. Second, we investigated whether including the CCC as an input feature in addition to neuropsychological measures in a single cognitive domain would result in an increase in classification utility. If the classification performance of the classifiers with the input features in a single domain could be improved by including the CCC as an additional input feature, it would suggest that the CCC measured unique variances/components beyond each domain itself. Thirdly, we trained and selected the optimal multivariate SVMs with two to thirteen input features respectively. The candidate input features included the CCC, MMSE, and the measures of the five domains. If the CCC performed a role in most of these optimal classifiers, it would suggest that the CCC serves as a key feature that detects a critical deficit in MCI.
The protocol of machine learning in this study included training, validation (including cross-validation and independent sample testing), and significance testing. For the training of classifiers, we linearly scaled all input features to the range of [0, 1] and trained SVMs using the fitcsvm function in the Statistics and Machine Learning Toolbox in MATLAB version 2014b (MathWorks, Natick, MA). We chose the SVM algorithm of sequential minimal optimization (SMO) and linear kernels (kernel scale was set to 1). The box constraint, a trade-off parameter that adjusts the balance between maximizing classification margin and minimizing separation error in building decision surface, was set to 100 [66].
In the MCI versus HC classification, we randomly selected 70% of MCIs and HCs respectively to build a training set (i.e., 39 MCIs and 39 HCs) on which we trained and cross-validated classifiers. The remaining 30% of participants’ data (i.e., 16 MCIs and 16 HCs) were used for independent validation. In the amnestic MCI versus nonamnestic MCI classification, however, because the sample size was small (27 amnestic MCIs and 28 nonamnestic MCIs), we validated the classification utility of classifiers using 5-fold cross-validation. We performed 5-fold cross-validation (100 times) to estimate each classifier’s accuracy (Ncorrect assessments / Nsamples), sensitivity (Ntrue positive assessments / Npositive samples), and specificity (Ntrue negative assessments / Nnegative samples). In each cross-validation, the sample was randomly split into five subsets, with one subset as a test set and the remaining four subsets combined as a training set. A classifier was built based on the training set and was evaluated using the test set. This procedure was repeated for 5 times and each subset served as the test set once. The folds at each iteration were same for all the classifiers in the comparisons of classification utility. In addition to the measures of accuracy, sensitivity, and specificity, we also reported the classification edge and the number of support vectors of SVMs. Classification edge, the weighted mean of margins, represents the distance defined by SVM between binary classes. The amount of support vectors is in a trade-off relationship with edge.
We performed nonparametric permutation tests to examine whether a classifier had an accuracy, sensitivity, or specificity significantly higher than chance level. For example, a permutation-based null distribution of accuracy of each classifier was created by breaking up the mapping of class labels (MCI versus HC; amnestic versus nonamnestic MCI) and cognitive features (1000 times). The p-value of the “real” accuracy of each trained classifier was obtained by locating the “real” accuracy in the sampled permutation null distribution. The null hypothesis that class labels and features are independent and that the classifier has not learned patterns was rejected if the p-value was less than 0.05.
In order to examine whether the classifier with the CCC as the only input feature performed better than other classifiers including neuropsychological measures in single cognitive domains as input features in classifications, we conducted one-way repeated measures ANOVAs (Greenhouse-Geisser correction was used for nonsphericity) and follow-up multiple comparisons between the features of the CCC and those in other cognitive domains. We also examined whether the classification utility of the CCC was significantly better than the average performance of the neuropsychological features in single cognitive domains by using paired t-tests.
To test whether classifiers with neuropsychological measures in a single domain and the CCC as input features would have higher classification performance than their counterparts without the feature of the CCC, we performed repeated measures multivariate analysis of variance (MANOVA) tests. The test statistic of Pillai’s trace was reported and Bonferroni correction was applied for follow-up multiple comparisons.
RESULTS
Performance on the neuropsychological tests
The MCI group showed significantly poorer performance on all the neuropsychological tests compared to the HC group (Table 1). The amnestic MCI group showed poorer performance on AVLT (Delayed recall: p < 0.001; Total score: p < 0.01) and ROCFT Recall (p < 0.05) compared to the nonamnestic MCI group. There was no other significant difference between the two MCI subgroups found.
