
Abstract
Background:
The driving behavior of patients with mild Alzheimer’s disease dementia (ADD) and patients with mild cognitive impairment (MCI) is frequently characterized by errors. A genetic factor affecting cognition is apolipoprotein E4 (APOE4), with carriers of APOE4 showing greater episodic memory impairment than non-carriers. However, differences in the driving performance of the two groups have not been investigated.
Objective:
To compare driving performance in APOE4 carriers and matched non-carriers.
Methods:
Fourteen APOE4 carriers and 14 non-carriers with amnestic MCI or mild ADD underwent detailed medical and neuropsychological assessment and participated in a driving simulation experiment, involving driving in moderate and high traffic volume in a rural environment. Driving measures were speed, lateral position, headway distance and their SDs, and reaction time. APOE was genotyped through plasma samples.
Results:
Mixed two-way ANOVAs examining traffic volume and APOE4 status showed a significant effect of traffic volume on all driving variables, but a significant effect of APOE4 on speed variability only. APOE4 carriers were less variable in their speed than non-carriers; this remained significant after a Bonferroni correction. To further examine variability in the driving performance, coefficients of variation (COV) were computed. Larger headway distance COV and smaller lateral position COV were observed in high compared to moderate traffic. APOE4 carriers had smaller speed COV compared to non-carriers.
Conclusion:
The lower speed variability of APOE4 carriers in the absence of neuropsychological test differences indicates reduced speed adaptations, possibly as a compensatory strategy. Simulated driving may be a sensitive method for detecting performance differences in the absence of cognitive differences.
INTRODUCTION
According to recent epidemiological data from the European Union, older persons are 1.4 times more likely to suffer fatal injuries in motor vehicle accidents. As the percentage of persons of advanced age increases in society, so does the number of older licensed drivers [1]. Driving constitutes a multifactorial process, combining demands on sensory, physical, and cognitive functions—namely visual attention, visual perception, executive functions, and memory [2].
Alzheimer’s disease dementia (ADD) is the most prevalent neurodegenerative disorder and the main cause of major neurocognitive dysfunction worldwide. A number of researchers have demonstrated that ADD adversely affects driving performance. During the mild stages of the disease patients with ADD seem to maintain their basic driving skills, although driving errors are prominent in such patients [3]. Among the most critical driving performance characteristics of patients with ADD are low average speed [4], slow reaction time [5], and high accident probability [6]. In addition, some studies suggest that patients with ADD make lane violations [3], maintain a greater headway distance [7], and have orientation difficulties, with increased possibilities of getting lost [4].
Mild cognitive impairment (MCI) is a clinical dia-gnostic entity that applies to 16–20%of the general population above the age of 65 and is considered to be a preclinical stage of dementia, most commonly ADD. Subjective concerns about deterioration of at least one cognitive domain and objective cognitive deficits for the individual’s age, with preserved functional activities, constitute the clinical criteria of MCI. Memory impairment is the distinguishing feature among MCI phenotypes and enhances differentiation between the amnestic and non-amnestic subtype. MCI due to AD is considered an etiological diagnostic entity, defined by episodic memory impairment and pathological cerebrospinal fluid biomarkers, that constitutes a predementia stage of ADD [8]. Although MCI patients are considered to be safe drivers [9], a number of studies report important driving errors in such patients in comparison to cognitively intact healthy older persons [10,11, 10,11]. Critical driving measures that differentiate patients with MCI from healthy individuals are low average speed, increased reaction time and distance from the vehicle ahead [7], difficulty in maintaining a proper lateral position of the vehicle [12], as well as difficulty in making left turns [13].
Various factors contribute to impaired driving behavior: type of dementia, disease stage, other comorbidities [14], and severity of cognitive decline in both patients with MCI and ADD [15]. One of the factors associated with cognitive decline is APOE4, a well-documented genetic risk factor of AD found in almost 40%of patients with ADD [16] and in an almost 30%of patients with amnestic MCI (aMCI) [17].
