
Abstract
Background:
Gait impairments are emerging predictors of dementia. However, few studies have examined whether gait predicts decline in specific cognitive domains.
Objective:
This study aimed to determine whether gait speed or other gait characteristics were associated with decline in specific cognitive domains and the role of the ApoE4 genotype in modifying these associations.
Methods:
Participants (n = 410; mean age 72.0±7.0 years) were randomly selected from the electoral roll. At baseline, gait speed was assessed using the GAITRite walkway. Gait variability in step time, step length, step width, and double support time (DST) was calculated as the standard deviation of each measure across all steps. In a subsample (n = 177), speed was measured under fast pace. The difference between usual and fast pace was calculated. At baseline, 2.6 and 4.6 years processing speed, memory, executive and visuospatial function were measured using neuropsychological tests. Multivariable mixed models were used to examine 1) associations between gait and the different cognitive domains over time and 2) whether the presence of ApoE4 genotype modified these associations.
Results:
Higher DST variability was associated with greater decline in memory (p for interaction 0.03). Slow gait speed predicted decline in processing speed (p = 0.02) and visuospatial function (p = 0.03). In ApoE4 carriers, gait speed also predicted decline in memory (p = 0.02). Other gait characteristics did not predict decline in any of the cognitive domains (p > 0.05).
Conclusions:
These findings add to the evidence that gait is an early indicator of cognitive decline, but that specific gait measures may provide diagnostic insights into specific cognitive domains.
Keywords
INTRODUCTION
Dementia is one of the largest global health concerns for older people [1]. Early identification of people at risk might provide a potential avenue to combatting the early accumulation of pathology and prevent or delay disease onset. Although much progress has been made, there is still an unmet need due to a lack of simple and inexpensive biomarkers to detect early cognitive deficits, but impairments in gait are emerging as a potential simple solution [2].
Results from longitudinal studies have shown that slower gait speed predicts both incident cognitive impairment or dementia [3–7]. However, more recently other gait characteristics such as gait variability and walking speed reserve (WSR) have emerged as early, and potentially more sensitive markers of dementia [8]. For example, greater gait variability (the magnitude of the fluctuation in a gait parameter from one step to the next), under both single and dual-task has been shown to be associated with dementia onset, whereas gait speed was not [7, 9].
Few studies have examined whether gait variability is associated with decline in specific cognitive functions. Such information may provide clinical biomarkers to augment prediction of dementia from an earlier stage. In cross-sectional studies greater variability in step time [10] and stride time [11–13] were associated with poorer executive function [10, 13], processing speed [11], and episodic memory [13], whereas greater variability in double support phase was associated with poorer executive function, processing speed, and visuospatial ability [10]. There has only been one longitudinal study to our knowledge examining this topic. A variability factor, composed of variability in stride length and swing time was not associated with decline in global cognition or the domains of executive function, attention, and memory [7]. However, gait variability may not behave as one construct [14, 15]. For example, gait variability in distinct gait characteristics are correlated with different cognitive, medical, and sensorimotor factors [15, 16]. Therefore, examining variability as one factor might be problematic if gait characteristics show differing sensitivity to cognitive decline. Hence, examining individual gait variability measures may help in finding the most sensitive markers of cognitive decline.
Greater WSR (the extent gait speed can be increased from usual pace) has also been identified in a cross-sectional study of older people from a memory clinic as a marker of worsening cognitive stage [8]. Increasing walking speed to maximal levels may demand additional cognitive input [17], and hence WSR has the potential to be an early marker of cognitive decline that has not yet been investigated.
Therefore, this study aimed to determine, in a population-based sample, whether baseline gait speed and other gait characteristics (temporal and spatial gait variability and WSR) were associated with cognitive decline in specific cognitive domains (executive function, processing speed, memory and visuospatial function). As a secondary aim we examined whether the presence of ApoE4 genotype, a genetic marker of Alzheimer’s disease, modified any association between poorer baseline gait and decline in cognitive domains.
