
Abstract
Background:
As the demand for dementia care grows rapidly worldwide, heavy “caregiver burden” has been associated with stress and depression. Even so, standard metrics for interdisciplinary research of caregiver burden are limited.
Objective:
The objective of the present review is to recommend valid, reliable, and comprehensive self-report instruments of caregiver burden.
Methods:
A systematic review was performed using four databases, searched in April 2021. Articles that established or evaluated self-report instruments for dementia caregiver burden were included, while studies that involved non-dementia caregivers or did not clearly define caregiver burden were excluded. Established guidelines for reliability and agreement studies were used to assess quality and risk of bias. Assessments of self-report instruments were made based on reliability, validity, feasibility, and quality of psychometric evaluations, and comparative evaluations were presented in visual form using radar graphs.
Results:
Search terms yielded 1,720 articles, and 40 were included in the systematic review after excluding those of low quality. Based on the results of these studies, we recommend the Zarit Burden Interview, Screen for Caregiver Burden, Caregiver Burden Interview, and Burden Scale for Family Caregivers, due to their validity, reliability, and inclusion of multiple subjective and objective dimensions of burden.
Conclusion:
Targeting specific sources of caregiver burden can help prevent negative outcomes for both dementia patients and caregivers. Future studies should apply self-report instruments to measure and address caregiver burden longitudinally.
INTRODUCTION
In 2011, President Obama signed the National Alzheimer’s Project Act (NAPA) into law, and the resulting National Plan to Address Alzheimer’s Disease has named support and services for “family members and other unpaid caregivers” as one of five foundational goals [1]. The World Health Assembly has released a “global action plan for dementia,” naming the “development of supportive environments for carers” one of four areas of focus [2]. Today, dementia is the most prevalent condition that necessitates caregivers in societies across the world [3]. Dementia caregivers spend significantly more hours per week and assist with more activities and instrumental activities of daily living (ADL and IADL) on average than non-dementia caregivers, due to the insidious cognitive and functional decline associated with dementia [4].
With the heavy and unique demands of dementia caregivers, a family- and caregiver-centered approach is necessary to optimize dementia care. For “informal,” unpaid caregivers, caregiver burden has been considered the “best recognized marker” of stress in addition to depression and has even been found to mediate the association between “patient problem behaviors” and caregiver depression [5]. For people with dementia in many cultures, informal caregivers are an “ongoing support system,” with a role so significant that caregiver burden has been found to correlate with health outcomes of care recipients, such as institutionalization and survival rates [6]. Furthermore, the psychological needs of a dementia caregiver have been found to correlate inversely with the extent to which a dementia patient can stay active [7]. In line with these findings, the WHO deems the needs of family caregivers a primary objective in palliative care, and healthcare professionals have increasingly come to see the “unit of care” as the family, not only the patient [2].
Standard definitions of “caregiver” and “caregiver burden” are necessary for a meaningful review of this crucial topic. Theoretical models for studying the needs, stress, and consequent burden of caregivers have evolved since the earliest work by nursing and gerontology researchers in the 1970s [8]. In 1980, the Zarit Burden Index (ZBI), which measures burden quantitatively as a “unidimensional variable,” was developed, and it remains one of the most frequently utilized self-reported caregiver burden instruments today [7]. From the 1980s onwards, metrics have been developed based on more nuanced theoretical frameworks, such as the “stress-appraisal-coping model.” This model considers caregiver burden an “outcome variable,” which is caused by “stressors,” such as nocturnal wandering and continence difficulties [8], and is modulated by individual caregivers’ coping mechanisms [7]. It has also been called a “transactional model of stress,” as it describes the modes of exchange between an individual and his/her environment [8]. Applied to dementia caregiving, the stress-appraisal-coping model illustrates a significant shift from a medical approach, which prioritizes diagnosis and biological treatment, to a psychosocial one, which allows greater understanding of community-based care [8]. The model also highlights the significance of self-report instruments, which permit caregivers to voice their psychosocial experiences in a systematic, academically and clinically useful way.
Schoenmakers et al. proposed that caregiver burden is a “multidimensional biopsychosocial reaction to the demands of care in relation to the personal time, the social roles, the physical and emotional states, the economic and supportive resources of caregivers, as well as the other multiple roles that they have to fulfill” [9]. This description captures the complexity of caregiver burden and highlights several important points. First, it is a “reaction” to caregiving demands, and as such, filtered through the unique background, experience, and identity of each caregiver. To thus predict the reactive nature of caregiver burden, Conde-Sala et al. describe “stress process model,” which is composed of “contextual variables” that predispose, “primary stressors” that relate to disease or condition, and “secondary stressors” from other aspects of caregiving [10]. Second, caregiver burden is “multidimensional,” and factors related to caregiving, whether contributing to or resulting from it, can be social, psychological, financial, or physical [11]. Third, considerations of caregiver burden should take a holistic, person-centered approach, recognizing that caregivers fill “multiple roles” outside of their relation to the care recipient. Over time, multiple authors have developed an increasingly precise system for describing caregiver burden, consolidated in Fig. 2.
