
Abstract
Background:
Several studies have shown increased levels of cerebrospinal fluid (CSF) synaptosomal-associated protein 25 (SNAP-25) in patients with Alzheimer’s disease (AD). However, results have been inconsistent thus far.
Objective:
We conducted meta-analyses summarizing the associations of CSF SNAP-25 levels with AD to assess the utility of SNAP-25 as a novel biomarker for AD.
Methods:
We conducted a meta-analysis of differences in CSF SNAP-25 levels in patients with AD or mild cognitive impairment (MCI) and in cognitively healthy controls (HC). We calculated pooled correlation coefficients comparing SNAP-25 levels and total tau (T-tau) or hyperphosphorylated tau (P-tau) in CSF.
Results:
Eight studies enrolling 1,162 individuals (423 AD, 275 MCI, 464 HC) were included for quantitative analysis. Patients with AD (ratio of means [RoM] = 1.50, 95% confidence interval [CI]: 1.30,1.74) and MCI (RoM = 1.45, 95% CI: 1.12,1.87) had increased levels of CSF SNAP-25 as compared to HC. The difference in CSF SNAP-25 levels when comparing AD and MCI (RoM = 1.05, 95% CI: 0.96,1.14) was not statistically significant but showed a trend toward significance. Statistically significant correlations were found when comparing CSF SNAP-25 with CSF T-tau (Spearman correlation coefficient, ρ=0.78; ρ=0.66; ρ=0.69, respectively) and P-tau (ρ=0.77; ρ=0.70; ρ=0.62, respectively) levels in patients with AD, MCI, and HC.
Conclusion:
Increased CSF SNAP-25 levels differentiated patients with AD or MCI from controls, suggesting the utility of this biomarker in the early diagnosis of AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a common neurodegenerative disease characterized by progressive cognitive decline and behavioral impairment in the context of complex and heterogeneous pathophysiology [1]. The major pathological features of AD include neuritic amyloid-β (Aβ) plaques, intracellular neurofibrillary tangles, neuronal degeneration, and synaptic loss [2]. Synapse loss is an early event that precedes the clinical manifestations of AD as well as even the early accumulation of Aβ plaques in AD brains and is more highly correlated with cognitive impairment than plaques or tangles [3, 4]. Several core cerebrospinal fluid (CSF) biomarkers, including Aβ42, total tau (T-tau), and hyperphosphorylated tau (P-tau), have been established for the diagnosis of AD in clinical practice. Biomarkers detecting synaptic loss and dysfunction, however, are still under development [5].
Synaptosomal-associated protein 25 (SNAP-25) is a presynaptic protein that is involved in the formation of the soluble N-ethylmaleimide-sensitive factor attachment protein receptor complex [6]. Combined with vesicle-associated membrane protein 2 and syntaxin-1, SNAP-25 mediates the fusion of synaptic vesicles with the presynaptic plasma membranes triggered by Ca2 + during neurotransmitter release and plays a significant role in vesicular exocytosis, neurite outgrowth, and long-term potentiation [7, 8]. SNAP-25 is highly expressed in the central nervous system, and its involvement in the physiological processes of synaptic vesicle recirculation, synaptogenesis, axon extension, and neuronal repair has been reported [9, 10]. Some studies have reported decreased levels of SNAP-25 in multiple brain regions within AD [11–13]. Moreover, some studies in recent years have reported that CSF SNAP-25 concentrations in patients with AD or mild cognitive impairment (MCI) are statistically significantly increased compared with that noted in controls [14–16]. Studies have also shown that increased CSF SNAP-25 levels may be predictive in the genesis and progression of AD, suggesting SNAP-25 as an auspicious biomarker for reflecting synaptic degeneration and synaptic loss [16, 17]. In addition, CSF SNAP-25 levels have shown good correlations with CSF tau levels [14–16, 18], a known biomarker for AD, in several studies. However, the results of relevant studies have been inconsistent and, to our knowledge, no meta-analysis has been performed assessing the correlations between CSF SNAP-25, AD occurrence, AD progression, and various aspects of AD presentation. Consequently, in the current study, we conducted a meta-analysis of differences in CSF SNAP-25 levels between AD, MCI, and cognitively healthy controls (HC) as well as the associations of CSF SNAP-25 levels with CSF T-tau and P-tau levels to assess the utility of CSF SNAP-25 as an alternative biomarker for AD. We hypothesized that our findings would support the efficacy of CSF SNAP-25 as a biomarker with utility in AD diagnosis and in the monitoring of AD progression.
MATERIALS AND METHODS
We conducted meta-analyses according to PRISMA (the Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines [19]. Ethics review is not necessary for meta-analyses of the published literature.
Search Strategy
Using the search terms “synaptosomal-associated protein 25”, “SNAP-25”, “Alzheimer’s disease”, and “mild cognitive impairment,” we performed online searches of the PubMed, Web of Science, Embase, and Cochrane Library databases. We limited our review to articles published in the English language. We collected all relevant articles published from the inception of each database to October 2021, and the references of the included studies were traced to ensure proper recall rates.