METHODS
Participants
The Tasmanian Study of Cognition and Gait (TASCOG) is a longitudinal study of the neural correlates of gait and cognition. In January 2005, the initial cohort (baseline) was randomly selected from the Southern Tasmanian Electoral roll with ethical clearance obtained from the Southern Tasmanian Health and Medical Human Research Ethics committee. Written consent was obtained from all participants. Participants were included if they were aged 60 to 85 years and were able to walk without a gait aid. They were excluded if they had a history of dementia or Parkinson’s disease, lived in an institution or if there was any contraindication to MRI as this was part of the larger study. Follow-up assessments were conducted in March 2008 (Phase 1) and March 2010 (Phase 2) using identical methods.
Gait assessment
Assessment of gait was carried out at preferred walking speed using the 4.6 m GAITRite walkway (GAITRite system, CIR Systems, PA, USA). Each walk started 2 m before and finished 2 m after the walkway, to allow for acceleration and deceleration. Each participant completed 6 walks. The GAITRite software provides an output for gait speed for each walk as well as individual foot-fall information for a range of gait parameters. Intra-individual variability was calculated as the standard deviation of each gait measure. Variability in step time, double support time (DST), step length, and step width were chosen as they have been cross-sectionally associated with poorer cognitive function, particularly poorer executive function and processing speed [10, 13]. In a subsample of participants recruited consecutively (n = 177), gait speed was measured at fast pace and WSR was calculated as the difference in gait speed between preferred and fast pace walking (WSR = [fast gait speed – preferred gait speed]).
Cognitive function
Cognitive function in four specific domains were assessed with a comprehensive neuropsychological test battery at baseline and each follow up phase. a) Executive function: the Controlled Word Association Test (COWAT, using the letters F, A, and S), the Victoria Stroop test (Stroop color time - Stroop word time), the Digit Span subset of the Wechsler Adult Intelligence Scale-III; b) Processing speed: the Symbol Search and Digit Symbol Coding subsets of the Wechsler Adult Intelligence Scale-III, c) Visuospatial function: the Rey Complex Figure copy task and d) Memory: the Hopkins Verbal Learning Test—Revised and a 20 min delayed reproduction of the Rey Complex Figure copy task. For each participant, raw scores from the individual cognitive tests at each phase were standardized against the sample mean scores of the respective tests at baseline. Then principal component analysis was applied to the baseline data to derive one summary variable for each of the four domains, and the same derived components were applied at each follow-up phase, so that change could be measured.
Covariates
Demographics
Baseline age, sex, and education were obtained via a self-reported questionnaire. For the purposes of analyses, education was stratified into a binary variable using high school equivalent and below as the cut-off.
Medical history
The following variables were also considered as baseline covariates. 1) Body mass index (BMI): calculated using the height (m) and weight (kg) at baseline. 2) Cardiovascular disease and risk factors (CVD): The presence or absence of any of the following conditions were determined by a questionnaire: hypertension, hypercholesterolemia, ischemic heart disease, diabetes mellitus, and stroke. Based on the number of risk factors present at baseline, a CVD score was created. 3) Mood: assessed with Geriatric Depression Scale (short version) and a score of >5 was used to classify participants into either depressed or not. 4) ApoE4 genotype: derived from whole blood DNA and participants were considered APOE4 positive if they carried at least one copy of APOE4 allele.
Data analysis
Associations between baseline gait and cognitive decline
Longitudinal mixed effect models were used to determine whether baseline gait (gait variability, WSR, and gait speed) predicted decline in different cognitive domains. Cognitive indices of the four domains, derived from principal component analyses, at each time point were the dependent variables. To consider if baseline gait was a significant predictor of cognitive decline a model that included time, baseline gait and an interaction term between them was used:
If the interaction term beta3 was significant, the interpretation would be that individuals with different baseline gait values have different slopes with respect to time, and therefore rates of cognitive decline. When model residuals were tested for normality, variability in step time and DST were positively skewed and therefore transformed with appropriate functions. Coefficients of these gait measures were presented in the original units by back transforming with appropriate non-linear combinations of the model parameters. Unadjusted and models adjusted for baseline age, sex, and education were performed. There was a substantial participant drop out between the baseline and follow up phases. To address any bias that could arise due to this attrition, we performed a sensitivity analysis with inverse propensity weighting. Participants who remained and have the same factors as in the drop out sample were weighted by their probability of being a complete case. Thereby, those participants receive a larger weight and contribute more to the models. Propensity weights were created using baseline age, sex, education, gait speed, and medical history (history of high blood pressure, diabetes, myocardial infarction, stroke, diabetes, arthritis, depression).