Performance on the MFT-M
There were 0.8% trials as invalid responses or outliers excluded. For accuracy, the main effect of Group was significant, F(1,108) = 24.08, p < 0.001,

The performance of the MCI and HC groups across conditions on the MFT-M and the results of CCC estimation. Mean accuracy (A) and reaction time (RT) (B) as a function of Group, Ratio, and ET. Error bars in panel A and B represent standard errors. Mean CCC of the MCI and the HC groups (C) and mean CCC in amnestic MCI (a-MCI) and nonamnestic MCI (na-MCI) groups (D). Error bars in panel C and D represent 95% confidence intervals. *p < 0.05; ***p < 0.001
For RT, the main effect of Group was not significant, F(1,108) = 0.20, p = 0.65. There were significant main effects of Ratio, F(2,216) = 858.87, p < 0.001,
The mean CCC of each group
The difference in the CCC between the MCI and HC groups was significant with a large effect size, t(108) = –5.55, p < 0.001, Cohen’s d = 1.11 (Fig. 3C). The CCC was significantly lower in the MCI group (M = 3.06 bps, SD = 0.55 bps, 95% CI: 2.94∼3.18 bps) than in the HC group (M = 3.59 bps, SD = 0.43 bps, 95% CI: 3.45∼3.73 bps). The difference in the CCC between the amnestic and nonamnestic MCI groups was also significant with a medium effect size, t(53) = –2.30, p = 0.013, Cohen’s d = 0.62. The CCC was significantly lower in the amnestic MCI subgroup (M = 2.90 bps, SD = 0.54 bps, 95% CI: 2.70~3.10 bps) than in the nonamnestic MCI subgroup (M = 3.22 bps, SD = 0.52 bps, 95% CI: 3.02∼3.42 bps) (Fig. 3D). These results indicate that there was the deficit of cognitive control in terms of CCC in MCIs, and that this deficit was even worse in amnestic MCIs.
The relationship between the CCC and neuropsychological measures
The CCC was significantly correlated with the MMSE scores in the HC group (r = 0.26, p = 0.03) and it was significantly correlated with the MMSE scores in the MCI group (r = 0.29, p = 0.02). For measures in the domain of executive function, the CCC was significantly correlated with the completion time on the Stroop test in the HC group (r = –0.27, p = 0.02). In the MCI group, the CCC was significantly correlated with the completion time (r = –0.24, p = 0.04) and the number of correct responses (r = 0.38, p = 0.003) on the Stroop test and with the completion time on the TMT-B (r = –0.31, p = 0.01). In the attention domain, the CCC was significantly correlated with the performance on the TMT-A in the HC group (r = –0.29, p = 0.02). In the language domain, the CCC was significantly correlated with the scores on the CVFT in the MCI group (r = 0.27, p = 0.02). In the domain of visuospatial ability, the CCC was significantly correlated with the scores on the ROCFT Copy test in the MCI group (r = 0.29, p = 0.02). In the memory domain, the CCC was marginally correlated with the scores on the ROCFT Recall test in the HCs (r = 0.22, p = 0.054). The correlations between the CCC and the scores on the rest neuropsychological tests (including AVLT, CDT, BNT, and SDMT) were not significant (p > 0.05). Details of the correlations between these cognitive measures in the MCI and HC groups can be found in Supplementary Tables 1 and 2. These results suggest that the CCC is associated with all cognitive domains except the memory domain.
Classification of MCI
For the comparisons of classification utility between the CCC and the measures of the other cognitive domains, the main effect of Feature on accuracy was significant for the MCI versus HC classification, F(5,495) = 221.85, p < 0.001,
The performance of SVMs with different input features in cross-validation in the classification of MCI versus HC
CCC, capacity of cognitive control. Values in parentheses are standard deviations. N represents sample size. The superscript ns indicates statistical non-significance in permutation tests that examined whether the performance of each classifier was higher than chance level (p > 0.05).
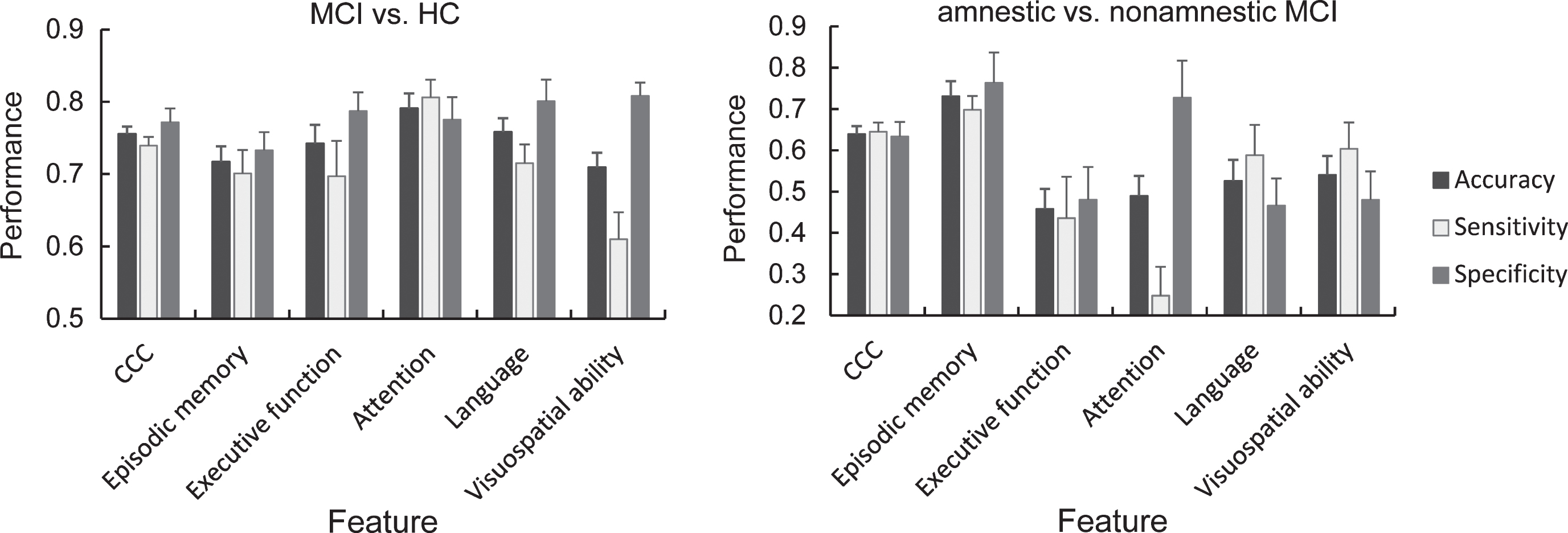
The accuracy, sensitivity, and specificity of SVMs with input features of the CCC and neuropsychological measures in single cognitive domains in the classification of MCI versus HC (left panel) and amnestic versus nonamnestic MCI (right panel). Error bars represent standard deviations.
