
Abstract
Background:
The rate of cognitive decline in Alzheimer’s disease (AD) has been found to vary widely between individuals, with numerous factors driving this heterogeneity.
Objective:
This study aimed to compute a measure of cognitive decline in patients with AD based on clinical information and to utilize this measure to explore the genetic architecture of cognitive decline in AD.
Methods:
An in-house cohort of 616 individuals, hereby termed the Cardiff Genetic Resource for AD, as well as a subset of 577 individuals from the publicly available ADNI dataset, that have been assessed at multiple timepoints, were used in this study. Measures of cognitive decline were computed using various mixed effect linear models of Mini-Mental State Examination (MMSE). After an optimal model was selected, a metric of cognitive decline for each individual was estimated as the random slope derived from this model. This metric was subsequently used for testing the association of cognitive decline with apolipoprotein E (APOE) genotype.
Results:
No association was found between the number of APOE ɛ2 or ɛ4 alleles and the rate of cognitive decline in either of the datasets examined.
Conclusion:
Further exploration is required to uncover possible genetic variants that affect the rate of decline in patients with AD.
INTRODUCTION
Alzheimer’s disease (AD) is the most prevalent neurodegenerative disease and the most common cause of dementia. Worldwide, it is estimated to affect more than 45 million people, and due to the global aging of the population, this number is expected to rise fourfold by 2050 [1]. In the UK, there is an estimated 850,000 people with AD [2], resulting in a total estimated societal cost of £26.3 billion per annum, despite the fact that a large part of the care for people with AD is provided by informal unpaid caregivers [3]. Notably, AD is the leading cause of death in England and Wales, accounting for 12.7% of all deaths registered [4]. As the world’s population continues to age, the resources required to adequately address AD will greatly increase, and effective interventions to delay the onset and the progression of the disease will be necessary to reduce the impact it has both on the people directly affected and on society as a whole.
The severity of the symptoms and the rate of disease progression are important factors to consider regarding AD, as people with a severe phenotype or a rapid decline are considerably more likely to require additional care resources, including early institutionalization and increased total societal costs even with informal caregiving [5, 6]. Therefore, attenuating the rate of cognitive decline in people with AD can be effective in decreasing the societal burden of dementia in addition to reducing the risk for developing AD.
Both population-based and clinical studies have shown that only about 30% of AD patients manifest a slow progression, with the majority of individuals declining rapidly after diagnosis [7–9]. Various factors have been implicated in the rate of progression in AD, including educational attainment, medical comorbidities, nursing home placement, age, and baseline cognition level [10–13]. However, the results remain inconclusive and there are currently no reliable methods to predict disease progression in AD.
There are numerous methods of assessing disease severity and progression in individuals with AD, most of them being questionnaire-based assessment scales. The most commonly used scale, both in research and in clinical settings, is the Mini-Mental State Examination (MMSE) [14]. MMSE has the advantage of being quick and easy to administer, which is particularly important when it comes to dementia patients; however, it only examines cognition and does not take into account other areas of functioning that AD tends to affect. Other assessment scales, like Clinical Dementia Rating [15] and Activities of Daily Living [16], focus on additional domains of every day functioning, making them a preferred method of assessing different areas of deterioration, apart from cognition. Moreover, there are also a number of biological predictors commonly used in monitoring progression in AD, including blood and cerebrospinal fluid biomarkers [17], as well as neuroimaging methods [18].
The evidence for a genetic predisposition to faster decline in patients with AD is inconclusive. Apolipoprotein E (APOE) ɛ4 allele is the strongest genetic risk factor for sporadic AD [19]. Numerous studies have examined the association of the APOE genotype with disease progression and cognitive decline in patients with AD. However, the results are conflicting, with some studies finding that the APOE ɛ4 allele is associated with faster progression [20–22], and other showing opposing results [23–25].
It is evident that being able to predict the rate of decline in AD patients using readily available clinical information would be of great use both to patients and their caregivers, as well as medical professionals. Moreover, identifying individuals that are at risk of a rapid decline would be of great use in the design and implementation of clinical trials for therapeutic interventions, as they are the patients that are most likely to manifest results within a short timeframe. Various methods of predicting cognitive decline have been suggested. Machine learning algorithms have been previously employed to assess progression in dementia, using a wide variety of predictors, including neuroimaging data [26, 27], amyloid positron emission tomography (PET) [26], and various cognitive assessment scales [28, 29]. Latent class models and mixed effects models have also previously been investigated [13, 30]. However, there is no universally accepted method of modelling cognitive decline in AD patients.
