
Abstract
Background:
Age-related hormone changes play important roles in cognitive decline in older men, and apolipoprotein E ɛ4 (APOE ɛ4) is a risk factor for Alzheimer’s disease (AD).
Objective:
This study aimed to investigate the interactive role of androgen decline and APOE ɛ4 genotype in the pathogenesis of amnestic mild cognitive impairment (aMCI) and AD.
Methods:
In total, 576 elderly men over 65 years old from communities in Shijiazhuang were enrolled in this study, including 243 with normal cognition (NC), 271 with aMCI, and 62 with probable AD. Cognitive function was evaluated with a battery of neuropsychological tests. The serum levels of androgen and gonadotropin were detected by ELISA and chemiluminescence immunoassay.
Results:
The levels of free testosterone (FT) and dihydrotestosterone (DHT) were lower in the aMCI group (p < 0.05), and even lower in the AD group (p < 0.001), but the levels of follicle stimulating hormone (FSH) and luteinizing hormone (LH)
were higher in AD group (p < 0.01), comparing with that in NC or aMCI group. The interaction of lower FT or DHT levels with APOE ɛ4 had a risk role in global cognitive impairment (p < 0.05). The area under the curve (AUC) of the ROC curve for predicting aMCI by serum FT levels was 0.745.
Conclusion:
These results indicated that the interaction of androgen decline and APOE ɛ4 genotype play a role in aMCI and AD. Serum FT levels have a predictive value for aMCI and might be a potential biomarker for prodromal AD.
INTRODUCTION
Alzheimer’s disease (AD) is a progressive neurodegenerative disease characterized by memory loss, multiple cognitive impairments, and changes in personality. The 2011 version of clinical diagnostic criteria for AD from the National Institute on Aging and the Alzheimer’s Association (NIA-AA) emphasized that AD includes mild cognitive impairment (MCI) that occurs before dementia [1]. The most common subtype of MCI is amnestic MCI (aMCI), 80% of which will progress to AD within 6 years [2]. Therefore, the identification of high-risk factors of AD, including aMCI, at early stages is the most effective strategy for AD prevention and therapy.
The etiology of AD is complex and many factors are related to its occurrence, including inheritance, environment, metabolism, intestinal flora, viral infections, and sex hormones. Partial androgen deficiency in aging males is a group of clinical symptoms of hypogonadism and androgen regulation disorder [3], in which impaired cognitive function is one of the main symptoms [4], indicating that androgen affects the function of learning and memory. It is noted that male reproductive function lacks a clear termination time point as it does in females. During aging, the level of androgen declines gradually [5], which might directly contribute to the pathogenesis of AD by affecting the deposition of amyloid-β peptide [6].
There are two main sources of androgens: testosterone (T), synthesized by Leydig cells of the testis, and dehydroepiandrosterone (DHEA) and its sulfated derivative (DHEAS), secreted by the reticulum of the adrenal cortex. Total T (TT) in the blood mainly exists in three forms: 1∼2% of T is a free form (FT), 40∼50% of T is bound to albumin loosely, which can freely dissociate from albumin and change into FT, and 50∼60% of T is tightly bound to high-affinity sex-hormone-binding globulin (SHBG) and cannot easily dissociate. FT is the bioactive form and acts as an indicator of the bioactivity of T in the blood. Some studies have shown that decreases of FT occur in the MCI stage, 5∼10 years prior to AD diagnosis [7], and lower T levels contribute to the progression of AD [8] and impaired cognition in elderly men [9–11]. Treatment with T improves the cognitive function of the elderly [12, 13]. Studies have shown that gonadotropins, which regulate the secretion of T, such as follicle stimulating hormone (FSH) and luteinizing hormone (LH), increase in AD patients [14], and high levels of LH are associated with AD pathological formation [15, 16]. These reports suggest that the decreased T and gonadotropins play key roles in the pathogenesis of AD. However, one study reported that there was no significant association between either of the sex hormones or gonadotropins with cerebral Aβ-positivity rate in males [17], and another previous study suggested that DHEA levels in the prefrontal cortex were significantly higher in male AD patients [18]. These inconsistent results prompted us to perform the current study to estimate the roles of decreased T and gonadotropins in aMCI and AD.
The apolipoprotein E (APOE) gene on chromosome 19 is polymorphic (derived from the combination of polymorphic rs429358 and rs7412), which results in 3 major isoforms: ɛ2 (112T + 158T), ɛ3 (112T + 158C), and ɛ4 (112C + 158C). These 3 alleles encode 6 genotypes, including ɛ2ɛ2, ɛ2ɛ3, ɛ3ɛ3, ɛ2ɛ4, ɛ3ɛ4 and ɛ4ɛ4. Epidemiological studies have shown that the APOE gene is an AD pathogenic gene [19], and APOE ɛ4 accelerates the progression from MCI to dementia [20, 21]. APOE ɛ4 regulates androgen synthesis and the activity of its receptor. Conversely, androgen also regulates expression of the APOE ɛ4 gene. Studies have reported that higher levels of FT are associated with better cognitive function in non-APOE ɛ4 carriers [22]. Another study showed that FT levels were positively correlated with the delayed memory function in APOE ɛ4 carriers [23]. These divergent results of the interaction between APOE ɛ4 and androgens and their effects on cognition remain to be explored.
In this cross-sectional study, elderly men were enrolled, and their cognitive function, serum levels of androgens and gonadotropins, and APOE gene polymorphisms were tested. This study aimed to evaluate whether the levels of androgens and gonadotropins and their interaction with APOE ɛ4 are associated with cognition and explore the predictors of aMCI and AD.