In addition, to determine whether poor baseline gait combined with the presence of ApoE4 genotype was associated with greater decline in cognitive functions a three-way interaction term (baseline gait× ApoE4×time) was tested in the model. Where a gait characteristic was associated with cognitive decline over time, the rate of change in the cognitive function was calculated and graphically presented at the highest and lowest quartiles of that baseline gait measure (poorer versus better gait performance).
We performed two secondary analyses. Gait variability and cognitive impairment are both strongly linked to gait speed, therefore we were interested in determining whether the effects of baseline gait variability on cognitive decline are independent of gait slowing. We tested this by adding a gait speed×time interaction term to the models and examined its effect on associations between gait variability and cognitive decline. Secondly, gait is thought to be a good overall marker of a person’s health status. Therefore, we performed a separate analysis to examine whether poorer gait performance (slow speed, greater variability, and smaller WSR) may be associated with cognitive decline due to the combined effects of dementia risk factors (CVD, BMI, or depression). To do this, the associations between dementia risk factors (i.e., CVD score×time) and cognitive decline were tested using mixed effects models as above. For any risk factor that was associated with cognitive decline, we examined whether the effects were mediated through gait characteristics by comparing models including just the risk factor and time interaction, with models that had this term as well as a gait×time interaction term. STATA (StataCorp LLC Texas, USA) version 15.0 was used in all the analyses.
RESULTS
Baseline characteristics of the sample
Table 1 summarizes the characteristics of participants at baseline (n = 410). The average age of participants was 72.0 (SD 7.0) years, 56.8% were male and the baseline gait speed was 1.14 (SD 0.21) m/s. From the initial cohort, 282 participants were available at phase 1 while 250 participants were available at phase 2. Participants who completed all phases were younger (p < 0.001), had lower prevalence of any CVD (p = 0.035), a lower depression score (p = 0.003), faster gait speed (p < 0.001), lower temporal variability (p < 0.05), and better cognitive performance (p < 0.001). The differences in baseline characteristics between participants who were lost to follow up and those who completed all three phases are summarized in (Supplementary Table 1).
Baseline characteristics of the study sample (n = 410)
SD, standard deviation; BMI, body mass index; CVD, cardiovascular disease; COWAT, Controlled Oral Word Association Test; kg, kilograms; ms, milliseconds; cm, centimeter; *in a subsample of n = 384 participants; **in a subsample of n = 177 participants; Presence of any CVD is a summary score based on the number of risk factors including hypertension, hypercholesterolemia, ischemic heart disease, diabetes mellitus, and stroke.
Cognitive scores at each phase are summarized in (Supplementary Table 2).
Baseline gait measures and associations with decline in specific cognitive functions
Unadjusted associations between baseline gait measures and cognitive decline are summarized in (Supplementary Table 3).
Gait variability and WSR
Baseline higher DST variability (ms) was associated with greater decline in memory: [β= –0.59 (95% CI –1.13, –0.06) p = 0.03]. Figure 1 depicts the difference in the rate of change in memory over time between people in 25th and 75th quartiles of DST variability. Variability in step length, step width and step time and WSR were not significantly associated with decline in any of the cognitive domains (Table 2).
