
Abstract
Background:
The effects of B vitamins on mild cognitive impairment (MCI) patients’ cognition have been mixed, suggesting the existence of moderating factors.
Objective:
A post hoc analysis of a negative B vitamin trial was performed to examine the potential modulating effect of regional brain atrophy on the cognitive response to B vitamins in MCI patients.
Methods:
In the 24-month randomized trial, 279 MCI outpatients took 500μ#x03BC;g methylcobalamin and 400μ#x03BC;g folic acid once per day or placebo tablets once per day. Sixty-four aspirin users were excluded from analysis as aspirin use has been found to have significant negative interaction effects. Subjects were followed up at months 12 and 24. The primary cognitive outcome was clinical dementia rating scale sum of boxes (CDR_SOB). In a subgroup of 83 subjects, MRI brain scans were performed at baseline to estimate regional brain atrophy ratios.
Results:
Among the trial subjects who had MRI data, B vitamin supplementation had no significant effect on CDR_SOB, despite having significant homocysteine lowering effects. The atrophy ratio of the left frontal lobe significantly moderated the effect of B vitamin supplementation on CDR_SOB, after adjusting for confounders, in that B vitamin supplementation was associated with lower CDR_SOB scores (i.e., better cognitive function) at the 24th month among those patients with above median atrophy ratios, but not among those with lower atrophy ratios, in the left frontal lobe.
Conclusion:
B vitamins may be more effective in slowing down cognitive decline in MCI patients with atrophy in the left frontal lobe.
INTRODUCTION
Mild cognitive impairment (MCI) is a transitional condition between cognitive decline associated with normal aging and more serious cognitive impairment that meets the criteria for dementia. Individuals with MCI are at higher risk of developing dementia [1]. It is possible to prevent the exacerbation of MCI at its initial stages or even reverse it back to normal cognition, but this is much less likely to occur as MCI progresses into dementia [2]. Therefore, it is crucial to intervene and prevent cognitive decline at the earliest possible time.
Some trials suggested that B vitamins (vitamin B12 and folic acid) can slow or prevent cognitive decline and brain atrophy in MCI patients [3–5]. Vitamin B12 and folate play essential roles in myelin formation and brain integrity, and thus are crucial for cognitive health. Vitamin B12 contributes to maintaining the structural and functional integrity of glial cells, myelin, and the interstitium in the nervous system by regulating the synthesis and levels of certain growth factors (e.g., the myelinotoxic nerve growth factor and the myelinotrophic epidermal growth factor) and cytokines (e.g., the myelinotoxic tumor necrosis factor-α and the myelinotrophic interleukin-6) [6]. Folate plays a critical role in one-carbon metabolism, and it regulates the survival of oligodendrocytes and myelination (e.g., by affecting the myelin lipid metabolism) in the central nervous system [7]. B vitamins may also protect cognitive function by reducing the concentration of serum/plasma homocysteine (Hcy) [5, 8]. High levels of serum/plasma Hcy can adversely affect brain health and cognitive function through cerebrovascular and neurotoxic mechanisms, such as oxidative stress, DNA damage, impairment of neurotransmitters, apoptosis, excitotoxicity, and amyloid deposits [8, 9]. As methionine synthase is a vitamin B12 and folate-dependent enzyme that catalyzes the remethylation of Hcy to methionine, supplementation of B vitamins could facilitate the remethylation process and thereby reduce serum/plasma Hcy and its adverse effects, especially among subjects with a suboptimal status of Hcy, folate, and vitamin B12 [10].
However, some trials, including our recent trial, failed to detect the beneficial effects of B vitamins on cognitive function and brain health [11–13]. The mixed results suggest the existence of factors that moderate the effects on B vitamins. Some trials showed that the cognitive benefits of B vitamins were evident when the omega-3 fatty acid concentration was high but not when it was low [14, 15]. We have recently found a negative interaction effect of aspirin on the cognitive response to vitamin B12 and folic acid in older people with MCI [13, 17]. In addition, we found that those who did respond to B vitamins in our trial had activation of Warburg effects on metabolomics analysis [18]. Further investigations into the results of subgroup analysis may shed light on how B vitamins may impact the cognitive decline in older people with MCI.
