
Abstract
Background:
Instrumental activities of daily living (IADL) impairment can begin in mild cognitive impairment (MCI), and is the core criteria for diagnosing dementia in both Alzheimer’s (AD) and Parkinson’s (PD) diseases. The Functional Activities Questionnaire (FAQ) has high discriminative power for dementia and MCI in older age populations, but is influenced by demographic factors. It is currently unclear whether the FAQ is suitable for assessing cognitive-associated IADL in non-demented PD patients, as motor disorders may affect ratings.
Objective:
To compare IADL profiles in MCI patients with PD (PD-MCI) and AD (AD-MCI) and to verify the discriminative ability of the FAQ for MCI in patients with (PD-MCI) and without (AD-MCI) additional motor impairment.
Methods:
Data of 42 patients each of PD-MCI, AD-MCI, PD cognitively normal (PD-CN), and healthy controls (HC), matched according to age, gender, education, and global cognitive impairment were analyzed. ANCOVA and binary regressions were used to examine the relationship between the FAQ scores and groups. FAQ cut-offs for PD-MCI (versus PD-NC) and AD-MCI (versus HC) were separately identified using receiver operating characteristic analyses.
Results:
FAQ total score did not differentiate between MCI groups. PD-MCI subjects had greater difficulties with tax records and traveling while AD-MCI individuals were more impaired in managing finances and remembering appointments. Classification accuracy of the FAQ was good for diagnosing AD-MCI (69%, cut-off ≥1) compared to HC, and sufficient for differentiating PD-MCI (38.1%, cut-off ≥3) from PD-CN.
Conclusion:
The FAQ task profiles and classification accuracy differed between MCI related to PD and AD.
Keywords
INTRODUCTION
In both Alzheimer’s (AD) and Parkinson’s (PD) diseases, there is a spectrum of cognitive dysfunctions ranging from mild cognitive impairment (MCI) to dementia [1, 2]. MCI represents a prodromal stage of dementia in both diseases, and is defined as an undue decline from a premorbid cognitive level not normal for age but verified through cognitive testing, with preserved daily functioning [1–3]. In contrast, AD and PD dementia are characterized by a loss of independence indicated by problems with activities of daily living (ADL), in addition to cognitive decline. Although the presence of MCI is a risk factor for both types of dementia, not all MCI patients will develop dementia, as some individuals revert back to normal cognition or remain cognitively stable [4, 5]. Therefore, the investigation of factors associated with cognitive decline is crucial for identifying those MCI patients at a higher risk for developing dementia.
Research demonstrating the presence of ADL impairments in MCI is accumulating [6], specifically in complex instrumental activities of daily living (IADL), which include managing finances or using public transportation. These impairments in ADL emerge in the transition from MCI to dementia [7], and mild IADL changes can even be predictive of future cognitive decline [8]. Furthermore, there is increasing evidence for the presence of mild IADL impairment in AD-related amnestic MCI (AD-MCI) [9, 10], and individuals with AD-MCI and mild IADL deficits are at higher risk for progression to dementia [11, 12]. In PD-MCI, deficits in ADL function have also been shown to be related to worsening cognition and increased risk for PD dementia (PDD) in cross-sectional [13–18] as well as longitudinal studies [19]. However, assessing the impact of cognitive dysfunction on ADL is a challenge in PD, due to the interacting effect of motor impairment on daily function [14, 19–22]. Motor symptoms may therefore alter IADL function in PD-MCI differently than in AD-MCI [18, 23]. This highlights a need to examine both cognitive and motor influences on ADL to determine to which degree they contribute to deficits in both AD and PD. A better understanding of patients’ IADL characteristics, especially in the early stages of dementia, can facilitate personalized interventions in patients with different neurodegenerative disorders.
While IADL performance can aid in evaluating the progression of both PD and AD [24], previous research has mainly focused on the comparison of IADL impairment between AD dementia and PDD [14, 25–28]. Patients with PDD are characterized by a more severe progression of IADL dysfunction over time than AD dementia patients [28]. Importantly, motor disability was shown to be a significant contributor to IADL impairment in PDD, highlighting its role as a confounder [29]. However, a notable limitation of these studies is that patient groups were not matched for age, gender, ethnicity, or severity of cognitive impairment [28, 31]. One study controlling for these factors by comparing homogeneous patient groups with AD dementia and PDD was not able to detect differences in overall severity of IADL dysfunction, but identified different behavior and error profiles associated with this impairment in both groups [25].