This study aims to derive, assess, and compare measures of cognitive decline, while accounting for different number of participants’ assessments and potential confounders in patients with AD, and to test the association of the APOE genotype for the progression measure derived. A replication of the results was attempted using Alzheimer’s Disease Neuroimaging Initiative (ADNI) [31] data.
METHODS
Sample
This study included individuals from two datasets, a cohort 616 individuals known as the Cardiff Genetic Resource for AD genotyped as part of the GERAD dataset [32, 33] and a subset of the publicly available ADNI database, including participants that enrolled in ADNI with AD or were diagnosed with AD at later assessments. Out of the Cardiff Genetic Resource for AD, 540 individuals had late-onset AD (LOAD), with onset of symptoms at 65 years of age and above, and 76 had early onset AD (EOAD). The number of assessments varied between individuals, with a range between 2 and 8, with an interval spanning between 7 months and 16 years. The ADNI design is described in detail elsewhere [31]. Out of the available ADNI participants, 577 had two or more assessments with a diagnosis of AD and were included in this analysis, 518 having LOAD and 59 having EOAD. MMSE was used as a measure of cognitive function in this study.
Generation of measures of decline
In order to account for all available assessments, a number of linear mixed effects models were constructed and subsequently compared. Mixed effect models are an advantageous method of analyzing longitudinal data as they allow for random disease progression effects that vary between individuals, as well as the varying number of assessment per individual and the variable length of time between assessments, which are commonly seen in longitudinal studies [34]. For all the models we tested, MMSE score at several assessment points was the dependent variable, and to account for the fact that the same individual was assessed at multiple time points, the individual ID was included as a random effect. Since the rate of progression may depend on disease duration [7], we first assessed the model where duration at the time of each assessment was included as a random effect. Disease duration, defined as time elapsed between onset of AD symptoms and each cognitive assessment, was selected as the variable of interest, based on existing literature highlighting the fact that time elapsed since symptom onset affects cognitive decline more than age in AD patients [7]. Age at disease onset is not known for the participants of ADNI. Therefore, for individuals that entered the study as AD patients, disease duration was calculated as time elapsed from study enrolment [22]. For individuals that developed dementia while the study was ongoing, duration was defined as time elapsed since the first assessment in which they were classified as AD patients. Next, the inclusion of a number of additional independent variables was assessed. Age at each assessment was added as a fixed effect, then a random effect, and subsequently age was added as both a fixed and a random effect. Duration and gender were also added as fixed effects sequentially, as they have been shown to influence the rate of decline [22, 35]. The models are further described in Supplementary Table 1. The random slopes for disease duration generated by the models were extracted for each individual and utilized as measures of cognitive decline in subsequent analyses.
The derived rate of decline measure was compared between individuals with EOAD and LOAD, using linear regression, adjusting for age and sex.
All statistical analyses were performed using the statistical software R [36] and the linear mixed models were generated using the package lme4() [37].
APOE genotype analysis
The samples were genotyped in two stages. For the first stage, the genotyping was performed on the Illumina 610 microarray and is described in detail elsewhere [32, 33]. For the second stage, genotyping was performed on Illumina GSA array, and completed in three waves in Lille, Cardiff, and Edinburgh. The number of APOE ɛ4 and ɛ2 alleles was derived for each individual using the rs429358 and rs7412 variants. For ADNI, APOE genotype was available through whole genome sequencing, and is described in detail elsewhere [31]. The association of the number of ɛ4 and ɛ2 alleles with decline was assessed using linear regression. The statistical analyses were conducted using R [36].
RESULTS
Sample characteristics
The demographic characteristics of the Cardiff Genetic Resource for AD are illustrated in Table 1. For the individuals with LOAD, the mean age at recruitment was 81.89, mean age at last assessment was 84.33 and the mean number of assessments was 3.13. Mean MMSE score at first assessment was 16.82, mean MMSE score at last assessment was 11.34 and 69.82% of the individuals were female. For the individuals with EOAD, the mean age at recruitment was 66.80, mean age at last assessment was 69.85 and the mean number of assessments was 3.15. Mean MMSE score at first assessment was 18.49, mean MMSE score at last assessment was 12.96 and both sexes were equally represented in the dataset. Note, that even at the first assessment the MMSE score for 40 individuals were 0. We have included these individuals in the analyses, as it has been shown that cognitive fluctuation is common in AD [38], and for a number of these individuals MMSE score in later assessments was not 0.