“Caregiver burden” was added as a MeSH term in 2020. As research regarding this important topic proliferates, standards for the instruments used to measure it have yet to be established. In particular, researchers, clinicians, and caregivers themselves may find metrics of caregiver burden specific to dementia to be helpful, but they have not yet been reviewed. Deeken et al. wrote a comprehensive review of self-report instruments for the needs and quality of life of caregivers in 2003 but did not consider dementia-specific metrics [7]. Zacharopoulou et al. reviewed measurement tools for dementia-specific measures of caregiver quality of life in 2015 but did not include metrics of caregiver burden or offer specific recommendations for which measures to use [12].
To fill in this research gap, this review will summarize the strengths and limitations of self-report instruments that are most appropriate to the burden of dementia caregivers. We aim to answer the question: which self-report instruments for dementia caregiver burden are the most valid, reliable, and comprehensive? The purpose of this work is to offer dementia researchers and care providers a set of practical recommendations, to advance the study of and interventions for the burden of dementia caregivers.
MATERIALS AND METHODS
Search strategy
Four databases widely used in the health sciences, PubMed, Embase, PsycINFO, and Web of Science, were searched for relevant articles. The search was last conducted on April 28, 2021 by two reviewers (JT and GJ) independently, and selected articles from database and manual search were published from 1983 to the present (2021). On PubMed, a comprehensive search was performed using MeSH terms as follows: ((((“Caregivers/psychology”[Mesh]) OR “Family”[Mesh] OR “Home Nursing/psychology”[Mesh]) AND (“Dementia”[Mesh] OR “Alzheimer Disease”[Mesh])) AND (“Nursing Assessment/methods”[Mesh] OR “Surveys and Questionnaires/methods”[Mesh] OR “Surveys and Questionnaires/standards”[Mesh] OR “Needs Assessment”[Mesh] OR “Self-Assessment”[Mesh] OR “Psychological Tests”[Mesh] OR “Psychometrics/methods”[Mesh])). On Embase, the search was performed using Emtree headings as follows: (‘caregiver burden’/exp OR ‘caregiver burden’) AND (‘dementia’/exp OR ‘dementia’) AND (‘self report’/exp OR ‘self report’ OR ‘self evaluation’/exp OR ‘self evaluation’ OR ‘psychometry’/exp OR ‘psychometry’). On PsycINFO, the search terms were: (MeSH Subject Heading) dementia AND (All Text) “caregiver burden” AND (Word in Major Subject Heading) psychometrics OR validity OR reliability. On Web of Science, the search was performed using: (Topic) “caregiver burden” AND dementia AND (Abstract) instrument OR psychometric.
Qualitative studies, cross-sectional studies, cohort studies, longitudinal studies, and case-control studies that established or evaluated self-report instruments for dementia caregiver burden were included. Intervention studies that did not evaluate the validity or reliability of the metrics they used, as well as studies of caregivers for people without diagnosed dementia, were excluded. Metrics that did not explicitly state “burden” as part of their titles were included if they assessed both objective (i.e., quantifications of straining tasks and circumstances) and subjective (i.e., specific experiences and perceptions) aspects of caregiving burden. Examples of instruments that were thus included in review were the Family Distress in Advanced Dementia scale and the Kingston Caregiver Stress Scale. By contrast, metrics that assessed “hassles,” “problems,” “quality of life,” “wellness” or “wellbeing,” depression, anxiety, guilt, and attitudes, focusing on subjective or objective domains but not both, were excluded.
Data collection and quality assessment
All titles and abstracts were independently assessed by two reviewers (JT and GJ). Full-text copies of potentially relevant reviews were then obtained and assessed for inclusion by two reviewers independently. Disagreements regarding initial assessment were discussed and resolved with a third reviewer (YC).
The quality of each included study was assessed by two reviewers independently (JT and GJ), using Kottner et al.’s guidelines for reliability and agreement studies [13]. The guidelines include 14 points, including factors that contribute to risk of bias such as sampling method, missing data, independence of rating processes, and sample characteristics. Missing data was most likely not at random, but rather due to selection bias and the sensitive nature of caregiver burden. It can be assumed that some caregivers would be reluctant to express subjective caregiver burden for personal reasons, including feelings of guilt. Of note, certain safeguards against bias, i.e., randomization, allocation concealment, blinding, were not feasible or relevant, given the nature of self-report instruments. Based on quartiles of resulting quality assessment scores, it was decided that studies scoring 8 or below were of low quality, 9–10 were of moderate quality, and 11 to 14 were of high quality. Studies of low quality were excluded from review and synthesis (Fig. 1).
