
Abstract
Background:
Although a growing body of evidence shows an important role of apolipoproteins in the pathogenesis of Alzheimer’s disease (AD), the association of apolipoprotein C-III (APOC-III) with cognitive decline is not clear.
Objective:
To examine whether higher cerebrospinal fluid (CSF) and plasma APOC-III levels were associated with better cognitive performance over time in the early stage of AD.
Methods:
Baseline CSF and plasma APOC-III levels were analyzed in relation to cross-sectionally and longitudinally cognitive performance over a 12-year period. Data were extracted from the Alzheimer’s Disease Neuroimaging Initiative database, and 234 subjects (89 subjects with normal cognition (NC) and 145 subjects with mild cognitive impairment (MCI)) with CSF APOC-III measurements and 454 subjects (58 subjects with NC and 396 subjects with MCI) with plasma APOC-III measurements were included.
Results:
In the cross-sectional study, we did not find a significant relationship between CSF APOC-III and cognitive performance in pooled individuals with MCI and NC. However, longitudinal analysis found that higher baseline CSF APOC-III was significantly associated with slower cognitive decline over a 12-year period in individuals with MCI, but not the healthy controls, after controlling for several covariates and Alzheimer biomarkers. Plasma APOC-III levels showed a mild correlation with CSF APOC-III levels, but were not associated with longitudinal cognitive changes in the pooled sample or in diagnosis-stratified analyses.
Conclusions:
Higher CSF APOC-III levels are significantly associated with slower cognitive decline over a 12-year period among individuals with MCI.
INTRODUCTION
Apolipoproteins are a group of proteins associated with lipid and cholesterol metabolism [1, 2], and emerging findings have implicated apolipoproteins as important players in neurogenerative processes [3–8]. In particular, apolipoprotein C-III (APOC-III) is a component of triglyceride-rich lipoproteins involved in lipids, glucose metabolism, and possibly cognition [9–11]. Some evidence suggested that APOC-III can bind circulating amyloid-β (Aβ), and levels of APOC-III in plasma were reduced in patients with Alzheimer’s disease (AD) [10, 12]. Further, it has been reported that higher plasma APOC-III levels are associated with better cognitive performance in cross-sectional analyses [10, 11]. However, no studies have reported longitudinal cognitive associations with plasma or cerebrospinal fluid (CSF) levels of APOC-III in subjects with mild cognitive impairment (MCI) and normal cognition (NC).
Thus, we aimed to address this gap by evaluating the association of plasma and CSF APOC-III with cognitive decline in individuals with MCI and NC. In the cross-sectional study, baseline plasma and CSF AOPC-III levels were analyzed in relation to baseline demographic variables, cognitive performance and AD pathologies (CSF Aβ42, t-tau, p-tau levels) in individuals with MCI and NC. In the longitudinal study, baseline plasma and CSF APOC-III levels were used as predictors for change in cognition over a 12-year period.
MATERIALS AND METHODS
Alzheimer’s Disease Neuroimaging Initiative study
Data used in the preparation of this article were downloaded on 13 June 2018 from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu). The ADNI was launched in 2003 with the primary goal of identifying neuropsychological, clinical, biochemical, and neuroimaging markers of potential progression of MCI to early AD dementia. Each ADNI site obtained local institutional review board approval, and written informed consents were obtained from all the subjects.
Participants
From the dataset, we selected participants between 55 and 90 years old who met the following criteria for MCI and NC and had baseline APOC-III samples and follow-up measurements of cognitive function. 234 subjects had CSF APOC-III measurements at baseline (Table 1). 454 subjects had plasma APOC-III measurements at baseline (Supplementary Table 1).
Demographic information of study sample
NC, normal controls; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; ADAS-Cog 11, Alzheimer’s disease assessment scale-cognitive 11-item; RAVLT, Rey auditory verbal learning test; APOC-III, apolipoprotein C-III; Aβ42, amyloid 42; t-tau, total tau; p-tau, phosphorylated tau.