Little is known about differences or similarities of the IADL profiles associated with MCI in AD and PD. One of the earliest IADL changes in AD-MCI may be the ability to manage finances [8], while difficulties remembering appointments was often the most impaired IADL [6]. These two activities best discriminated between cognitively normal and MCI patients [7]. Financial abilities have also been shown to be impaired in PD-MCI patients [17]. Moreover, keeping appointments, following recent events, managing finances, and using a telephone were specific ADL items that were unaffected by motor dysfunction, but able to identify PDD [14]. Only a few studies have evaluated IADL function in the prodromal dementia stage in AD and PD, reporting no differences in overall severity of IADL impairment between AD-MCI and PD-MCI [30, 32].
The focus of this study was therefore to explore the ADL profiles associated with the prodromal stage of AD and PD patients, as both of these neurodegenerative diseases have a well-characterized MCI stage. IADL dysfunction in AD is driven by memory impairment, which is a specific diagnostic feature occurring early in the disease. Therefore, items evaluating memory loss in everyday function might be more sensitive for assessing IADL within the frame of AD than for other diseases that have a more heterogenic profile of cognitive impairment in the prodromal stage of dementia, such as PD-MCI [33]. First, we aimed to investigate the association between cognitive dysfunction in the context of AD and PD and impairment on IADL using the Functional Activities Questionnaire (FAQ) [34]. In line with previous studies, we hypothesized that either AD-MCI and PD-MCI patients would demonstrate a similar overall degree of IADL dysfunctions assessed by the FAQ total score [30, 32], or patients with PD-MCI would score higher than AD-MCI, primarily due to the influence of motor performance in PD. Secondly, we aimed to specifically compare the task-related IADL profiles between AD-MCI and PD-MCI as, to the best of our knowledge, this comparison has not yet been performed. We hypothesized that both groups would be impaired in financial activities, with AD-MCI performing worse on items associated with memory impairment and PD-MCI showing more impairment in items related to non-memory domains, as well as tasks more prone to be affected by motor impairment. Lastly, we aimed to compare diagnostic merits of the FAQ for MCI due to AD and PD. The FAQ demonstrates good discriminative abilities in terms of distinguishing normal individuals and those with cognitive decline [34]. Therefore, we hypothesize that FAQ would have similar discriminant power for detecting IADL dysfunction in AD-MCI and PD-MCI patients, with a suspected higher cut-off for PD-MCI patients due to the potential influence of motor impairment.
METHODS
Study design and participants
Data used in the preparation of this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu), and from the “Amyloid-Beta in cerebrospinal spinal fluid as a risk factor for cognitive dysfunction in Parkinson’s Disease (ABC-PD)” study carried out at the University of Tübingen [18]. In the present analysis, the following groups were studied: individuals with AD-MCI and healthy controls (HC) from the ADNI study, and PD-MCI and cognitively normal PD patients (PD-CN) from the ABC-PD study.
The ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The primary goal of ADNI has been to test whether serial magnetic resonance imaging (MRI), positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of MCI and early AD. Inclusion criteria, and study protocols for ADNI patients are reported at http://www.adni-info.org/Scientists/ADNIStudyProcedures.aspx. Respective criteria for the ABC-PD study have been described elsewhere [18]; in brief, PD patients between 50 and 85 years without a diagnosis of PDD or concomitant diseases affecting cognition were recruited. Data for the ABC-PD study were collected and subsequently managed using REDCap [35] hosted by the Hertie Institute for Clinical Brain Research.
