
Abstract
Background:
Previous studies suggest a positive effect of tea intake on cognition. Additional micronutrients that may moderate this association was not previously examined.
Objective:
To examine the association between tea consumption and cognition and explore the interaction between tea consumption and iron intake.
Methods:
Data from the China Health and Nutrition Survey between 1997 and 2011 was used. 4,820 individuals (≥55 years) were included in the analyses. Measurement of cognitive function was conducted in 1997, 2000, 2004, and 2006. Tea consumption was self-reported. Food intake was assessed by 24-hour dietary recalls of three consecutive days during home visits between 1997 and 2011. Multivariable mixed linear regression and logistic regression was used to assess the association.
Results:
Tea consumption was associated with reduced global cognitive function decline. In fully adjusted models, regression coefficients (95% CIs) for those who consumed 0 cups/day,<2 cups/day, 2–3.9 cups/day, and≥4 cups/day of tea were 0, –0.09 (–0.55–0.37), 0.05 (–0.34–0.45), and 0.87 (0.46–1.29), respectively. This effect was stronger in adults > 60 years. Tea consumption of≥4 cups/day was inversely associated with self-reported poor memory (OR 0.70 (95% CI 0.56–0.86)) and memory decline (OR, 0.73 (95% CI 0.62–0.87)). There was a significant interaction between tea consumption and iron intake in relation to cognition. High iron intake was inversely associated with cognition in non-consumers of tea but not in tea consumers.
Conclusion:
Higher tea intake is associated with reduced cognitive decline in adults and inhibits the adverse effect of high iron intake.
INTRODUCTION
Dementia is a general term for cognitive decline that is known to affect the quality of life, especially among the elderly population. Cognition-related diseases such as mild cognitive impairment and Alzheimer’s disease (AD) are gradually increasing and becoming a significant global public health concern [1, 2]. In 2010, it was estimated that around 36 million people globally experienced dementia; this number is expected to double by 2030 and triple by 2050 [2]. In China alone, 9.5 million adults aged 60 years and above have experienced dementia [3]. Among the many modifiable risk factors associated with cognitive decline, the dietary factor has been well-established [4]. Previous studies have indicated an association between diet and cognitive function in children [5], adults [6], and the elderly [7]. It has been shown that following a Mediterranean diet [8] and the consumption of omega-3 fatty acids [9], vitamin E [10], eggs [11], milk [12], and coffee [13] is related to a decreased risk of cognitive disorders.
Tea drinking originated in Asia, and now it has spread throughout the world to be the most popular consumed beverage. In recent years, researchers have examined the relationship between tea intake and cognitive function [14–18]. Tea consumption is linked to a lower risk of cognitive impairment and dementia [14–16] and associated with a decrease in the progression of cognitive dysfunction [19, 20]. Moreover, a study on middle-aged and older adults in China found that habitual tea consumption (especially green tea) was significantly associated with a decreased prevalence of cognitive impairment [21]. A meta-analysis on the relationship between tea intake (green and black) and the risk of cognitive disorders, showed that a higher tea intake was linked to a decreased risk of cognitive disorders [14]. Nevertheless, inconsistent findings also have been documented [18, 23] with some null associations [17]. A 21-year follow-up longitudinal study in Finland reported that tea consumption was not associated with AD or dementia [17].
Furthermore, research has shown that the neuroprotective, anti-oxidative, and anti-inflammatory effect of tea is attributed to its components, most notably polyphenols such as catechins and its derivatives [24–27]. Experimental and animal studies suggest that tea polyphenols may be used in treating neurodegenerative diseases, such as AD and Parkinson’s disease [28]. Besides polyphenols, other tea components such as caffeine, may decrease the risk of dementia and enhance cognitive decline, although more studies with longer follow-up periods are encouraged to draw a conclusion [29]. Moreover, theanine, an amino acid abundant in tea, was found to have a positive effect on memory in mice [30]. Another important aspect to mention is that tea consumption was shown to have beneficial effects on diabetes [31], which in itself is a well-known determinant of dementia and cognitive impairment [32].
The strength of the association between tea intake and cognitive impairment risk remains unsettled due to the differences in study populations and methodological approaches in previous studies. Furthermore, little is known about whether the relationship of tea consumption and cognition is moderated by additional micronutrients. Of note, it is known that tea inhibits iron absorption [33], and it was previously shown that iron intake is inversely associated with cognitive function in Chinese individuals [34]. Similarly, iron consumption was shown to be positively associated with disorders that induce cognitive decline in Western societies [35]. Despite this evidence, the relationship between tea drinking, iron intake, and cognitive health was not previously explored.
