
Abstract
Background:
The evidence regarding dementia and late-life weight change is inconsistent, and data on body weight fluctuation and dementia are limited.
Objective:
To test the hypothesis that weight loss and substantial weight fluctuation predict cognitive decline independent of body weight and traditional risk factors of dementia.
Methods:
This study utilized longitudinal data from the National Alzheimer’s Coordinating Center for 10,639 stroke- and dementia-free older adults (60.9%female, mean age 71.6 years, median follow-up 5.5 years). Trends in weight change and weight fluctuation were estimated for each individual by regressing repeated body weight measurements on time. Cognitive decline was examined as diagnostic progression from normal to mild cognitive impairment (MCI) or dementia and from MCI to dementia.
Results:
Compared to participants with stable weight, those with weight loss had increased odds of diagnostic progression (adjusted OR = 1.35, 95%CI [1.21, 1.51]). Also, large weight fluctuation was associated with increased odds of diagnostic progression (OR comparing the extreme quartiles = 1.20, 95%CI [1.04, 1.39]) after adjusting for traditional risk factors for dementia and body weight change. The magnitude of the association appeared larger among those older than 80 and those with 3 or more cardiometabolic risk factors at baseline (both p for interaction < 0.05).
Conclusion:
Weight loss and substantial weight fluctuation during late-life were associated with increased odds of cognitive decline independent of body weight and traditional risk factors of dementia. Our results suggested the linkage between late-life body weight instability and cognitive decline especially among those with greater age or higher cardiometabolic risk.
INTRODUCTION
Alzheimer’s disease and other dementias are a critical health problem among older adults, with about 50 million existing cases and 10 million new cases diagnosed worldwide every year [1]. Given the irreversible nature and tremendous burden of the disease, it is particularly important to identify potentially modifiable risk factors. While midlife obesity has been identified as a risk factor for dementia [2, 3], the association in late-life is inconsistent [4–9]. Many studies suggest that late-life weight loss is associated with an increased risk of cognitive decline [4–7], while other studies also show a similar relationship between late-life weight gain and dementia [8, 9]. Also, it is unclear whether the association differs between participants with normal cognition and those with mild cognitive impairment (MCI).
Emerging evidence also suggests that large visit-to-visit body weight fluctuation could be linked to major adverse health outcomes such as total mortality and cardiovascular mortality [10, 11]. Body weight fluctuation, which refers to intra-individual weight loss and gain over a period of time, may indicate the inability to maintain intrinsic physiological stability. This speculation is consistent with increasing data showing associations between fluctuation of metabolic biomarkers (e.g., blood pressure, glucose level, cholesterol level, and body weight) with cardiovascular events [12–15]. Giving the shared modifiable risk factors for cardiovascular diseases and dementia [16–18] and the considerable overlaps between cerebrovascular and Alzheimer’s disease pathology [19], large visit-to-visit metabolic fluctuation may have a role in risk for cognitive decline as well. There are studies suggesting that large weight fluctuations may be associated with cognitive decline [20–23]. However, it is unclear whether such association differs between participants with normal cognition and those with MCI; it is also undetermined whether the putative association of body weight fluctuation with cognitive decline is independent of the longitudinal trend in body weight change.
To investigate the relationship between longitudinal trend in body weight change and body weight fluctuation and cognitive decline, we utilized longitudinal data from National Alzheimer’s Coordinating Center (NACC).
MATERIALS AND METHODS
Study population
The study population came from the NACC’s Uniform Data Set (http://naccdata.org). Established by National Institute on Aging to collect data from nationwide Alzheimer’s Disease Research Centers (ADRCs) in the United States, NACC serves as one of the largest Alzheimer’s disease databases with standardized clinical and neuropathological research data. We used data collected from 37 past and current ADRCs between September 2005 and September 2020, with details described elsewhere [24]. Among 30,956 total individuals in the NACC database, those who were over 50 years old at baseline, with body weight measurements from at least 3 visits, and free of clinically diagnosed dementia and stroke at the initial visit were included. We excluded patients with stroke to restrict confounding and reduce the issue of reverse causation. 11,207 participants met the criteria. Among them, 7,742 had normal cognition, 568 had impaired-not-MCI, and 2,897 had MCI at the initial visit (see the flowchart in Fig. 1). We then excluded those with impaired-not-MCI given that the proportion is small and is a transitional period between normal cognition and MCI with equivocal clinical importance. Ultimately, 10,639 participants were enrolled. They were followed up approximately annually (interquartile range: 1.0–1.2 years), with body weight and cognitive status recorded at each visit.