Subjects with NC had a Mini-Mental State Examination (MMSE) [13] score ranging between 24 and 30, and a Clinical Dementia Rating (CDR) [14] score of 0. The criteria for MCI included an MMSE between 24 and 30, a CDR of 0.5, objective memory deficits based on delayed recall scores of the Wechsler Memory Scale Logical memory II, preserved activities of daily living, and an absence of dementia.
CSF analysis
CSF Aβ42, t-tau, and p-tau levels were determined using the multiplex xMAP Luminex platform (Luminex Corp., Austin, TX, USA) and Innogenetics INNO-BIA AlzBio3 (Innogenetics, Ghent, Belgium) immunoassay reagents as described previously [15].
CSF APOC-III was measured as part of a CSF multiple proteomic processing stream using an xMAP multiplex panel (MyriadRBM) [16], details of which can be found at the ADNI website (http://adni.loni.ucla.edu/). Test-retest validation was conducted in the 16 randomly selected CSF samples to ensure reliability. Values are given in μg/ml. The data were natural log transformed to better approximate a normal distribution.
Plasma APOC-III measurements
Plasma APOC-III was measured as part of a plasma multiple proteomic processing stream using an xMAP multiplex panel (MyriadRBM), details of which have been described previously [17] and can be found at the ADNI website (http://adni.loni.ucla.edu/). Values are given in μg/ml. Plasma APOC-III levels were log-transformed for statistical analyses.
White matter hyperintensities (WMH) measurements
WMH volumes were estimated from T1-, T2-, and proton density (PD)- weighted MR images using an automated technique, details of which has been described previously [18, 19]. The data used in the present study were obtained from the ADNI file “UCD_ADNI1_WMH.CSV”.
Cognitive outcomes
Subjects underwent clinical and cognitive measurements at each ADNI visit. In the present study, the cognitive outcomes included the following: 1) MMSE and 2) ADAS-Cog 11. The data used in this analysis were extracted from the ADNI files “MMSE.csv” and “ADAS_ADNI1.CSV”.
Statistical analysis
First, t-tests and chi-square tests were conducted to assess differences in demographic and clinical variables between controls and MCI patients. Second, Spearman correlations were performed to examine the cross-sectional associations between APOC-III and other variables in the pooled sample. Third, to examine the associations of baseline CSF APOC-III levels (dichotomized by –1.24μg/ml, high APOC-III group is defined as≥–1.24μg/ml while low APOC-III group < –1.24μg/ml) and plasma APOC-III levels (dichotomized by 2.13μg/ml, high APOC-III group is defined as≥2.13μg/ml while low APOC-III group < 2.13μg/ml) with cognitive decline, linear mixed models were fitted for each cognitive outcome (MMSE and ADAS-Cog 11). To evaluate whether cognitive status had a modification effect, these analyses were performed within each diagnostic group separately. All models included main effects of baseline age, gender, education, APOE4 genotype, Rey auditory verbal learning test (RAVLT) immediate recall scores [20], Aβ42, t-tau, p-tau, cholesterol, triglyceride, WMH, and their interactions with time, as well as random effects consisting of a random intercept and a random slope for each subject. All analyses were performed with R software (version 3.3.3) [21]. The level of statistical significance was set at p < 0.05.
RESULTS
Demographic information
A total of 234 participants were included in this analysis (Table 1). There were no significant differences in age or educational attainment between controls and MCI patients. Compared with controls, MCI patients were more likely to be APOE4 carriers, male and had lower MMSE scores, lower RAVLT immediate recall scores, greater ADAS-Cog 11 scores, and higher levels of CSF t-tau, p-tau but lower levels of Aβ42. However, no significant difference was found in CSF APOC-III between the two groups.
As shown in Supplementary Table 1, a total of 454 subjects with plasma APOC-III samples were included in the present study.
Association of APOC-III levels with demographic and clinical variables in cross-sectional study
As shown in Table 2, CSF APOC-III was associated with age in the pooled sample (rho = 0.143, p = 0.029). However, no correlations between CSF APOC-III and other variables were found (all p > 0.05). In addition, CSF APOC-III was not associated with gender or APOE4 genotype (all p > 0.05).