Inclusion and exclusion criteria
Inclusion criteria for this systemic review were as follows: 1) studies comparing CSF SNAP-25 levels in subjects with AD or MCI with those of a control group with normal cognition; 2) studies reporting mean or median levels of CSF SNAP-25. Exclusion criteria were as follows: 1) study samples overlapping with those of other studies (if there were overlapping studies, we included studies with the largest number of patients with AD); 2) studies for which the mean values and standard deviations for CSF SNAP-25 could not be extracted.
Data extraction and quality control
Data extraction was carried out independently by two researchers (Q.Q.L. and H.L.). If there was any disagreement, differences were resolved by consulting a third study author or through discussions among study authors. The mean values and standard deviations for CSF SNAP-25 levels as well as the correlation coefficients comparing CSF SNAP-25 and CSF T-tau or P-tau levels were extracted for subsequent meta-analyses. For studies not reporting mean values and standard deviations for CSF SNAP-25, data were extracted from the reported graphs via GetData Graph Digitizer software (version 2.25) (GetData Pty Ltd., Kogarah, Australia). We selected the Agency for Healthcare Research and Quality (AHRQ) quality assessment scale as the guideline for the quality evaluation of the included articles [20].
Statistical analysis
Ratio of means (RoM) was used to determine the differences in CSF SNAP-25 levels when comparing AD, MCI, and HC. We present effect estimates and 95% confidence intervals (CI) for RoM. Standardized mean differences (SMD) were used as another pooled effect measure for reporting differences. For studies providing medians and interquartile ranges (rather than means and standard deviations), we used the data conversion methodology presented by Wan et al. [21]. We adopted formulas recommended by the Cochrane Handbook to combine subgroup data in some of the referenced studies [22]. Subgroup analysis was chosen to address heterogeneity, with heterogeneity tests based on Chi-squared tests and the I2 statistic. The pooled effect was calculated via a fixed-effects model only when p was > 0.1 and I2 was ≤25%. All of the above processes were carried out via Review Manager software (RevMan version 5.4.1) (Cochrane Training, London, UK). R statistical software (version 4.1.0) (The R Project for Statistical Computing, Vienna, Austria) and the meta package were used to calculate the pooled Spearman correlation coefficient between CSF SNAP-25 and tau levels. We likewise used R software and the meta package to perform sensitivity analyses in order to detect studies that statistically significantly influenced the pooled estimate upon meta-analysis. The existence of publication bias was assessed via the symmetry of the funnel plot or the p-value obtained in Egger’s test [23].
RESULTS
Literature selection and study characteristics
We identified 85 records from PubMed, 266 from Web of Science, 245 from Embase, three from the Cochrane Library, and one record from a review found through the initial database search; among these identified studies, eight were selected independently by two researchers (in consultation with other study authors) according to the aforementioned inclusion and exclusion criteria (Fig. 1). All eight studies included were cross-sectional analyses comparing CSF SNAP-25 levels in AD patients (n = 423) with controls (n = 464). Five of these studies reported CSF SNAP-25 levels in MCI groups (n = 275). We identified six studies reporting correlation coefficients comparing CSF SNAP-25 and CSF T-tau levels (n = 613) and four comparing CSF SNAP-25 and CSF P-tau levels (n = 402). Most studies provided data on medical and demographic variables (e.g., age, sex, Mini-Mental State Examination scores [MMSE]). The methods used to measure CSF SNAP-25 levels likewise differed across studies, as shown in Supplementary Table 1. The primary characteristic data extracted from these studies are listed in Table 1. Five studies were of medium quality and three studies were of high quality based on the AHRQ checklist. Specific evaluation results are shown in Supplementary Table 2.