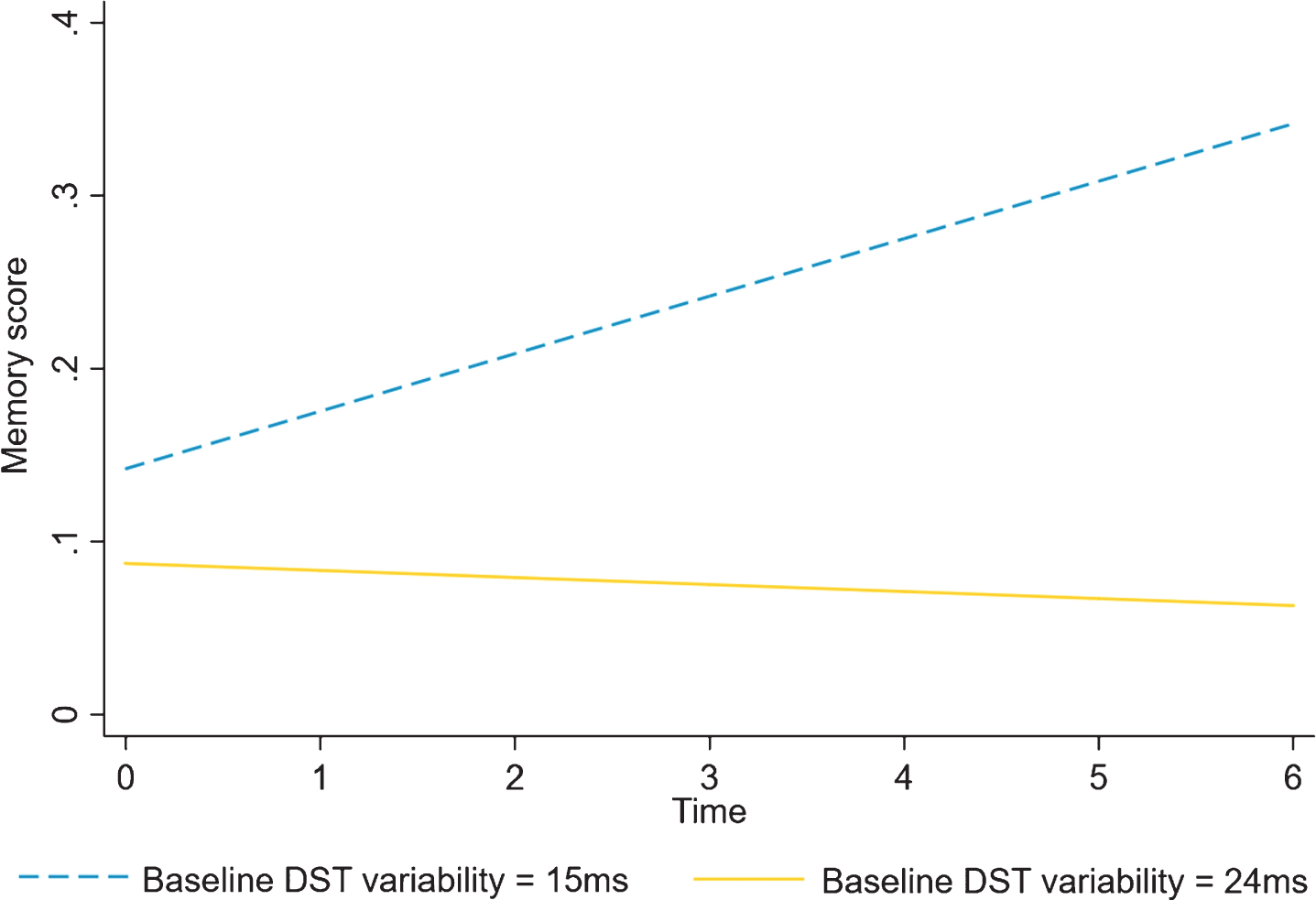
The model fit of baseline double support time variability and its association with memory over time; Differences in change in memory over time are shown for the highest and lowest quartile of baseline DST variability.
Adjusted associations between baseline gait measures and decline in each cognitive domain. Beta coefficients are the coefficients for interaction terms between baseline gait measures and time, and represent change in each cognitive function per year predicted by baseline gait
β coefficients of the interactions between baseline gait measures and time adjusted for baseline age, sex and education, 24 statistical tests were performed in this analysis. An adjustment to p-values for multiple comparison was not made as both gait and cognitive variables are correlated and tests of multiple comparisons assume independence of outcomes.
Gait speed
Baseline slower gait speed was associated with greater decline in processing speed: [β= 0.10 (95% CI 0.01, 0.18) p = 0.02] and visuospatial function: [β= 0.76 (95% CI 0.06, 1.45) p = 0.03]. Figure 2a shows the differences in the decline in processing speed and visuospatial function in people with faster and slower gait speeds (categorized with quartiles where differences in decline are shown for people in the 25th and 75th quartiles).