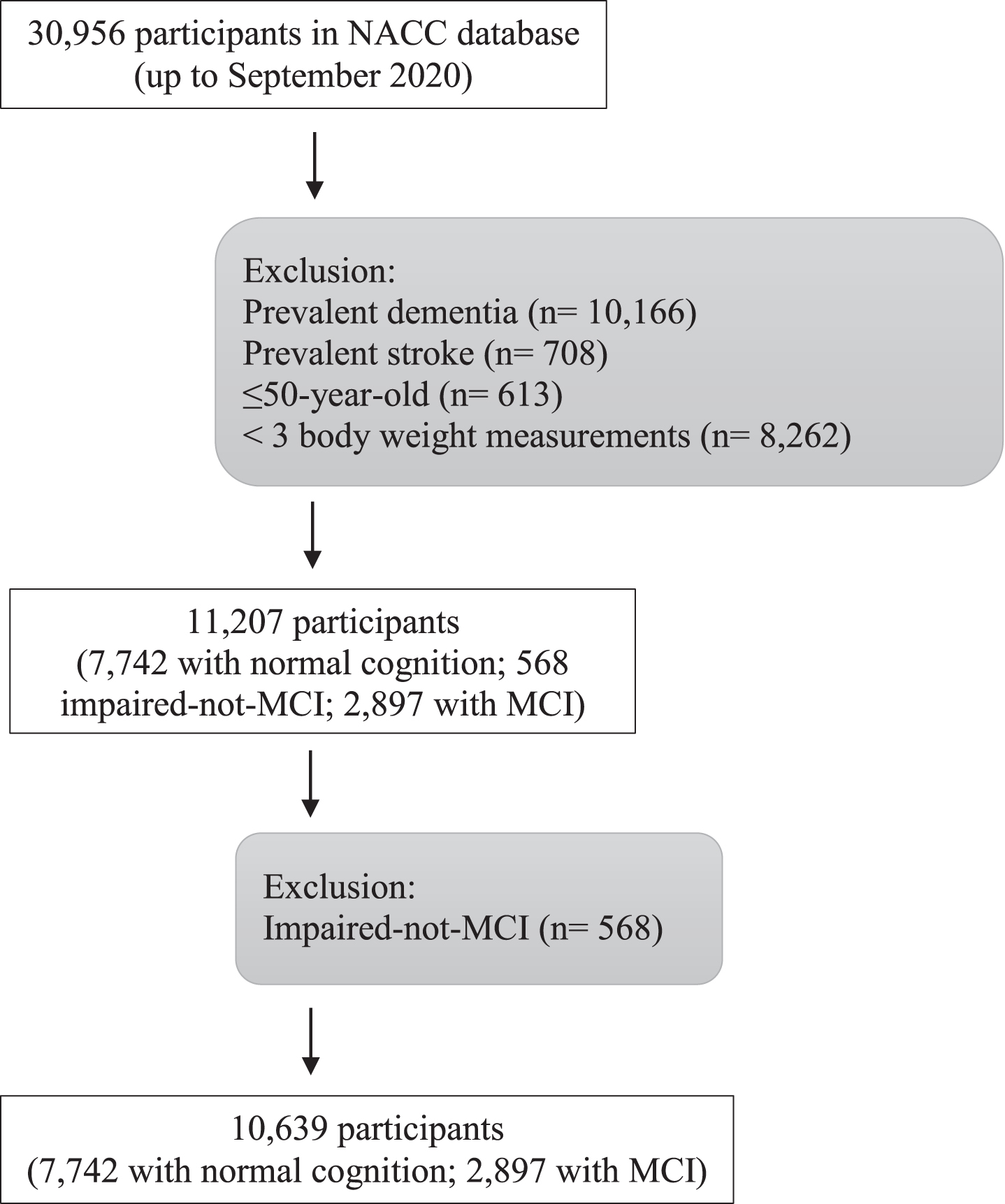
Study flow chart.