The performance of SVMs with different input features in cross-validation in the classification of amnestic versus nonamnestic MCI
CCC, capacity of cognitive control. Values in parentheses are standard deviations. N represents sample size. The superscript asterisks represent statistical significance in permutation tests that examined whether the performance of each classifier was higher than chance level: *p < 0.05; **p < 0.01; ***p < 0.001.
There was a significant main effect of Feature on sensitivity for the MCI versus HC classification, F(5,495) = 399.21, p < 0.001,
There was a significant main effect of Feature on specificity for the MCI versus HC classification, F(5,495) = 110.91, p < 0.001,
With respect to whether including the CCC as an input feature in addition to neuropsychological measures in a single cognitive domain would increase classification utility, there was a significant increase in accuracy in the MCI versus HC classification if the CCC was included, V = 0.84, F(5,95) = 101.25, p < 0.001,
There was a significant main effect of inclusion of the CCC on sensitivity in the MCI versus HC classification, V = 0.86, F(5,95) = 117.29, p < 0.001,
There was a significant effect of inclusion of the CCC on specificity for the MCI versus HC classification, V = 0.93, F(5,95) = 245.11, p < 0.001,
The CCC was included in ten out of twelve optimal classifiers in the MCI versus HC classification (Table 4) and was included in eleven out of twelve optimal classifiers in the amnestic versus nonamnestic MCI classification (Table 5). All these optimal SVMs performed significantly higher than chance level on accuracy, sensitivity, and specificity.
The performance of optimal SVMs in cross-validation in the classification of MCI versus HC
Refer to Table 1 for the meanings of the numbers in the Feature column. N represents sample size. Values in parentheses are standard deviations. All the accuracy, sensitivity, and specificity are significantly higher than chance level.
The performance of optimal SVMs in cross-validation in the classification of amnestic versus nonamnestic MCI
Refer to Table 1 for the meanings of the numbers in the Feature column. N represents sample size. Values in parentheses are standard deviations. All the accuracy, sensitivity, and specificity except the one with a superscript ns are significantly higher than chance level.
The classification performance of SVMs with the input features of the CCC, the neuropsychological measures in a single domain, and the assemblage of the two on the independent sample is presented in Table 6. Table 7 presents the performance of the twelve optimal SVMs with two to thirteen input features in the independent sample tests.
The performance of SVMs with different input features in independent sample tests in the classification of MCI versus HC
CCC, capacity of cognitive control.
The performance of the optimal SVMs in independent sample tests in the classification of MCI versus HC
Refer to Table 1 for the meanings of the numbers in the Feature column.
DISCUSSION
Our results indicate that deficits in cognitive functions in older adults with MCI are related to the decline in cognitive control. In this study, the MCI participants showed poorer performance on the MFT-M compared to the HC participants, which is in line with the results of previous studies using the Stroop task [33, 43–45], the flanker task [37, 67], the ANT [47], the go/no-go task [68–70], and the stop-signal task [71], suggesting that MCI is associated with general deficits in information processing under conditions of uncertainty [8]. Significant lower CCC in the MCI group compared to the HC group further demonstrates that the decline in cognitive control is also associated with the capacity reduction in the cognitive control process. In addition, the CCC was significantly lower in amnestic MCIs compared to nonamnestic MCIs, suggesting that amnestic MCI is associated with a greater deficit in cognitive control compared to nonamnestic MCI.