Cognitive deficits in MCI patients who are carriers of APOE4 are more severe in comparison with non-carriers, mainly affecting episodic memory [18], both verbal [19] and visuospatial [20]. The greater episodic memory impairment of carriers of APOE4 relative to non-carriers extends to ADD [21]. In addition, aMCI carriers of APOE4 progress to AD dementia at an increased rate and have increased rate of cognitive and functional deterioration [18].
The main aim of the current study was to examine whether the presence of APOE4 in patients with aMCI or mild ADD affects their driving performance compared to non-carriers in a simulated driving environment. The study is a preliminary investigation of the effect of APOE4 on driving measures in a small group of patients. A secondary aim was to explore possible differences in the cognitive functions of the two groups through neuropsychological assessment.
MATERIALS AND METHODS
Participants
Participants were recruited through the DRIVER BRAIN study (“Performance of drivers with cerebral diseases at unexpected incidences”) investigating the impact of neurological disorders on various driving parameters (https://www.nrso.ntua.gr/geyannis/res/rn59-driverbrain-performance-of-drivers-with-cerebral-diseases-at-unexpected-incidents-in-the-framework-of-the-research-programme-aristeia-of-the-general-secretariat-for-research-and-technology-2012/). The 28 participants of the current study were selected from a total of 98 patients with MCI and ADD (Fig. 1). Participants had been referred to the Cognitive Disorders/Dementia Unit, 2nd Department of Neurology of the NKUA “Attikon” University General Hospital for evaluation. In order to participate in the DRIVER BRAIN study, patients had to meet the following criteria: a) be diagnosed with either aMCI or ADD, b) have a valid driving license, c) be active drivers, defined as driving at least once a week for 10 km per week and 2500 km per year, d) be experienced drivers, defined as having driven for more than three years after acquiring their driving license. Exclusion criteria were a) history of psychosis, b) significant