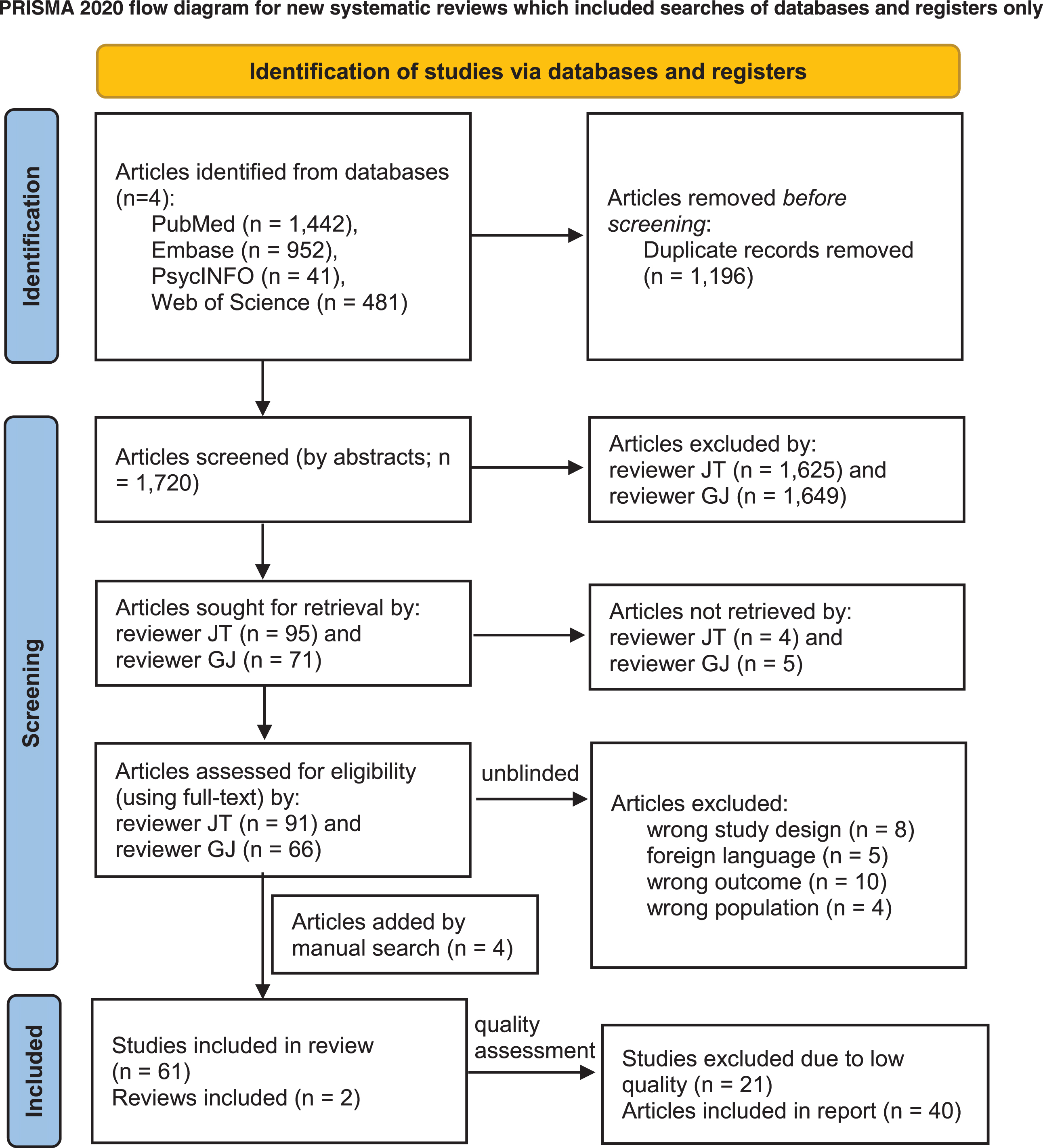
Process of selecting articles for review. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71
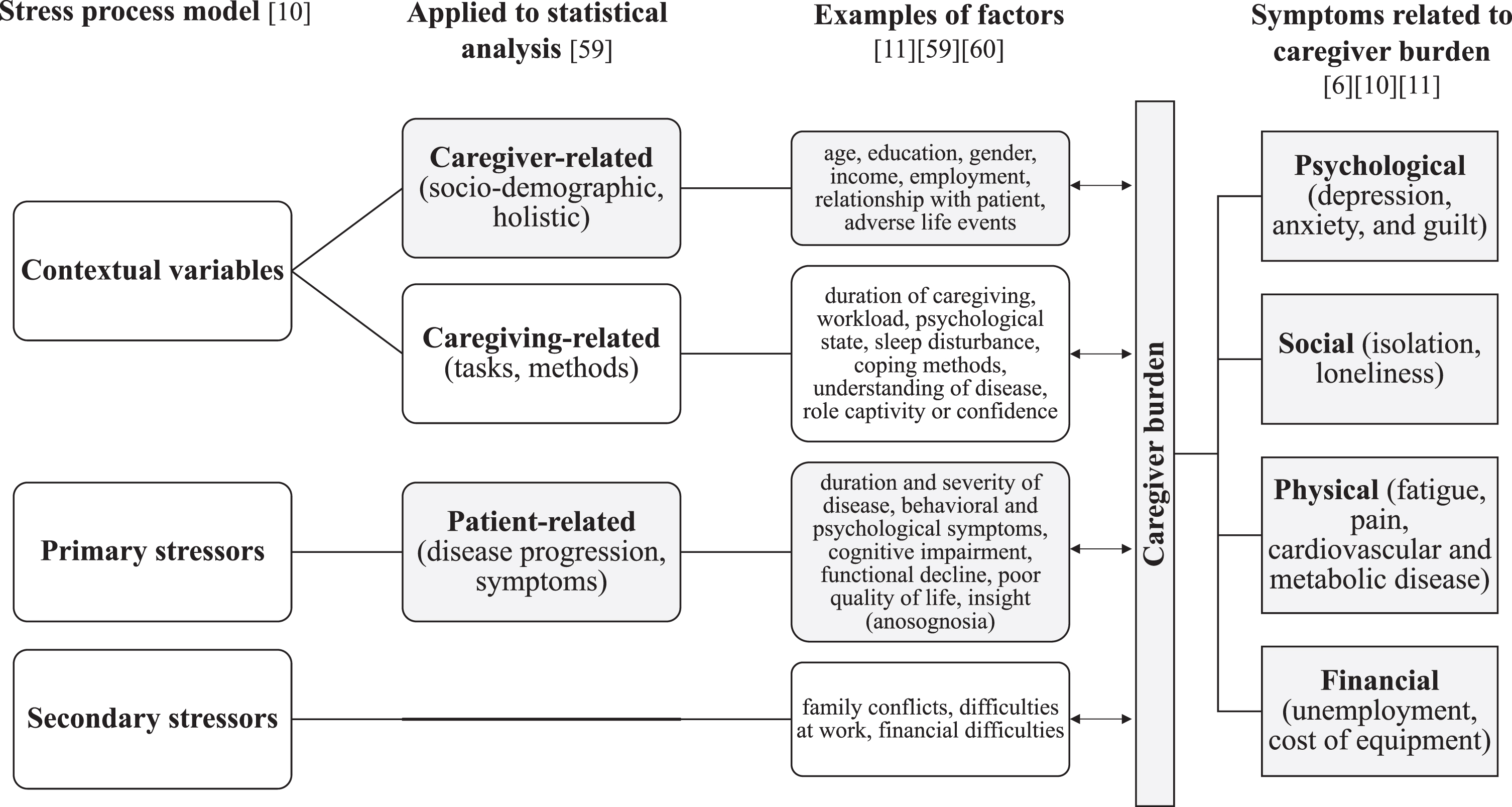
Summary of models for studying caregiver burden.
Data extraction was undertaken by two reviewers independently (JT and GJ). A customized data extraction form was used to manually extract the following information: burden instrument, references, psychometric test population, items and format, number of factors or subscales, validity, and reliability. Several of these variables were consistent with each outcome domain specified in the study’s objectives: validity, reliability, and comprehensiveness (represented by number of factors or subscales). For synthesis, included studies were grouped by the self-report instrument that they evaluated. Some self-report instruments lacked a moderate-high quality study reporting its validity, reliability, or factor analysis. These instruments were given a score of “0” in the domain for which there was no reported value. Two independent reviewers (JT and GJ) conducted all levels of data abstraction and quality appraisal with a third arbitrator (YC) to settle discrepancies.
Data synthesis
Assessments of self-report instruments were made based on four main properties: reliability, validity, factor analysis, and expedience. First, reliability was defined as the logical correlation of results between responses of a single subject over time (internal consistency reliability, reported as Cronbach’s alpha) and/or between subjects (inter-rater reliability, IRR). Second, validity included the relevance of items to the subject population (face and content validity), correspondence with other metrics (convergent, also called criterion, validity), and sensitivity to subgroups within a population (construct validity) [14]. Third, multidimensionality involved the inclusion of both objective and subjective items, such as the categorical tasks required due to caregiving and the individual appraisal thereof [15], in addition to explicit subscores from the instrument or demonstrations of more than one factor from factor analysis. To some extent, multiple factors contributed to construct validity. Fourth, expedience was assessed by the number of items and relative time needed to administer the instrument. Medical teams, public health researchers, and other professionals can consider which of these four factors (reliability, validity, objectivity and subjectivity, and expedience) should be prioritized when choosing the instrument most suited to their clinical or academic goals.