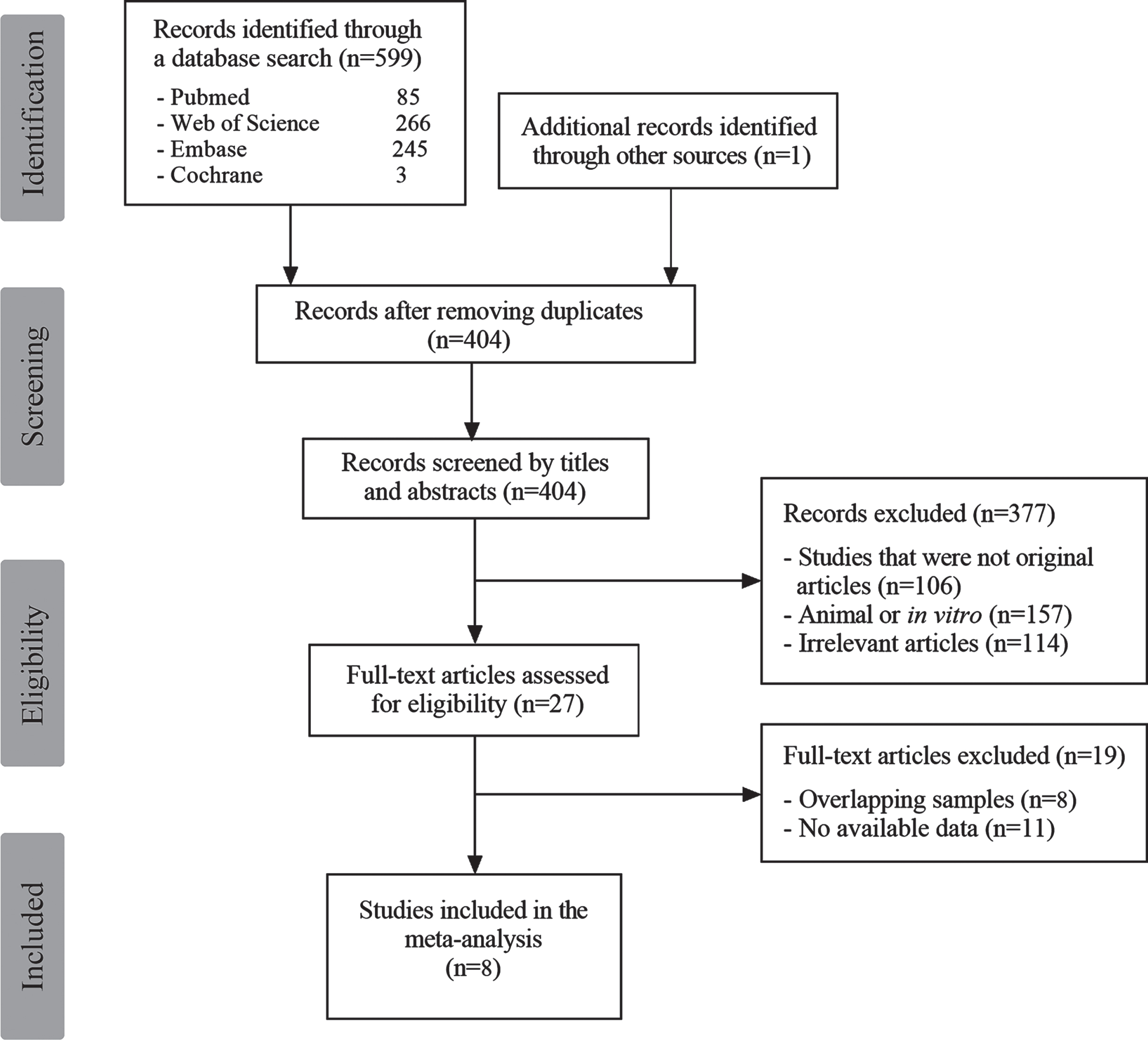
PRISMA diagram describing the study selection process.
CSF SNAP-25 levels in AD and HC
Statistically significant heterogeneity (I2 = 88%, p < 0.00001, χ2 = 57.83) was seen in the meta-analysis of the eight studies comparing CSF SNAP-25 levels in AD and HC based on a random-effects model that was used to calculate the overall RoM. Forest plots demonstrated that CSF SNAP-25 levels were increased in patients with AD as compared with controls (RoM = 1.50, 95% CI: 1.30, 1.74, p < 0.00001) (Fig. 2A).
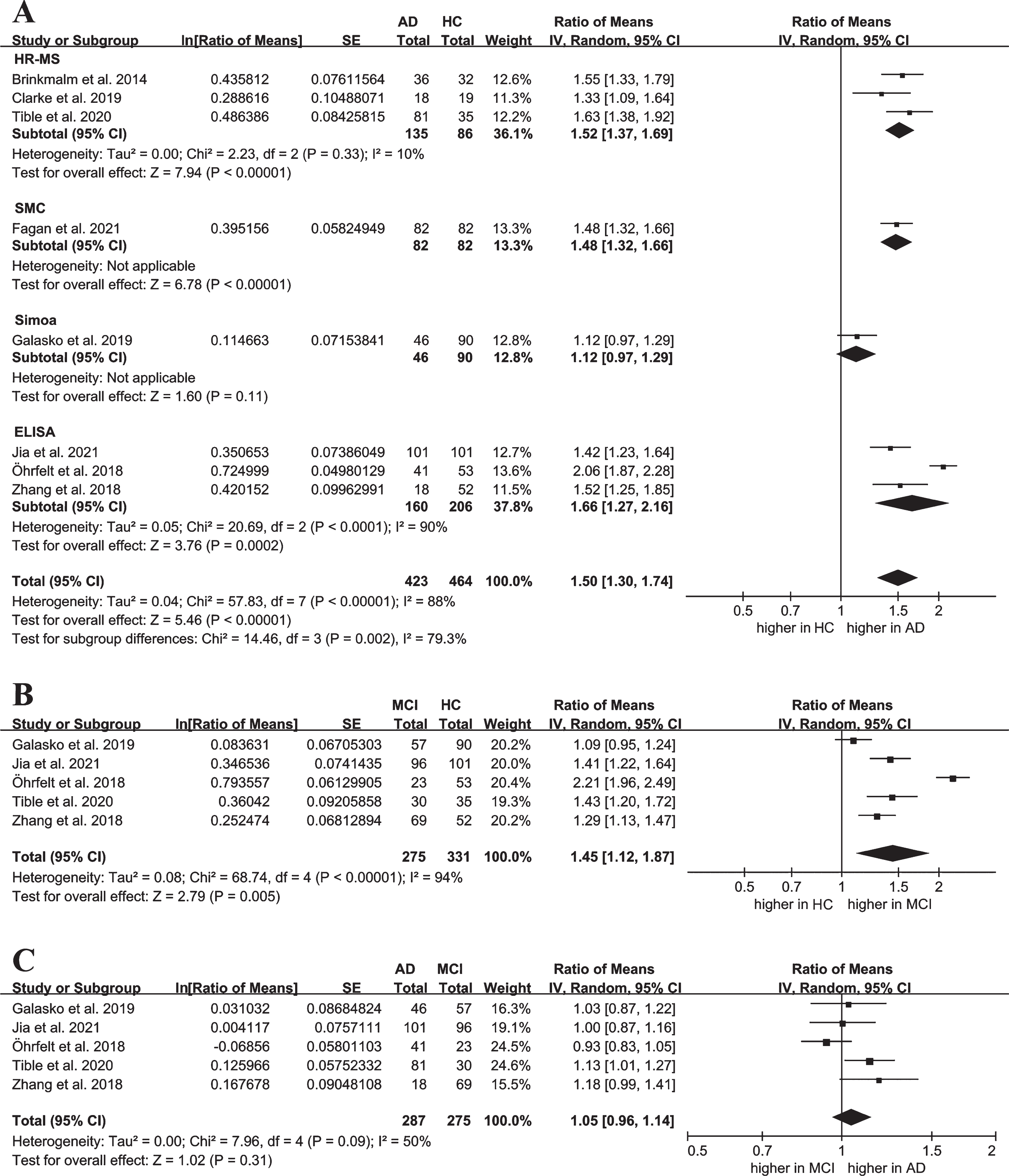
Forest plot of differences in CSF SNAP-25 levels when comparing Alzheimer’s disease (AD), mild cognitive impairment (MCI), and cognitively healthy controls (HC). A) Subgroup analysis according to the detection method comparing CSF SNAP-25 levels in AD patients and controls. B) Forest plot of CSF SNAP-25 levels in MCI as compared to controls. C) Forest plot of CSF SNAP-25 levels in AD as compared to MCI. CSF, cerebrospinal fluid; df, degrees of freedom; ELISA, enzyme-linked immunosorbent assay; HR-MS, high-resolution mass spectrometry; SE, standard error; Simoa, single molecule analysis; SMC:,single molecule counting; SNAP-25, synaptosomal-associated protein 25.
Based on the detection method for CSF SNAP-25 implemented in each study, the eight studies were divided into four groups for meta-subgroup analysis. Results in the high-resolution mass spectrometry (HR-MS) subgroup demonstrated that CSF SNAP-25 levels in AD were higher than in HC (RoM = 1.52, 95% CI: 1.37, 1.69, p < 0.00001) and that there was little heterogeneity in this subgroup (I2=10%, p = 0.33, χ2 = 2.23) (Fig. 2A). Similarly, we found differences in the single molecule counting (SMC) subgroup (RoM = 1.48, 95% CI: 1.32,1.66, p < 0.00001) (Fig. 2A). CSF SNAP-25 levels were statistically significantly increased in patients with AD as compared to controls (RoM = 1.66, 95% CI: 1.27, 2.16, p = 0.0002), with high heterogeneity (I2=90%, p < 0.0001, χ2 = 20.69) when enzyme-linked immunosorbent assay (ELISA) was used for examination (Fig. 2A). The single molecule analysis (Simoa) subgroup showed no statistical difference but did exhibit a trend toward significance in CSF SNAP-25 levels (RoM = 1.12, 95% CI: 0.97, 1.29, p = 0.11) (Fig. 2A). Forest plots of meta-analyses that calculated the pooled SMD are shown in Supplementary Figure 1.
Characteristics of studies and participants involved in the meta-analyses
AD, Alzheimer’s disease; HC, cognitively healthy controls; ELISA, enzyme-linked immunosorbent assay; HR-MS, high-resolution mass spectrometer; IWG, the International Working Group; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; NIA-AA, National Institute on Aging-Alzheimer’s Association; NINCDS-ADRDA, National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association; Simoa, single molecule analysis; SMC, single molecule counting; UK, United Kingdom; USA, United States of America. “-” represents no relevant information; NA represents data not reported in the respective studies. The data of age and MMSE score are shown as mean (standard deviation).
CSF SNAP-25 levels in MCI and HC
Five studies available for the comparison of SNAP-25 levels between MCI and controls were pooled in this meta-analysis. The result of the random-effects model used for this comparison indicated that patients with MCI had increased levels of CSF SNAP-25 as compared with controls (RoM = 1.45, 95% CI: 1.12,1.87, p = 0.005) (Fig. 2B).