Cognitive decline in amnestic MCI (aMCI) is primarily driven by Alzheimer’s disease (AD). The onset of cognitive decline in AD is often preceded or co-existed by brain atrophy, and AD appears to affect some brain regions, e.g., hippocampus, more than others at least in its early phase [19]. Moreover, vitamin B12 or folate deficiency has been found to cause demyelination or atrophy more in frontal and temporal lobes [20]. The potential modulating effect of regional brain atrophy on the cognitive response to B vitamins may therefore shed light on the subtypes of MCI patients who are more likely to respond to B vitamins.
MATERIALS AND METHODS
The Hong Kong version of the Montreal Cognitive Assessment (MoCA) was used to screen 975 older outpatients (≥65 years old) for MCI (with a MoCA score below 22) [21] from April 2013 to July 2016. Following the written informed consent, each patient had a fasting blood sample taken and tested, and his/her cognitive state was clinically diagnosed. Clinically diagnosed MCI patients were invited to participate in a randomized trial if they did not meet any one of the following exclusion criteria: dementia or peripheral neuropathy, clinical depression, renal failure, anemia, disabling stroke, hypothyroidism, receiving centrally acting medications or B vitamin supplementation, serum active vitamin B12 <28 pmol/L, serum folate <9.5 nmol/L, serum creatinine >200μ#x03BC;mol/L, serum Hcy concentration <10μ#x03BC;mol/L (as previous studies showed no significant B vitamin effect on cognition in subjects with serum Hcy lower than this level [3, 17]), and having no reliable caregiver/family member reporting the subjects’ cognitive functioning weekly. In the end, 279 subjects participated in the randomized trial. These subjects were randomly assigned to the active B vitamin supplementation group (138 subjects, of whom 107 were non-aspirin users) and the placebo group (141 subjects, of whom 108 were non-aspirin users). Subjects in the active group took two active tablets (methylcobalamin 500μ#x03BC;g and folic acid 400μ#x03BC;g) once per day, while those in the placebo group took two similar-looking placebo tablets once per day for 24 months.
The subjects were reviewed by geriatricians 12 months and 24 months after the baseline. Cognitive function assessments and fasting blood assays (including measurements of serum Hcy, active vitamin B12, folate, and other biochemical markers) were done at baseline and each follow-up. The primary cognitive outcome was the Chinese version clinical dementia rating scale (CDR) sum of boxes (CDR_SOB) score [22], which reflects cognitive functioning in six domains: memory, orientation, community affairs, judgment and problem solving, home and hobbies, and personal care. CDR_SOB scores range from 0 to 18, with a higher score indicating a worse level of cognitive function. The secondary cognitive outcomes were executive function (transformed to Z score) measured by the Category Fluency Test and memory (transformed to Z score) measured by the International Shopping List Test, with higher Z scores indicating higher levels of executive function and memory, respectively.
MRI scans were performed on a subsample of 52 eligible subjects (of whom 41 were non-aspirin users) in the active group and 53 subjects (of whom 42 were non-aspirin users) in the placebo group at baseline and the 24-month follow-up. T1-weighted acquisitions were carried out using a Siemens 1.5T MRI system. Structure Image Evaluation using Normalization of Atrophy (SIENA), an established automated method, was used to estimate the atrophy rate (percentage per year) of the whole brain from baseline up to 24 months after the baseline [23]. An automated model of AccuBrain®[24, 25], a validated tool that has been used in clinical practice and research, was used to measure morphometrics (volumes, volume ratios, atrophy ratios) of different brain lobes. The atrophy ratio of a certain lobe refers to the ratio of the volume of cerebrospinal fluid (CSF) to the brain parenchyma in the lobe [26], with a higher value indicating more severe atrophy in the lobe.
The randomized trial procedures are displayed in Fig. 1. More details about the methodologies (e.g., subject selection, fasting-blood assay, randomization steps) have been described elsewhere [13]. The trial was registered at the Clinical Trials Registry of the Centre for Clinical Research and Biostatistics (CUHK_CCT00373), and the research ethics approval was obtained from the medical ethics committee of The Chinese University of Hong Kong and New Territories East Cluster of Hospital Authority of Hong Kong.