In this study, the aim was twofold: 1) to assess the longitudinal association between tea intake and cognitive function among Chinese adults using data from the China Health and Nutrition Survey (CHNS) over a 15-year period; 2) to examine the interaction between tea intake and iron intake in relation to cognition.
METHODS
Study design and sample
The current study was a population-based longitudinal study using data from the CHNS, based on repeated measurements of cognitive function and dietary intake over fifteen years. The CHNS study is an ongoing, prospective, household-based open cohort study conducted in 15 provinces in China between the years 1989 and 2015 [36, 37]. The multistage random cluster sampling process is used to collect samples from urban and rural areas. Data collection of ten waves have been conducted between 1989 and 2015. During the survey years 1997, 2000, 2004, and 2006 cognitive screen tests were conducted among individuals above 55 years of age. Dietary data in 2015 was not published, and the 1989 survey was collected only in a subgroup, so we only used data between 1997 and 2011. In total, 4,820 individuals (2,306 men and 2,514 women) between 1997 and 2006 attended cognitive screen tests. Of these subjects, 4,657 participants attended the screen test in at least two surveys. Subjects included in the analysis were those who did at least one cognitive screen test. Moreover, fasting blood collection and assessment were conducted for the first time in the 2009 wave. After at least 12 h of overnight fasting, a blood sample of (12 mL) was collected by venipuncture. Serum samples were frozen and stored (at –86°C) for later laboratory analysis.
The CHNS was approved by the institutional review committees of the University of North Carolina (United States) and the Chinese National Institute of Nutrition and Food Safety. The response rate was > 60% based on those who participated in 1989 and remained the same in the 2006 survey. All participants provided informed consent before participation in the study.
Outcome variable: Cognitive function
Objective measures for global cognitive function and self-report for memory were used to assess cognitive function. For the total global cognitive score, cognitive screening was done through a face-to-face interview and involved a subset of modules from the Telephone Interview for Cognitive Status–Modified [38]. This tool has been previously used in other population studies in China to assess cognitive function [39]. Composite scores of memory, counting back, and subtraction scores were used to calculate the global cognitive score. Three main tasks constituted the cognitive screening, an immediate (score 10) and delayed (score 10) recall of a ten-word list, backward counting from 20 to 1 (score 2), and 7 serial subtractions (score 5). The final total score ranged from 0 to 27. A lower cognitive score represents poorer cognition. For the first task (scores 1 through 20) a score of 1 is given to each word recalled correctly. The sum of the immediate and delayed ten-word recall was used to calculate the total verbal memory score. For the second task, a score of 2 was given to those who counted backward correctly on the first try. If counting backward was done correctly on the second try, a score of 1 was given. As for the final task, subjects did 5 consecutive subtractions of 7 from 100. Each correct subtraction was given a score of 1.
For self-reported memory, subjects were asked “How is your memory? (1) very good, (2) good, (3) OK, (4) bad, (5) very bad, (9) unknown”. Subjects who answered “bad” or “very bad” were considered as having a poor memory. As for memory change, it was assessed by the question “In the past twelve months, how has your memory changed? (1) improved, (2) stayed the same, (3) declined, (9) unknown”. Subjects who answered “declined” were considered as having memory decline.
Exposure variable: Tea and iron consumption
Tea intake was relatively stable among survey waves, so tea consumption in each wave was used in the multivariable model. Detailed information on the tea types consumed by the participants was not available. Therefore, any type of tea consumed was included in the analyses. Cumulative mean iron intake data were collected in multiple waves. Detailed information on dietary measurements has been previously discussed [36]. Individual dietary intake data were collected by a trained investigator at each wave using a 24-h dietary recall on each of three consecutive days. At the start and end of the three-day survey period, interviewers recorded and weighed food and condiments in home inventory, food acquired from markets/gardens, and food waste. The Chinese Food Composition Table was used to convert food consumption data to nutrient intakes [40]. The current dietary assessment method has been validated for energy intake [41].