Cohort characteristics
Generation of measures of decline
The model selected as the optimal model for assessing rate of decline in this dataset included age at assessment and disease duration as random and fixed effects and sex as fixed effect. The random effects of age at assessment and disease duration were included to model individual-specific variation in cognitive decline. The fixed effect of sex, age at assessment and disease duration were significant predictors of cognitive performance (β= 2.779, p = 4.34×10–19, β= –0.165, p = 4.28×10–17, and β= –1.217, p = 1.32×10–18, respectively), therefore they were also included in the model. The direction of the effect indicates that cognitive performance decreases with age (by 0.165 MMSE points per year of age) and disease duration of AD (by 1.217 MMSE points per year of disease). Furthermore, females have higher cognitive performance than males of the same age and disease duration (by 2.779 MMSE points). The distribution of random slopes for disease duration derived from this model is shown in Fig. 1.
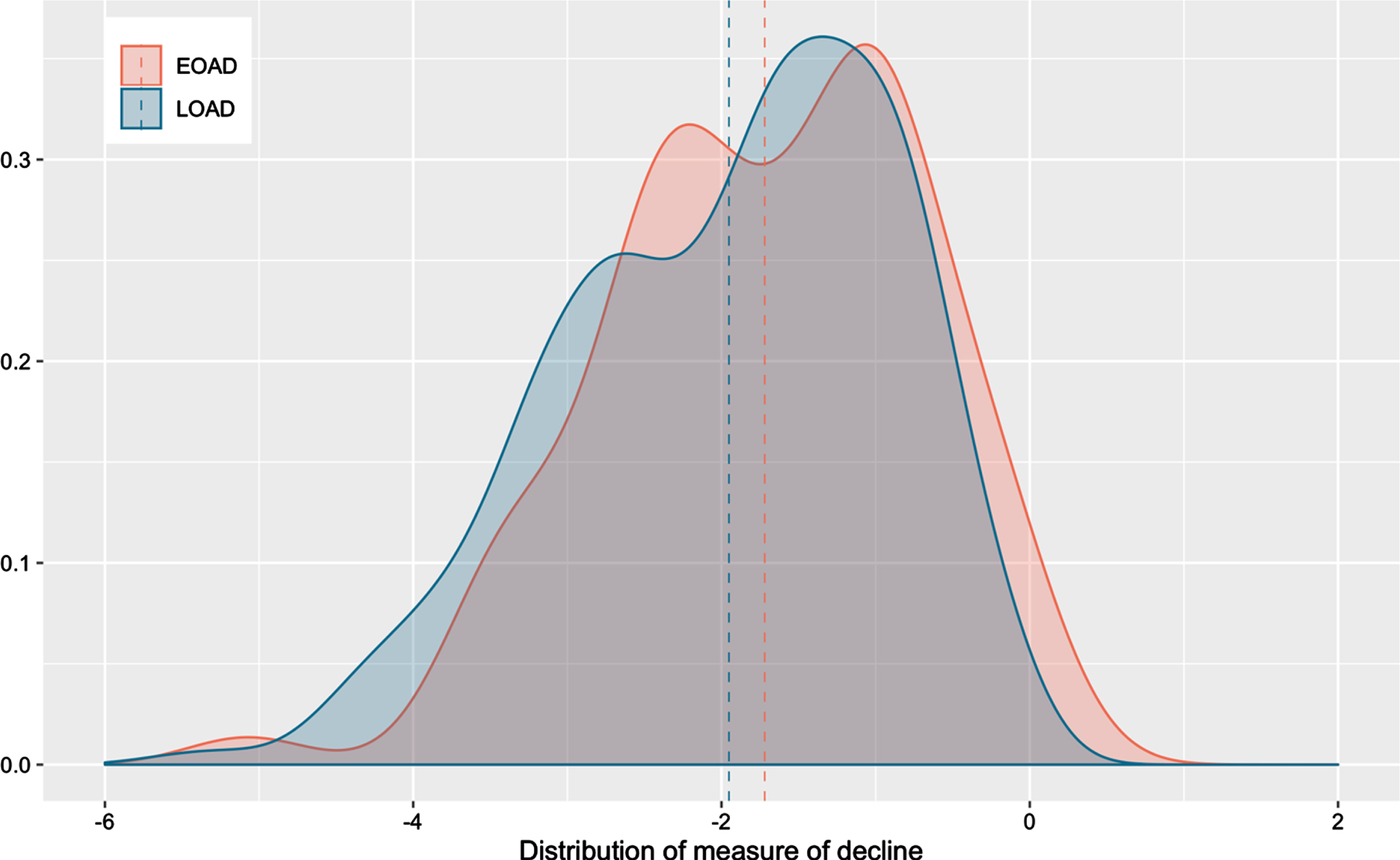
Density plot of random slopes derived from the model for the Cardiff Genetic Resource for AD.