Body weight assessment
Each participant had three or more body weight measurements with a median of six (interquartile range: 4–9) per person. Body weights measured after the occurrence of the primary outcome, i.e., diagnostic progression of cognitive function, were not used. We assessed baseline body weight (at the first visit), body weight change, and body weight fluctuation. Body weight change refers to the rate of change (in kg/year) calculated in a linear regression model for each individual’s body weight measurements over time. Visit-to-visit body weight fluctuation (in kg) was defined as the root mean square error (RMSE) from the same linear regression model. We used the same model to estimate weight change and weight fluctuation for each individual so that weight fluctuation reflects the residual weight variability that is not captured by weight change. A schematic graph is provided in the Supplementary Material (Supplementary Figure 1). In our sensitivity analyses (see below), we also used the coefficient of variation (CoV), a commonly used measure defined as the standard deviation divided by the mean, to assess body weight fluctuation.
Cognitive status assessment
Cognitive status was classified into normal cognition, MCI, and dementia. It was made by the study clinician (often reviewed by a consensus panel, typically including neurologists, neuropsychologist, geriatricians, etc.) at each visit according to the modified Petersen criteria for MCI [25] and the NINCDS-ADRDA criteria for dementia [26]. The primary outcome of the study was diagnostic progression across longitudinal visits. To be specific, participants progressing from normal cognition to MCI or dementia, or from MCI to dementia during the follow-up period were defined as having cognitive decline. We also assessed progression in cognitive and functional status using the CDR® Dementia Staging Instrument. Specifically, we used the Clinical Dementia Rating Scale Sum of Boxes (CDR-SOB) score that was quantified at each visit [27].
Assessment of other covariates
Demographic characteristics, including age, gender, years of education, and race, along with weight, height, smoking habits, Apolipoprotein E (APOE) ɛ4 carrier status, and medical history (such as hypertension, diabetes mellitus, hypercholesterolemia, depression, heart attack, atrial fibrillation, and congestive heart failure) were collected according to the NACC’s Uniform Data Set data collection protocol [28]. These variables were considered as potential confounding factors in the analyses.
Statistical analysis
In primary analyses, we analyzed the association of body weight change and body weight fluctuation with cognitive decline. We first investigated the relation between body weight change (in kg/year) and diagnostic progression using a logistic regression model with adjustment for potential confounders, including baseline cognitive diagnosis, age, gender, race, weight, height, years of education, smoking habits, APOE ɛ4 carrier status, medical history (including hypertension, diabetes mellitus, hypercholesterolemia, heart attack, atrial fibrillation, and congestive heart failure), depression status (whether diagnosed and whether treated), and years of follow-up. Body weight change was classified into three categories, i.e., weight loss (< –1 kg/year, which is the bottom quartile), stable weight (weight change within 1.0 kg/year) and weight gain (≥1 kg/year). 1 kg/year was selected based on the distribution of body weight change to facilitate an intuitive clinical interpretation. The analysis using body weight change as a continuous variable is not reported due to the observed non-linear association.
We then investigated the association between visit-to-visit body weight fluctuation (in kg) and diagnostic progression using a logistic regression model, with adjustment for the confounding factors just described above. To assess the association of body weight fluctuation with cognition decline independent of body weight change over time, we further adjusted for the rate of weight change (in kg/year) in the analysis. Body weight fluctuation was analyzed both as a continuous variable and a quartile-based categorical variable.
We performed the above analyses for the sample as a whole and then separately for participants with normal cognition and with MCI at the initial visit. To assess whether the association was modified by baseline cognitive status (either normal cognition or MCI) and the interaction between weight fluctuation and weight change, a product term was added to the models.