Covariates
Demographic measures were age and gender. Socioeconomic status measures were education level (low: Illiterate/primary school, medium: Junior middle school, and high: High middle school or higher), per capita yearly family income level (low, medium, and high), urbanization levels [36] (low, medium, and high). Additionally, other covariates were smoking status (nonsmokers, ex-smokers, and current smokers), level of physical activity (recorded in metabolic equivalent of task (MET)) estimated with self-reported activities (such as occupational, domestic, transportation, and leisure-time physical activity), alcohol drinking (yes or no), body mass index (BMI), self-reported history of diabetes and stroke (yes or no), and hypertension (systolic blood pressure more than 140 mmHg or diastolic blood pressure more than 90 mmHg or self-reported hypertension).
Two dietary patterns were created based on thirty-five food groups (including alcohol) which were gathered from 24-h dietary recalls of three consecutive days with the use of factor analysis [42]. One dietary pattern ‘traditional south pattern’ is characterized by an increased intake of rice, pork, and vegetables, and decreased wheat intake. The other dietary pattern ‘modern dietary pattern’ is characterized by an increased intake of beer, fruits, milk, soy milk, eggs, and deep-fried food.
Statistical analysis
All analyses were conducted using STATA 17 (Stata Corporation, College Station, TX, USA). Tea consumption in each survey wave was measured and recoded into four levels: non-consumers,<2 cups/day, 2–3.9 cups/day, and ≥4 cups/day. The serving size of one cup is equal to 240 mL of tea. A mixed-effects model using the mixed command in Stata was used to assess the relationship between tea consumption and cognitive function. Cognitive function decline is indicated by a negative regression coefficient. The models used were model 1: adjusted for age, gender, and energy intake (as a continuous variable); model 2: further adjusted for fat intake (continuous), smoking (nonsmoker, ex-smoker, current smoker), income (low, medium, high), education level, alcohol drinking, urbanization (low, medium, high), and physical activity level; model 3: further adjusted for overall dietary patterns (continuous); and model 4: further adjusted for hypertension and BMI. Model 5 further excluded subjects who attended only one wave of the cognitive function tests. All the adjusted variables were considered as time-varying covariates (except for gender). To compare differences between groups for categorical variables the chi-square test was used and the ANOVA test for continuous variables. To assess the relationship between tea consumption and poor cognitive function risk, mixed-effects logistic regression was used, adjusting for the aforementioned covariates in model 4. Subgroup analyses of the tea-cognitive function association was conducted to assess the age differences between people less than 60 years of age and people greater than or equal to 60 years of age. We used this age as a divider due to the fact that the general retirement age in China is 60. To assess the interaction between tea intake and several variables including BMI, hypertension, gender, and iron intake, a product term of each pair of variables was put in the regression model. To visually present the interaction, the command marginsplot was used in Stata. Significance was considered when p < 0.05 (two-sided).
RESULTS
Descriptive results
Table 1 depicts the sample characteristics of subjects who took part in the first cognitive function test according to levels of tea consumption. Of the participants, 59.4% did not consume tea, 11.2% consumed <2 cups/day, 14.3% consumed 2–3.9 cups/day, and 15.1% consumed ≥4 cups/day. The intake of energy, protein, and fat was positively associated with tea consumption. Traditional and modern dietary patterns also slightly increased across tea intake levels. However, there was no difference in iron intake and BMI across quartiles of tea intake. Those who did not consume tea were more likely to have hypertension, diabetes, and stroke.
Sample characteristics of Chinese adults aged ≥55 years old attending the first cognitive function test by quartiles of tea intake (n = 4,657)
Values are mean (SD) or n (%).
Overall, the mean global cognitive score declined between 1997 and 2006 (Fig. 1). Participants who consumed tea ≥4 cups/day had the highest cognition score across all years. Tea consumption was inversely associated with hemoglobin (Hb) levels in 2009, especially in men (Supplementary Figure 1). However, it did not increase the risk of anemia.