Density plot of random slopes derived from the model for ADNI.
The difference in rate of decline between individuals with LOAD and EOAD was compared. Interestingly, individuals with EOAD seem to decline slower than individuals with LOAD, although the difference is not statistically significant (β= –0.158, p = 0.307). These results are illustrated in Supplementary Figure 3.
Association of cognitive decline with APOE
The purpose of this analysis was to determine whether APOE is a significant predictor of the rate of cognitive decline. As above, the measure of decline used here was derived from the optimal mixed effect linear model. The number of APOE ɛ2 and ɛ4 alleles was not associated with progression in this analysis (p-values 0.938 and 0.423, respectively). This result is also illustrated in Supplementary Figures 5 and 6.
Replication
The publicly available ADNI dataset was used to replicate the analyses described above. The demographic characteristics of the dataset are illustrated in Table 2.
Cohort characteristics of ADNI dataset
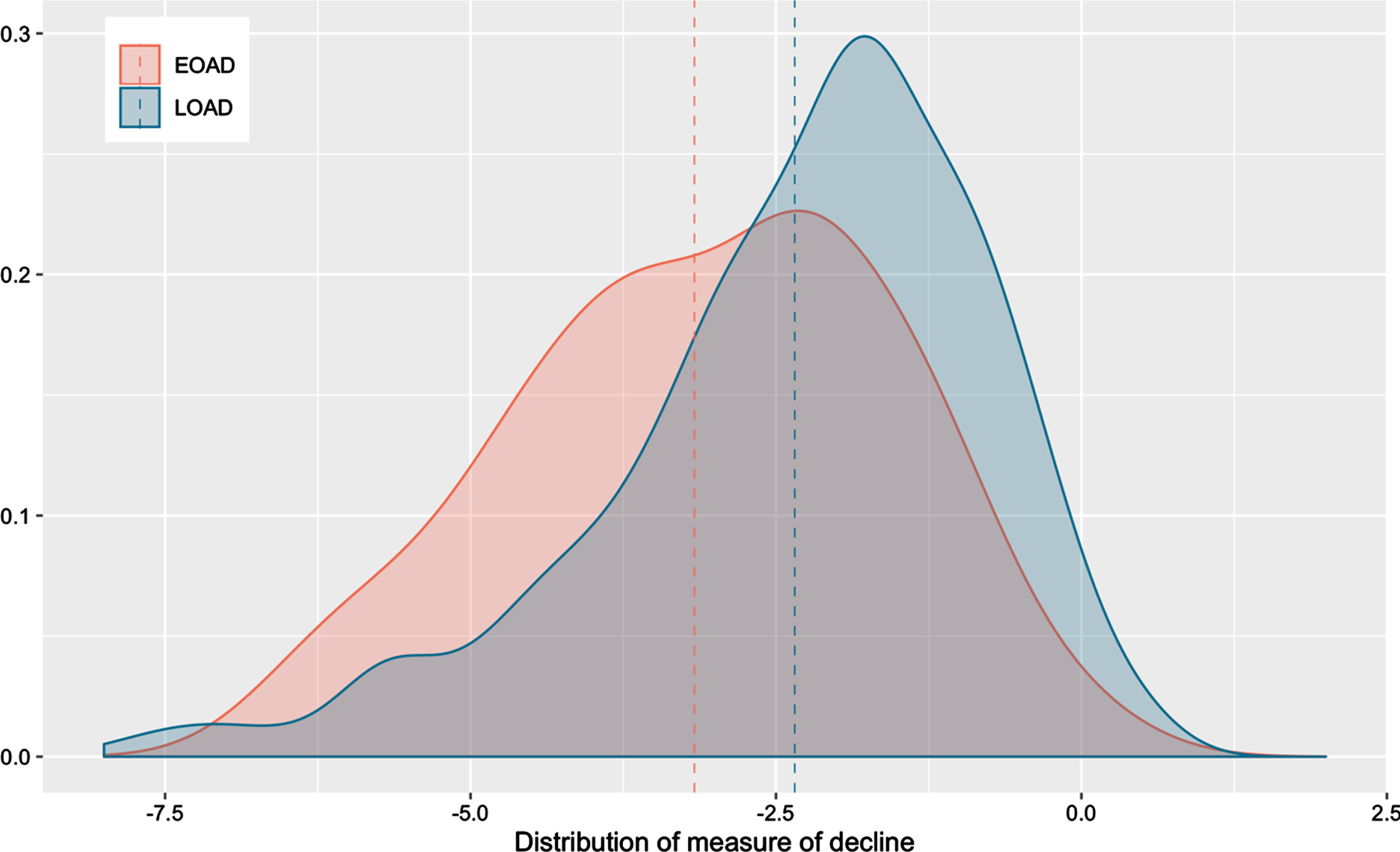
The distribution of measures of decline is illustrated in Fig. 2.