Following the ADNI classification criteria, subjects with subjective and caregiver-rated memory complaints, confirmed through neuropsychological memory assessments, as well as a Clinical Dementia Rating Scale (CDR) [36] memory score of 0.5, were classified as AD-MCI. Patients were defined as HC if they had: 1) no significant memory complaints beyond those expected for age, 2) normal memory and global cognitive function, 3) no significant IADL dysfunction indicative for AD (CDR memory = 0), and 4) no cerebrospinal fluid (CSF) amyloid-beta 1–42 (Aβ1–42) burden, (≥980 pg/ml, the Roche Elecsys amyloid-beta 1–42 immunoassay). Diagnosis of PD-MCI was made in accordance with the Level-II recommendations of the Movement Disorder Society Task Force [1]. Criteria included: 1) presence of subjective cognitive decline, 2) cognitive impairment defined as test scores 1.5 standard deviations below the normative mean in at least two neuropsychological tests, and 3) preserved IADL assessed using a validated German version of the Pill-Questionnaire (normal IADL function, score = 0) [37]. If patients did not meet these criteria, they were classified as PD-CN. Details about the neuropsychological assessments and domains for both studies can be found in Supplementary Table 1. Only patients in the PD-CN group with normal CSF Aβ1–42 levels (≥600 pg/ml, the Innotest/Fujirebio amyloid-beta 1–42 solid phase enzyme immunoassay) were analyzed.
All participants scored above 24 points on the Mini-Mental State Examination (MMSE) [38], and had no indication of major depression assessed by the Geriatric Depression Scale (GDS) [39] (score <6 points) and/or the Beck Depression Inventory-II (BDI-II) [40] (score <20 points). To avoid confounding effects of demographic characteristics and global cognitive state, data of a selected sample were analyzed. AD-MCI and PD-MCI subjects were matched one-by-individually according to sex, age (±2 years), education status, and MMSE score (±2 points), except for one pair where the difference in MMSE scores was 3 points (25 to 28 points). Additionally, HC and PD-CN subjects were selected that were similar in age, sex, and education to the corresponding MCI groups. Out of 195 ADNI participants (62 HC and 133 AD-MCI) and 145 PD patients (72 PD-CN and 73 PD-MCI) meeting inclusion and exclusion criteria for analysis, 42 matched pairs were generated.
Assessments
Demographic characteristics considered in the present analysis included age, gender, marital, and education status, as well as age at onset and disease duration for PD patients. Global cognitive state and mild signs of depression were assessed using the MMSE and the GDS, respectively. Additionally, daily dose of all antiparkinsonian medication taken by PD patients was expressed using the levodopa equivalent daily dose (LEDD) [41]. The Unified Parkinson’s Disease Rating Scale Part III (UPDRS-III) [42] and Hoehn & Yahr Staging [43] were used to assess motor impairment in PD patients.
IADL impairment was measured by the FAQ [34], which consists of 10 items corresponding to complex daily tasks such as handling finances, preparing meals, shopping, remembering appointments, and traveling out of house. The ability to perform each item is rated, usually by an informant, from 0 to 3 (0 = normal or never did but could do now, 1 =has difficulty but does by self or never did but would have difficulty now, 2 = requires assistance, 3 = dependent), with a maximum impairment score of 30 points. The FAQ was administered as an interview to informants in the ADNI cohort, whereas it was administered as a questionnaire that was filled out by an informant or by the patient themselves when no informant was available in the ABC-PD cohort.
Statistical analyses
Statistical analyses were carried out using IBM SPSS version 25 (SPSS Inc., Chicago, IL, USA). All α levels were set at 0.05. Assumptions of normality were tested with Shapiro-Wilk tests. There were no missing data. Demographic and clinical variables for all groups were assessed using Chi-squared tests for categorical variables, ANOVA with post-hoc Tukey’s HSD tests for parametric variables, and independent samples, Kruskal-Wallis test with post hoc Dunn’s pairwise tests (Bonferroni corrected) where appropriate. For PD characteristic analyses, Chi-squared tests for categorical variables, t-tests for parametric and Mann-Whitney U tests for non-parametric variables were conducted. Furthermore, as the FAQ has been shown to be influenced by the type of informant [44], a chi square test was conducted to evaluate the distribution of type of informant (self-report versus informant) in patients with PD. For all further analyses, age was included as a covariate, as a previous study [45] found an association between the FAQ and age. Based on the between-group analyses, demographic variables differentiating between study groups were included in further analyses as covariates, as reported below.