motor or visual disorder, c) complaints about dizziness or nausea while in a moving vehicle, d) record of traffic accidents in the last two years, to ensure that only competent drivers participated in the study, e) evidence of alcohol or drug addiction. Additional criteria for the current study were agreeing to provide a blood sample for APOE genotyping. Fourteen participants who were APOE4 carriers (4 female) and 14 who were non-carriers (1 female) were recruited for the study.
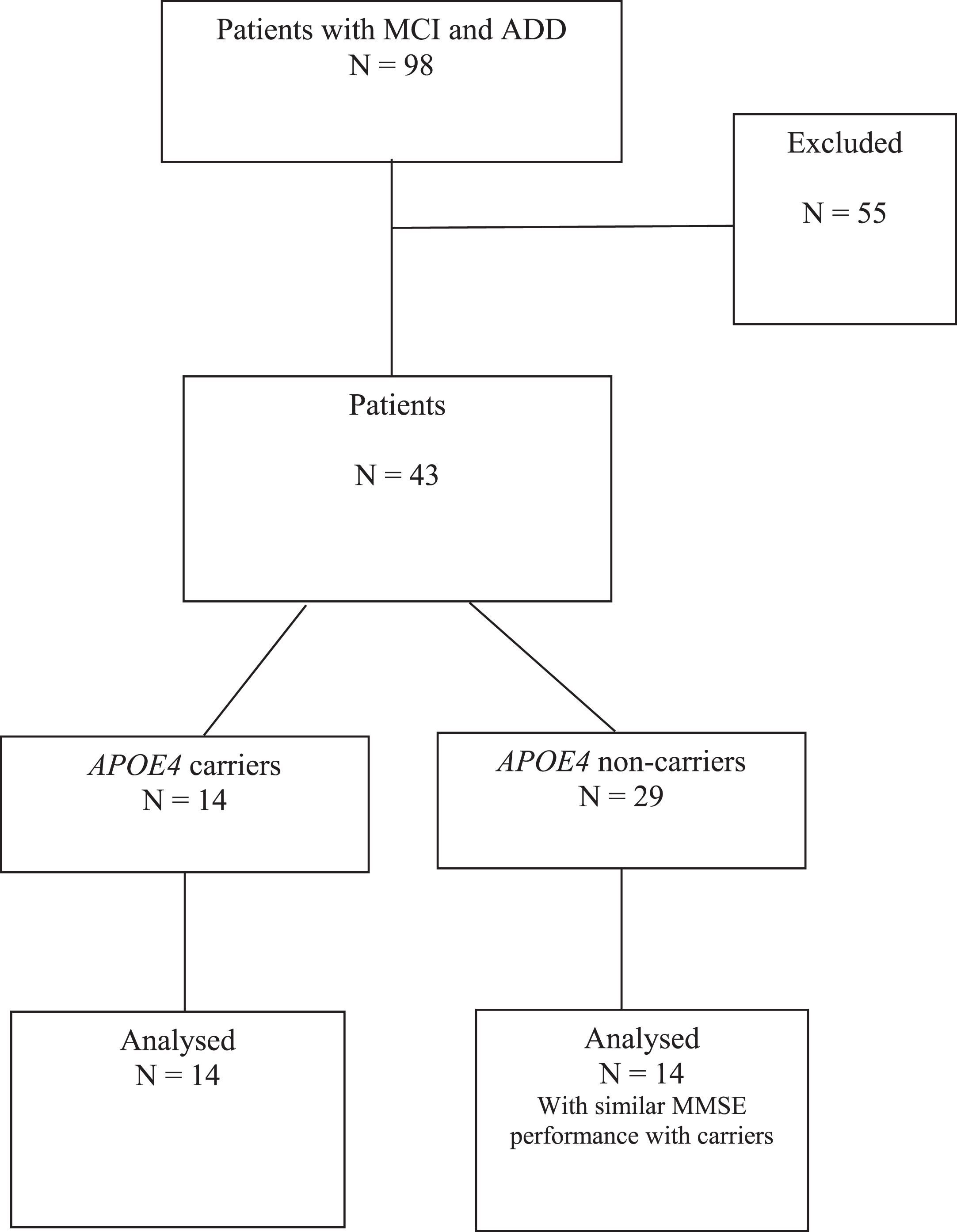
Flow diagram of participants in the current study. Participants were excluded from the current study either for not providing a blood sample (n = 43) by the time of the current study analysis or for dropping out from the explored driving conditions due to simulation sickness (n = 12).
Medical/neurological evaluation
All participants underwent a comprehensive neurological and full ophthalmological evaluation. The Useful Field of View (UFOV) [22] was also administered as a test of visual attention and processing speed. Memory complaints, functionality of daily living, neuropsychiatric symptoms, and drug and alcohol use were ascertained from a medical history, verified by an informant. To exclude metabolic and structural causes of memory impairment, blood tests and brain MRI scans were evaluated. The diagnosis of aMCI was made according to the Petersen and Morris criteria [23] along with a score of 0.5 on the Clinical Dementia Rating Scale (CDR) [24], and the diagnosis of ADD was in accordance with the McKhann et al. criteria [25], along with a score of 1 on the CDR indicating mild disease stages. All diagnoses were made by the same behavioral neurologist with expertise in cognitive disorders and dementia (SGP).
At the initial evaluation, four patients in the APOE4 carriers group were taking anticholinesterases, two were taking antidepressants, and no patient was taking medication for sleep. In the APOE non-carriers group, two patients were taking anticholinesterases, two patients were taking antidepressants and two patients were taking medication for sleep.