METHODS
Study samples
Subjects were randomly selected from the community centers in Shijiazhuang, Hebei Province, China. This study was performed from March 2018 to July 2019. The data of medical history, physical condition, nervous system, and mental functions of more than 3000 men over the age of 65 were recorded. After exclusion of cerebrovascular disease, moderate to severe hypertension and diabetes, cancer, mental illness and other systemic diseases, alcohol and drug abuse problems, depression, or a family history of AD, 2,062 subjects were selected. Of these, 1,665 men were with normal cognition (NC), 332 with MCI (include 290 with aMCI), and 65 with probable AD. In view of aMCI being the typical prodromal stage of AD [24], aMCI subjects and a similar number of NC controls were selected in this study. Subsequently, 576 subjects voluntarily agreed to participate in blood sample collection, including 243 with NC, 271 with aMCI, and 62 with probable AD. A 10 mL sample of venous blood was collected from each subject before breakfast in the morning after psychological testing. This study was approved by the Ethics Committee of the Hebei Medical University, and the written informed consent was obtained from each subject.
Neuropsychological assessment and diagnostic criteria
Global cognitive function and five cognitive domains (memory, language, attention, visuospatial and executive function) assessment were performed by well-trained research neurologists in this study. The Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA) (Beijing version) [25], and Clinical Dementia Rating scale (CDR) were used to evaluate global cognitive function. In the Beijing version of MoCA, the cut-off value of normal cognition is >24 points [26], and one point is added for those with less than 7 years of education [27]. Memory function was evaluated with the Auditory Verb Learning Test (AVLT), and this scale also assessed the subjects’ immediate recall, long delay free recall, long delay cued recall, and long delay recognition function. The Animal Fluency Test (AFT) and Boston Naming Test (BNT) were used to evaluate the language function. The Digit Span Test (DST) was used to assess the attention domain, which includes Digit Span Forward (DSF) and Digit Span Backward (DSB). Visuospatial function was evaluated using the Clock Drawing Test (CDT). Executive function was assessed with the Trail Making Test (TMT), which includes A (TMT-A) and B (TMT-B) parts. In addition, the Activity of Daily Living (ADL), Geriatric Depression Scale (GDS), and Hachinski Ischemic Scale (HIS) were used to exclude unqualified subjects.
The cut-off values of NC were MoCA > 24 points, MMSE≥27 points, and CDR = 0. The aMCI was diagnosed based on Petersen’s criteria [28] and National Institute on Aging and Alzheimer’s Association (NIA-AA) [29]. The subjects met the following criteria: 1) Complaint of memory by participant or family; 2) Cognitive impairment quantified with neuropsychological tests (AVLT score greater than 1.5 SD below the appropriate mean [30] and CDR memory = 0.5 or 1); 3) Cognitive decline inconsistent with age, although retaining basic cognitive function (MoCA≤24 [26], MMSE≥24 [31]); 4) Normal or slightly impaired activities of daily living (ADL≤26 [32]); 5) No dementia (CDR = 0.5).
AD was diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Associations (NINCDS-ADRDA) [33], in line with the probable AD dementia criteria of NIA-AA [34]. Medical history, physical examination of the nervous system, B-ultrasonic examination of the abdomen, biochemical examination of the blood, and head MRI examination were performed. Dementia including frontotemporal degeneration, Lewy body dementia, and other neurodegenerative dementia, and cerebrovascular disease, metabolic disease, and infectious disease were excluded.
Measurement of androgens and gonadotropins
In this study, the levels of six androgens and two gonadotropins were measured in peripheral blood, including TT, FT, dihydrotestosterone (DHT), bioactive testosterone (BT), DHEA, DHEAS, FSH, and LH. In addition, the levels of sex hormone-binding globulin (SHBG) were also tested. TT, SHBG, FSH, and LH were tested with a method of chemiluminescence immunoassay (CLIA Kit; Beckman Coulter Inc., Brea, CA, USA). Measurements of FT, DHT, DHEA, and DHEAS were performed by enzyme-linked immunosorbent assay (ELISA Kit; DRG International, Mountainside, NJ, USA). BT was calculated from the value of albumin and SHBG using the biological testosterone formula. The direct laboratory measurement of FT was selected in this study to avoid errors caused by indirect measurements [35, 36].
Detection of single nucleotide polymorphisms in the APOE gene
Single nucleotide polymorphisms (SNPs) of rs429358 and rs7412 were detected by first-generation sequencing. The instruments used were the ABI 2720 PCR Thermal Cycler and 3730 sequencer (Thermo Fisher, Waltham, MA, USA), and the PCR reagent was 2×GC rich PCR MasterMix (Ruibiotech, Beijing, China).
Statistical analysis
The subjects were divided into four subgroups (Q1, Q2, Q3, Q4) according to hormone value quartiles: Q1≤P25 was the lowest level of hormone, P25 < Q2≤P50 was lower, P50 < Q3≤P75 was higher, and Q4 > P75 was the highest.
A univariate test, such as Chi-square test, ANOVA, welch ANOVA, Analysis of Covariance or Kruskal-Wallis test, was used to test inter-group differences, and Bonferroni correction was used for all multiple comparisons. After controlling for age and education factors, two-way ANOVA was used to analyze the effects of APOE ɛ4 and androgens on cognition. Pearson’s correlation coefficient was used to assess the relationship between cognition and the levels of androgen and gonadotropin. Age, education, and APOE genetic polymorphisms were controlled, and logistic regression analysis was used to detect the OR and 95% CI of aMCI and AD in different androgen (Q1: Q4) and gonadotropin (Q4: Q1) subgroups. We selected statistically significant variables for multiple logistic regression analysis (stepwise method). After obtaining the independent predictors of aMCI, the logit (P) of the regression function was used as the joint predictor L’ and L was used as a test variable to create the receiver operating characteristic curve (ROC) and obtain the area under the curve (AUC) value. The cutoff value was calculated using the maximum Yuden Index (YI). We applied the external validation method to obtain the validated AUC and tested the sensitivity and specificity of the cut off values. All tests were two-sided, and p < 0.05 was considered statistically significant.
All data were analyzed using SPSS software version 22.0 (SPSS, Inc., Chicago, IL, USA). Graphs were generated using GraphPad Prism version 8.0 (GraphPad Software, Inc., San Diego, CA, USA).