In our secondary analyses, we assessed cognitive decline by the slope (i.e., rate of change) of the CDR-SOB score (in points/year), derived from a time-adjusted linear mixed effect model with random intercept and slope to account for inter-individual differences in baseline score and rates of change over time. The association between body weight fluctuation and estimated slope of CDR-SOB score was assessed in a linear regression model. To assess potential effect modification, we stratified the analysis by gender, age, follow-up period, and the number of cardiometabolic risk factors. For cardiometabolic risk, we categorized participants into low-risk and high-risk groups according to the number of cardiometabolic risk factors (including ever smoker, heavy drinking, obesity, history of hypertension, diabetes mellitus, and hypercholesterolemia) that each participant had at baseline. Participants with no more than two risk factors were classified into the low-risk group, and those with more than two risk factors were classified into the high-risk group. We conducted the above analyses in the fully adjusted models.
In the sensitivity analyses, we used CoV to measure body weight fluctuation. In order to compare the association estimates between RMSE and CoV, standardized z-scores were used for both measures. We also used an alternative approach, i.e., mixed-effect model to estimate body weight change and body weight fluctuation. As inflammation related mechanisms have been suggested to link body weight to cognitive decline [29, 30], we further adjusted for the use of anti-inflammatory medications in the analyses.
For participants with missing body weight measurements (5.1%of total repeated measurements), only available body weight measurements contributed to the models that estimated body weight change and body weight fluctuation. Other covariates with incomplete data (less than 5.0%) were handled by adding an additional category indicating missing values. All effect estimates are given with corresponding 95%confidence intervals. All p-values presented are two-sided, with a p-value of 0.05 or less considered statistically significant. Statistical analyses were performed using R version 3.6.1. (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
There were 10,639 participants included in the study. Of them, 6,483 (60.9%) were female and the mean (SD) age at baseline was 71.6 (8.7) years. 7,742 (72.8%) participants had normal cognition while 2,897 (27.2%) were classified as having MCI at baseline. The characteristics of the participants are summarized in Table 1 according to their weight change status and Supplementary Table 1 according to their weight fluctuation status. Over the median follow-up of 5.5 (interquartile 3 to 8) years, 2,900 (27.3%) participants had diagnostic progression, with 1,727 (16.2%) progressing from normal cognition to MCI, 170 (1.6%) from normal cognition to dementia, and 1,003 (9.4%) from MCI to dementia.
Participant characteristics by groups of body weight change*
*The body weight changes for overall participants were –0.38 kg/year±1.56 kg/year (mean±SD). **Characteristics at initial visit are given as mean±SD or percentage except where otherwise noted. ***Classified as body weight change ranging from –1.0 kg/year to 1.0 kg/year.
Longitudinal body weight change and cognitive decline
Compared to participants with stable weight over time, weight loss was associated with increased odds of diagnostic progression (OR = 1.35, 95%CI [1.21, 1.51]), as was weight gain over time (OR = 1.18, 95%CI = [1.01, 1.37]), after adjusting for potential confounding variables in the model as shown in Table 2. Similar relationship was observed both for participants with normal cognition and MCI at baseline.
Association of body weight change over time with diagnostic progression
*Odds ratios were estimated with adjustment for baseline cognitive status, age, sex, race, weight, height, years of education, smoking habits, APOE ɛ4 carrier status, medical history (including hypertension, diabetes mellitus, hypercholesterolemia, heart attack, atrial fibrillation, and congestive heart failure), depression status (whether diagnosed and whether treated), and years of follow-up. **Reference level, with body weight change ranging from –1.0 kg/year to 1.0 kg/year. # p for interaction between baseline cognitive status and body weight change was 0.270.
Visit-to-visit body weight fluctuation and cognitive decline
Large visit-to-visit body weight fluctuation was associated with higher odds of diagnostic progression (OR comparing the highest to lowest quartile = 1.23, 95%CI [1.06, 1.42], p for trend = 0.002) after adjusting for potential confounding variables. After further adjusting for body weight change, large body weight fluctuation was still associated with increased odds of diagnostic progression, albeit slightly attenuated, (OR = 1.20, 95%CI [1.04, 1.39], p for trend = 0.006) as shown in Table 3. Similar association was observed for both participants with normal cognition and MCI at baseline.