Neuropsychological assessment
Cognitive functions were assessed with an exten-sive neuropsychological battery evaluating: a) general cognitive function (Mini-Mental State Examination, MMSE) [26]; b) executive functions (Frontal Assessment Battery (FAB) [27]; Trail Making Test A (TMT A) and B (TMT B) (a Greek version of the TMT [28]); Wechsler Adult Intelligence Scale-3rd edition (WAIS-III) Letter Number Sequencing (LNS) [29]; Symbol Digit Modalities Test written version (SDMT) [30]; Semantic Verbal Fluency-category: animals), c) visuospatial perception and constructional ability (Judgement of Line Orientation (JLO) [31]; Clock Drawing Test (CDT), scored according to Freedman et al. criteria [32]), d) verbal episodic memory (a Greek version of the Hopkins Verbal Learning Test- Revised (HVLT-R) [33]), and e) visuospatial episodic memory (Brief Visuospatial Memory Test-Revised (BVMT-R) [34]).
Measurement of APOE and genotyping
During the medical evaluation, venous blood in EDTA vacutainer tubes was drawn for apolipoprotein E genotyping. DNA isolation was performed with the High Pure Polymerase Chain Reaction (PCR) Template Kit by Roche. For the APOE’s gene amplification a real-time qPCR kit (TIB MolBiol) was used in the Light Cycler PCR platform by Roche [35]. PCR followed by HhaI restriction digestion and analysis in ethidium bromide-stained 4%high-resolution agarose gels was also performed as a confirmative test for positive or ambiguous APOE4 samples [36].
Driving simulator experiment
Driving behavior was assessed through a driving simulator experiment. The driving simulator was a quarter-cab Foerst FPF (3 LCD screens 42”, full HD: 1920×1080 pixels-total field of view 170 degrees). The simulator was validated against a real word environment [37].
The experimental procedure took place at the Department of Transportation Planning and Engineering of the National Technical University of Athens. The experiment included both rural and urban driving conditions. Only the rural conditions were used in the current study because of increased participant attrition in the urban conditions due to simulation sickness (from the selected participants only 22 drove in both the rural and urban conditions). After a brief practice session, participants drove in a simulated rural single carriageway road with a 3 m lane width with zero gradient and mild curves. Each driving condition (moderate, high traffic volume) was 2.1 km long. Two unexpected incidents occurred at fixed points on the roadway: a deer or a donkey suddenly appeared on the road. Moderate traffic volume was calculated as Q = 300 vehicles per hour and high traffic volume as Q = 600 vehicles per hour. Both conditions were included in the current study in order to compare the effect of different driving demands on the driving measures.
For the current study, the driving measures that were examined were: a) average speed (in km/h), b) speed variability (SD), c) headway distance, the distance from the leading vehicle (in meters), d) headway distance variability (SD), e) lateral position, the distance from the right road border in meters, f) lateral position variability (SD), g) reaction time (RT) in unexpected incidences (in ms), h) accident probability, a binary variable reflecting the occurrence of a crash in the unexpected incidents.
Ethical considerations
The study was conducted in accordance with the Helsinki Declaration and was approved by the Research Ethics Committee of the Attikon General University Hospital. Participants were informed about the study and were asked to sign a written consent, which included a request for permission to conduct genetic testing related to neurodegenerative disorders. It was clarified that participation would be voluntary and that participants had the right to withdraw at any time. It was highlighted that personal data would remain confidential and that the results of genetic testing and performance measures would be used for research purposes only.
Statistical analysis
Independent samples t-tests were used for the comparisons between carriers and non-carriers of the APOE4 in terms of demographic characteristics and performance on the neuropsychological tests. GLM mixed two-way ANOVAs were used with participant type (APOE4 carriers, non-carriers) as between-subject variable and condition (moderate, high traffic volume) as withing-subject variable. Chi-square tests of independence were used to assess differences in accident probability. Pearson correlation coefficients were computed to examine the relationship of the neuropsychological measures with the driving measures. To further explore the relationship of the driving measures to APOE4 status, analyses were conducted using the coefficient of variation (COV) of each driving measure. The COV is a measure of intraindividual variability, computed as the raw intraindividual SD divided by the raw intraindividual mean. The COV adjusts for mean level of performance, which can affect the SD, as lower SDs tend to be associated with lower means [39]. Analyses were conducted using IBM SPSS Statistics v22.0 and statistical significance level was p < 0.05.