Between-group analysis of covariance (ANCOVA) models with post-hoc Bonferroni tests examined the relationship between the dependent FAQ total score and both group and informant status as independent variables, with significant demographic characteristics as covariates (age, GDS, education status). The interaction term between the two independent variables was calculated for all models, with the exception of Model 3 where the distribution of informant status over study groups did not allow for an interaction term to be built. In model 1, group classification was used as the independent variable. A second model examined the presence of cognitive impairment; model 2a examined cognitive impairment (PD-MCI and AD-MCI) versus no cognitive impairment (PD-CN and HC) groups. The same analysis was conducted only for the PD group in model 2b, with the UPDRS-III score as an additional covariate, to examine the influence of cognition in a purely motor disorder. In the third model, study groups were divided according to their diagnosis (PD-CN and PD-MCI versus HC and AD-MCI) to determine the effect of the presence of motor impairment, with the MMSE score as an additional covariate.
To predict classification of subjects into AD-MCI or PD-MCI, a binary logistic regression was conducted using all FAQ items, with age as a covariate. A receiver operating characteristic (ROC) analysis was conducted to define the diagnostic accuracy of the FAQ total score for both AD-MCI and PD-MCI diagnoses by means of sensitivity and specificity. Classification accuracy of the FAQ was judged based on the area under curve (AUC) as follows: 0.9–1.0 excellent, 0.8–0.9 very good, 0.7–0.8 good, 0.6–0.7 sufficient, 0.5–0.6 bad, <0.5 test not useful [46]. The optimal cut-off score for each disease group was defined by the highest Youden’s Index (sevitivity+specificity-1). Frequency of subjects in each study group with FAQ scores above the cut-off was compared using a Chi-squared test.
RESULTS
Demographics
Post-hoc Dunn’s comparisons showed that AD-MCI and PD-MCI groups had lower MMSE (p < 0.001 for both) and GDS scores (p = 0.003, p = 0.04, respectively) than HC subjects, indicating more severe cognitive impairment and greater depressive symptoms (see Table 1). Demographical variables, global cognitive impairment, and severity of depression did not statistically differ between AD-MCI and PD-MCI patients. AD-MCI patients had lower MMSE scores than PD-CN patients (post-hoc p = 0.02). PD-MCI patients had lower global cognition levels assessed using the MMSE (post-hoc p = 0.002) and more severe motor staging, based on the Hoehn and Yahr scale, than PD-CN. Results of the Chi-square test for education between groups were significant, with more PD-CN patients having obtained a non-university level degree, and more HC patients having achieved university-level degree than both MCI groups. The distribution of the type of FAQ informant (self-report versus informant) was not significantly different between the PD groups (χ2(1,84) = 0.76, p = 0.51).
Demographic and clinical characteristics of the population
Unless otherwise indicated, results are expressed as Median (range), †Data of one person could not be assessed, ††between-group analyses not conducted as variables are used in further comprehensive analyses. ADL, Activities of Daily Living; AD-MCI, Alzheimer’s disease-related amnestic mild cognitive impairment; FAQ, Functional Activities Questionnaire; HC, healthy controls; GDS, Geriatric Depression Scale; LEDD, Levodopa equivalent daily dose; MMSE, Mini-Mental State Exam; PD, Parkinson’s disease, PD-CN, Parkinson’s disease normal cognition; PD-MCI, Parkinson’s disease with mild cognitive impairment; SD, standard deviation; UPDRS-III, Unified Parkinson’s Disease Rating Scale III. Post hoc tests were significant between: aHC and AD-MCI, bHC and PD-MCI, cPD-CN and AD-MCI, dPD-CN and PD-MCI. *p < 0.05.
Group comparison of FAQ total score
Results of the ANCOVA models are reported in Table 2. The analysis of all groups (Model 1) showed that group status was significant, after controlling for all covariates. Post-hoc Bonferroni tests showed that HC patients had lower FAQ total scores than AD-MCI (mean difference, MD = –3.16, p < 0.001) and PD-MCI (MD = –2.43, p = 0.002) patients. PD-CN patients also had lower FAQ total scores than AD-MCI (MD = –2.57, p = 0.01) and PD-MCI (MD = –1.84, p = 0.04) patients. Both control groups (HC and PD-CN) did not differ in their FAQ scores, nor did the MCI (AD-MCI and PD-MCI) groups. Among covariates only age was a significant predictor of the FAQ total score, with increasing age leading to higher FAQ scores (t = 2.93).