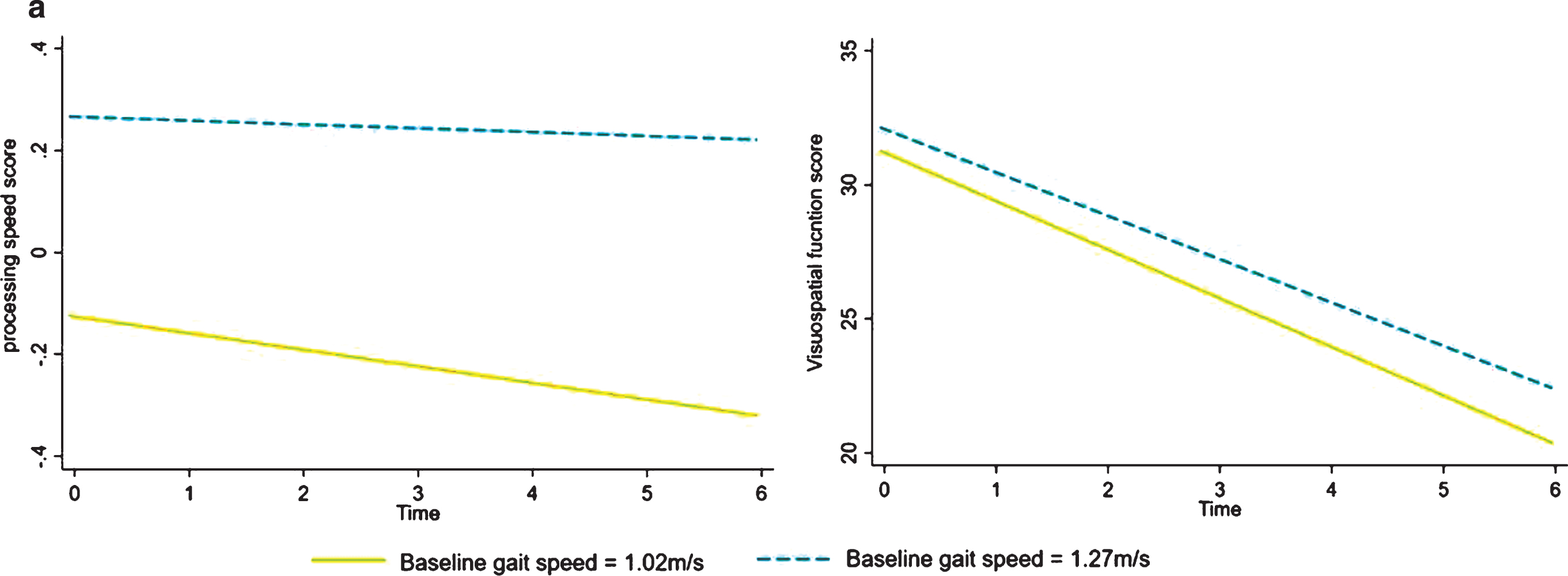
The model fit of baseline gait speed and its association with a) processing speed and b) visuospatial function over time; Differences in change in processing speed and visuospatial functions are shown for the highest (faster) and lowest (slower) quartiles of baseline gait speeds.
As there were some participants (41.7%) did not complete all 3 phases we also present the associations between baseline gait characteristics and cognitive decline, after applying propensity weights (Supplementary Table 4). Associations that we found above remained significant and stronger in the weighted models. In addition, baseline greater DST variability was associated with decline in visuospatial function: [β= –2.92 (95% CI –5.31, –0.54) p = 0.02] and baseline slow gait speed predicted decline in executive function: [β= 0.10 (95% CI 0.02, 0.18) p = 0.01].
Effect modification by ApoE4
Three hundred and eighty-four participants had blood analyses for ApoE4. Slower baseline gait speed predicted decline in memory only in those with ApoE4: [β= 0.34 (95% CI 0.04, 0.63) p = 0.02] (Fig. 2b). There were no other significant interactions (p > 0.05).
