
Abstract
Background:
Subjective cognitive decline (SCD) refers to the self-perception of cognitive decline among cognitively normal elderly individuals. SCD related worry confers a higher risk of developing cognitive decline. However, the clinical characteristics of SCD patients with worry are not clear.
Objective:
To explore the clinical characteristics of SCD patients with worry.
Methods:
A cross-sectional study was carried out, with 270 consecutive participants of the Sino Longitudinal Study on Cognitive Decline (SILCODE) study. Participants were classified as normal controls (n = 36), SCD patients without worry (n = 91), or SCD patients with worry (n = 143) and were comprehensively compared on 1) their self-perception of cognitive decline, 2) multiple cognitive domains, 3) neuropsychiatric symptoms, and 4) sleep status.
Results:
SCD patients with worry had significantly more self-perception of cognitive decline (p < 0.001); increased depression (p < 0.001) and anxiety (p < 0.001); decreased sleep quality (p < 0.001), sleep latency (p < 0.05), sleep time (p < 0.01), and sleep efficiency (p < 0.05); more sleep disorders (p < 0.05) and daytime dysfunction (p < 0.05); and a higher global score on the Pittsburgh Sleep Quality Index (p < 0.001) than normal controls. Although there was a significant increase only in self-perception of cognitive decline (p < 0.001), anxiety (p < 0.001), and Pittsburgh Sleep Quality Index scores (p < 0.05), the severity of the increase in those without worry was between that in SCD patients with worry and normal controls.
Conclusion:
Our findings show that participants who had SCD with worry showed distinct clinical characteristics compared with normal controls and SCD patients without worry, which could be useful for understanding the higher risk in SCD patients with worry of subsequently developing Alzheimer’s disease.
Keywords
INTRODUCTION
Alzheimer’s disease (AD), characterized by memory loss and other impairments of the cognitive domain, is the most common cause of dementia [1, 2]. Current anti-amyloid approaches to prevent, delay, and treat AD are not effective for patients with mild to moderate AD dementia [3–7]. Therefore, the best time to treat AD would be in the ultra-early phase, namely, in the preclinical stage of AD, when the damage is reparable [8]. Preclinical AD clinically manifests as normal performance in objective cognitive tests and sometimes presents mild neurobehavioral symptoms including depression, anxiety, and apathy [9], which has become a major research focus [10, 11]. As such, the key point is to identify these patients at the preclinical stage of AD.
Currently, there is a strong agreement that subjective cognitive decline (SCD) could be considered the preclinical stage of AD [12]. SCD refers to a self-perception of cognitive decline among cognitively normal elderly individuals [13]. A growing body of evidence suggests that SCD increases the risk of incident mild cognitive decline (MCI) or dementia due to AD [14, 15]. Meanwhile, SCD is associated with increased levels of AD biomarkers [16–18]. However, at the same time, it is worth noting that not all cases of SCD predict a decline to MCI or dementia [19], as other factors such as neuroticism, medication, and substance use may contribute to SCD [20]. Therefore, there is an urgent need to clarify which characteristics of SCD patients could predict cognitive decline over a relatively short time frame. Previous longitudinal studies revealed that SCD with worry was associated with a significantly increased risk of developing MCI or dementia [14, 22]. Worry increases the specificity in predicting cognitive decline for SCD patients. It is likely that SCD with worry may present more serious clinical problems than SCD without worry. Consequently, it is important to characterize the clinical profiles of SCD patients with worry to understand the utility of the condition in predicting subsequent progression to MCI or AD.
Here, we comprehensively investigate the clinical characteristics of SCD patients with worry relative to SCD patients without worry and normal controls regarding their self-perception of cognitive decline, multiple cognitive functions, neuropsychiatric symptoms and sleep status. We hypothesized that markedly different clinical profiles would be found in subjects with SCD with worry.
METHODS
Ethics statement
Our study protocol was approved by the medical ethics committee of Xuanwu Hospital of Capital Medical University, Beijing, China, and all participants gave their written informed consent before any study procedures began.