In this dataset, cognitive decline was more rapid in individuals with EOAD than individuals with LOAD, contrary to what was previously indicated using the Cardiff Genetic Resource for AD (β= 0.154, p = 0.025). These results are illustrated in Supplementary Figure 9.
The association of the number of APOE alleles was tested using linear regression. The number of APOE ɛ4 and ɛ2 alleles was not significantly associated with the measure of decline (p-values 0.689 and 0.052, respectively). The results are illustrated in Supplementary Figures 10 and 11. Table 3 summarizes the effect of APOE genotype on cognitive decline for both datasets examined.
Association of APOE genotype with cognitive decline for both cohorts
DISCUSSION
The aims of the project were 1) to identify potential confounders to cognitive decline and establish an adequate measure of assessing cognitive decline in patients with AD; and 2) to examine the association of the rate of decline with APOE, the strongest genetic risk factor for developing AD. Linear mixed effects models were selected as a method of assessing decline in our dataset as they can substantially tolerate the variance in datapoints commonly seen in population cohorts. MMSE score was utilized as a measure of cognitive function in this study as it was the assessment most widely documented in our cohort. Multiple models using MMSE as the dependent variable were assessed and the most parsimonious model with the best fit for this dataset was selected. The model selected included age at assessment, gender, and disease duration as fixed effects, and age at assessment and disease duration as random effects. Random slopes of disease duration were extracted from this model and used in further analyses as a measure of cognitive decline. Mixed effects linear models are used in a number of studies assessing the rate of decline in AD [13, 22], as they are considered a robust method for handling longitudinal data [34]. Others have utilized different methods, including multi-task exclusive relationship models [27] and machine learning algorithms [29]. However, the measures of cognition and methods of modeling vary widely between studies, and there is no established method of assessing the rate of cognitive decline in AD.
To examine how the age at disease onset influences cognitive decline in AD, the rate of decline in individuals with EOAD and LOAD was compared. Interestingly, individuals with LOAD seem to decline slightly faster than individuals with EOAD in the Cardiff Genetic Resource for AD dataset, however this result was not significant (p = 0.307). Based on existing literature, there is a suggestion that patients with EOAD tend to deteriorate faster [39–42], although there are studies showing no association of rate of decline with age at disease onset [43], and others showing that patients with an earlier onset decline slower [44], as found in this dataset. A factor that could influence in this result is that average disease duration at recruitment was 6.32 for LOAD individuals, compared to for 8.74 EOAD. Therefore, if cognitive decline is not a linear process, it is possible that the two groups are on different phases of disease, which affect cognition differently, or even that the individuals in the EOAD group have already declined significantly at the point of recruitment, therefore they do not show much further decline as the study continues. Moreover, another important factor influencing this result is that age at symptom onset is often based on the patient’s or caregiver’s account and not on examination by a clinical professional. Therefore, the reliability of this variable is questionable. This can be problematic as the duration of the disease, defined as time from first manifestation of symptoms, is an important predictor of disease severity and progression in AD. Moreover, the sample size for the EOAD group was rather small (N = 76), therefore any results drawn from it should be interpreted with caution.
A replication of this result was attempted using the publicly available ADNI dataset, where a measure of cognitive decline was computed using the same methods as in the Cardiff Genetic Resource for AD cohort. In this dataset individuals with EOAD showed a borderline significant accelerated decline compared to individuals with LOAD (β= 0.154, p = 0.025). However, as ADNI does not include information on age at disease onset, disease duration was calculated differently for this cohort than for the Cardiff Genetic Resource for AD cohort, which may account for some of the differences in results.