RESULTS
Clinical characteristics
Demographic, physical and cognitive characteristics of the subjects in NC, aMCI, and AD groups were shown in Table 1. There were significant differences in age and education status among the NC, aMCI, and AD groups. No differences were found in the indexes of physical condition among the three groups. However, the scores of MMSE, MoCA, and the scales of each cognitive domain showed significant differences among the three groups.
Demographic, physical characteristics, and cognitive functions of the subjects in NC, aMCI and AD groups
BMI, body mass index; TC, total cholesterol; TG, triglyceride; LDL-C, low density lipoprotein; HDL-C, high density lipoprotein; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; AFT, Animal Fluency Test; BNT, Boston Naming Test; DSF, Digit Span Forward; DSB, Digit Span Backward; CDT, Clock Drawing Test; TMT-A, Trail Making Test-A; TMT-B, Trail Making Test-B. asignificant difference between NC and aMCI group. bsignificant difference between NC and AD group. csignificant difference between aMCI and AD group.
Relationship of cognition and the levels of androgens and gonadotropins
Firstly, we found the decrease of androgen and the increase of gonadotropins were associated with cognitive decline in elderly men (Fig. 1). The results indicated that the levels of TT, FT, DHT, BT, and DHEA were positively correlated with global cognitive function, while the levels of FSH and LH were negatively correlated with them (Fig. 1). The correlative index of FT levels with the scores of MoCA and long delay free recall was 0.265 and 0.289, respectively, showing the highest correlation coefficient between them (Fig. 1). The results of multiple tests showed that the levels of FT and DHT were lower in the aMCI group and even lower in AD group compared with NC group. However, the levels of FSH and LH were increased in the AD group compared with the aMCI and NC groups (Fig. 2).

Correlation between the cognitive scores with the levels of androgen and gonadotropin in elderly men. Blank indicated that there was no correlation. A darker color indicates a stronger correlation between them.
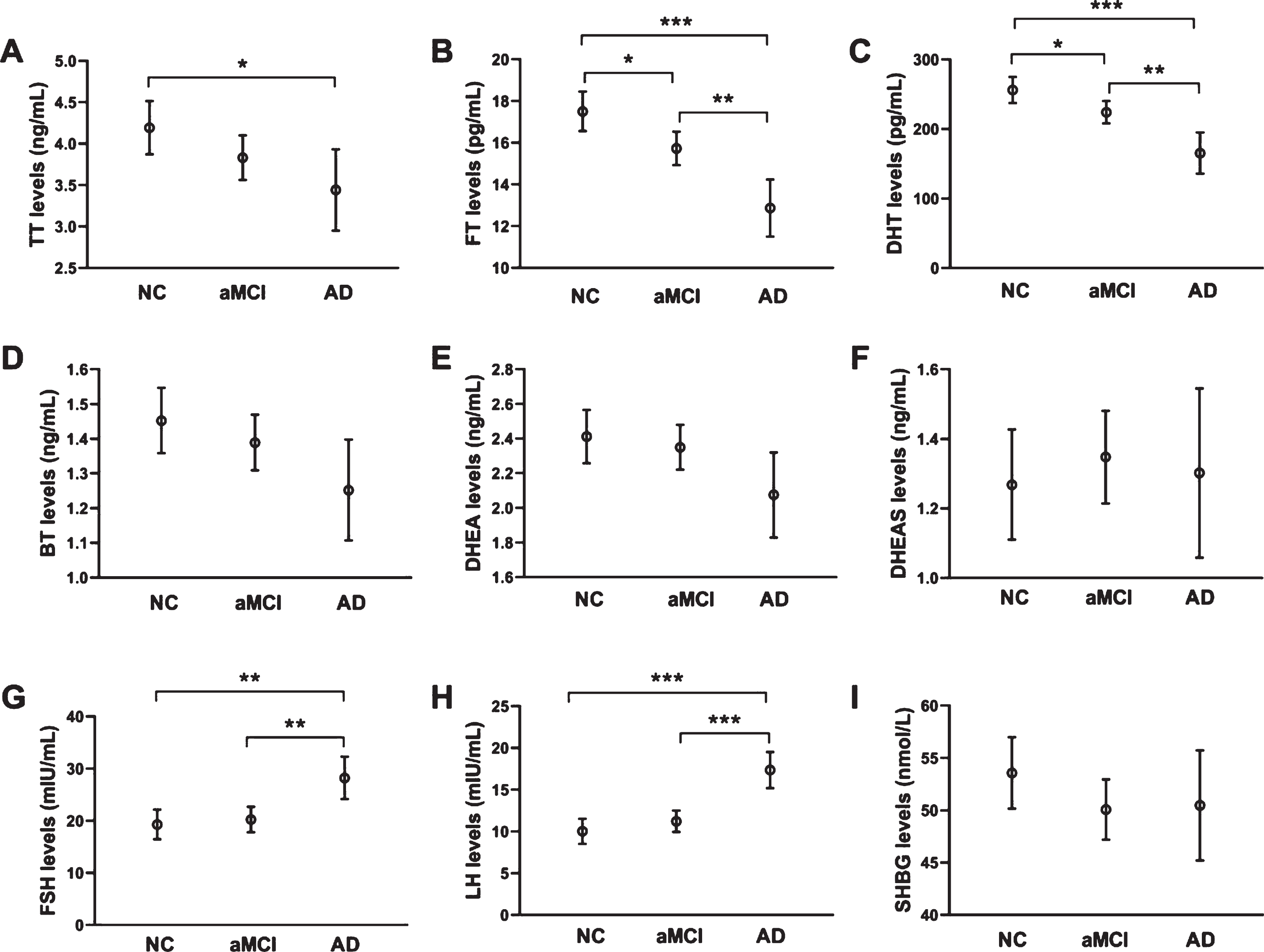
Multiple comparison of androgen, gonadotropin and SHBG among NC, aMCI, and AD groups. Error bars show 95% confidence intervals. Ages were controlled in the analysis of covariance. *p < 0.05, **p < 0.01, ***p < 0.001.