Association of body weight fluctuation with diagnostic progression
*Odds ratios were estimated with adjustment for baseline cognitive status, age, sex, race, weight, height, years of education, smoking habits, APOE 4 carrier status, medical history (including hypertension, diabetes mellitus, hypercholesterolemia, heart attack, atrial fibrillation, and congestive heart failure), depression status (whether diagnosed and whether treated), years of follow-up, and body weight change. **Range of each quartile: Q1: ≤0.70 kg; Q2: 0.70 kg to ≤1.25 kg; Q3: 1.25 kg to ≤2.00 kg; Q4: > 2.00 kg. ***Reference level. # p for interaction between baseline cognitive status and body weight fluctuation was 0.137.
Consistently, large body weight fluctuation was associated with greater increase in CDR-SOB score progression (p < 0.001) after fully adjusting for potential confounders including body weight change as shown in Supplementary Table 2. The estimated association was more pronounced in participants with normal cognition at baseline compared to those with MCI (p for interaction < 0.001).
Subgroup and sensitivity analyses
In subgroup analyses, the association of body weight fluctuation with diagnostic progression of dementia did not differ significantly by body weight change group (i.e., weight loss, stable weight, or weight gain), gender, or follow-up period. However, effect modifications were noted by age and cardiometabolic risk, and the association of body weight fluctuation with the diagnostic progression of dementia was more pronounced in older participants (p for interaction = 0.009) and those with high cardiometabolic risk (p for interaction < 0.001), as shown in Fig. 2. In the sensitivity analyses, similar associations were also observed when the coefficient of variation was used to quantify body weight fluctuation (Supplementary Table 3). The associations also remained essentially the same after using a mixed-effect model to estimate body weight change and body weight fluctuation (Supplementary Tables 4 and 5) and further adjusting for anti-inflammatory medications (Supplementary Tables 6 and 7).
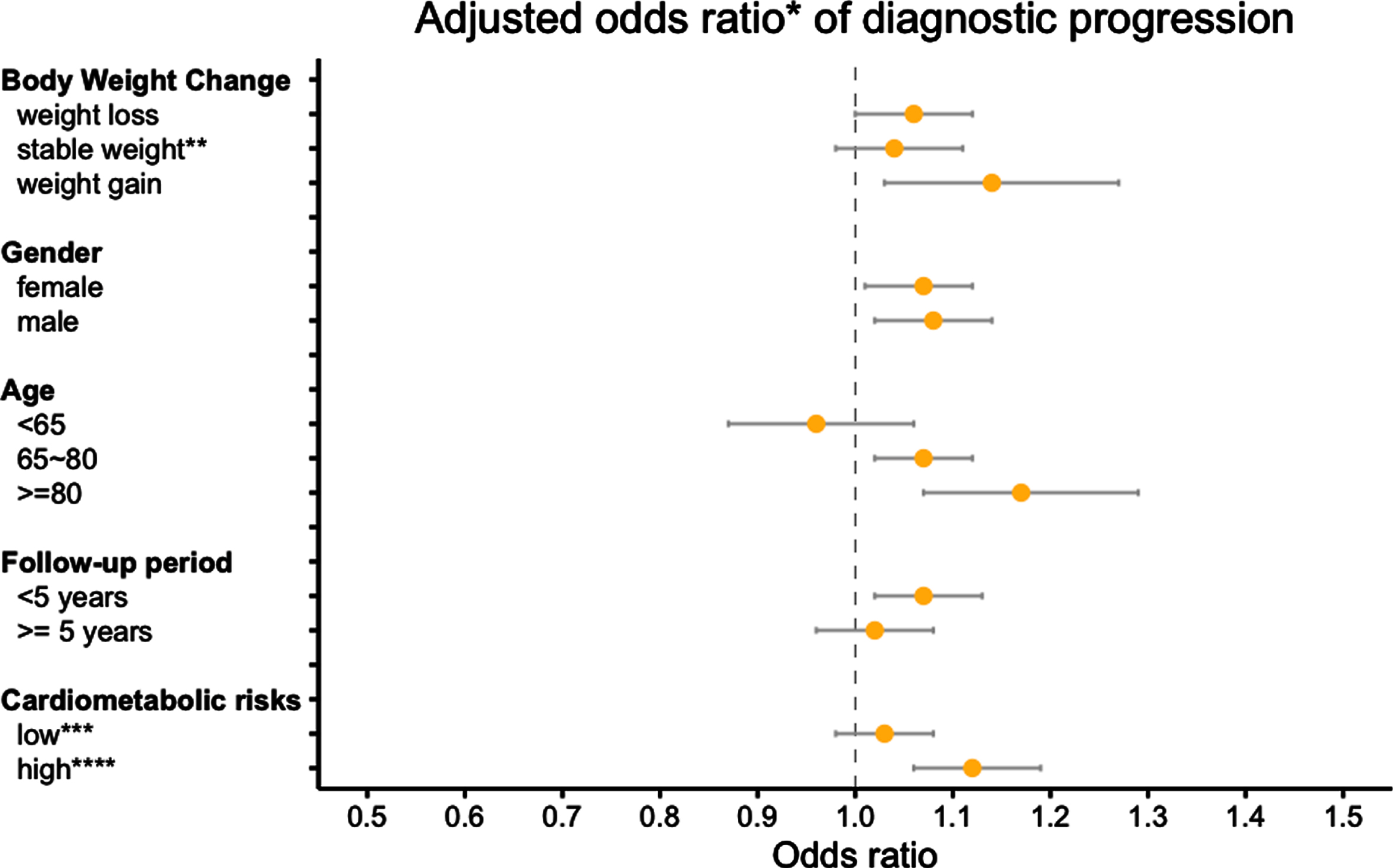
Adjusted odds ratio of diagnostic progression associated with body weight fluctuation between different subgroups. (p for interaction between subgroups = 0.319 for body weight change, 0.741 for gender, 0.009 for age, 0.701 for follow-up period, and < 0.001 for cardiometabolic risks). *The analyses were conducted in the fully adjusted model. **Stable weight refers to body weight change from –1.0 kg/year to 1.0 kg/year. ***Low cardiometabolic risk referred to participants with 2 or fewer cardiometabolic risk factors at baseline. ****High cardiometabolic risk refers to participants with 3 or more recognized cardiometabolic risk factors at baseline.
DISCUSSION