Measures of validity and reliability varied between studies, and assessments of multidimensionality and expedience were qualitative in nature. As a result, meta-analysis and sensitivity analyses, as well as analysis of reporting bias (e.g., publication bias) and certainty of evidence, were not applicable. Instead, to facilitate comparisons of the reviewed self-report instruments’ performance in each of these four domains, radar graphs were composed. To create these graphs, the ZBI was set as the norm of “1,” such that “1” represented: for “Validity,” the establishment of both content and criterion validity; for “Reliability,” a Cronbach alpha of 0.71 to 0.93; for “Multidimensionality,” a single score with multiple factors found in analysis; and for “Expedience,” 22 Likert scale-type items. Values greater than 1 on the radar graph axis indicate strengths of an instrument compared with the ZBI, and values less than 1 indicate relative weaknesses.
RESULTS
Selected articles
Figure 1 shows the process of selecting the articles for review. A total of 1,720 articles were identified, of which 61 articles were selected for quality assessment and data extraction. An example of a study that might appear to meet the inclusion criteria, but was actually excluded, was a systematic review of the relationship of specific items on the Neuropsychiatric Inventory to caregiver burden in dementia. This was excluded because, while it did describe metrics of caregiver burden in terms of associations with neuropsychiatric symptoms, the review’s objective was not to establish reliability, validity, or other quality assessments of caregiver burden instruments. Manual search based on bibliographies of related review papers yielded an additional four articles.
Abbreviations of self-report instruments and other terms used in this article
The Zarit Burden Interview
To date, several instruments have been developed to measure caregiver burden and demonstrated psychometric validity and reliability in multiple studies, differentiation of factors contributing to burden rather than a unidimensional “summary score,” and feasibility in terms of time and staff required to administer, record results of, and analyze data. The 22-item ZBI has been by far the most extensively used metric for caregiver burden, takes less than 10 minutes to complete, and has been shown in multiple recent studies to have excellent internal consistency and inter-rater reliability, across caregiver gender and educational levels [16]. However, it was not formulated specifically for the context of dementia and has been criticized for addressing burden as a “unidimensional variable” that conflates objective and subjective measures [7].
Table 2 and Supplementary Table 1 shows data from the studies of moderate-high quality that evaluate ZBI’s reliability and validity. Cronbach’s alpha, a measure of internal consistency, ranged from 0.71 to 0.93. Validated translations include Japanese, Mandarin Chinese, Cantonese, Thai, Portuguese, Italian, Spanish, and Turkish. Many authors of studies in countries outside the United States have suggested that the ZBI may be useful for “cross-cultural comparison,” showing differences that may be attributed to values such as filial obligation in Taiwan [17, 18]. The most frequently validated abbreviated versions that show acceptable reliability include the 4-item ZBI, which may be used for rapid, community-based screening [19, 20], and the 12-item ZBI, which offers another abridged version for ease of clinical use [20–24]. Despite the ZBI’s single score output, studies have used exploratory and confirmatory factor analysis to show that it assesses multiple factors. The number of factors that account for variation of ZBI scores in any given population has ranged from two to six. Commonly occurring factors include “personal strain” and “role strain,” which describe “the impact of providing care on the life partner (e.g., health problems and lack of privacy)” and the perception of being unable to perform the caregiving role to the best of one’s ability, respectively [25]. These findings suggest that the evidence supporting use of the ZBI is growing in varied clinical and cultural contexts.
Summary of psychometric studies evaluating the Zarit Burden Interview (ZBI)
aReliability shown by Cronbach’s alpha for internal consistency, unless otherwise stated.
Other self-report instruments of dementia caregiver burden
In addition to the ZBI, we found fourteen self-report instruments for dementia caregiver burden that had been validated by moderate- to high-quality studies: the Caregiver Burden Inventory (CBI), Cost of Care Index (CCI), Caregiver Strain Index (CSI), Screen for Caregiver Burden (SCB) and its short version, Caregiving Burden Scale, Impact of Caregiving (IOC) Inventory, Caregiver-Perceived Burden Questionnaire (CPBQ), Care-EOD (Early Onset Dementia), Impact of Alzheimer’s Disease on Caregiver Questionnaire (IADCQ), Burden Scale for Family Caregivers (BSFC) and its short version, Thai dementia patients’ caregiver burden (Thai-DCAB) scale, Family Distress in Advanced Dementia scale, Kingston Caregiver Stress Scale (KCSS), Montgomery Borgatta Caregiver Burden Scale (MBCBS), and Dementia Burden Scale-Caregiver (DBS-CG).
Comparing strengths of self-report instruments
Table 3 and Supplementary Table 2 show data from the studies of moderate-high quality that evaluate each of these instrument’s reliability and validity. Figure 3 uses radar graphs to visually display the strengths of each reviewed instrument in four categories, relative to the ZBI. Three instruments were notable for their consistent validity across studies, multidimensionality, and accessibility.
Summary of psychometric studies evaluating other dementia caregiver burden self-report instruments
Please see Supplementary Table 1 for abbreviations. aReliability shown by Cronbach’s alpha for internal consistency, unless otherwise stated. Figures rounded to two decimal places. bCaregivers’ Assessment of the Patient (CAP) and the Caregivers’ Assessment of Themselves (CAT).