Lower levels of FT and DHT are risk factors for aMCI and AD
The risk of aMCI in the FT Q1 subgroup (with the lowest levels of FT) was 2.581 times higher than that in the FT Q4 subgroup (with the highest levels of FT) (OR = 2.581, p = 0.024). Meanwhile, the risk of aMCI in the DHT Q1 subgroup was 2.227 times higher than that in the DHT Q4 subgroup (OR = 2.227, p = 0.036) (Fig. 3A). These results suggested that the lower levels of FT and DHT were risk factors for aMCI. In addition, compared with the Q4 subgroup, the OR of AD and aMCI in Q1 subgroup for FT was 2.946 (p = 0.031), DHT was 3.541 (p = 0.018), BT was 2.760 (p = 0.033), and DHEA was 5.049 (p = 0.007). For LH, the risk of AD in the Q4 subgroup was higher than that in the Q1 subgroups (OR = 3.118, p = 0.019) (Fig. 3B). These results indicated that lower androgen and higher gonadotropin (LH) levels were risk factors in the process of aMCI converting to AD.
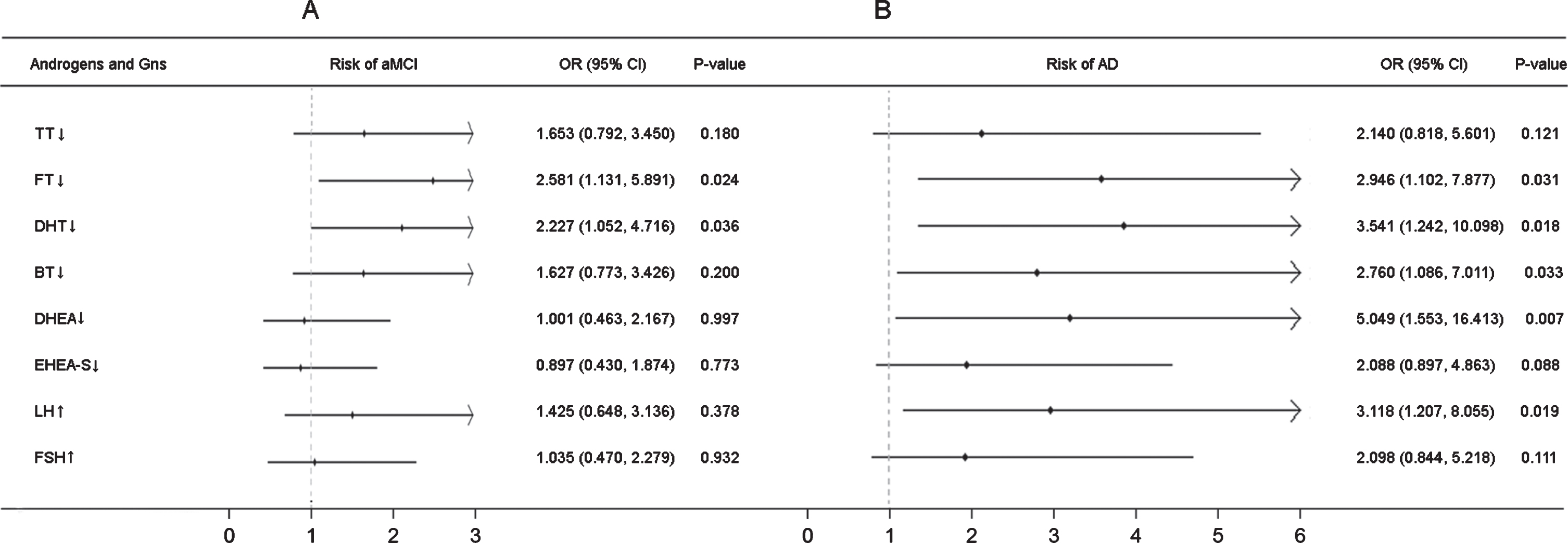
Effects of lower androgen and higher gonadotropin levels on the risk of aMCI and AD. Age, education, and APOE genetic polymorphism were controlled. A) OR values of TT, FT, DHT, BT, DHEA, and DHEA-S are odds ratio of aMCI and NC in Q1 group to that in Q4 group; OR value of FSH and LH are odds ratio of aMCI and NC in Q4 group to that in Q1 group. B) OR values of TT, FT, DHT, BT, DHEA, and DHEA-S are odds ratio of AD and aMCI in Q1 group to that in Q4 group; OR values of FSH and LH are odds ratio of AD and aMCI in Q4 group to that in Q1 group.
Interaction of androgens and APOE ɛ4 in cognition impairment
Non-carriers of APOE ɛ4 had higher scores of global cognitive function, memory function, and executive function compared with APOE ɛ4 carriers (Fig. 4). In the aMCI group, the OR of APOE ɛ4 carriers to non-carriers was 0.997 (p = 0.990); however, the proportion of APOE ɛ4 carriers was increased in the AD group (OR = 2.547, p = 0.003) (Table 2). After adjusting for age and education, the performance of MMSE and MoCA was affected by the interaction of androgens (FT and DHT) and APOE ɛ4 (Table 3). In APOE ɛ4 non-carriers, the scores of MMSE and MoCA were decreased in the FT Q1 subgroup, while in APOE ɛ4 carriers, besides the FT Q1 subgroup, the scores of Q2 and Q3 were all decreased compared with the FT Q4 subgroup (Fig. 5A, B). In APOE ɛ4 non-carriers, the scores of MMSE and MoCA were decreased in the DHT Q1 subgroup, whereas in APOE ɛ4 carriers, the scores in the DHT Q1 subgroup decreased more compared with the scores in the other subgroups (Fig. 5C, D). These results suggested that interaction of lower FT or DHT levels with APOE ɛ4 had a risk role in global cognitive impairment.