Analysis of covariance models for the Functional Activities Questionnaire total score and cognitive status
AD-MCI, Alzheimer’s disease-related amnestic mild cognitive impairment; HC, Healthy controls; GDS, Geriatric Depression Scale; IV, independent variable; MMSE, Mini-Mental State Exam; PD, Parkinson’s disease; PD-CN, Parkinson’s disease normal cognition; PD-MCI, Parkinson’s disease with mild cognitive impairment; UPDRS-III, Unified Parkinson’s Disease Raring Scale III. Post hoc tests were significant between: aHC and AD-MCI. bHC and PD-MCI. cPD-CN and AD-MCI. dPD-CN and PD-MCI. *p < 0.05.
Evaluation of task-related IADL profile
A binary logistic regression analysis was conducted to predict classification of subjects into AD-MCI or PD-MCI, including all FAQ items as predictors, and age as covariate (χ2 = 41.85, p < 0.001 with df = 11) (see Table 3). FAQ items 1 (handling finances), 2 (assembling taxes), 9 (remembering occasions), and 10 (traveling out of house) significantly discriminated between both patient groups. AD-MCI subjects reported higher degrees of impairment on items 1 (p = 0.01) and 9 (p = 0.03), whereas PD-MCI patients had more problems relating to items 2 (p = 0.02) and 10 (p = 0.04). For item 2, 28.6% of patients in both groups scored ≥1 point, while 7 (16.7%) PD-MCI patients compared to only 4 (9.5%) of AD-MCI patients scored ≥2 points.
Results of the binary logistic regression analysis including all FAQ items between AD-MCI and PD-MCI patients
Unless otherwise indicated, results are expressed as Number of patients scoring≥1 (%). AD-MCI, Alzheimer’s disease-related amnestic mild cognitive impairment; B, unstandardized beta; CI, confidence interval; FAQ, Functional Activities Questionnaire; OR, odds ratio; PD-MCI, Parkinson’s disease with mild cognitive impairment; SD, standard deviation. *p < 0.05.
Influence of cognition and motor performance on FAQ scores
In ANCOVA model 2a (Table 2), the groups with MCI had significantly higher FAQ total scores than the groups without cognitive impairment (MD =–2.13, p < 0.001). Independent of this between-group effect, higher age explained a higher FAQ total score (t = 2.86). The analysis was repeated in the PD subsample, additionally controlling for motor severity using the UPDRS-III (model 2b). In this model, PD-MCI patients had significantly higher FAQ total scores than PD-CN patients (MD = –1.56, p = 0.007), with higher GDS scores independently associated with higher FAQ total scores (t = 2.25). Additionally, there was a significant effect of type of informant, with informants reporting higher FAQ scores than patients (MD = –1.28, p = 0.02). Results of ANCOVA model 3 showed that diagnosis of PD per se, comprising both patients with PD-CN and PD-MCI, did not have a significant impact on the FAQ total score compared to the group containing HC and AD-MCI patients. The inclusion of the MMSE as an additional covariate confirmed that lower global cognitive status was associated with higher FAQ total scores (t = –4.14).
Classification accuracy for AD-MCI and PD-MCI according to FAQ scores
Figure 1 shows the ROC curves of the FAQ total score for diagnosis of MCI in both AD and PD, comparing MCI versus controls for each respective cohort. For classifying AD-MCI, an optimal FAQ cut-off score ≥1 was defined, showing a sensitivity and specificity of 69% and 90.5%, respectively. The optimal cut-off of the FAQ total score for distinguishing PD-MCI from PD-CN was ≥3 points. While the sensitivity of PD-MCI diagnosis was low (38.1%), specificity was excellent (92.9%). In addition, 9.5% of the HC and 7.1% of the PD-CN group scored above the pre-defined group cut-offs. An overview of diagnostic parameters, including the likelihood ratios, is displayed in Table 4.