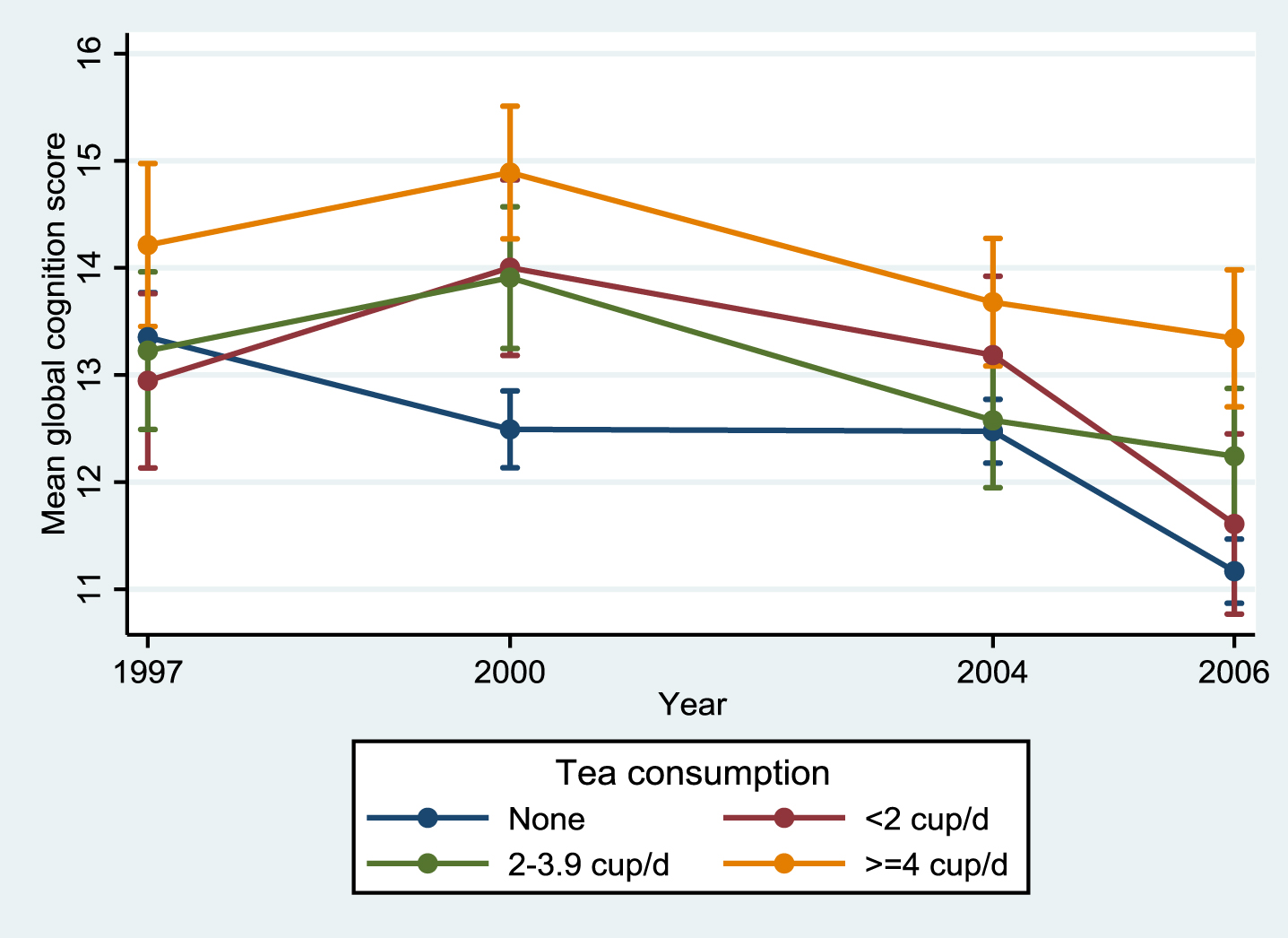
Mean global cognitive score (95% CI) by year and quartiles of tea consumption among Chinese adults aged ≥55 years and who attended at least two waves of cognition tests, China Health and Nutrition Survey.
Association between tea consumption and cognitive function
Tea consumption was positively associated with cognitive function on a global cognitive scale (Table 2). After adjusting for age, gender, and energy intake, those who drank ≥4 cups of tea per day had a higher global cognitive score compared with non-consumers. In the fully adjusted model (model 5), regression coefficients (95% CIs) for the global cognitive score for tea non-consumers, those who consumed 0 cup/day, <2 cups/day, 2–3.9 cups/day, and ≥4 cups/day were 0, –0.09 (–0.55–0.37), 0.05 (–0.34–0.45), and 0.87 (0.46–1.29), respectively. This result did not differ significantly between those < 60 years of age and those ≥60 years of age or between those from different regions, although the association seems to be stronger among those ≥60 years of age and living in the north (Table 4).