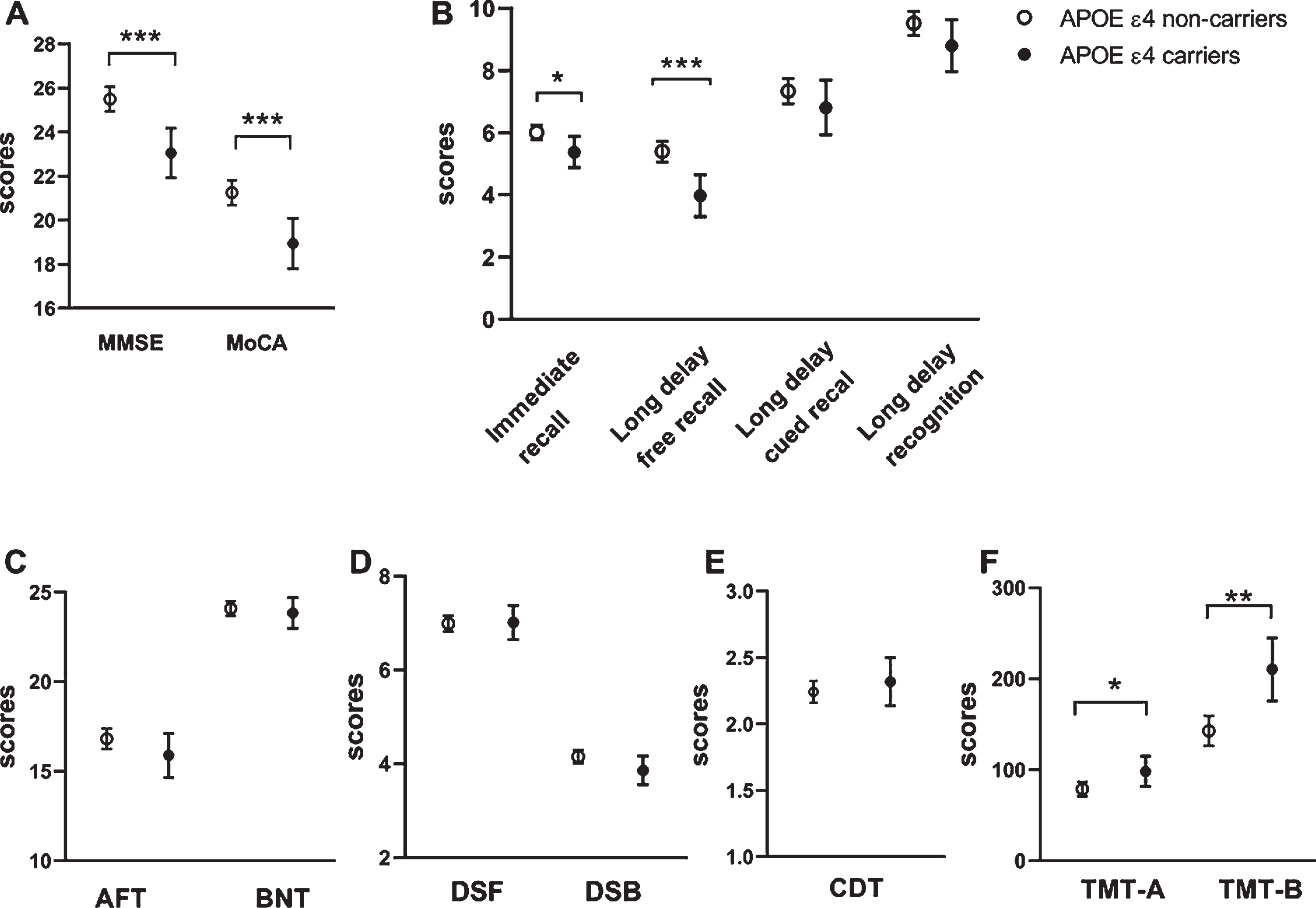
Comparisons of global cognitive function and five cognitive domains between APOE ɛ4 carriers and non-carriers. A) Global cognition function (MMSE and MoCA); B) Memory function (immediate recall, long delay free recall, long delay cued recall, and long delay recognition); C) language function (AFT and BNT); D) attention function (DSF and DSB); E) visuospatial function (CDT); F) Executive function (TMT-A and TMT-B). Error bars represent means (95% confidence intervals). Age and education level were controlled in the analysis of covariance. *p < 0.05, **p < 0.01, ***p < 0.001.
APOE ɛ4 allele is a risk factor for AD
OR, odds ratio; 95% CI: 95% confidence interval.
Interactive effects of FT and DHT with APOE ɛ4 on the cognition function in elderly men
The data were presented as mean±standard deviation. Age and education were controlled. FT, Q1: ≤11.74 pg/mL, Q2:11.75–15.69 pg/mL, Q3:15.70–19.88 pg/mL, Q4: >19.88 pg/mL. DHT, Q1: ≤157.58 pg/mL, Q2:157.59–208.24 pg/mL, Q3:208.25–290.94 pg/mL, Q4: >290.94 pg/mL.