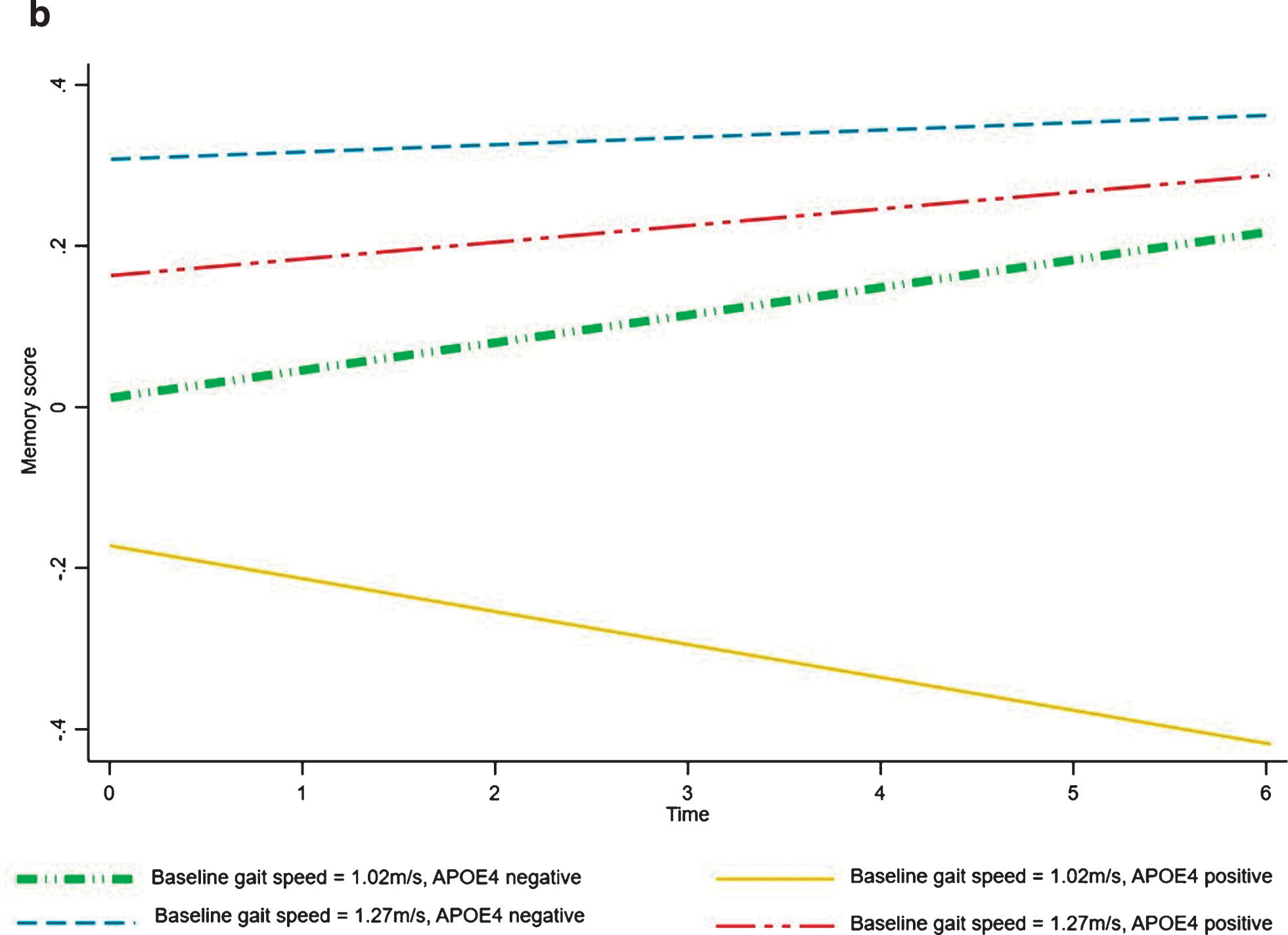
The model fit of baseline gait speed and its association with memory over time in people with and without the ApoE4 genotype; Differences in change in memory is shown for the highest (faster) and lowest (slower) quartiles of baseline gait speeds combined with presence or absence of APOE4 genotype.