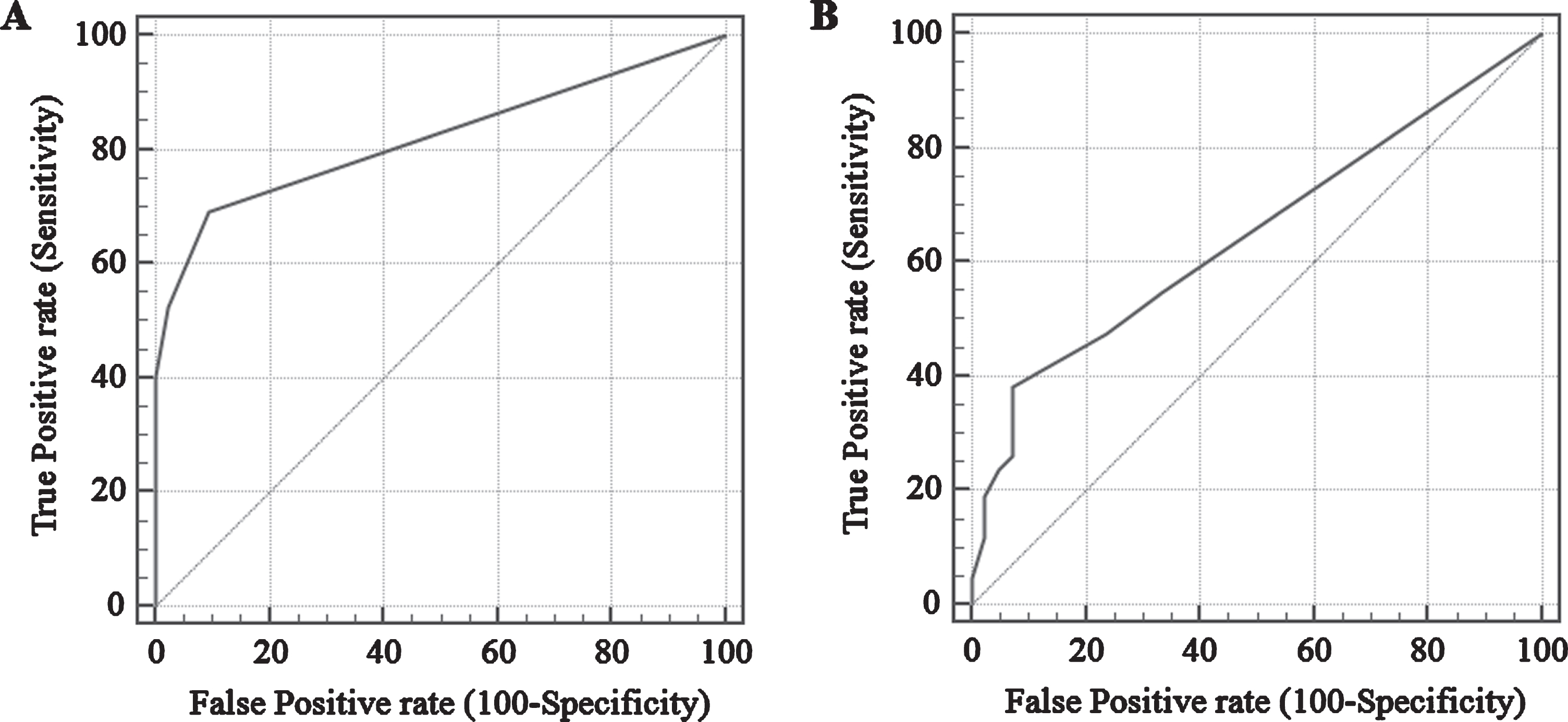
ROC curves of the FAQ total score for (A) HC versus AD-MCI and (B) PD-CN versus PD-MCI, including sensitivity and specificity.
Diagnostic values of the FAQ total score for differentiating HC from AD-MCI and PD-CN from PD-MCI
AD-MCI, Alzheimer’s disease-related amnestic mild cognitive impairment; AUC, area under the Curve; CI, confidence interval; HC, healthy controls; FAQ, Functional Activities Questionnaire; PD-CN, Parkinson’s disease normal cognition; PD-MCI, Parkinson’s disease with mild cognitive impairment. *p < 0.05
DISCUSSION
This study explored IADL profiles associated with MCI in AD and PD. The present data analyses revealed no significant differences in global functional impairment expressed by the FAQ total score between AD-MCI and PD-MCI. However, task-related IADL profiles were different between the MCI groups. Most importantly, the number of patients with IADL impairment according to the calculated disease-specific cut-offs was nearly twice as high in AD-MCI (69.0%) as in PD-MCI (38.1%).