CSF SNAP-25 levels in AD and MCI
We combined five studies to calculate the pooled differences in CSF SNAP-25 levels when comparing AD with MCI in the meta-analysis. A random-effects model was likewise used for this comparison, in consideration of statistical heterogeneity (I2 = 50%, p = 0.09, χ2 = 7.96). A forest plot showed that an evaluation of differences in CSF SNAP-25 levels in comparing AD and MCI (RoM = 1.05, 95% CI: 0.96,1.14, p = 0.31) indicated no statistical significance (Fig. 2C).
Correlations between CSF SNAP-25 and CSF tau levels
As shown in Fig. 3, the pooled Spearman correlation coefficient for the included studies indicated a statistically significant correlation between CSF SNAP-25 and CSF T-tau levels in patients with AD (Spearman correlation coefficient, ρ = 0.78, 95% CI: 0.72, 0.82, p < 0.01) (Fig. 3A), MCI (ρ= 0.66, 95% CI: 0.39, 0.83, p < 0.01) (Fig. 3B), and HC (ρ= 0.69, 95% CI: 0.54, 0.79, p < 0.01) (Fig. 3C). A similar result was found in the meta-analysis reporting the correlation between CSF SNAP-25 and CSF P-tau in patients with AD (ρ=0.77, 95% CI: 0.70, 0.83, p < 0.01) (Fig. 3D), MCI (ρ = 0.70, 95% CI: 0.52, 0.82, p < 0.01) (Fig. 3E), and HC (ρ=0.62, 95% CI: 0.52, 0.71, p < 0.01) (Fig. 3F).
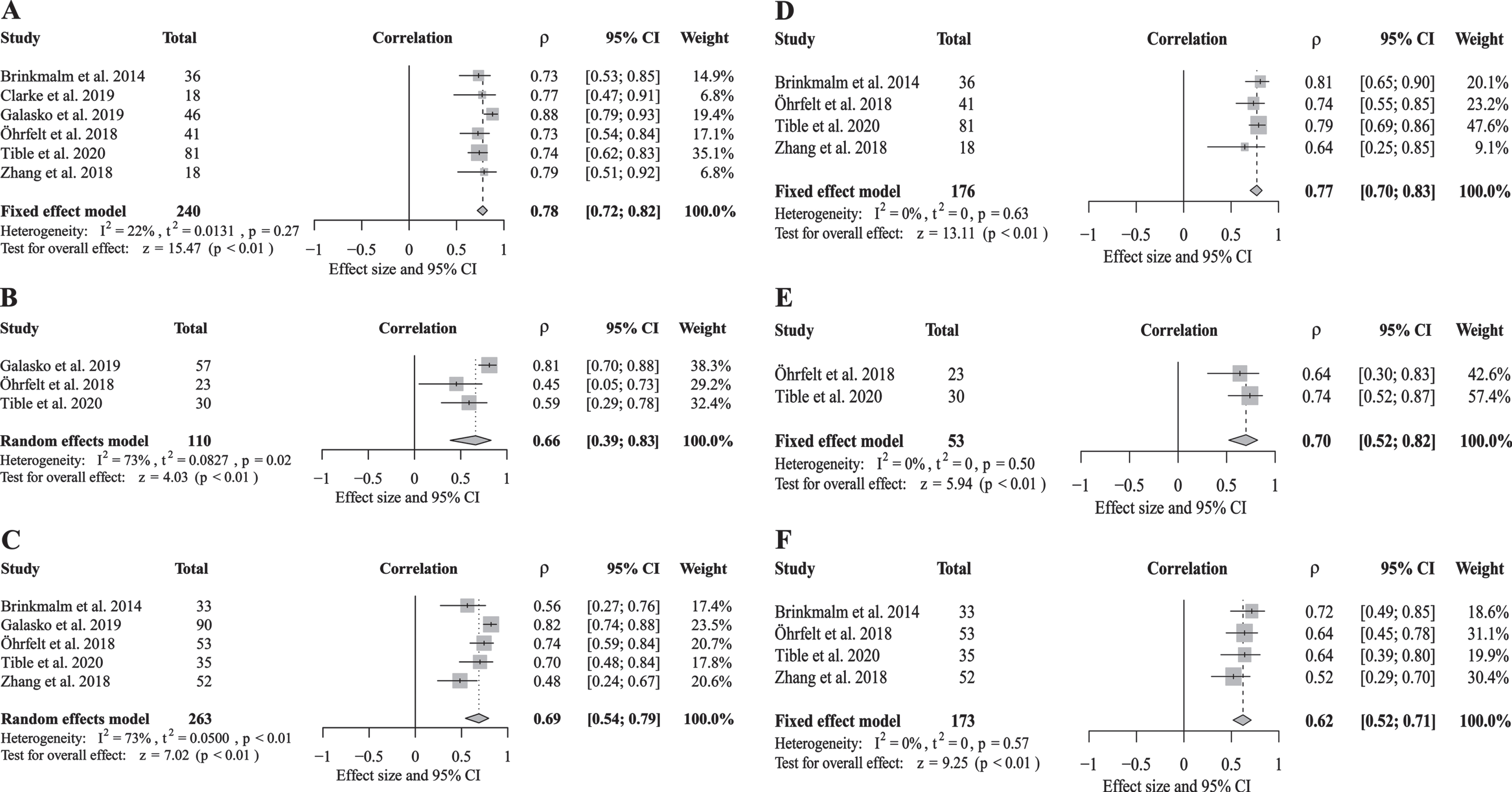
Forest plot of correlations between CSF SNAP-25 and total tau (T-tau) levels in patients with Alzheimer’s disease (AD) (A), mild cognitive impairment (MCI) (B), and in cognitively healthy controls (HC) (C), and correlations between CSF SNAP-25 and hyper-phosphorylated tau (P-tau) levels in patients with AD (D) and MCI (E) and in HC (F). CI, confidence interval; ρ, Spearman correlation coefficient; CSF, cerebrospinal fluid; SNAP-25, synaptosomal-associated protein 25.