Regression coefficients (95% CI) for cognitive function by quartiles of tea intake among Chinese adults aged 55 years and above attending China Health and Nutrition Survey (n = 4,820)
Model 1 was adjusted for age, gender, and energy intake (as a continuous variable). Model 2 was based on model 1 but further adjusted for intake of fat (continuous), smoking, alcohol drinking, income (low, medium, and high), urbanicity (low, medium, and high), education (low, medium, and high), and physical activity level (continuous). Model 3 was further adjusted for overall dietary patterns based on factor analysis. Model 4 was further adjusted for BMI (as a continuous variable) and hypertension (yes or no). Model 5 was based on model 4 but further excluded those who only participated in one wave of the cognitive function tests. All the adjusted variables are treated as time-varying covariates (except gender).
Subgroup analyses of the association between tea consumption and global cognitive function score
After adjusting for covariates, an inverse association was observed between tea intake and self-reported poor memory and self-reported memory decline (Table 3). Compared with non-consumers, tea intake of ≥4 cups/day was inversely associated with self-reported poor memory (OR, 0.70 (95% CI 0.56–0.86)) and 27% decreased risk of having self-reported memory decline (OR, 0.73 (95% CI 0.62–0.87)).
No statistically significant results related to the impact of age were found. A subgroup analyses on the effect of age revealed that those above 60 years of age had greater global cognitive function score.
Interaction between tea consumption and iron intake in relation to cognitive function
An interaction was found between tea consumption and iron intake in relation to global cognitive score (p = 0.180) (Fig. 2). Among tea consumers, no association between iron intake and cognition was found. In contrast, among non-consumers of tea, there was an inverse association between iron intake and cognitive function score. There was no interaction between tea intake and gender, hypertension, and overweight/obesity in relation to cognition (data not shown).
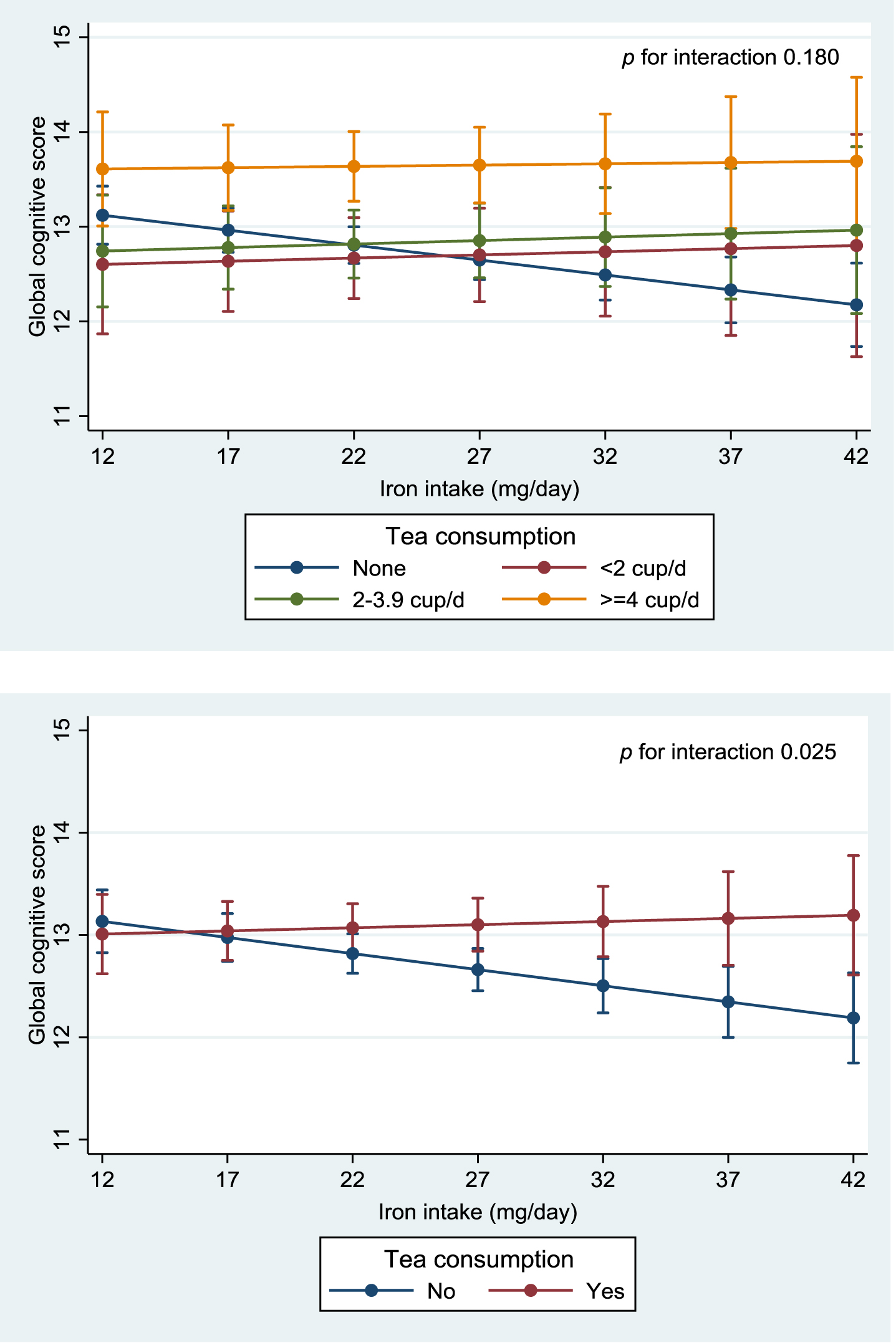
Interaction between tea consumption and iron intake in relation to global cognitive function. Values were regression coefficients (95% CI) from a mixed linear regression model. The model was adjusted for age, gender, intake of energy. and fat (as continuous variables), smoking (nonsmoker, ex-smoker, current smoker), BMI, alcohol drinking, income (low, medium, high), urbanicity, education, and physical activity, overall dietary patterns (continuous) and hypertension. The model included all subjects participated in at least two waves of the survey. p for interaction between iron intake and tea intake was 0.180. An ordinal value (1, 2, 3, 4) was assigned to reflect the quartiles of tea consumption intake level and treated as a continuous variable while testing for interactions.
DISCUSSION