Correlation between CSF APOC-III and demographic and clinical variables in the pooled sample
MMSE, Mini-Mental State Examination; ADAS-Cog 11, Alzheimer’s disease assessment scale-cognitive 11-item; RAVLT, Rey auditory verbal learning test; Aβ42, amyloid 42; t-tau, total tau; p-tau, phosphorylated tau; WMH, white matter hyperintensities.
As shown in Supplementary Table 2, plasma APOC-III was positively associated with serum total cholesterol and triglyceride levels in the pooled sample (all p < 0.001). Compared with men, women had higher levels of plasma APOC-III (2.19±0.15 versus 2.11±0.15, p < 0.001). However, no correlations between plasma APOC-III and other variables were observed (all p > 0.05).
Correlations between CSF and plasma APOC III levels in the MCI and NC groups
CSF and plasma APOC-III levels showed a mild correlation (r = 0.17, p = 0.021) in the correlation analysis that included 191 individuals (45 subjects with NC and 146 subjects with MCI) who had the CSF and plasma samples. In diagnosis-stratified analyses, there was a significant association between CSF and plasma APOC-III levels in the NC group (r = 0.332, p = 0.026). However, in the MCI group, plasma APOC-III was not associated with CSF APOC-III (r = 0.11, p = 0.196; Fig. 1).
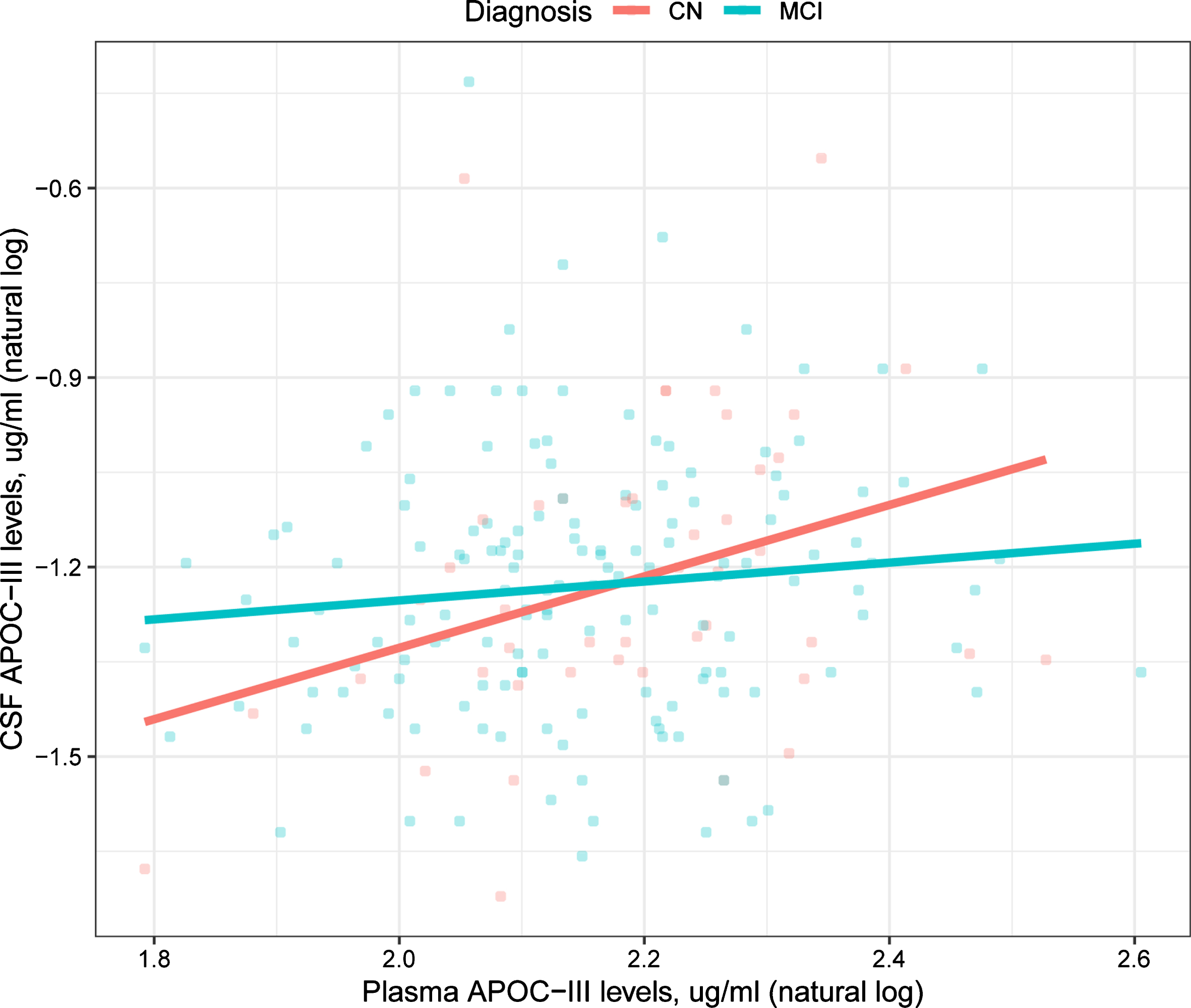
Correlations between CSF and plasma APOC III levels in the MCI and NC groups.