Sensitivity analysis
By omitting individual studies successively and recalculating the pooled RoM, we found that the study conducted by Öhrfelt et al. statistically significantly influenced the overall effect in terms of the contrasts in SNAP-25 levels when comparing AD and HC, MCI and HC, and MCI and AD (Fig. 4).
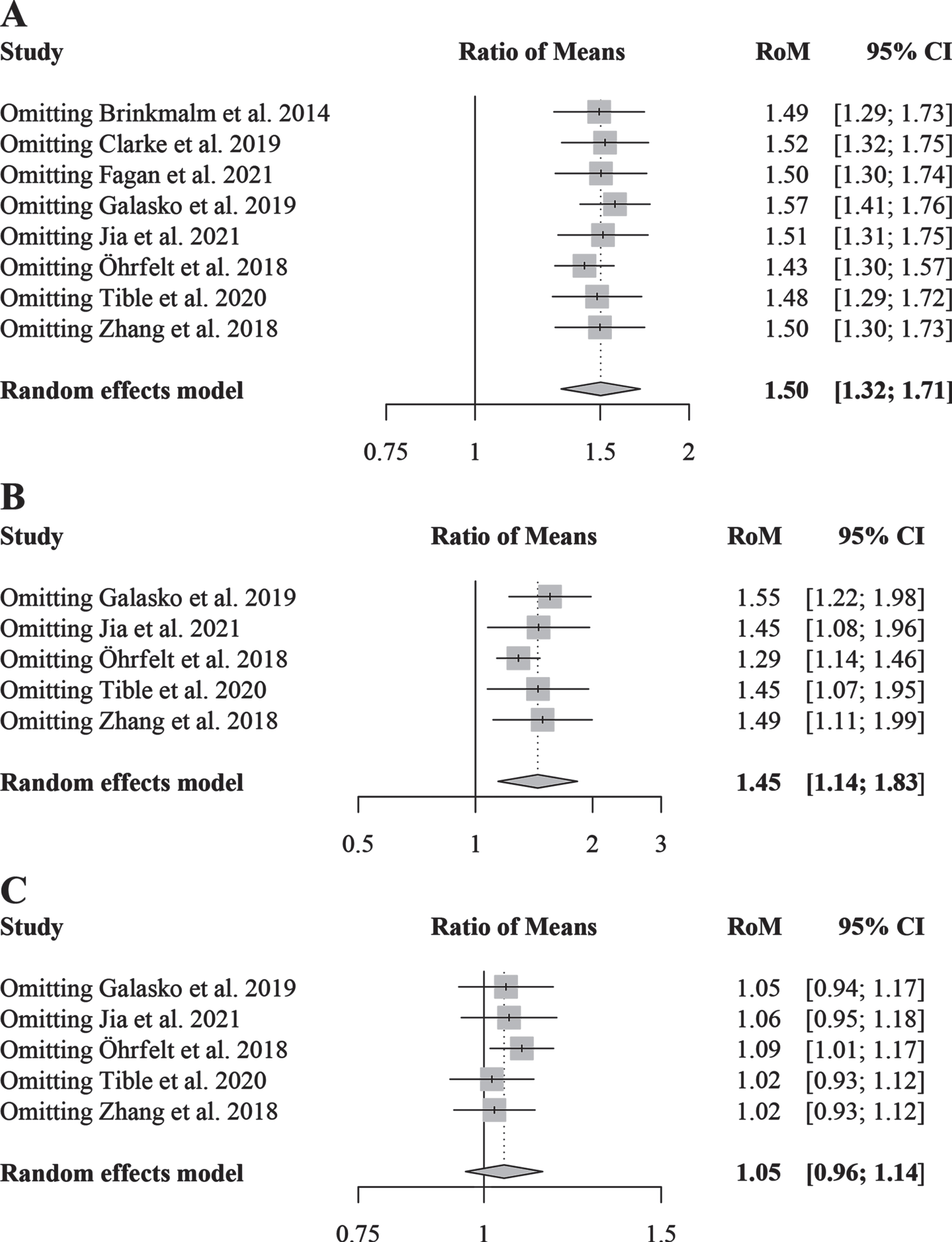
Sensitivity analysis comparing CSF SNAP-25 levels in Alzheimer’s disease (AD) and cognitively healthy controls (HC) (A), mild cognitive impairment (MCI) patients and HC (B), and AD and MCI patients (C). CSF, cerebrospinal; RoM, ratio of means; SNAP-25, synaptosomal-associated protein 25; CI, confidence interval.