RESULTS
Demographics
Independent samples t-test were conducted in order to compare the two groups in age, years of education, driving experience (years) and MMSE score (Table 1). The two groups did not differ in demographic characteristics and MMSE score and therefore no demographic adjustments were made in the comparisons of test performance.
Demographic characteristics and MMSE of carriers and non-carriers of APOE4
MMSE, Mini-Mental State Examination; APOE4, Apolipoprotein E4 allele.
Driving performance
Mixed two-way ANOVAs showed that traffic vol-ume had a statistically significant main effect on speed [F(1,26) = 11.88, p = 0.002,
Descriptive statistics of driving measures and driving measures COV by traffic load and APOE4 presence
Lat. Posit, lateral position; Head, headway distance; RT, reaction time; COV, coefficient of variation; APOE4, Apolipoprotein E4 allele.
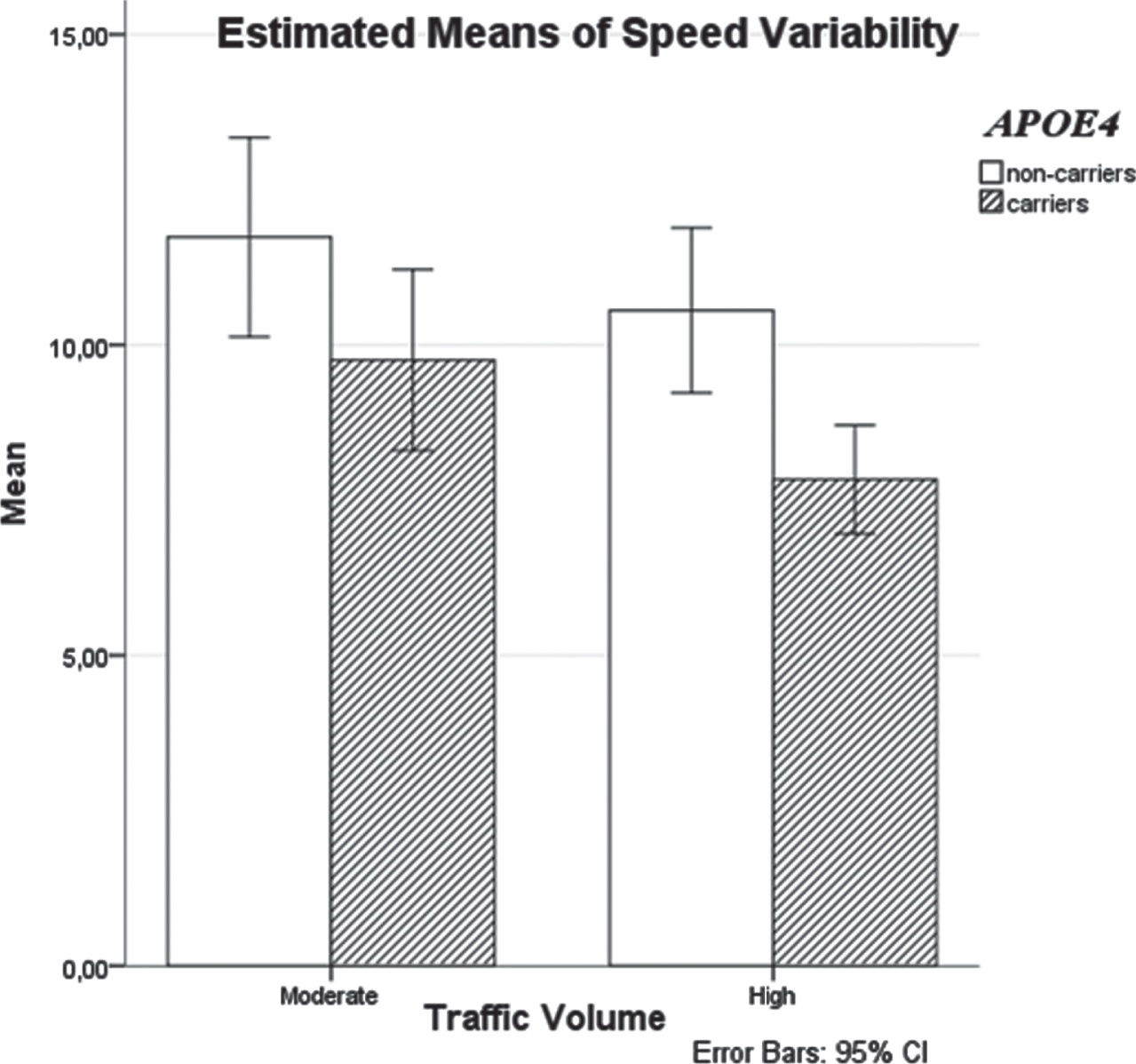
Differences in speed variability between APOE4 carriers and non-carriers by traffic volume.