Association of APOC-III levels with conversion from MCI to dementia
We examined whether CSF and plasma APOC-III levels predicted conversion from MCI to dementia. Cox proportional hazard models were conducted for APOC-III as a dichotomous variable (CSF APOC-III was dichotomized by –1.24μg/ml; Plasma APOC-III was dichotomized by 2.13μg/ml) when controlling for age and gender. CSF and plasma APOC-III were not associated with conversion from MCI to dementia (low CSF APOC-III: HR = 1.4, p = 0.11, Fig. 2; low plasma APOC-III: HR = –0.26, p = 0.07, Supplementary Figure 1).
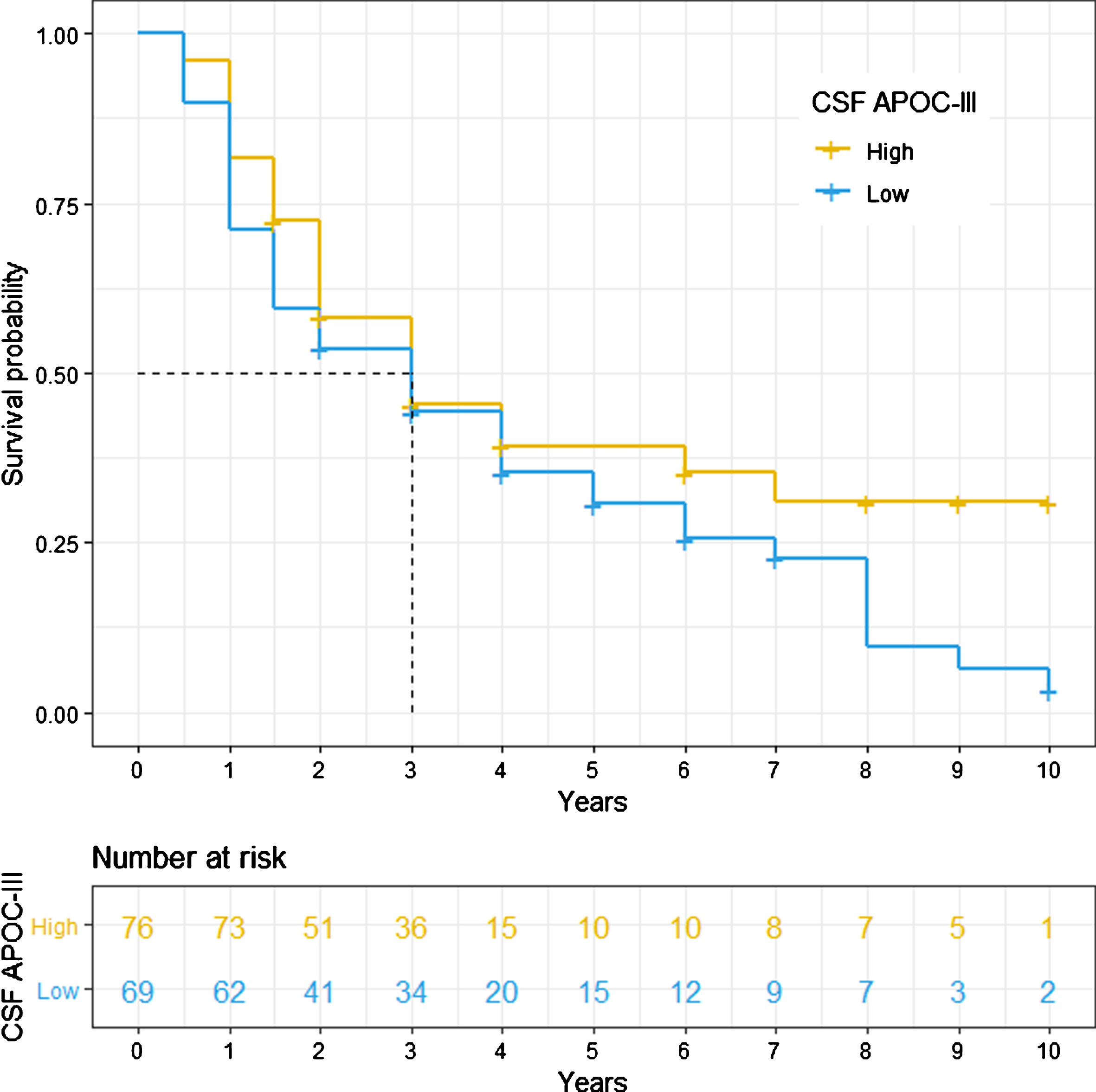
Conversion from MCI to dementia for CSF APOC-III.
Association of APOC-III levels with cognitive decline over a 12-year period
Findings from the linear mixed models of cognitive change over time by CSF APOC-III levels (dichotomized by –1.24μg/ml: low CSF APOC-III was defined as CSF APOC-III levels < –1.24μg/ml; high CSF APOC-III was defined as CSF APOC-III levels≥–1.24μg/ml) are demonstrated in Table 3 and Fig. 3.
Summary of linear mixed models