Our study, based on a longitudinal cohort of older adults free of stroke and dementia at baseline, found that weight loss over a period of four to nine years was associated with greater odds of cognitive decline. Substantial visit-to-visit body weight fluctuation was also associated with increased odds of cognitive decline, independent of weight loss or gain. Such association was more pronounced among those at older age or with higher cardiometabolic risk.
While obesity in midlife is a risk factor for mortality, morbidity in general, and dementia in particular, the association between body weight and dementia is more complex in late life, and in fact many studies suggest an “obesity paradox”, where there is higher risk of disease with lower body weight in many studies beginning in late life [31–33]. In the current study, we tried to better understand this paradox by looking at change in body weight over time. We found that the odds of cognitive decline increased in those who had weight loss over time, consistent with previous reports [4, 5], both in those with normal cognition and those with MCI at baseline. Also, we found that compared to participants with stable weight, both participants with weight loss and those with weight gain had increased odds of cognitive decline. The findings are similar to a nationwide study in Korea [9], where both weight loss and weight gain were found to be associated with the risk of dementia.
This study extends the observations from previous cohorts [20–23] that linked large body weight fluctuation to higher dementia risk in several ways. First, we assessed the association in those with and without cognitive decline at baseline. Second, to test the hypothesis that body weight fluctuation was associated with cognitive decline independent of baseline body weight, body weight change, and traditional risk factors for dementia, we adjusted for these factors simultaneously in our models. Our findings suggest that body weight fluctuation could be a risk factor for cognitive decline. Since we observed the association among people with normal cognitive and mild cognitive impairment, suggesting that weight fluctuation could either be a risk factor or an early-stage marker of cognitive decline. If the observed association is causal, the consistent results across both subgroups highlight the importance of body weight management for the prevention of dementia regardless of cognitive status through, for example, paying more attention to the elderly people with weight change greater than 1 kg/year. Also, the effect of weight fluctuation was only slightly attenuated after further adjusting for body weight change, similar to findings in a 20-year follow-up study of older women [21]. This finding is in many ways expected, given that in our study weight fluctuation was defined as the residual variability in body weight beyond the trend in weight change. Additionally, we found that this novel association between body weight fluctuation and cognitive decline was stronger among those with high cardiometabolic risk and those over age 80, suggesting that body weight fluctuation may reflect frailty status in older adults.