We subsequently examined the relationship of the driving measures to APOE4 status using the COV. Mixed two-way ANOVAs showed a significant main effect of traffic volume on lateral position COV [F(1,26) = 55.28, p < 0.001,
The chi-square test of independence showed that accident probability did not differ by APOE4 presence, either in moderate (χ2(2, N = 28) = 2.49, p =0.29) or in high traffic volume (χ2(2, N = 28) = 0.38, p = 0.83).
Neuropsychological performance
Independent samples t-test were used to compare APOE4 carriers and non-carriers on the neuropsychological measures. There were no significant differences between the two groups (Table 3). The Supplementary Material includes the correlations between the neuropsychological tests and the driving measures for each traffic volume condition.
Performance of APOE4 carriers and non-carriers on neuropsychological measures
FAB, Frontal Assessment Battery; TMT-A/TMT-B, Trail Making Test A and B; LNS, Letter Number Sequencing (WAIS-III); SDMT, Symbol Digit Modalities Test; HVLT-R total, Hopkins Verbal Learning Test-Revised Total; HVLT-R DR, Hopkins Verbal Learning Test-Revised Delayed Recall; HVLT-R REC, Hopkins Verbal Learning Test-Revised Recognition; HVLT-R DI, Hopkins Verbal Learning Test-Revised Discrimination Index; BVMT-R total, Brief Visuospatial Memory Test-Revised Total; BVMT-R DR, Brief Visuospatial Memory Test-Revised Delayed Recall; BVMT-R REC, Brief Visuospatial Memory Test-Revised Recognition; BVMT-R DI, Brief Visuospatial Memory Test-Revised Discrimination Index; JLO, Judgment of Line Orientation; CDT, Clock Drawing Test; APOE4, Apolipoprotein E4 allele.
DISCUSSION
The objective of the current study was to compare APOE4 carriers with aMCI or mild ADD with non-carriers on a number of driving measures in two simulated rural driving conditions: with moderate and high traffic volume. APOE4 presence affected driving speed variability in the absence of differences in neuropsychological test performance.
APOE4 carriers had significantly lower speed variability than non-carriers, which was maintained after the utilization of speed COV. A recent study found smaller deceleration variability in speed in naturalistic in-car driving in older persons with worse cognitive health using the speed COV [40]. Lower speed variability in our study might reflect a conservative way of driving, compatible with the “driving profile” of patients with mild ADD [4].
Driving can be viewed as a multitasking procedure involving serial switching between information sources. Speed variability demands efficiently shifting attention between in-vehicle task performance and the environment, which means disengaging attention from one task before attending to another. By this notion, steady speed maintenance might be an attempt to serialize a behavior in a multicomponential task: temporarily “ignore” speed changes and focus on other driving measures aiming at a safer operation of the vehicle. This disproportional focus in order to avoid mistakes and safely operate the vehicle leaves the speed operation “ignored”, or in other words disengaged by attention.