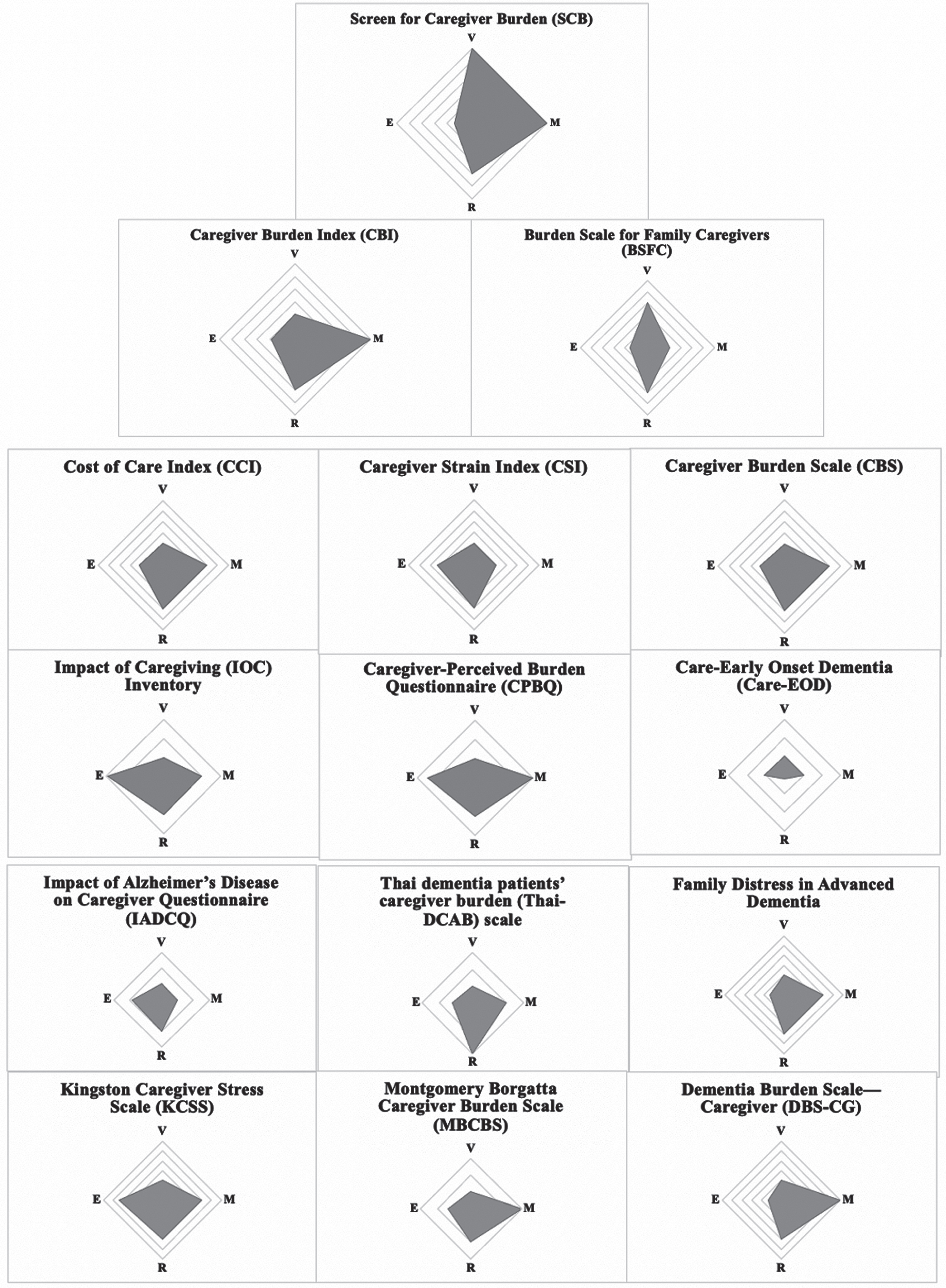
Subjective summary of strengths for metrics of burden of caregivers for people with dementia, relative to the Zarit Burden Interview (ZBI). E, expedience (number of items and mean time to administer); V, validity (content, criterion, and/or construct); M, multidimensionality (number of explicit subscores or extrapolated factors); R, reliability (internal consistency and/or test-retest). Each metric was compared with ZBI, such that a value of “1” represented: (E) 22 Likert scale-type items, (V) establishment of both content and criterion validity, (M) a single score with multiple factors found in analysis, (R) Cronbach alpha of 0.71 to 0.93. The maximum value represented by each radar graph axis, i.e., the outermost gridline, is 2. Values greater than 1 on the radar graph axis indicate strengths of an instrument compared with the ZBI, and values less than 1 indicate relative weaknesses.