Study population
The participants in our study were part of an ongoing study cohort: the Sino Longitudinal Study on Cognitive Decline (SILCODE). SILCODE, an observational longitudinal study carried out by Xuanwu Hospital of Capital Medical University, Beijing, China (ClinicalTrials.gov, NCT 03370744), is the first project committed to promoting SCD research in China. The main purpose of this project is to collect longitudinal data from the SCD population and then study the dynamic changes in brain networks to explore the progressive mechanisms of AD in the brain and to construct a high-precision multimodal model for the ultra-early diagnosis of AD. Baseline recruitment started in 2017 and is still ongoing. Participants in this study consisted of normal controls (NC) and SCD, MCI, and AD patients. Participants were recruited from the memory clinic, recruitment activities in the community, and referrals from local clinicians in China. At the baseline visit, every participant underwent a standardized diagnostic evaluation including a medical history interview, physical and neurological examinations, laboratory tests, and neuropsychological tests. In addition, we collected structural magnetic resonance imaging (sMRI), diffusion tensor imaging (DTI), resting-state functional magnetic resonance (rs-fMRI), and AV-45-positron and emission tomography (Aβ-PET) or 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET) separately with a GE 750w Signa integrated PET/MRI system (America). For the parameters of each sequence, please refer to http://www.abimaging.org. Each participant will be followed up every 15 months. All participants aged between 60 and 80 years old were Mandarin-speaking, had at least 6 years of education, and were right-handed. The main exclusion criteria were as follows: 1) a history of central nervous system disease that may cause cognitive impairment including stroke, Parkinson’s disease, or traumatic brain injury; 2) psychiatric disease, such as severe depression or anxiety; 3) other systemic disease such as severe anemia, thyroid dysfunction, syphilis, or gas poisoning that could lead to cognitive impairment; 4) alcohol or drug abuse; and 5) severe visual or auditory disabilities or failure to finish the PET-MRI examination. The diagnostic criteria of NC were as follows: 1) no self-reported persistent decline in cognitive capacity and neither worry nor concern about their cognition, and 2) no measurable cognitive impairment according to the results of standard neuropsychological assessments. The diagnostic criteria of SCD patients were as follows: 1) the presence of self-perceived continuous cognitive decline compared to a previous normal status and unrelated to an acute event, and 2) failure to meet the following criteria for MCI. The diagnostic criteria of MCI patients are defined by an actuarial neuropsychological method proposed by Jak and Bondi [23]. Participants are considered to have MCI if any of the following three criteria are met: 1) having impaired scores (defined as >1 SD below the age-corrected normative mean) on both measures within at least one cognitive domain (i.e., memory, language, or speed/executive function); 2) having impaired scores in each of the three cognitive domains sampled; and 3) a Functional Activities Questionnaire (FAQ) score ≥9. The diagnostic criteria of AD patients are based on the diagnostic guidelines for dementia due to AD delivered by the National Institute on Aging-Alzheimer’s Association workgroups (NIA-AA) with a total Clinical Dementia Rating (CDR) score ≥1 [24]. A total of 270 participants from the baseline visit were included in the current analysis (Fig. 1).
The flow chart of this study. MCI, mild cognitive decline; AD, Alzheimer’s disease, NC, normal controls; SCD–, subjective cognitive decline patients without worry; SCD+, subjective cognitive decline patients with worry.
Clinical and laboratory variables
A case report form (CRF) was used by neurologists to record demographic and clinical variables, such as age, gender, years of education, ethnicity, marital status, social support over the past year (“living alone” or “living with family”), eating habits (“vegetarian”, “carnivorous”, or “ordinary diet”), body mass index (BMI, kg/m2), history of hypertension, diabetes, hyperlipidemia, smoking, alcohol use, drinking tea or coffee, and eating fish. In this study, a BMI >24 kg/m2 was considered overweight.
In addition, blood samples were collected from all participants after an overnight fast. This work was performed by the staff of the clinical laboratory to detect levels of blood glucose, blood lipids, homocysteine, folic acid, vitamin B12, thyroid hormone, hemoglobin, and blood coagulation and to determine a syphilis-free status and the apolipoprotein E (ApoE) gene polymorphism status.