Our results support the hypothesis that severity of IADL impairment assessed by the FAQ total score does not differentiate between AD-MCI and PD-MCI patients when matched for global cognitive status, gender, age, and education. This is in accordance with previous research reporting no difference in IADL scores between amnestic MCI and PD-MCI [30, 32], or between AD and PDD patients when comparing overall performance-based ADL functioning [25]. In contrast to these reports, Farlow and colleagues [28] reported higher ADL impairment referring to both basic ADL and IADL tasks in PDD compared to AD. However, their study groups were not matched according to the level of global cognitive impairment, which was shown in our sample to have a strong influence on the severity of ADL impairment. Our findings highlight the importance of matching groups to avoid confounding effects, to accurately compare IADL profiles in different diseases.
The present analyses revealed differences in task-related IADL impairment between the MCI groups. We had hypothesized that both groups will be impaired in financial activities, with AD-MCI performing worse on remembering appointments and PD-MCI showing more impairment on tasks prone to be affected by motor impairment. Our results showed AD-MCI patients were more impaired than PD-MCI patients in IADL related to memory (remembering appointments), and handling finances, reflecting complex skills in major life areas and interpersonal interactions [7, 11]. Interestingly, patients with PD-MCI showed more problems with assembling taxes than AD-MCI patients. Previous studies have shown that impairment in assembling tax records distinguishes HC from AD-MCI patients [7], while handling finances are impaired in PD-MCI compared to PD-CN patients [17]; these findings were reversed in our results. It is possible that general financial capabilities are impaired with increasing cognitive deficits, regardless of the underlying neurodegenerative disease. We also cannot rule out that there are cultural differences between the US and Germany affecting financial and tax abilities that may affect our cohorts. However, previous studies in AD patients have shown that the FAQ item handling finances predicted progression from HC to AD-MCI and from MCI to AD dementia [7, 47]. This item may be of more value as a prognostic factor, than a differentiating factor. Moreover, more PD-MCI patients required assistance or were dependent on another person for assembling tax records. It has been previously postulated that assembling tax records is a complex task that involves executive functioning [7]. These executive functions contribute to ADL deficits, which are affected early in the disease course of PD [48, 49], possibly translating into a poorer ability to manage tax records. Future studies should examine associations between cognitive domains and the individual FAQ items.
PD-MCI patients also showed greater problems with mobility, which has been reported to be impaired in PD patients (walking in neighborhood, going by car, going by bus, driving a car) [50], and is one of the earliest deficits able to differentiate between pre-diagnostic PD and controls [51]. While our ANCOVA analysis showed that global cognitive functioning, and not motor severity, was the primary predictor of the FAQ, an influence of motor impairment cannot be excluded. It should also be noted that informants rated ADL dysfunction higher than PD patients did, which has been shown in previous studies where PD patients were shown to rate themselves as less impaired on measures of ADL than their caregivers [37, 52–54]. However, the interaction term between PD cognitive group and informant status was not significant, suggesting distribution across the groups was the same. It cannot be ruled out that some over-reporting of ADL dysfunction may have still occurred, as both patients and informants may have rated based on motor abilities instead of cognitive function. As other studies have been unable to verify this effect [55, 56], future studies should examine how informant ratings in PD reflect cognition or motor impairments.
All AD-MCI subjects had amnestic cognitive impairment, in accordance with the ADNI inclusion criteria. In AD, amnestic multi-domain MCI is usually found to be the most affected subtype on a functional level [57–59], and varying MCI subtypes differ in their profile of IADL impairment [58, 61]. To date, little is known about functional levels among subtypes of patients with PD-MCI, which can be classified as both amnestic and non-amnestic multi-domain MCI, the latter of which is probably associated with more marked executive dysfunction [62]. Compared to AD-related MCI, PD-MCI seems to be associated with more pronounced attentional and visuo-constructive deficits [32, 62]. Moreover, attention and language skills have been identified to be related to both IADL impairment and diagnosis of dementia in PD [63–65]. Therefore, we hypothesize that the differences in IADL task profiles of AD-MCI and PD-MCI can be explained by different cognitive deficit patterns that are associated with AD and PD, respectively.