Secondary analyses
The addition of the gait speed×time interaction term did not meaningfully alter the associations between DST variability and decline in memory: [β= –0.62 (95% CI –1.24, –4.20e–06) p = 0.048]. None of the dementia risk factors (CVD, BMI, or depression) were significantly associated with cognitive decline, therefore mediation by gait characteristics of these effects were not tested.
DISCUSSION
In this cohort of community-dwelling older people, greater DST variability was the only gait variability measure that was associated with cognitive decline, predicting decline in the memory domain. In contrast, slower gait speed was associated with decline in both processing speed and visuospatial function, as well as memory but only in people with ApoE4 genotype. These findings contribute to the understanding of gait measures that may have the potential to be translated into functional markers to identify older people at risk of cognitive decline and future dementia.
Gait variability
Higher DST variability was associated with decline in memory. This is consistent with cross-sectional studies, where higher DST variability was associated with mild cognitive impairment and dementia [2, 18]. In a longitudinal study, a higher score on a gait variability factor (loaded on variability in stride length and swing time) predicted future dementia [7], but not decline in executive function, attention, or memory [7]. Gait is multifaceted with correlations between individual gait measures, but different gait characteristics may not necessarily behave uniformly [14, 15] and may be controlled by different brain constructs [19]. Therefore, using factor analysis could be problematic if gait characteristics vary in their sensitivity to cognitive decline.
Currently little is known about the brain regions involved in the control of DST variability, hence we can only speculate on why DST variability is more sensitive to memory decline than other variability measures. One reason may be that DST variability may capture both central and peripheral impairments to a greater extent than other measures and therefore provide a good marker of outcomes that are associated with a wide range of risk factors. For example, in prior cross-sectional studies DST variability was associated with a greater number of sensorimotor [20] and cognitive domains [10] than other variability measures, and showed the strongest associations with increased risk of falls in a prospective study over 12 months [14]. The neural correlates of DST variability are currently unknown. The double support phase of gait is the only period where both feet are in contact with the ground and it is more variable in the presence of poor balance [20, 26]. The hippocampus and parahippocampal gyrus are the primary areas of memory and spatial navigation [27], but beyond this traditional role, the hippocampus also appears to be involved in human balance control. This is indirectly supported by higher hippocampal volumes in veteran ballet dancers and slackliners [28] and in healthy older people following balance training [29, 30]. Therefore, it is plausible that age associated changes in the hippocampal formation result in both greater DST variability and memory impairment, however this remains speculative.
Walking speed reserve
Interestingly WSR was not associated with decline in any of the cognitive domains despite cross-sectional evidence that a smaller WSR was associated with worse cognitive profiles [8]. Given only a subsample of our participants (n = 177) had fast pace gait speed measured, it is possible that we lacked statistical power for the required interaction term. For example, the effect size measured for WSR and visuospatial function is small but potentially clinically meaningful: a one standard deviation difference in baseline WSR is associated with a change in visuospatial function score over five years of 1.05 in the z-score. However, a simulation using the study data shows that a sample size of 503 would be required to obtain 80% power. Alternatively, as the beta-coefficients were this small or smaller for most domains, there truly may be no relationship between WSR and cognitive decline.
Gait speed
Slower gait speed at baseline was associated with greater decline in processing speed and visuospatial function. This is in line with the few prior longitudinal studies to date [31–34] and consistent with knowledge of brain regions important for these cognitive functions (i.e., prefrontal, medial temporal, and parietal) and their association with slow gait [35]. Slow gait speed did not predict decline in the executive domain, which in our study comprised of tests of verbal fluency (COWAT), working memory (digit span), and inhibition (the Stroop interference). This is in contrast to other studies that found gait speed (or a pace factor) was associated with other combinations of tests that represent executive function, such as animal naming alone [32], a factor score comprising of the Digit Symbol and Trail Making Test B [34] or the Digit Symbol and Letter Fluency tests [7]. Furthermore, the Rey Complex Figure task used in the assessment of visuospatial function in our study may have also captured some elements of planning and thereby executive function.