ApoE genotyping
The single nucleotide polymorphisms (SNPs) rs7412 and rs429358 form the ApoE ɛ2/ɛ3/ɛ4 haplotype. APOE was genotyped using the standard Sanger sequencing method (Sangon, Shanghai, China) with the following primers: 5′-ACGCGGGCACGGCTGTCCAAGG-3′ (forward) and 5′-GGCGCTCGCGGATGGCGCTGA-3′ (reverse). APOE was amplified using the following conditions: 1 cycle at 98°C for 10 s, 35 cycles at 72°C for 5 s, and 1 cycle at 72°C for 5 min. Polymerase chain reaction (PCR) was performed in a final volume of 30μl containing 10 pmol of forward and reverse primers, and 50 ng of genomic DNA template using PrimeSTAR HS DNA polymerase with GC Buffer (Takara Bio, Kusatsu Shiga, Japan).
Neuropsychological tests
Trained research assistants conducted all neuropsychological tests. A subjective cognitive decline questionnaire (SCD-Q) of nine items was applied to measure self-perceived cognitive decline, with higher scores indicating greater perceived cognitive decline [25]. The Hamilton Depression Rating Scale (HAMD) [26] and the Hamilton Anxiety Scale (HAMA) [27] were used to assess neuropsychiatric symptoms. The Auditory Verbal Learning Test-Huashan version (AVLT-H), an adapted Chinese version of the California Verbal Learning Test, was used to assess immediate recall, short-delayed free recall (5 min), long-delayed free recall (20 min), and long-delayed recognition [28]. Executive function was assessed by the Shape Trailing Test A (STT-A) and Shape Trailing Test B (STT-B) [29]. Language was assessed by the animal fluency test (AFT) [30] and the Boston Naming Test (BNT) [31]. Memory and Executive Screening (MES) [32], a brief cognitive screening tool for the early detection of AD, focuses on both memory and executive function. The Montreal Cognitive Assessment-Basic (MoCA-B) [33] was performed to assess global cognitive condition. The Pittsburgh Sleep Quality Index (PSQI) [34], Rapid-eye-movement Sleep Behavior Disorder Screening Questionnaire (RBDSQ) [35], and Epworth Sleepiness Scale (ESS) [36] were applied to assess participants’ sleep status.
Definitions of SCD with worry and without worry
A semi-structured interview developed by the German Center for Neurodegenerative Diseases (DZNE) longitudinal cognitive impairment and dementia study (DELCODE) [37] was used to evaluate the details of SCD before cognitive testing. This interview included information about the presence and onset of concerns, comparisons with other and a history of visiting a physician, related not only to memory but also other cognitive domains. For example, if one participant had a memory complaint, its duration (within the last 6 months, between 6 months and 2 years, between 2 years and 5 years, more than five years, or unclear) would be further determined. Then, they would be asked if they are worried about it and how they compare themselves with their peers (if they feel they are worse or not). They would also be asked if they had visited the memory clinic previously because of memory complaints. Participants without measurable cognitive impairment who denied a decline in memory were considered NC. Participants without measurable cognitive impairment who had memory complaints but did not worry about them were classified as SCD patients without worry. Participants without measurable cognitive impairment who had memory complaints and worried about them were classified as SCD patients with worry. Finally, the characteristics of SCD patients were assessed to exclude sudden memory complaints caused by other conditions (e.g., stroke, gas poisoning).
Statistical analyses
The statistics were summarized to illustrate the characteristics of the variables’ distributions. The Kolmogorov–Smirnov test and a Q-Q plot were used to confirm normality. All normally distributed continuous variables were reported as the mean±standard deviation (SD). Analysis of variance (ANOVA) was performed and Dunnett’s multiple comparison tests were conducted for post hoc comparison. Non-normally distributed continuous variables were described with the median and interquartile ranges, and Kruskal-Wallis tests (nonparametric tests) were used for post hoc comparison. The chi-squared (χ2) test was employed to assess differences between groups for categorical variables and were reported as percentages. A linear regression model was used to correct the effects of anxiety and depression on sleep status in each group, as covariates, to avoid differences between groups caused by emotional factors. All data analyses were conducted using SPSS (version 25.0 for Window). Figures were made using GraphPad Prism version 8.0.0 for Windows, GraphPad Software, San Diego, California USA. p < 0.05 was considered significant.