As the FAQ is a measure originally conceptualized to detect functional dependence in normal aging and mild dementia, it may be more heavily weighted towards memory-dependent IADL [33]. In our sample, the discriminant ability of the FAQ for AD-MCI was good compared to controls, but the suggested cut-off (≥1 points) might overestimate IADL impairment in MCI. Previous studies demonstrated good diagnostic accuracy values of the FAQ for screening cognitive decline within AD [33, 67] and suggest a cut-off value of 1 for differentiating normal cognition from MCI or dementia [66], similar to our findings. For PD, we found an FAQ cut-off value ≥3 to distinguish cognitively impaired patients, with sensitivity and specificity of 38.1% and 92.9%, respectively. This is lower than the cut-off found in a previous study for differentiating between PD patients with normal cognition and those with PD-MCI or PDD [23]. Their cut-off of 3.5 had a sensitivity of 47.4% and specificity of 88.1%; however, it should be noted that the authors applied a shortened 8-item version of the FAQ where items 5 and 6 were found to be influenced by motor impairment and were therefore excluded [23]. The total 10-item FAQ score, which we used in our analyses, may thus not be comparable with the cut-off values reported previously.
Differences in cut-offs and previous reports of the discriminative ability of the FAQ for MCI might be at least partly caused by the high prevalence of MCI (50%) and the comparison of individuals matched for social-demographic and global cognitive status. As our intention was to compare the discriminative abilities of the FAQ for MCI in individuals with and without additional motor impairment like PD, our analysis might be not valid for the clinical diagnosis in a more heterogenic population. A solution might be incorporating Aβ1–42 status as a biomarker when defining MCI [68], to make sure that AD pathologic change underlies AD-MCI. Low Aβ1–42 values have also been identified as a potential risk marker for a more rapid disease course in PD [69, 70], but the predictive value of a dichotomized abnormal (low) Aβ1–42 value is still under discussion. To compare both MCI groups according their diagnostic criteria, we therefore decided to use the clinical consensus criteria, excluding additional information gained by adding biomarkers. Future studies should aim to validate cut-offs for AD-MCI, as well as define accurate cut-offs for PD-MCI that take into account motor influences on ADL function.
The lower classification accuracy of the FAQ for our PD-MCI sample might be explained by the fact that only a subgroup of patients presented with IADL problems (38.1% compared to 69% of AD-MCI). These results are in accordance with the literature, showing a similar prevalence of mild IADL impairment among PD-MCI patients [13, 71]. In line with previous research [45], the present study also confirms that age is positively associated with IADL impairment when measured by the FAQ. For future research, we suggest developing separate normative standards for IADL impairments within PD-MCI, while also correcting for age effects.
This study faces some limitations. First, despite controlling for PD-specific motor impairment, we were not able to completely exclude this influence on the FAQ ratings. Second, the matched groups comprised only 42 participants each; however, we identified a distinct IADL profile in our homogenous MCI groups despite low sample size. Future studies in larger samples are needed to confirm our findings and to monitor change in IADL profiles over time in disease-specific MCI groups. For the identification of first symptoms of IADL impairment in PD, more sensitive assessments, such as performance-based tests or scales targeting the assessment of more complex IADL tasks, should be evaluated. It should also be noted that, due to the uneven distribution of informant ratings across the groups, the null effects of the interaction term (Informant Status x Group) in the ANOVA analyses should be interpreted with caution. Lastly, it must be noted that cross-cultural differences may have contributed to between-group differences. While little research has examined cultural and racial differences in the context of dementia, a recent study was not able to detect an ADL item bias across data from eight Western countries [72]. Therefore, we do not conclude that our differences are influenced by culture, although we cannot completely rule this out.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank all patients for their participation.
This work was supported by an unrestricted grant from Janssen Research and Development, a division of Janssen Pharmaceutica N.V. The funding of the ABC-PD study is pre-competitive.
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.