NC, normal controls; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; ADAS-Cog 11, Alzheimer’s disease assessment scale-cognitive 11-item; RAVLT, Rey auditory verbal learning test; APOC-III, apolipoprotein C-III; Aβ42, amyloid 42; t-tau, total tau; p-tau, phosphorylated tau; WMH, white matter hyperintensities. Main effects of independent parameters are included in each linear mixed model (estimates not shown). Estimates are unstandardized values, indicating the amount of change in each cognitive outcome per year.
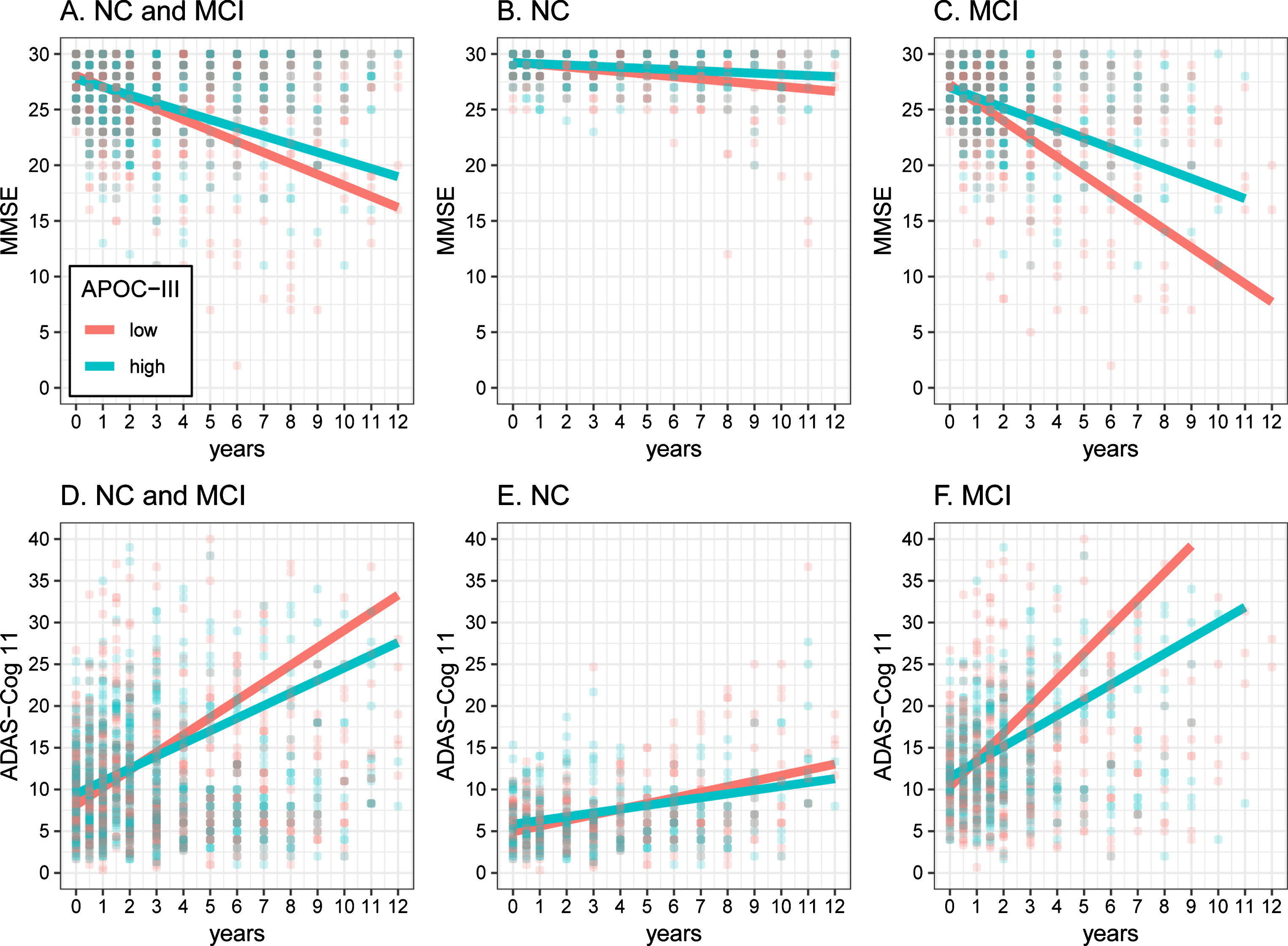
Association of CSF APOC-III levels with cognitive decline over a 12-year period. NC, normal controls; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; ADAS-Cog 11, Alzheimer’s disease assessment scale-cognitive 11-item.
In the pooled sample, there were marginally significant associations of CSF APOC-III with rates of change of MMSE (Estimate = 0.2124, p = 0.0731) and ADAS-Cog 11 (Estimate = –0.4372, p = 0.0605) during follow-up after accounting for age, sex, education, APOE4 genotype, RAVLT immediate recall, Aβ42, t-tau, p-tau, total cholesterol, triglyceride, and WMH (Table 3 and Fig. 3A, D).
In diagnosis-stratified analyses, high CSF APOC-III was associated with slower rates of decline on the ADAS-Cog 11 in the MCI group (Estimate = –0.8831, p = 0.0275, Table 3 and Fig. 3F), but not the control group (Estimate = –0.1441, p = 0.2902, Table 3 and Fig. 3E). Further, there was a marginally significant association of high CSF APOC-III with slower rates of decline on the MMSE in the MCI group (Estimate = 0.3935, p = 0.0562, Table 3 and Fig. 3C), but not the control group (Estimate = 0.0849, p = 0.1824, Table 3 and Fig. 3B).
However, as shown in Supplementary Table 3 and Fig. 2, there was no association between plasma APOC-III and cognitive decline in the pooled sample or in diagnosis-stratified analyses (all p > 0.05).
DISCUSSION
In the present study, cross-sectional analysis did not find a significant relationship between CSF APOC-III and cognitive performance in pooled individuals with NC and MCI. However, longitudinal analysis showed that higher baseline CSF APOC-III was significantly associated with slower cognitive decline over a 12-year period in individuals with MCI, but not the healthy controls, after controlling for several covariates and Alzheimer biomarkers.