RESULTS
Demographic characteristics
Of the 270 participants, 36 (13.3%) did not indicate self-perceived cognitive decline, 91 (33.7%) indicated self-perceived cognitive decline without worry, and 143 (53%) indicated self-perceived cognitive decline with worry. The mean age was 65 (63–69) years old, 64.4% of subjects were female and the mean years of education was 12 (11–15) in this study. As shown in Table 1, there was no difference between participants in demographic, social support, clinical, lifestyle, or genetic characteristics. The proportion of ApoE ɛ4 allele carriers in this sample was 22.2%, with 19.4% of NC, 18.7% of SCD patients without worry, and 25.2% of SCD patients with worry being carriers.
Demographic characteristics of the study participants
All continuous variables in the table were non-normally distributed and described as median (interquartile). NC, normal control; SCD–, subjective cognitive decline without worry; SCD+, subjective cognitive decline with worry; BMI, body mass index. *The p value was calculated using Kruskal-Wallis test. #The p value was calculated using Chi-square.
Neuropsychological testing
Table 2 displays the results of the neuropsychological tests. Measures of cognitive function including AVLT-H, STT-A, STT-B, AFT, BNT, MES, and MoCA-B assessments, revealed no significant differences between NC, SCD patients without worry, and SCD patients with worry.
Score for each neuropsychological test
All continuous variables in the table were non-normally distributed and described as median (interquartile). NC, normal controls; SCD–, subjective cognitive decline patients without worry; SCD+, subjective cognitive decline patients with worry; SCD-Q, subjective cognitive decline questionnaire; HAMD, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Scale; AVLT-H-I, auditory verbal learning test-immediate recall; AVLT-H-D1, auditory verbal learning test- short-delay free recall (5 min); AVLT-H-D2, auditory verbal learning test- short-long free recall (20 min); AVLT-H-R, auditory verbal learning test-long delay recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MES, Memory and Executive Screening; MoCA-B, Montreal Cognitive Assessment-Basic; PSQI, Pittsburgh Sleep Quality Index; RBDSQ, Rapid-eye-movement Sleep Behavior Disorder Screening Questionnaire; ESS, Epworth sleepiness scale. *The p value was calculated using Kruskal-Wallis test.