In this longitudinal open cohort study with adults greater than 55 years of age, we found that increased tea consumption was negatively associated with cognitive impairment as measured by global cognitive scores among those who attended at least two cognitive tests between 1997 and 2006 in the CHNS. The association was independent of lifestyle and sociodemographic factors. Those who consumed ≥4 cups of tea per day were less likely to have poor cognitive function than those who did not consume tea. These results do not have statistically significant differences between different ages (<60 versus ≥60 years) and regional groups (north versus south). Higher tea consumption was inversely associated with self-reported poor memory and memory decline. Moreover, an interaction between tea consumption and iron consumption in relation to cognitive function was found. Across all levels of tea consumption, no association between iron intake and cognition was found. In contrast, high iron intake was inversely associated with cognitive function among non-consumers oftea.
Tea consumption and cognitive function
Our findings were in line with several studies linking tea consumption with decreased risk for cognitive impairment among middle-aged and older Chinese adults [16, 21] and other populations [43]. A previous dose-response meta-analysis found that higher tea consumption (green, black) was linked to a decreased risk of cognitive disorders [14]. The dose-response analyses revealed a reduced risk of 6%, 19%, and 29% after 100 mL, 300 mL, and 500 mL per day of tea consumption, respectively [14]. A study conducted by Ng and his collogues [16] on Chinese adults (aged ≥ 55 years) in the Singapore Longitudinal Ageing Studies cohort, showed that regular tea intake lowered the risks of cognitive impairment and decline from both cross-sectional and longitudinal analysis [16]. Moreover, a 5.7-year prospective cohort study was conducted on elderly Japanese individuals (13,645 participants), which revealed that frequent green tea intake was significantly linked with a decreased risk of incident dementia (hazard ratio for ≥5 cups/day versus < 1 cup/day: 0.73 (95% CI: 0.61–0.87)) [44].
Odds ratios (95% CI) for self-reported poor memory and self-reported memory decline by levels of tea intake among Chinese adults aged ≥ 55 years old by characteristics, China Health and Nutrition Survey (n = 4,820)
Model 1 was adjusted for age, gender and energy intake (as a continuous variable). Model 2 was based on model 1 but further adjusted for intake of fat (continuous), smoking, alcohol drinking, income (low, medium, and high), urbanicity (low, medium and high), education (low, medium and high), and physical activity level (continuous). Model 3 was further adjusted for overall dietary patterns based on factor analysis. Model 4 was further adjusted for BMI (as a continuous variable) and hypertension (yes or no). Model 5 was based on model 4 but further excluded those who only participated in one wave of the cognitive function tests. All the adjusted variables are treated as time-varying covariates (except gender).