We found that the CCC was associated with the MMSE score, indicating a relationship between the CCC and intellectual ability [53, 73]. The CCC was correlated to the performance on the Stroop test and TMT-B in the domain of executive function. Participants in these two tests were required to perform the task as accurately and quickly as possible. Thus, the two tasks involve processing speed that is the nature of the CCC. Therefore, the correlations between the CCC and the measures on the Stroop test and the TMT-B support the information theory account of cognitive control [8, 13]. The CCC was also associated with the TMT-A in the attention domain, the ROCFT Copy in the visuospatial domain, and the CVFT in the language domain, which were likely due to the cognitive control involved in these tests [57, 75]. In addition, many of the significant correlations were shown in MCIs rather than HCs, which suggests the deficits in cognitive functioning in MCIs is associated with the decline in CCC.
The CCC may serve as a core feature in both differentiating MCIs from HCs and classifying amnestic and nonamnestic MCIs. The CCC showed better classification performance than the average performance of neuropsychological measures in single cognitive domains. Keep in mind that the classifiers with the neuropsychological measures as input features have the circular inference issue because these features (variables), instead of the CCC, were used as the variables that operationally defined MCI and that the group differences between MCI and HC in these variables were statistically significant. The CCC showed comparably high classification performance as those classifiers with input features in single cognitive domains suggests that the deficit in cognitive control is a key feature of MCI. In the classification of amnestic versus nonamnestic MCIs, in addition to the classifier including the features in the memory domain, only the CCC classifier had valid classification utility (i.e., accuracy and sensitivity higher than chance level, see Table 3), suggesting more server deficits in cognitive control in amnestic MCIs compared to nonamnestic MCIs again.
In addition, the inclusion of the CCC as an additional feature improved the performance of classifiers with neuropsychological features in single cognitive domains, suggesting that the CCC might measure unique variances/components beyond the five domains that was used in the assessment of MCI in this study. The CCC served as an input feature in most of the optimal classifiers, suggesting that the CCC detected a critical deficit in MCI. Thus, measuring the CCC in MCI may help in the diagnosis of this neuropsychological disorder. However, because the decline in cognitive control has been found in major mental disorders, the CCC may not be used to differentiate different mental disorders.
The measures of TMT-A and SDMT in the attention domain showed higher classification performance than the CCC, indicating a decline in processing speed in elderly with MCI. In addition, measures in the language domain had comparable classification power as that of the CCC. Previous studies indicate that BNT and CVFT measure cognitive control in addition to verbal fluency [74, 76]. It might also be possible that the high performance of the measures in these two domains is because they served as key variables in the identification of MCI during the recruitment phase.
The reduced CCC in MCI may be linked to deficits in the frontoparietal network and associated white matter tracts. The frontoparietal network serves as the entity of cognitive control of information processing uncertainty reduction, with the anterior cingulate cortex (ACC) as a key brain structure [8]. Previous studies have shown deficits in the frontoparietal network, especially the frontal areas and the ACC [47, 77–80] in MCI and AD patients. Disruption of the white matter of the frontoparietal network is associated with cognitive decline [81–84]. In addition, the reduced CCC may be a sign of the impairment of attentional networks involved in the implementation of cognitive control and comprises the functions of alerting, orienting, executive control, and their interactions [12, 85–88]. Previous studies have also indicated the selective impairment of attentional network in individuals with amnestic MCI. Specifically, the amnestic MCI participants showed preserved alerting and orienting function but impaired functions associated with executive control, which was accompanied with a decreased connectivity of the dorsal frontoparietal network and a reduced gray matter volume and diminished activation of the ACC [47, 90].
This study may have potential clinical implications. The CCC may be used as an additional variable in the diagnosis of MCI. The results of machine learning indicate the competitive power of the CCC in detecting MCI. The possible use of the CCC in early diagnosis of MCI or AD is also suggested by previous findings that the impaired executive functions can be present at the very early stage of AD accompanied with memory failure and precede the onset of language and visuospatial deficits [91–93]. Although the MFT-M may not be the best instrument detecting MCI in clinical settings, the evidence of significantly reduced CCC in individuals with MCI and the classification power of the CCC as a key feature support the hypothesis that the deficit in cognitive control is a core feature of MCI.
Footnotes
ACKNOWLEDGMENTS
Research reported in this publication was supported by the National Natural Science Foundation of China (NSFC) grant (31571129) to Q.G., National Key Research and Development Project of China (2018YFC1315202), the Shenzhen Peacock Plan (KQTD2015033016104926), and the Guangdong Pearl River Talents Plan Innovative and Entrepreneurial Team grant (2016ZT06S220). The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.