Publication bias
The results of the funnel plot (Supplementary Figure 2) and Egger’s regression test (p = 0.1599) suggested a low risk of publication bias when comparing CSF SNAP-25 levels in patients with AD and controls.
DISCUSSION
The present study sought to evaluate the associations of CSF SNAP-25 levels with AD diagnosis via a quantitative evaluation method. The meta-analysis results demonstrate statistically significantly increased CSF SNAP-25 concentrations in patients with AD as compared to control subjects, suggesting that SNAP-25 may be a novel CSF biomarker of synaptic pathology in AD. Increased CSF SNAP-25 levels were likewise observed in MCI as compared to HC, suggesting the utility of SNAP-25 as a biomarker in the early diagnosis of AD. Of note, CSF SNAP-25 levels did not differ at the level of statistical significance when comparing participants with MCI and AD, indicating that guidelines delineating concentration changes in CSF SNAP-25 levels during AD progression remain unknown and that the value of CSF SNAP-25 needs to be studied more comprehensively in terms of the staging of AD. The statistical heterogeneity in the reported meta-analyses may be explained by the results of subgroup and sensitivity analyses. We likewise found that CSF SNAP-25 levels showed a statistically significant correlation with CSF tau levels, whether in AD, MCI, or HC, suggesting that increased CSF SNAP-25 levels might indirectly reflect the severity of the neuronal injury and the tau-associated pathologic state in brains.
The pathophysiological mechanism of elevated CSF SNAP-25 levels in patients with AD remains unclear. Studies have reported decreased levels of SNAP-25 in multiple brain regions in AD [11–13]. This could be due to the fact that SNAP-25 mRNA expression was significantly decreased in the brains of AD patients [13]. Moreover, the pathophysiological process in the brains of AD patients may contribute to the release of intracellular SNAP-25 from neuronal cells into the CSF, leading to elevated SNAP-25 levels in the CSF. Studies have demonstrated that the upregulation of calpain in the brains of AD patients could cleave SNAP-25 into shorter fragments [24, 25], which might cross the cell membrane and enter the CSF. Studies have reported that elevated CSF SNAP-25 levels in early AD may be associated with amyloid-induced synaptic injury [26, 27]. Zhang et al. suggested that progressive MCI patients with positive CSF Aβ results had significantly higher CSF SNAP-25 levels than those with negative results [16]. It has also been shown that increased SNAP-25 levels in the CSF are associated with the APOE ɛ4 allele. The study by Butt et al. showed that carriers of the APOE ɛ4 allele had significantly higher CSF SNAP-25 levels than non-carriers in cognitively normal individuals. In addition, more APOE ɛ4 alleles are associated with higher CSF SNAP-25 levels both in amyloid positive individuals and in amyloid negative individuals [28]. Wang et al. and Tible et al. found elevated CSF SNAP-25 levels that were associated with the APOE ɛ4 allele in MCI individuals and AD patients, respectively [15, 29]. A study has demonstrated that human APOE4-targeted replacement mice showed elevated CSF SNAP-25 levels in the absence of neuropathology, which suggested that APOE4 plays a role in the early stages of the increase of CSF SNAP-25 levels [30].
The current meta-analysis reported no statistically significant differences in CSF SNAP-25 levels when comparing MCI and AD patients. A study conducted by Sutphen et al., however, reported increased CSF SNAP-25 levels in patients with AD as compared to MCI patients with negative Aβ readings [31]. This result indicates that combining CSF SNAP-25 with CSF Aβ might be used for the effective staging of AD diagnoses. An increased CSF SNAP-25/Aβ42 ratio has been shown to correlate with the extent of hippocampal atrophy in patients with progressive MCI as well as the rate of progression of cognitive impairment in subjects with normal cognition in a longitudinal study [16]. It has likewise been reported that baseline levels of CSF SNAP-25 are useful for predicting progression from MCI to AD; however, this biomarker is much less effective in distinguishing AD from MCI [17]. Additional prospective studies are warranted to explore the effects of changes in CSF SNAP-25 levels with respect to AD progression.