The three groups differed significantly from each other (p < 0.001, respectively) on SCD-Q score. SCD patients with worry had the highest score, followed by SCD patients without worry, and NC had the lowest score (Fig. 2A).
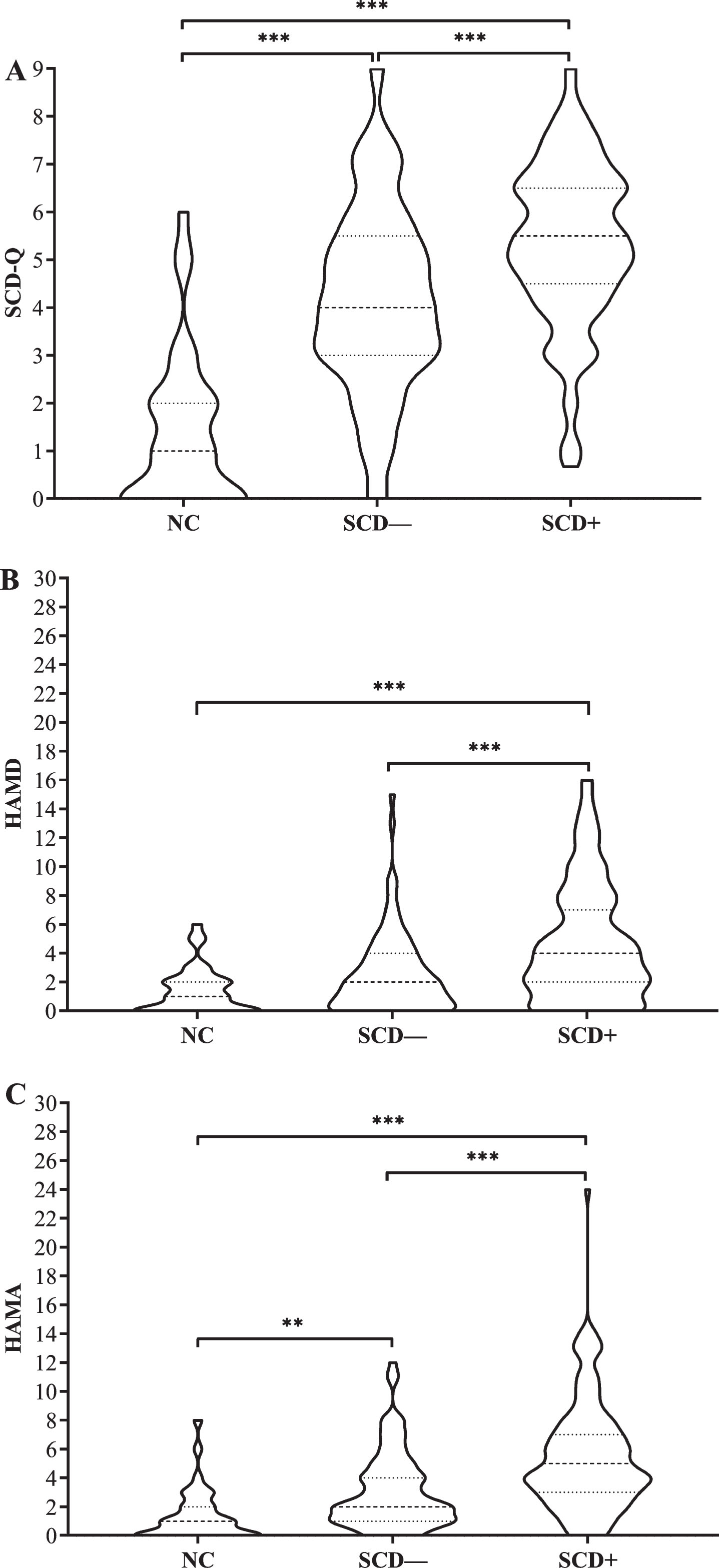
Showing group differences in neuropsychological tests. A) SCD-Q, B) HAMD, C) HAMA. NC, normal controls; SCD–, subjective cognitive decline patients without worry; SCD+, subjective cognitive decline patients with worry. **p < 0.01, ***p < 0.001.
Regarding HAMD scores, SCD patients with worry had the highest score, followed by SCD patients without worry, and NC had the lowest score. Significant differences were found between SCD patients with worry and NC (p < 0.001), between SCD patients with worry and SCD patients without worry (p < 0.001), but not between SCD patients without worry and NC (Fig. 2B). Regarding HAMA scores, SCD patients with worry had the highest score, followed by SCD patients without worry, and NC had the lowest score. The three groups differed significantly from each other (Fig. 2C). Significant differences were found between SCD patients with worry and NC (p < 0.001), between SCD patients with worry and SCD patients without worry (p < 0.001), and between SCD patients without worry and NC (p < 0.01).
Table 2 shows group differences in sleep quality (p < 0.001), sleep latency (p < 0.01), sleep time (p < 0.01), sleep efficiency (p < 0.05), sleep disorders (p < 0.05), daytime dysfunction (p < 0.05), and PSQI global scores (p < 0.001), but not for hypnotic drug use (p > 0.05). Overall, SCD patients with worry had the highest scores, followed by SCD patients without worry, and NC had the lowest scores (Fig. 3). Furthermore, group differences for PSQI global scores remain significant when taking the scores of the HAMD and HAMA as covariates. Specifically, SCD patients with worry had the highest score, followed by SCD patients without worry, and NC had the lowest score. Significant differences were found between SCD patients with worry and NC (p < 0.01), between SCD patients with worry and SCD patients without worry (p < 0.001), and between SCD patients without worry and NC (p < 0.001). In addition, there were no significant differences among the three groups for RBDSQ and ESS assessments.