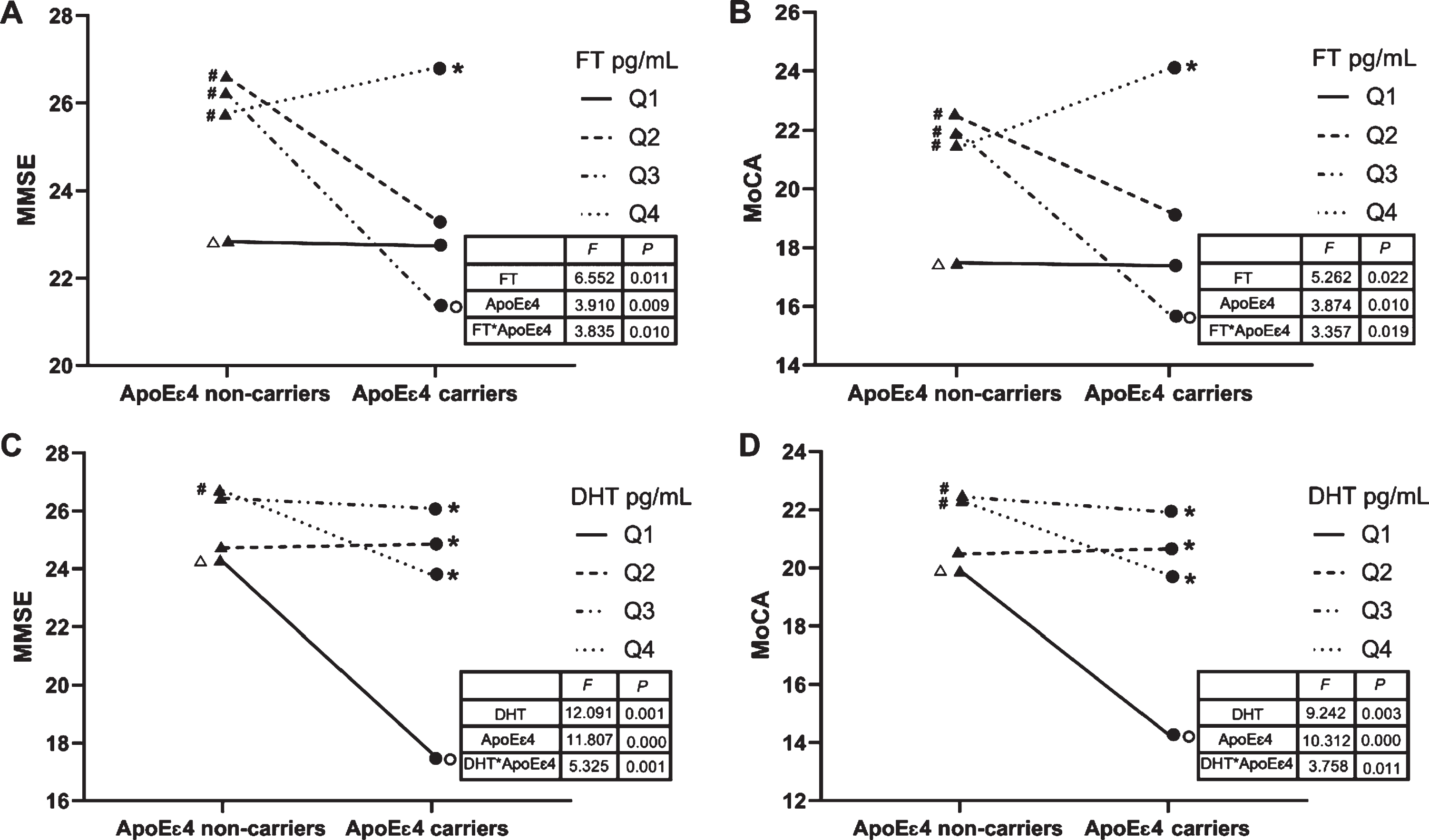
Interactive effects of lower FT or DHT levels with APOE ɛ4 on global cognitive function. A) Interactive effects between FT and APOE ɛ4 on the MMSE scores. B) Interactive effects between FT and APOE ɛ4 on the MoCA scores. C) Interactive effects between DHT and APOE ɛ4 on the MMSE scores. D) Interactive effects between DHT and APOE ɛ4 on the MoCA scores. Ages and education levels were controlled in the two-way ANOVA. #p < 0.05 compared with Δ. *p < 0.05 compared with 0.
The predictive value of the serum FT levels for aMCI diagnosis
Based on the results of univariate analysis (Table 1, Fig. 2), multiple logistic regression analysis was performed with age, education, FT and DHT as independent variables and with the cognition scores of NC and aMCI groups as the dependent variable. All variables, except for DHT, were included in the model. When the education period was ≥12 years, the MoCA scores were not linearly related to education status, and if the education period ≥12 years, it was calculated as 12 years. The equation obtained was Logit (P) = –1.660 + 0.070*age –0.210*education –0.074*FT (Table 4). Logit (P) was taken as the joint predictor variable L; after verification, L = –22.43 + 0.95*age –2.84*education –FT (65≤age, 0≤education≤12). The AUC value of FT ROC curve L was 0.745, and the cutoff value was 4.91, with the sensitivity and the specificity of 58.6% and 84.0%, respectively (Fig. 6A). The equation was subjected to external validation; the AUC value of FT ROC curve L’ was 0.712, with the sensitivity and the specificity of 61.3% and 81.5%, respectively, after verification of the cutoff value (Fig. 6B).
Multivariate logistic regression analysis of risk factors for aMCI
Multiple logistic regression analysis by stepwise method, cognitive scores of NC and aMCI group as dependent variables. FT, DHT, age, and education levels as covariates.
DISCUSSION
In this study, we found that: 1) lower androgen and higher gonadotropins levels are associated with pathogenesis of aMCI and AD; 2) the interaction of lower FT or DHT levels with APOE ɛ4 had a risk role in global cognitive impairment; and 3) peripheral blood FT levels had a predictive value for aMCI and might be a potential biomarker for prodromal AD.
Effects of androgens and gonadotropins on aMCI and AD
In current study, our results showed that TT, FT, DHT, DHEA, FSH, and LH were related to global cognitive function as reflected by MMSE and MoCA scores. In the AD patients, FT and DHT levels were lower, but the levels of FSH and LH were relatively higher, which were consistent with the previous findings [37, 38]. It was reported that FT has shown the strongest effect on cognition among all of the androgens [7, 39], and this was similar to our results. Further, our study found that lower levels of FT and DHT were risk factors for aMCI, and the risk of aMCI in the group with the lowest level of FT and DHT was twice that of the highest level group. These results indicated that lower levels of FT and DHT were sensitive indicators of aMCI and may have predictive value for identifying aMCI in elderly men. Studies have shown that FT and DHT can regulate the structure and function of the hippocampus [40] and alleviate mitochondrial dysfunction in AD [41]. Our previous studies also suggested that DHT treatment inhibited the progression of dementia in SAMP8 mice [42, 43]. In addition, lower levels of BT and DHEA and higher levels of LH are related to the increased prevalence of AD in elderly men. Most studies have reported that BT presents a lower risk of aMCI and AD in older men [44, 45]. The role of LH in AD is also supported by previous studies, which showed that higher levels of LH is a risk factor of AD in older men and play an important role in AD pathogenesis [15, 16].