We conducted subgroup analyses according to the different methods used to detect CSF SNAP-25 levels within the included studies. The results showed statistically significant heterogeneity among subgroups, with no heterogeneity (with the exception of the ELISA subgroup). These findings demonstrate that the technology implemented for detection might influence the diagnostic utility of CSF SNAP-25. In sensitivity analyses, excluding the study conducted by Öhrfelt et al. statistically significantly influenced the pooled effects in all comparisons. Most strikingly, as compared with other studies, the research by Öhrfelt et al. showed more strongly statistically significant differences in CSF SNAP-25 levels when comparing patients with AD and controls and when comparing patients with MCI and controls. This finding could be attributed to the novel sandwich ELISA methodology used to assess CSF SNAP-25 levels in this study; the longer N-terminal forms of SNAP-25 might also be analyzed via this methodology [14]. This also could explain the heterogeneity seen within the ELISA subgroup in this study. In an investigation conducted by Brinkmalm et al., the tryptic peptide assay for SNAP-25 (32–40) performed best when differentiating patients with AD from controls, while only SNAP-25 (Ac-2-16) was negatively correlated with MMSE scores in patients with AD [18]. These findings demonstrate that the diagnostic efficiency of different forms of CSF SNAP-25 might present varying levels of utility as biomarkers of AD diagnosis and progression. Therefore, additional studies exploring an optimal form of SNAP-25 as a CSF biomarker for AD are highly warranted. Notably, for the study by Fagan et al., we included symptomatic carriers of autosomal dominant AD mutations in the AD group and asymptomatic non-carrier siblings in the control group [32]. Compared with that noted in other studies included in the meta-analysis, subjects in this study were younger and had more definitive evidence of genetic inheritance. The results of this single study in the subgroup analysis were consistent with the overall meta-analysis, which is highly supportive of SNAP-25 as a marker involved in AD.
In the previously reported AT(N) system of AD detection (based on biomarkers), P-tau and T-tau are used as biomarkers to reflect tau-associated pathology and neurodegeneration in AD, respectively [5]. Studies have demonstrated correlations between tau pathology and synaptic loss in AD brains [33, 34], although the specific mechanisms mediating these associations remain unclear. The results of the current meta-analysis showed a statistically significant correlation between SNAP-25 and T-tau in the CSF, suggesting that CSF SNAP-25 has the potential to be added to the (N) biomarker group (i.e., in which biomarkers reflect neurodegeneration or neuronal injury). Notably, P-tau has demonstrated a more specific diagnostic performance in distinguishing AD from most other dementias. Considering the statistically significant correlations with P-tau reported in this study, we conclude that SNAP-25 may have similar diagnostic potential. Consistent with that conjecture, a study conducted by Tible et al. showed increased CSF SNAP-25 levels in AD but not in other neurocognitive diseases [15]. A previous study likewise showed that the diagnostic sensitivity of SNAP-25/Aβ42 was comparable to that of T-tau/Aβ42 and P-tau/Aβ42 [16], the known effective prognostic markers for AD, which can also be explained by the correlation of CSF SNAP-25 with T-tau and P-tau. Besides, our findings as well as that of previous studies suggest that CSF SNAP-25 may likewise be used as a candidate biomarker to reflect the therapeutic effects of tau-targeted drugs in clinical studies.
This is the first meta-analysis of SNAP-25 levels in CSF in patients with AD, and we increased statistical power through meta-analysis to improve the reliability and objectivity of the conclusions. In addition, we performed a subgroup analysis to find the source of heterogeneity, which also provided valuable insights for the research and clinical application of CSF SNAP-25 in AD. This meta-analysis also has several limitations. Only eight original articles were included as data sources in the meta-analysis. Therefore, meta-regression was unsuitable to explore sources of heterogeneity. The reliability of publication bias tests was similarly attenuated because of the small number of included studies. We did not analyze the relationship between CSF SNAP-25 and Aβ42, another core CSF biomarker, in this study, because some studies did not provide correlation coefficients for non-statistically significant groups. If only the provided statistically significant correlation coefficients were combined, it might cause bias. There was some clinical heterogeneity in the diagnostic criteria for AD and demographic data (e.g., mean age, sex, and MMSE scores) within the included studies. Accordingly, the random-effects model was used for calculating the pooled effect with the above questions in mind. It should be noted that this study was not performed on individual patient data, and that using GetData Graph Digitizer software as well as combining subgroups to obtain data in some studies might cause deviation in the final data. Data extraction was independently performed by two authors to minimize the likelihood of this bias.
Conclusion
To our knowledge, we conducted the first meta-analysis evaluating differences in CSF SNAP-25 levels among AD, MCI, and HC as well as the first meta-analysis evaluating correlations between CSF SNAP-25 and CSF tau levels. Our study findings suggest that CSF SNAP-25 might be an effective and novel biomarker for the early diagnosis of AD. More relevant clinical studies are warranted to confirm and supplement the results of our study in the future. In designing future research, we recommend considering the value and utility of controlling for potential confounding factors, determining unified protein detection methods, and detecting specific forms of SNAP-25 to establish available detection thresholds. Future highly powered longitudinal studies are necessary to explore the relationships of CSF SNAP-25 levels with clinical manifestations, brain imaging changes, and other biomarkers in order to evaluate the significance of this potential biomarker in the prediction, staging, and prognosis of AD. Our findings provide guidance to future research directions and will ultimately inform medical guidelines and preventive medicine initiatives.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the National Key R&D Program of China (No. 2020YFC2008500), the National Natural Science Foundation of China (No. 82071216), the Hunan Innovative Province Construction Project (No.2019SK2335), and the Huxiang Young Talents Project (No. 2021RC3028).