Three notable self-report instruments
The Screen for Caregiver Burden
The 25-item SCB and its shortened 7-item version were developed and validated using three separate trials and population samples, which included longitudinal data to support content, construct, and criterion validity. Cronbach alpha for overall internal consistency has been reported to be about 0.89 for the full 25-item version and 0.82 to 0.86 for the 7-item [26–28]. The SCB was specifically designed for spouses of people with Alzheimer’s disease (AD) dementia but has also been applied more broadly to caregivers of people with dementia. It includes six domains in three categories, in order to more precisely correspond to the behavioral and functional problems associated with AD: patient domains cover cognition concerns (e.g., asks repetitive questions) and behavior (e.g., drives when shouldn’t, gets lost); caregiver domains cover social (e.g., feeling alone), emotional (e.g., embarrassed, frustrated), economic (e.g., seeking public assistance), and physical (e.g., chores, keeping an orderly household) concerns. Studies have noted that the SCB was able to show differences in burden between caregivers and controls, despite matching demographic, physical health, and psychological distress variables, suggesting that it detects burden as “a distinct psychological condition, which a broader, more generic instrument may not be able to do” [29].
The Caregiver Burden Inventory
Like the SCB, the 24-item CBI provides multi-dimensional subgroup scoring [30]. Cronbach alpha for overall internal consistency is about 0.91, with values for each factor ranging from 0.79 to 0.93 [31, 32]. The CBI has been validated in various languages in the United States, Italy, Iran, and Taiwan. Five factors have emerged from analysis: emotional or psychological, time-dependence, physical, developmental, and social [32]. The CBI has been used to construct a more nuanced Caregiver Burden Profile [33].
Compared with the ZBI, the CBI more explicitly offers multi-dimensional subgroup scoring. Novak & Guest developed the CBI and applied it to visually depict and compare burden scores across 107 individual caregivers [33]. Using the CBI made it possible to precisely examine differences in caregiver burden, rather than reporting only a total burden score. For example, in cases where a low global burden score could mask significantly elevated subscale scores, a multidimensional measure like the CBI enables targeted interventions toward individual caregivers’ specific needs.
The Burden Scale for Family Caregivers
The 28-item BSFC and its shortened 10-item version have been validated among a sample of 351 family caregivers of community-dwelling dementia patients and shown to have a Cronbach’s alpha of 0.93 and 0.915, respectively. Factor analysis yielded a single-factor structure. The authors who developed the BSFC describe three advantages of the scale compared to the ZBI. First, the ZBI has only 4 inverse items, whereas the BSFC has 11. Thus, the BSFC reduces the risk of response bias. Second, while all ZBI items are directly related to the care-receiver, the BSFC also covers aspects of burden that do not directly refer to the caregiver’s contact with the care-receiver, such as the caregiver’s wish ‘to run away’ from the caregiving situation. Third, the BSFC is freely available in 20 languages (https://www.caregiver-burden.eu.
DISCUSSION
Summary and application of main findings
To assess self-report instruments of dementia caregiver burden and generate specific recommendations for future clinical and research use, data regarding their psychometric properties were extracted from moderate-high quality psychometric studies. The ZBI, SCB, CBI, and BSFC were recommended as self-report instruments for dementia caregiver burden based on reliability, validity, multidimensionality, and expedience.
These comprehensive tools can help elucidate important culture-dependent factors that differentiate how caregivers internally perceive and externally express burden. These insights can then be applied to more holistic, family-centered interventions. For instance, in East Asian countries where dementia is often accepted as “fate” or “heaven’s will,” family members may more easily accept their duty to provide care, preventing denial or guilt on one hand, but resulting in less willingness to seek help on the other [35]. This trend is rapidly changing with cultural shifts and globalization, however. In China and Taiwan, the Confucian principle of filial responsibility may have led to caregivers being predominantly children of people with dementia, in addition to spouses [36]. In these societies, grown children have had to balance filial piety with professional demands, and an increasing number are employing foreign paid caregivers for full-time assistance. In fact, it has been estimated that 64% of Taiwan’s long-term care is provided by such workers, predominantly from Southeastern countries like Indonesia, Vietnam, and the Philippines [37]. However, full-time help has been found in several studies to alleviate burden among family caregivers in Italy, but not in Taiwan [38]. This may be attributed to the value of filial piety.
To investigate this hypothesis, the ZBI, SCB, CBI, or BSFC can help evaluate subjective and objective caregiver burden across cultures, as well as between family, unpaid, and foreign paid caregivers. The ZBI is a good choice for cross-cultural comparison due to its widely used, validated translations, as well as its abbreviated versions, which facilitate rapid community screening use. It has also been found to assess multiple factors, and thus could be useful across various caregiver types. On the other hand, both the SCB and BSFC are dementia-specific; the SCB was designed for spousal caregivers, and the BSFC was designed for family caregivers. Such specificity may allow for interventions precisely targeted toward the populations of interest. However, the BSFC only assesses a single factor, while the SCB and CBI are multidimensional and may better distinguish individual caregivers’ specific needs. Overall, for its multidimensionality and cross-cultural validity, the ZBI may be best for assessing and comparing burden among unpaid family caregivers and paid foreign domestic workers.