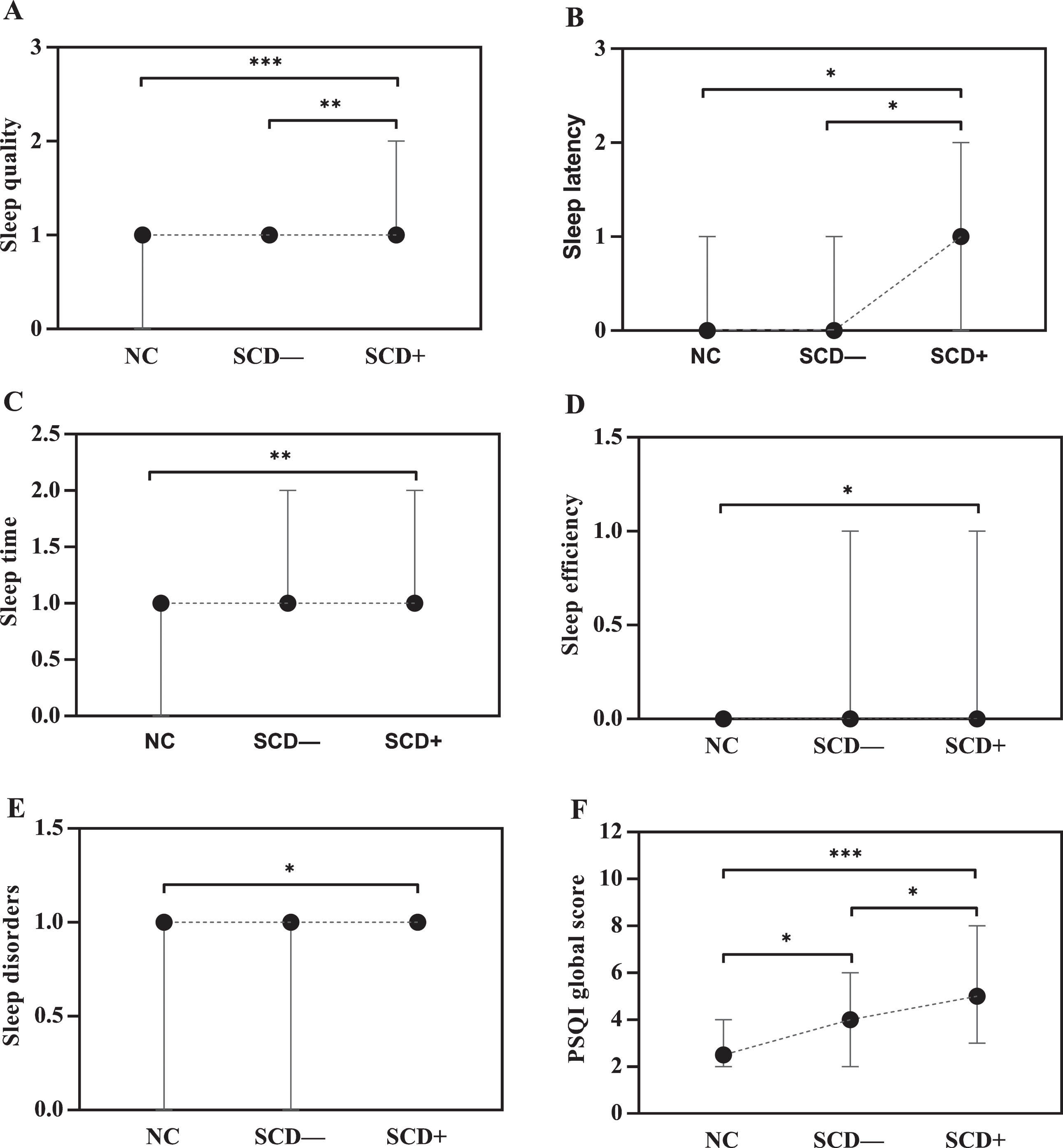
Showing group differences in PSQI. A) Sleep quality, B) Sleep latency, C) Sleep time, D) Sleep efficiency, E) Sleep disorders, F) PSQI global score. NC, normal controls; SCD–, subjective cognitive decline patients without worry; SCD+, subjective cognitive decline patients with worry. *p < 0.05, **p < 0.01, ***p < 0.001.