The mechanisms that might link body weight fluctuation to dementia are not fully understood. Mechanisms related to endocrine disturbance and adipocyte inflammation could be one explanation. According to an animal study, body weight fluctuation may cause greater adipocyte inflammation compared to consistent obese state [34]. There was also evidence from epidemiological studies suggesting a more abdominal fat distribution arising from body weight fluctuation [35, 36]. Altogether, previous studies suggested that greater weight cycling may induce dysregulation of adipose tissue and contribute to accelerated aging, including cognitive impairment. Our study also found a stronger association between weight fluctuation and cognitive decline among those with high cardiometabolic risk or older age, further suggesting the potential link between weight cycling, age-related morbidity, and frailty. On the other hand, the association could also be explained by reverse causation, i.e., weight loss and large weight fluctuation could be the prodromal symptoms of dementia [37]. For instance, there is evidence that many individuals lose their sense of smell prior to the onset of dementia [38, 39], which may lead to loss of appetite. In addition, small functional changes may make it more difficult to obtain or prepare food, which could lead to a change in dietary patterns or to dietary reductions.
Our study has several limitations. First, body weight fluctuation could partly result from measurement error. Nevertheless, the consistent associations observed across different cognitive subgroups using different metrics of variability suggest that our main findings are unlikely to be fully explained by measurement error. Second, our follow-up period over a median of 5.5 years was not long enough to establish the temporal order of the association of body weight change and fluctuation with cognitive decline, which needs to be confirmed in studies with longer follow-ups. Third, there was no information on whether weight loss and gain were intentional or unintentional, which may reflect different physiological changes. Residual confounding also cannot be ruled out given the observational nature of our study. Fourth, our study is based on a volunteer cohort with high levels of education and predominantly white. In addition, such cohorts are often enriched in those with higher risk of dementia onset due to family history or subclinical symptoms [40]. The baseline body weight in the current study was quantified in late life, which may not necessarily reflect the weight status during mid-life or earlier adulthood. Cautions are warranted when generalizing the findings to community-based or younger populations. On the other hand, our study is novel in that we assessed both body weight change and weight fluctuation as well as their joint impact on cognitive decline in older adults free of stroke and dementia at baseline. In addition, this prospective cohort had more than 10,000 participants with comprehensive assessment of cognitive status, allowing for studying the relationship across a wider cognitive spectrum, and sufficient statistical power for subgroup analyses to assess the important effect modification by age and cardiometabolic risk.
To conclude, in this cohort of older adults free of stroke and dementia, weight loss and substantial weight fluctuation were associated with increased odds of cognitive decline independent of body weight and traditional risk factors for dementia. The association of weight fluctuation with cognitive decline was stronger among those with older age or higher cardiometabolic risk. Further studies with longer follow-up duration are needed to test whether weight loss and large weight fluctuation are solely prodromal symptoms of dementia or risk factors that exacerbate cognitive decline.
Footnotes
ACKNOWLEDGMENTS
This work was partly supported by the National Institute On Aging of the National Institutes of Health under Award Number K99AG071742 (Yuan Ma). The NACC database is funded by NIA/NIH Grant U01 AG016976 and NIA/NIH Grant U01 AG32984. NACC data are contributed by the NIA-funded ADRCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P50 AG005134 (PI Bradley Hyman, MD, PhD), P50 AG016574 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Thomas Wisniewski, MD), P30 AG013854 (PI Robert Vassar, PhD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennett, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P50 AG005131 (PI James Brewer, MD, PhD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russell Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG053760 (PI Henry Paulson, MD, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P30 AG049638 (PI Suzanne Craft, PhD), P50 AG005136 (PI Thomas Grabowski, MD), P50 AG033514 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD), P50 AG047270 (PI Stephen Strittmatter, MD, PhD).