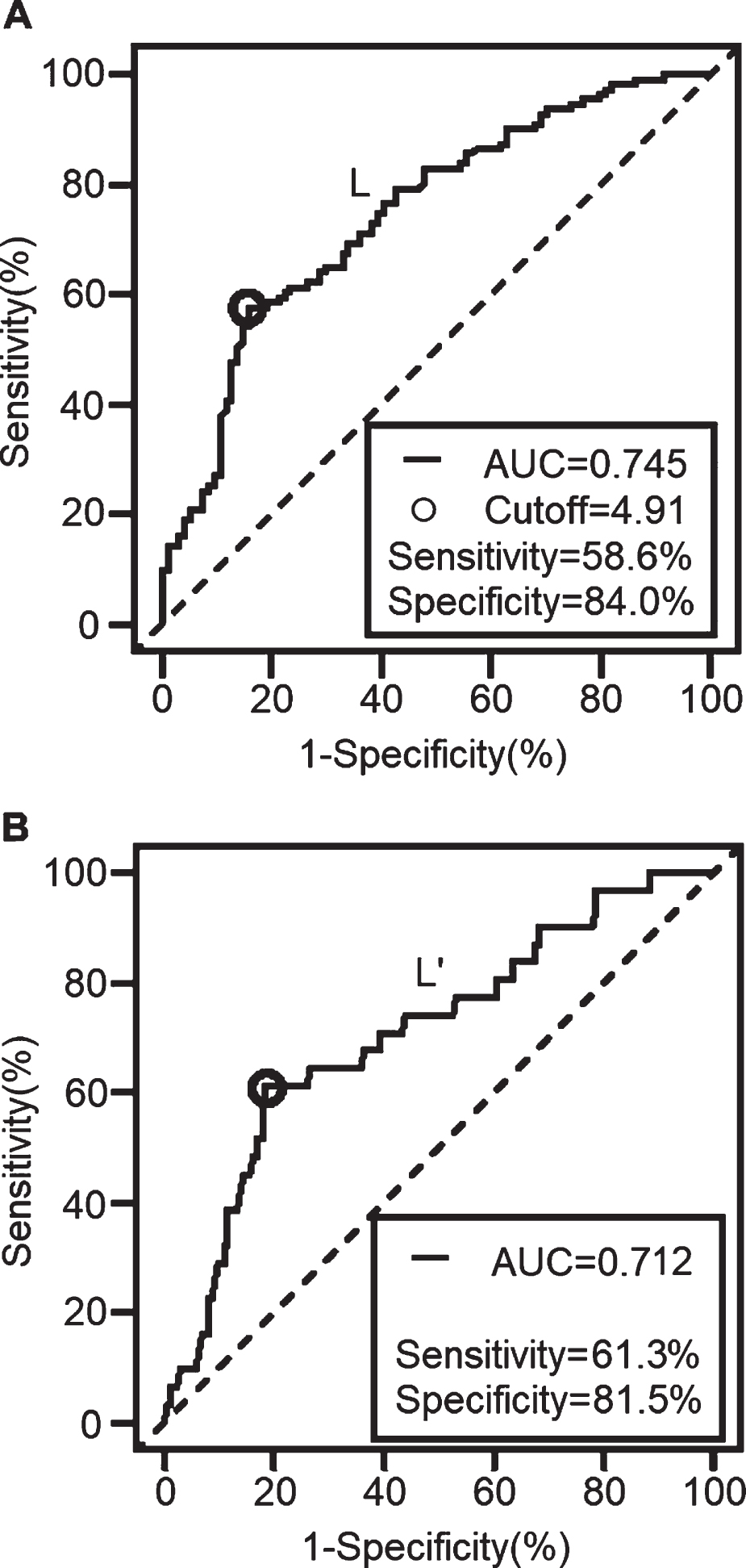
Receiver operating characteristic (ROC) analysis of FT for predicting aMCI. A) Fitting curve L: the model fitted by 70% of the subjects. B) Verification curve L’: the verification performed by 30% of the remaining subjects.
However, some studies have shown that low levels of androgen and high levels of gonadotropins are not risk factors for aMCI and AD. For instance, some researchers reported that neither FT nor gonadotropins showed a significant association with cerebral Aβ-positivity in males [17], the level of DHEA in peripheral blood was not associated with cognitive function in older men [46], and the cognition of older men with lower testosterone and age-associated memory impairment was not significantly improved by testosterone treatment compared with placebo subjects [47, 48]. The controversy of these results may be related to sample size, source of samples, identification technologies, limitations of neuropsychological scales, inadequate testing methods for sex hormones and confounding factors.
Interaction of lower levels of FT and DHT with APOE ɛ4 genotype on cognitive impairment
In our study, the rate of APOE ɛ4 allele carriers was higher in AD group, but no significant difference was found between the aMCI group and the NC group. This result supports the notion that APOE ɛ4 plays an important role in the acceleration of the conversion from aMCI to AD [20, 21]. Furthermore, APOE ɛ4 carriers showed impairment in overall cognition, memory, and executive function [49–51].