DISCUSSION
The goal of this study was to comprehensively investigate the baseline clinical features of SCD patients with worry relative to SCD patients without worry and normal controls within the SILCODE project. Our results showed that SCD patients with worry showed increased self-perceived cognitive decline, depression and anxiety symptoms, and sleep problems, whereas the demographic features, social support, lifestyle, and genetic characteristics among the three groups were comparable.
Our study found that the SCD-Q score for SCD patients with worry was significantly higher than that of NC and SCD patients without worry (both p < 0.001). SCD-Q is a useful tool for screening and quantifying SCD [25]. It includes measures for global memory functioning, temporal comparisons, and the ability to finish routine activities that were developed based on the SCD criteria proposed by the Subjective Cognitive Decline Initiative (SCD-I). Previous studies have suggested that a higher SCD-Q score can differentiate preclinical AD subjects from NC subjects and is associated with AD biomarkers [38, 39]. In addition, our previous epidemiological study confirmed that the SCD-Q is also applicable in Chinese SCD patients, with a Cronbach’s alpha coefficient of 0.847 and a coefficient of validity of 0.871 [40]. The results from that study showed that scores on the SCD-Q significantly increased with disease progression: NC<SCD<MCI<AD(early AD). Thus, the results in the current study were consistent with previous studies and indicated that SCD with worry may represent the last phase of preclinical AD. However, this conclusion needs to be further verified by our follow-up data.
We observed that scores related to neuropsychiatric symptoms between the three groups, assessed by the HAMD and HAMA, were within the normal range. However, there were significant differences among the groups. SCD patients with worry had increased depression and anxiety symptoms compared to SCD patients without worry or NC (p < 0.001, respectively). In addition to cognitive impairments, neuropsychiatric symptoms such as apathy, depression, anxiety, and sleep disorder were also common in AD patients. A meta-analysis revealed that depression and anxiety were highly prevalent in AD, at 42% and 39%, respectively [41]. Although the exact pathological underpinnings of neuropsychiatric symptoms in AD are still not clear, it has been proposed that neuropsychiatric symptoms and cognitive impairments share potentially common mechanisms in AD [42, 43]. Epidemiological studies have found that neuropsychiatric symptoms including anxiety, depression, agitation, and apathy in cognitively normal elderly individuals are a strong risk factor for developing MCI [44–47]. Most importantly, several studies have been conducted to investigate the relationship between neuropsychiatric symptoms and AD biomarkers in cognitively normal older people. For example, the results from a cross-sectional study derived from the Mayo Clinic Study of Aging (MCSA) showed that depression and anxiety symptoms were associated with elevated amyloid-β peptide (Aβ) levels as measured by PiB-PET in cognitively normal older people [48], and the same result was found in another study [49]. In particular, longitudinal studies have confirmed that higher Aβ burden was associated with increasing depression and anxiety symptoms in cognitively normal older adults [50, 51]. These studies link neuropsychiatric symptoms with characteristic pathological hallmarks of AD and provide evidence for the hypothesis that emerging neuropsychiatric symptoms represent an ultra-early manifestation of preclinical AD in elderly individuals with normal cognition. Consequently, these studies may offer important implication for understanding our current findings that SCD patients with worry showed increased neuropsychiatric symptoms compared to SCD patients without worry and NC, in that these differences may be due to SCD patients with worry suffering from the more severe pathological burden of AD. This issue will be explored in future studies.