Although reduced speed variability seems to reflect an impairment in attentional engagement because of reduced speed adaptations, it might indicate a compensatory strategy. Impairment would arise as an indication of decline in executive functions, including attentional operations, when driving in more complex environments [41]. Interestingly, there was no interaction of APOE4 status with traffic volume, a result that would support the idea of attentional impairment. Such an interaction would indicate that APOE4 carriers were more challenged when driving in a more cognitively demanding environment. Its absence suggests that APOE4 plays a role in the demands identification of driving under increased cognitive load. Therefore, not re-engaging in speed adaptions while driving might be attributed to scheduling a compensatory strategy rather than to limitations of cognitive control, as previously suggested [42].
Cognitive performance was not significantly different between the two groups, supporting the hypothesis that the effect of APOE4 on attentional disengagement is a compensatory strategy rather than an impairment mediated by cognitive differences, and indicating that the driving performance may be a more sensitive measure than the cognitive tests. Although the two groups were matched for mean MMSE score, a larger sample might have been more sensitive to a fuller spectrum of driving differences between APOE4 carriers and non-carriers, as sample size is an important factor when exploring possible effects of an allele on a clinical phenotype [43]. Moreover, due to the small number of participants, the inclusion of both aMCI and mild ADD drivers in each group may have increased the heterogeneity of each group. Nevertheless, a significant difference in speed variability with a large effect size did emerge, which persisted after the Bonferroni correction.
Traffic volume affected all driving measures in the expected direction: drivers drove slower, left smaller headway distances and larger distances from the right road border, and had larger RTs in unexpected events in the high relative to the moderate traffic volume condition. Speed and headway variability were smaller in the high relative to the moderate traffic volume, consistent with their smaller means; lateral position variability was also smaller in the high traffic condition. When adjusted for mean performance, a significant effect of traffic volume was shown in headway distance COV, with a larger COV in the high traffic volume condition, and in lateral position COV, with a smaller COV in the high traffic volume condition. The effects of traffic volume on headway distance COV and lateral position COV, but not on speed COV, are consistent with the results of a recent study on intraindividual variability of driving behavior in healthy individuals [44].
High traffic volume can be regarded as a condition of higher cognitive load compared to moderate traffic volume due to its increased cognitive demands. According to the cognitive control hypothesis, cognitive load, a measure of the demanded resources in a competing activity, selectively affects driving subtasks that demand cognitive control but not those relying on automatic performance [45]. Thus, the smaller lateral position COV and larger headway distance COV in high traffic could be attributed to an increase in cognitive load mobilizing a more efficient attempt for cognitive control. Speed would need a higher cognitive load to be affected, which was not induced by traffic volume differences.
To our knowledge, this is the first study to compare driving performance in APOE4 carriers and non-carriers with aMCI or mild ADD. APOE4 carriers had lower speed variability than non-carriers, which might indicate a compensatory strategy. In conclusion, the identification of sensitive tools which assess multitasking procedures such as driving on a simulator makes feasible the exploration of functional differences related to genetic biomarkers. Nevertheless, the finding of only one driving measure showing a significant effect of APOE4 status should be replicated in a larger sample. Future studies could explore the possible effect of APOE4 on different cognitively demanding driving conditions, such as driving with distraction, both in patients with neurodegenerative disorders and in healthy individuals.
Footnotes
ACKNOWLEDGMENTS
This research was carried out within the framework of the Operational Program “Education and Lifelong Learning” of the National Strategic Reference Framework (NSRF), namely the Research Funding Program: THALES. Investing in knowledge society through the European Social Fund, and the Action: ARISTEIA (Action’s Beneficiary: General Secretariat for Research and Technology), co-financed by the European Union (European Social Fund –ESF) and Greek national funds. The authors received no other funding for this study. An earlier version of the manuscript was presented at the 6th Congress of the European Academy of Neurology (May 2020).