Values are regression coefficients (95% CI). Models adjusted for age, gender, energy intake (as a continuous variable), fat intake (continuous), education, income (low, medium, high), urbanization, smoking, drinking, physical activity, dietary patterns (continuous), BMI and hypertension. Stratification variables were not adjusted in the corresponding models.
However, there are some inconsistent findings in the literature regarding the association between tea and cognition. A previous study suggested that the positive effect of tea intake is restricted to cognitively healthy elderly and does not extend to elderly with mild cognitive impairment [18]. Interestingly, a study conducted on 2,131 elderly Han individuals found that green tea intake had a protective effect against amnestic mild cognitive impairment in men but not in women [15]. Our study showed an insignificant interaction between tea consumption and gender. Nonetheless, the study further revealed that black or oolong tea did not show any protective effect [15]. On the other hand, a study showed that the consumption of particularly black or oolong tea had an inverse association with cognitive impairment and cognitive decline [16]. This discrepancy in the results among the different types of tea may be due to the diverse fermentation degrees during tea processing, which alters the amount of catechin available in tea leaves.
Furthermore, a population-based longitudinal study in Finland on 1,409 individuals (∼21 years follow up) reported no association between tea intake and Alzheimer’s disease or dementia [17]. This null finding may be attributed to the different measurements of the exposure and outcome variable. Unlike our study, this study used a semi-quantitative food frequency questionnaire to collect dietary information and used the Mini-Mental State Examination to measure cognitive status. Moreover, this study failed to adjust for potential confounders including alcohol consumption, energy intake, and dietary patterns, which may have contributed to their findings. In our study, the robustness of the tea consumption-cognition relationship is illustrated by controlling for the aforementioned confounders, in addition to socioeconomic status and chronic illness, as well as its being applicable to different groups (e.g., degree of urbanization, age, and region).
Although there was no significant interaction between age and tea drinking, the association between tea drinking and cognition was only significant among those with age ≥ 60 years. It could be due to the fact that cognition declines more in old age than young age. Furthermore, after retirement (≥60 years of age) the lifestyle became less healthy (e.g., less vigorous physical activity, more alcohol drinking) as compared with before retirement in China [45]. Future longitudinal studies should take into account normal cognitive decline as well as controlling for potential confounders. One caveat we would like to point out is that, although the dominant retirement age in China is 60 years, the mean age of retirement in this cohort was around 55 years. As the minimum age of inclusion in the cohort is ≥55 years, in subgroup analysis we split the cohort around 60 years which is the average age in the wider Chinese population even though it is 5 years earlier in this cohort. Nevertheless, such approach might result in residual confounding in the subgroup analyses. Future research needs to look at other cohorts, whose cut-off age and mean retirement age are consistent in this area of research.
Potential underlying mechanisms for tea consumption and cognitive function
The underlying potential mechanisms of the impact of tea consumption on cognitive health are complex. It is known that tea contains polyphenols, which may explain the neuroprotective, anti-oxidative, and anti-inflammatory effect of tea on cognitive function [24–27]. Catechins like epigallocatechin gallate are the main polyphenols of green tea. The neuroprotective action of epigallocatechin gallate has been previously discussed [28], particularly in reducing amyloid-β generation [46]. Cognitive decline is driven by a high amyloid-β burden [47]. Tea polyphenols have also been shown to pose a positive impact on cognition through the modulation of cell signaling and survival pathways and its iron-chelating activity [48–50]. It is worth mentioning that the amount of catechins is variable in different types of tea. Black tea or oolong tea contains less polyphenols than green tea [51], which is due to catechins undergoing enzymatic transformation during fermentation [52]. Furthermore, the amino acid theanine found in tea was found to attenuate memory impairment in mice [53]. Two previous randomized controlled trials revealed that L-theanine combined with caffeine enhanced performance on attention tasks [54, 55], with more studies needed to investigate the effect of caffeine in tea on cognitive function in isolation [29]. The cognitive protective effect of tea may be due to the synergistic effect of several of its chemical components rather than a single compound, as it contains various phytochemicals and nutrients, such as vitamin C.
Moreover, tea intake has been shown to decrease serum concentrations of total cholesterol and low-density lipoprotein cholesterol [56], decrease the risk of hypertension [57], and is associated with beneficial effects on diabetes [31]. Hypertension, dyslipidemia, and diabetes are linked with cognitive dysfunction [58, 59]. Consequently, tea intake may indirectly have a positive impact on cognitive health by decreasing the risk of relevant health problems.