We also found SCD patients with worry had the worst scores on six components of the PQSI, including sleep quality (p < 0.001), sleep latency (p < 0.01), sleep time (p < 0.01), sleep efficiency (p < 0.05), sleep disorders (p < 0.05), daytime dysfunction (p < 0.05), and PSQI global score (p < 0.001) among the three groups, which means SCD patients with worry had relatively poor sleep habits. Sleep alteration remained significantly different even when emotional factors were used as covariates. Until now, it has not been clear whether sleep disturbances contribute to AD or are secondary outcomes of AD, and research on the relationship between sleep disturbances and AD has attracted considerable attention. However, evidence is mounting that sleep disorders increase the risk of AD. A recent meta-analysis systematically reviewed the predictive roles of sleep disturbances, such as insomnia, sleep disordered breathing and other sleep problems in incident AD [52]. The results showed that individuals with sleep disorders were at a higher risk of developing AD than subjects without sleep disorders. It has been proposed that sleep disorders are involved in the pathogenesis of AD. Several studies in mice and humans have shown that disrupted sleep increased both Aβ and tau burden [53–56]. These studies suggest that sleep disorders may increase AD risk via increased Aβ and tau accumulation. However, sleep problems are common in AD and MCI patients [57–59]. Moreover, a community-based study found that SCD participants had disrupted sleep including increased nighttime wakefulness and reduced sleep efficiency [60]. Another cross-sectional study also found that sleep problems were associated with SCD [61]. Thus, our findings are consistent with previous studies in which the sleep status of SCD patients was worse than that of NC. One explanation could be that sleep and AD pathology is a bidirectional relationship: the accumulation of Aβ could alter sleep patterns, and then cause sleep problems [62]. A previous study confirmed that the normal cognitive group with Aβ deposition (in the preclinical stage of AD) experienced worse sleep quality than those without Aβ deposition [63]. Accordingly, we suspect that SCD with worry may represent advanced preclinical AD with more severe Aβ burden and verify that this hypothesis will be the main work of our research group in the future. In the present study, we also assessed daytime sleepiness and REM sleep behavior disorders in SCD patients with/without worry. However, the groups did not differ significantly from each other on RBDSQ and ESS scores. It can be inferred that an increased tendency toward daytime sleepiness occurs in advanced AD [64] and that REM sleep behavior disorders may not be characteristic of early AD but may represent an early clinical manifestation of other neurodegenerative disorders, such as Parkinson’s disease or multiple system atrophy [35].
There was no detectable difference between groups in terms of cognitive function, such as memory, language, executive function or global cognitive function, in traditional cognitive assessments. This finding aligns with perceptions and the results of most current studies suggesting that SCD does not meet the criteria for cognitive impairment and is within the normal range on standardized neuropsychological tests [20]. Nonetheless, studies suggest that there may be a subtle decline in psychomotor speed [65] and prospective memory tasks in SCD patients relative to NC [66]. These findings support the idea that the occurrence of SCD preceding MCI could be detected with traditional cognitive assessment.
It is important to note that this study has some limitations. First, the participants in this study have a relatively high level of education, younger age, and are mostly female. Thus, caution should be taken when generalizing the findings of this study to populations with different sociodemographic characteristics. Second, the present study was a cross-sectional study. We cannot determine whether SCD with worry is the cause of the differences in the clinical characteristics between groups, or whether subtle sleep problems or neuropsychiatric symptoms lead to SCD with worry. Moreover, it may be more valuable to capture complaints in domains such as language, attention, and executive function rather than only focusing on memory complaints. However, the study’s strengths are that we comprehensively investigated the clinical profiles of SCD patients with worry including self-perception of cognitive decline, multiple cognitive functions, neuropsychiatric symptoms and sleep status after we considered as many factors as possible that might have an impact on these results.
Overall, our results suggest that self-perception of cognitive decline, depression and anxiety symptoms, and sleep problems become progressively worse in SCD patients with worry patients. These results are helpful for understanding the higher risk associated with SCD with worry of subsequently progressing to MCI or AD.
Footnotes
ACKNOWLEDGMENTS
This article was supported by the National Key Research and Development Program of China (2016YFC1306300), National Natural Science Foundation of China (Grant 61633018, 81430037), Beijing Nature Science Foundation (7161009), and Beijing Municipal Commission of Health and Family Planning (PXM2019_026283_000002). We sincerely appreciate Xue Wang, the Library of Xuanwu Hospital of Capital Medical University for her help in searching for correlative references.