APOE ɛ4 inhibits the protection roles of androgens on the nervous system by down-regulating the synthesis of androgen [52] and the expression of androgen receptors [53], inhibiting the binding of androgen to its receptors [54], and reducing the anti-inflammatory effects of androgens [55]. Previous studies have reported that both APOE ɛ4 and androgens affect the progression of AD; however, their findings have been inconsistent [17, 56–58]. FT and DHT levels were sensitive indicators of cognitive impairment. To explore their interactive effects with APOE ɛ4 on cognitive impairment, we performed a two-way ANOVA for factorial analysis. The results showed that both FT and DHT interacted with APOE ɛ4 on global cognitive function. In APOE ɛ4 non-carriers, the level of FT was paralleled by cognitive performance; however, in APOE ɛ4 carriers, the protective effect of FT on cognition partially disappeared in subjects with medium FT levels. This result was consistent with Zhen and Reinvang’s findings [56, 57]. However, Panizzon and Lee showed different results from our study [17, 58]. In current study, DHT had protective effects on cognition, and elderly men with higher DHT levels in peripheral blood showed good global cognitive function in both APOE ɛ4 and non-APOE ɛ4 carriers. Furthermore, elderly male APOE ɛ4 carriers with the lowest DHT levels showed the worst cognitive function.
DHT is a specific androgen receptor (AR) agonist, which is affiliated more tightly with AR than testosterone (approximately 2 to 10 times that of testosterone). The major function of DHT is to regulate the transcription of target genes through the hormone-receptor-transcription pathway. The downstream gene of neprilysin (NEP) plays an important role in Aβ-degrading. Androgens promote the degradation of Aβ by the AR-mediated upregulation of NEP [59, 60]. Low concentrations of DHT in peripheral blood lead to an insufficient source of exogenous androgen in the central nervous system (CNS) and decreased AR binding, affecting the transcription of downstream target genes. In APOE ɛ4 carriers, the lack of DHT ligands, coupled with the restriction of receptor binding by APOE ɛ4, the transcription of target genes is more seriously inhibited, causing severe cognitive impairment and increasing the risk of AD.
After FT enters the CNS across the blood-brain barrier, it can be directly converted into DHT, alleviating AD pathology. It can also be aromatized to estrogen under the effect of P450 aromatase, activate the mitogen-activated protein kinase (MAPK) pathway, and upregulate α-secretase expression [61], which reduces Aβ production [62, 63]. Yaffe’s study found that estrogen had a protective effect on cognition in non-APOE ɛ4 carriers; however, the cognitive protection effect of estrogen disappeared in APOE ɛ4 carriers [64]. Burkhardt et al. found that FT levels are positively correlated with general cognition in non-APOE ɛ4 carriers and negatively correlated with executive function, working memory, and attention in APOE ɛ4 carriers [22]. Brown et al. found that FT is pro-inflammatory in APOE ɛ4 carriers [55]. These results are consistent with our finding that, in APOE ɛ4 allele carriers, FT is no longer a protective factor for cognition, even with a damaging effect.
The predictive value of serum levels of FT for aMCI and AD
Some studies have suggested that androgen and gonadotropins are potential biomarkers for screening AD [6, 65]. This study performed the ROC curve analysis for diagnosing aMCI in elderly men and conducted an external validation. The AUC values of L and L’ were both >0.7, indicating that the ROC curve was a moderate value for the diagnosis of aMCI. The cutoff value of L’ was 4.91, indicating that aMCI was considered when –22.43 + 0.95*age –2.84*education –FT≥4.91 and when FT≤0.95*age –2.84*education –27.34. For example, a 70-year-old man with 9 years of education would be considered aMCI when his peripheral blood FT level ≤13.6 pg/ml. It should be noted that its applicable age range is ≥65, and the education period over 12 years was calculated as 12 years. The AUC value of this prediction formula is with the medium value. Although the specificity of the cutoff value was good, the sensitivity was not very satisfied. This showed that, when FT level is used for the diagnosis of aMCI, it is necessary to combine it with other biomarkers, such as the value of Aβ and miRNA [66, 67]. Therefore, the combination of androgen and other biomarkers for the prediction of aMCI will be assessed in a future study.
In this study, the serum levels of androgen and gonadotropins were detected in the healthy population, aMCI and probable AD patients. The interaction effects of androgen and APOE ɛ4 on cognition were analyzed, and the cutoff value of androgen on the prediction of aMCI was explored. The results indicated that reduced androgen levels and increased gonadotropins levels were related to AD in elderly men. Serum FT levels may be used as a clinical biomarker to predict aMCI and AD in elderly population.
Advantages and limitations
This study has several advantages. Firstly, this is one of few studies to use experimental FT values to evaluate the relationship of androgens and cognitive impairment. Secondly, comprehensive testing of various androgens and their related gonadotropins could help to identify the potential biomarkers for aMCI or AD. Thirdly, we provided new clinical evidence of the interactive effects of androgen and APOE ɛ4 polymorphisms on AD in elderly men. The present study also involved several limitations. First, the cluster sampling method we applied led to a small sample size of probable AD. Second, neuroimaging of PET and cerebrospinal fluid examination was not performed. Third, using a single androgen as a potential biomarker of aMCI was relatively weak. In the future, we will combine other peripheral blood biomarkers (such as Aβ, miRNA) to improve the diagnostic value for aMCI or AD.
Conclusion
In summary, this cross-sectional study assessed the association of androgens and gonadotropins with the pathogenesis of aMCI and AD and investigated the interaction of androgens and APOE ɛ4 in cognitive impairment. Our results indicated that decreased FT and DHT and increased FSH and LH were associated with the pathogenesis of aMCI or AD in Chinese elderly men, and the interaction of androgen decline with APOE ɛ4 genotype play a role in this process. Serum FT levels have a predictive value for aMCI and might be a potential biomarker for prodromal AD. This study will help to understand the pathogenesis of aMCI and AD, and provide strategies for the prevention and treatment of AD.
Footnotes
ACKNOWLEDGMENTS
The authors sincerely thank all the subjects who participated in this study and the neurologist who helped us to identify the patients with aMCI or AD. This work was supported by the National Natural Science Foundation of China (91849134 and 31701047), the Natural Science Foundation of Hebei Province (H2018206361) and the Science and Technology Research Project of Higher Education Institutions in Hebei Province (BJ2017007).
The author has no conflict of interest to declare.