Tea consumption and iron intake and Hb status
To our knowledge, this is the first population-based longitudinal study that investigated the interaction between tea intake and iron consumption in relation to cognition. We found no association between iron intake and cognition across all levels of tea consumption. However, we found that among those who did not drink tea, there was an inverse association between iron intake and cognitive function score. It is known that tea interferes with iron absorption [33]. In our previous study, we showed that increased iron consumption had an inverse association with cognitive function [34]. In the study population, the mean iron intake was well above the recommended level. Also, it was previously shown that iron intake is positively associated with disorders that induce cognitive decline in Western populations [35]. Moreover, previous animal studies indicated an association between iron consumption and iron deposits in the brain [60]. The accumulation of iron in the brain may lead to oxidative stress in the brain [61]. Iron chelation, which is a known property of tea polyphenols, has been shown to be effective in the treatment of AD and Parkinson’s disease in animal models [62]. It is worthy of note that regional differences in iron status may contribute to the inconsistent findings on the association between tea intake and cognition. Furthermore, we found that tea consumption was inversely associated with Hb. However, there was no increase in the risk of anemia, contrary to findings of previous studies reporting iron deficiency anemia and poor oral iron therapy as a result of excessive tea consumption [63].
It is noteworthy that tea is a popular cash crop worldwide, especially in China. In the past two decades, there has been a rapid industrialization of China which resulted in increased contamination of the environment by heavy metals, particularly lead. This has caused increased contamination of tea plants. Some researchers reported that Chinese green tea possessed the highest quantity of heavy metals compared to other tested tea brands [64]. The potential health implications of such metals have been previously discussed, with studies suggesting an association between higher current or past lead exposure and a decrease in current cognitive performance in the elderly [65]. Nonetheless, the adverse effects of lead may be canceled out by other protective nutritional factors in tea.
Strengths and limitations
Our study includes several strengths. We had a longitudinal population-based study design, a relatively large sample size, and representation of both males and females, all of which increase the generalizability of our findings. Also, our study included multiple measurements of dietary intake and we used multivariate analyses to control for many potentially confounding risk factors. Taking into consideration that the current study obtained information from a place where tea drinking is popular among the elderly, it increases the statistical power of our results. Although the potential for selection bias is not a major limitation in our study, due to the multistage random cluster process used in CHNS, it cannot be excluded. Nevertheless, our study lacked information on the types of tea consumed as well as iron supplements taken among the subjects of our dataset. Future studies may need to assess if types of tea, such as black or green tea, makes any difference in this relationship. Potential mechanisms of the association could not be explored due to a lack of related biomarkers. Future studies may include imaging results to better illustrate cognitive changes as well as tease out potential mechanisms. Residual confounding cannot be excluded despite adjusting for potential confounding variables. Because of the low cognitive status of the current study cohort, the use of a 24-h dietary recall can pose bias because of its reliance on memory recall. However, energy misreporting prevalence was low among subjects attending the CHNS (7.9%) [66]. Furthermore, this study measured cognition only as a global measure relying on auditory processing skills, without other cognition measures such as verbal, visual, or speed of processing. Although the cognitive screening tests were conducted over a decade ago, the relationship between tea consumption and cognition still holds strong. Nevertheless, future studies with more up to date cognitive screening are needed to substantiate the finding. Tea consummation data was derived from 1997 to 2011 surveys, the latter one may raise a concern about reversal causation. However, a mixed effort model approach was used in our analyses to cooperate the change of exposures and outcomes simultaneously. This approach offsets this potential concern [67]. Future randomized control trials may help in exploring mechanisms and supporting the association between tea consumption and cognitive function.
In conclusion, our study showed that higher tea consumption is inversely associated with cognitive impairment risk among Chinese adults, independent of sociodemographic and lifestyle factors. Higher tea consumption was associated with a lower risk of self-reported poor memory and self-reported memory decline. Additionally, tea consumption inhibits the adverse effect of high iron intake on cognitive function. Further research is needed to explore the long-term effect as well as the mechanism and relationship between tea intake and iron intake in relation to cognitive function. Given that tea is a highly consumed beverage among most parts of the world, particularly Asia, and given that mild cognitive impairment is an increasing issue in old adults globally, our study may shed light on the potential role of tea consumption in prevention of cognitive decline.