For researchers, the use of such instruments is crucial to understanding both cross-cultural patterns and experiences specific to caregivers in local communities. They should offer a way to describe individuals’ experience systematically and quantitatively, while maintaining meaningful, qualitative insight. For healthcare professionals, partnering with informal and formal dementia caregivers is crucial to ensuring the best quality care, and measuring caregiver burden can not only improve caregivers’ psychological health, but also prevent negative outcomes, such as elderly abuse and institutionalization. For the general public, including policymakers, businesses, and consumers, understanding the burden and needs of dementia caregivers is also very important. “Dementia-friendly initiatives” have been promoted across countries by organizations, such as Alzheimer’s Disease International and its affiliates, as part of a movement toward empowerment and inclusion of not only people with dementia but their caregivers. Such programs can benefit all sectors of society.
However, self-report instruments for burden of dementia caregivers should be used with caution, particularly with respect to three issues. First, measures of burden should be used as a supplement rather than a convenient “single-assessment” in understanding each dementia caregiver’s experience [8]. Second, researchers should take care to address the “reluctance” and even “unwillingness” of dementia caregivers to explicitly acknowledge their caregiving burden [38], which directly impacts the criterion validity of each administration. Third, the purpose of measuring caregiver burden is to develop services and interventions based on observed results, which requires sensitivity and comprehensiveness in developing “individual profiles” of caregivers [8]. Beyond personalized attention to each caregiver, the next challenge is to scale such interventional programs to the community level.
Strengths and limitations
This study has several strengths. First, since the subject of dementia caregiver burden is relevant to multiple disciplines, including medicine, psychology, social work, and nursing, we decided to search PubMed, PsycINFO, Embase, and Web of Science. This allowed for a wider breadth of articles and more comprehensive assessment of existing self-report instruments. Second, quality of articles was assessed using established guidelines for reliability and agreement studies, allowing for a more standardized approach to exclude those of low quality [13]. Third, self-report instruments were assessed based on reliability, validity, multidimensionality, and expedience, with each characteristic displayed on radar graphs for easy comparison. Fourth, all quality assessment and analysis were conducted by two independent reviewers, with study design and supervision by experts in the field of epidemiology, medicine, and specifically dementia care.
This systematic review had certain strengths, but also limitations to the methods used. The process of evaluating and recommending the most suitable self-report instruments was subjective and relied on comparisons with the most frequently used instrument, i.e., the ZBI. Furthermore, the selected studies included in synthesis, showing the relative strengths of the recommended self-report instruments, were conducted across multiple countries, introducing variability in cultural, geographic, and other factors. Only studies published in English were included, introducing potential language bias. With these limitations to the review in mind, researchers and clinicians should use the provided radar graphs as a starting point, and then examine the items and structure of each instrument to choose one that is most suitable to their objectives.
There were certain limitations to the evidence included in this systematic review. First, an important caveat for interpreting our study is that most of the articles reviewed were cross-sectional studies. Due to the progressive nature of dementia and the resulting need for longitudinal studies to assess its effects over time, future studies should follow up with subjects to elucidate specific sources of caregiver burden, develop interventions targeting them, and evaluate their efficacy with greater validity and reliability. Such studies can be repeated in different cultural contexts over a longer period of time to elucidate what modifiable factors can be targeted for the greatest long-term benefits.
Second, the conceptualization and assessment of caregiver burden reviewed here are mostly limited to unpaid, informal caregivers. Zacharopoulou et al. add that such caregiving is “based on ties of affinity and emotional connection,” with no defined hours or time constraints [12]. In the United States, approximately 80% people with dementia receive informal, at-home care from family members, and clinicians generally believe that patients wish to remain at home as long as possible, such that early nursing home placement is considered a poor health outcome [6, 40]. By contrast, formal caregivers or foreign paid caregivers, such as those who have traveled from Indonesia, the Philippines, Thailand, and Vietnam to Taiwan [14], are becoming the main caregivers of people with dementia in many societies. Most studies in this review involve informal caregivers, who are unpaid and care for community-dwelling people with dementia. Variables associated with formal or foreign paid caregivers include differences in language and culture, as well as emotional support; these unique factors warrant further research.
In conclusion, caregiver burden is an increasingly used term to describe the psychosocial outcome of stress associated with providing care on a regular basis. Given its complex nature, particularly among caregivers of people with dementia, self-report instruments are a necessary tool to determine the nature of caregiver burden and opportunities for intervention. Based on a systematic review of 40 studies that assessed the reliability and validity of eighteen instruments, the ZBI, SCB, CBI, and BSFC are recommended due to their unique strengths.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Mr. Yu-Hong Lin, MSW, for his advice on what directions of research to pursue and his insights regarding dementia care from clinical and social perspectives. The authors received no financial support for the research, authorship, and/or publication of this article.