The association of APOE genotype with cognitive decline was assessed. APOE is the strongest genetic predictor of AD, however its effect on cognitive decline is still debatable, with some studies showing that APOE ɛ4 alleles can lead to faster decline in AD patients [20, 21], others showing that APOE genotype has no effect on cognitive and functional impairment [23, 25], and studies even finding that APOE ɛ4 alleles can lead to slower disease course in AD [24]. In this study, APOE genotype was not found to affect the rate of decline in either of the two datasets (Table 3 and Supplementary Figures 5, 6, 10, and 11). Del-Aguila et al. found an association between the rate of cognitive decline and the number of APOE ɛ4 alleles [22]; however, their study design was different, including individuals with mild cognitive impairment (MCI) as well as AD, and the method of assessing cognition used was CDR, not MMSE. Moreover, studies looking at neuroimaging progression biomarkers using ADNI have shown an association between the number of APOE ɛ4 alleles and the markers examined [45]; however, the presence of neuroimaging findings is not necessarily correlated with the presence of a more severe clinical phenotype in individuals with AD. Therefore, combining cognitive assessments with imaging biomarkers might be beneficial for an accurate estimation of the disease progression. Finally, a link between the rate of cognitive decline in individuals with MCI and the APOE genotype has been previously examined [46, 47], and an association between the APOE ɛ4 allele and the risk of progression from MCI to the early stages of AD has been established [48, 49]. However, as the Cardiff Genetic Resource for AD did not recruit individuals with MCI, this was not investigated in this study.
This study attempted to derive a measure of cognitive decline in AD using longitudinal data of cognition in AD patients. However, in addition to cognitive decline, AD progression leads to impairment in many functional activities. Therefore, integration of assessment scales that assess activities of daily living, like IADL and CDR, in the statistical modeling might improve the accuracy of the measures generated. The measure of decline computed in this project was tested for association with APOE genotype, a well-established genetic marker of AD that was available in our cohort. There are numerous other factors that have been shown to influence rate of cognitive decline in AD patients, like educational attainment, variables associated with diet and lifestyle and deprivation indices. Addition of such variables could enhance the model fit and produce more accurate measures of decline however they would substantially decrease the sample size due to high missingness in our data, therefore we did not include them in this study.
CONCLUSIONS
To conclude, this study investigated a method of computing a measure of the rate of cognitive decline in patients with AD in the Cardiff Genetic Resource for AD and tested it for association with the strongest genetic predictor for sporadic AD, APOE. No association was found between the rate of cognitive decline in AD patients and APOE genotype in this dataset or in the replication dataset. This result raises some important questions regarding the relationship between neuropathological findings and clinical progression in AD. Replication of these results in a larger dataset might help uncover latent associations between APOE genotype and rate of decline, however research into alternative genetic drivers of cognitive decline is also crucial.
Footnotes
ACKNOWLEDGMENTS
The IK studentship was supported by Wellcome Trust. The work at Cardiff University was supported by Medical Research Council (MRC) Centre (MR/L010305/1 and MR/T04604X/1), the Dementia Research Institute [UKDRI supported by the Medical Research Council (MRC) (UKDRI-3003), Alzheimer’s Research UK, and Alzheimer’s Society], Welsh Government, Joint Programming for Neurodegeneration (JPND), The Moondance Foundation.
The data have been used in this study were provided by ADNI (National Institutes of Health grant U01AG024904) and Department of Defense (DOD) ADNI (DOD award number W81XWH-12-2-0012). ADNI is funded by the National Institute of Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association, Alzheimer’s Drug Discovery Foundation, Araclon Biotech, BioClinica, Biogen, Bristol-Myers Squibb, CereSpin, Cogstate, Eisai, Elan Pharmaceuticals, Eli Lilly and Company, EuroImmun, F. Hoffmann-La Roche and its affiliated company Genentech, Fujirebio, GE Healthcare, IXICO, Janssen Alzheimer’s Immunotherapy Research and Development, Johnson & Johnson Pharmaceutical Research & Development, Lumosity, Lundbeck, Merck & Co, Meso Scale Diagnostics, NeuroRx Research, Neurotrack Technologies, Novartis Pharmaceuticals Corporation, Pfizer, Piramal Imagining, Servier, Takeda Pharmaceutical Company, and Transition Therapeutics. The Canadian Institutes of Health Research provides funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.