Gait speed was also associated with decline in memory, but only in people with the ApoE4 genotype. Emerging evidence suggests that having ApoE4, in addition to being a risk factor for Alzheimer’s disease, may put older people at risk of accelerated gait slowing and increased variability [36, 37]. ApoE4 is linked to increased amyloid-β deposition, cortical thinning and atrophy [38], potentially explaining its associations with both cognitive and gait impairments. Prior studies have reported contradictory results on whether gait speed is linked to memory decline. In the Einstein Ageing Study a pace factor (driven by speed and stride length), was not associated with decline in episodic memory [7], whereas slower speed was associated with memory decline in three studies [32, 39]. Interestingly, in the study from Meilke et al. [34], the significant association between gait speed and memory disappeared following the exclusion of participants with incident mild cognitive impairment or dementia. Further, older women in the study by Krall et al. [39] were followed up over a longer time period (nine years). Therefore, it is possible that gait speed in our study might have predicted memory decline in non-APOE4 carriers, had we followed up the cohort for a longer duration.
Clinical significance
The findings have the potential to be translated into clinical practice. Gait speed can easily be measured in a hallway with a stopwatch. The relatively quick, inexpensive, and non-invasive nature of measuring gait speed enhances its attraction when compared with imaging biomarkers, and it may be independent of language unlike cognitive testing [40]. In addition, gait speed was associated with the greatest range of cognitive domains (processing speed, visuospatial function, and memory in ApoE4 carriers only). However, further work is required to replicate these findings in a clinical population and to determine if there is a threshold for gait speed (or DST variability) that provides adequate predictive ability. Our findings suggest that incorporating DST variability into an assessment might provide additional information regarding future memory decline even in non-ApoE4 carriers, and potentially assist in more refined diagnostics. Quantitative testing of gait is becoming increasingly popular with the advent of instrumented walkways or foot sensors, and although may not be feasible for general practice, could be introduced into cognitive and memory disorder clinics.
Strengths and limitations
To the best of our knowledge this is the first study to examine whether gait characteristics, other than gait speed (gait variability or WSR), are associated with decline in specific cognitive domains, which were assessed using a comprehensive battery of neuropsychological tests. The use of a randomly selected sample of older people from the electoral roll increases the generalizability of our findings. We used longitudinal mixed effect models which are able to handle missing and unbalanced data. Further, we had ApoE4 genotyping allowing us to examine interactions between this genotype and motor phenotypes of cognitive decline.
The estimates for gait variability measures may have been more precise had we measured a greater number of steps, which in turn might have provided us with more power to detect associations with cognitive decline. However, we weighed this up with unnecessary fatigue. We had a moderate level of people who did not complete all three phases (41.7%). It is possible that this attrition may have had an effect on the estimates of associations between baseline gait and cognitive decline, However, the fact that the dropout group have a greater prevalence of disease, or are older, is not enough in itself to produce bias in the estimate. Such factors should show up in tests of 3-way interactions (i.e., disease×gait×time). We found no statistically significant or clinically convincing associations. Also, to address any bias due to attrition, we reported the results of a sensitivity analysis in which we applied propensity weights to the original models. However, we cannot rule out the presence of unobserved factors. For example, if participants with greater burden of unobserved disease were lost to follow-up, then the results may be biased towards the null hypothesis and then any statistically significant results represent a conservative estimate of the association. Finally, we did not include in our study protocol a walking whilst talking test, which has recently been found to predict incident dementia [9, 41]. Therefore, we are unable to compare whether gait characteristics we examined are more sensitive in predicting cognitive decline.
Conclusion
Discrete gait measures were associated with decline in specific cognitive domains. Greater DST variability and slow gait speed (only in those with ApoE4) predicted decline in memory, whereas gait speed predicted decline in processing speed and visuospatial function. These findings add to the evidence that gait is an early indicator of cognitive impairment, but that specific gait measures may provide diagnostic insights into specific cognitive domains.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the National Health and Medical Research Council (grant number 403000BH), Physiotherapy Research Foundation (grant number BH036/05), Perpetual Trustees, Brain Foundation, Royal Hobart Hospital Research Foundation (grant number 341M), and ANZ Charitable Trust and Masonic Centenary Medical Research Foundation.