Regarding the biology of APOC-III, it is primarily synthesized in the liver and intestine [22]. APOC-III is found on VLDL, LDL, HDL, and chylomicrons [22]. It has been reported that APOC-III is involved in lipids and glucose metabolism [9, 23]. In AD patients and cognitively normal individuals with AD family history, a significant reduction in APOC-III levels was observed in the blood [10]. Despite some evidence that APOC-III levels in the blood are cross-sectionally associated with cognitive performance [10, 11], our understanding of the relationship of plasma and CSF APOC-III levels and cognitive decline over time is limited. In the present study, our data showed that higher levels of APOC-III in CSF, but not plasma, were associated with slower cognitive decline in subjects with MCI. This protective effect of APOC-III on cognitive performance may be due to the fact that APOC-III, an Aβ-binding protein, could increase Aβ efflux and indirectly decrease the deposition of Aβ in brain [10]. However, the lack of association between plasma APOC-III levels and cognitive decline may be due to the presence of the blood-brain barrier, the more complicated origin and metabolism of plasma biomarkers. Interestingly, we found that plasma APOC-III levels were associated with CSF APOC-III levels in the NC group, but not the MCI group (Fig. 1). Based on our results, the lack of correlation between the levels of APOC-III in each of these compartments in the MCI group suggested that the disruption of plasma and CSF APOC-III equilibrium in the early stages of AD may contribute to the reduction of Aβ efflux. However, further basic and clinical studies are needed to support this notion. In addition, a previous genetic study suggested that the APOC-III 3017G allele may be associated with reduced risk of AD among APOE4 noncarriers in a Chinese cohort [24]. However, the precise mechanisms underlying the relationship between APOC-III and cognitive performance warrant further investigation.
However, in our study, associations of high CSF APOC-III and better cognitive performance were observed only in the longitudinal analysis, not the cross-sectional analysis. These findings may have several possible explanations. One possibility is that the severity of cognitive deficits of our participants may be relatively subtle at baseline. In other words, the neuropsychological assessments utilized in our study may be too insensitive to find a relationship between APOC-III and global cognitive function in a cross-sectional analysis. Another possibility is that the comparable levels of APOC-III between the NC and the MCI groups may also limit the power to detect the link between APOC-III and cognitive performance in a cross-sectional analysis.
In the present study, the association of CSF APOC-III with cognitive function in individuals with MCI remained statistically significant when CSF Aβ42 and tau proteins were controlled in the longitudinal analysis, indicating that CSF APOC-III is an independent predictor of cognitive decline, and that the cognitive changes associated with CSF APOC-III levels may go beyond the effects of Aβ amyloid plaques and tau neurofibrillary tangles. Although Aβ and tau have been two major therapeutic targets for AD [25], additional mechanisms may also take part in AD pathogenesis. Based on our findings, CSF APOC-III may have a beneficial effect on the cognition in individuals with MCI. However, the mechanisms underlying this potentially protective effect of APOC-III on cognition warrants further investigation.
Finally, in this study, we revealed that CSF APOC-III is associated with MMSE and ADAS-Cog 11 scores over time only in MCI patients. It is suggested that increased levels of APOC-III in CSF are particularly related to slower cognitive decline in the early stage of AD. However, in the NC group, no significant relationships between APOC-III and cognitive decline were observed. Thus, APOC-III may serve as a potentially useful target for cognitive decline, especially in the early stage of AD.
Several limitations should be noted. First, the convenience samples recruited in the present study may limit the ability to generalize our findings to other populations. Thus, our data should be interpreted with caution due to sample selection bias. Second, we investigated the association of APOC-III only with global cognition (MMSE and ADAS-Cog 11). It would be intriguing to explore a more comprehensive neuropsychological domains, including memory and executive function.
In conclusion, we found that increased CSF APOC-III levels were associated with slower cognitive decline in individuals with MCI. Further basic and clinical studies are needed to clarify the mechanisms underlying the relationship between APOC-III and cognition.
Footnotes
ACKNOWLEDGMENTS
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.