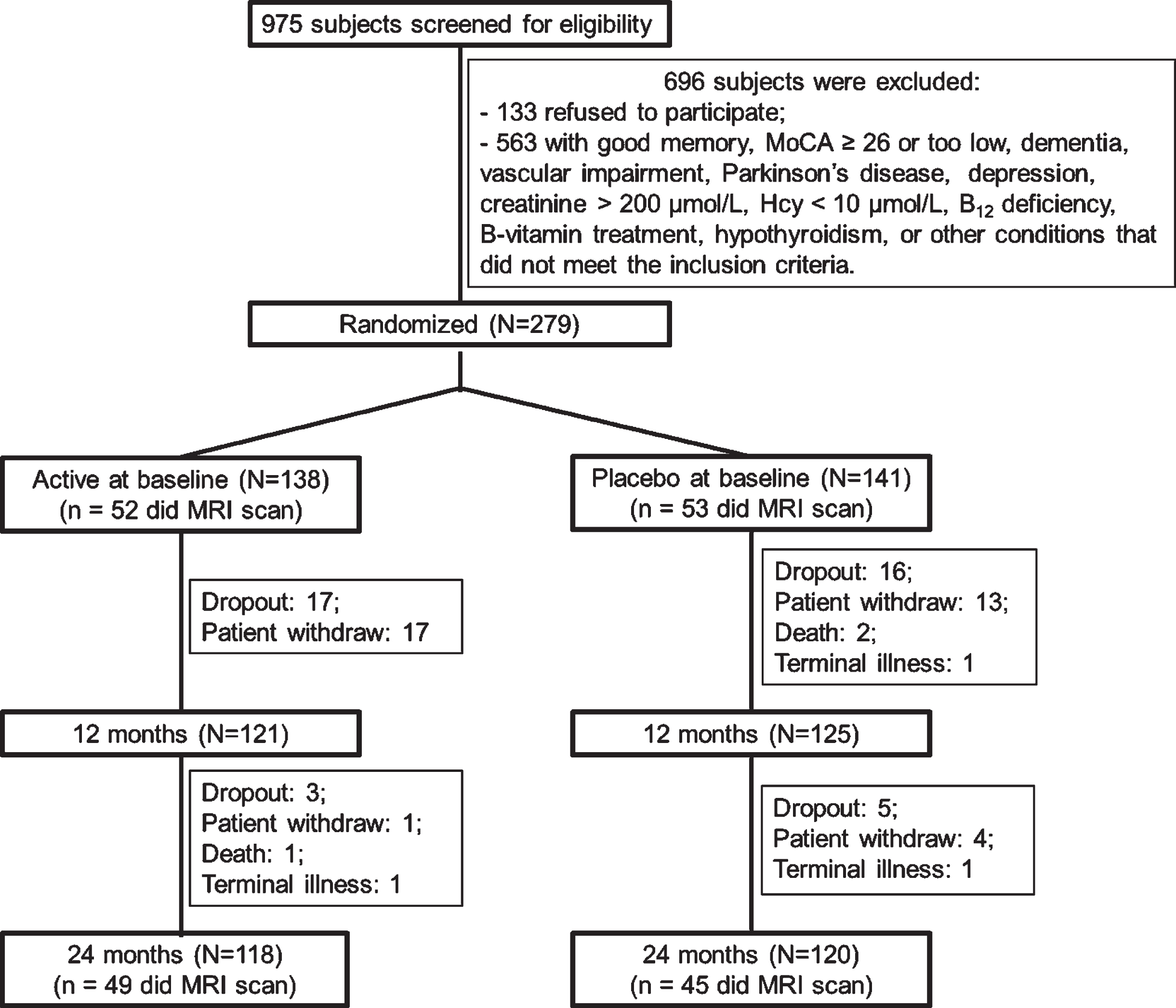
Flow chart illustrating the trial design and study procedures.
Statistical analysis
The study aimed to examine whether the atrophy ratios in different brain regions (particularly the frontal regions) moderated the effect of B vitamin supplementation on the subsequential cognitive function among MCI patients without taking aspirin. For this purpose, bivariate correlations were calculated to identify brain lobes whose atrophy ratios at baseline correlated with follow-up changes in CDR_SOB in placebo group subjects. This analysis was based on the rationale that if B vitamins affected cognition differently depending on atrophy in a certain brain region, atrophy of this brain region should be related to cognitive changes. The analysis results allowed us to narrow down our focus on the most critical brain regions.
Linear regression analyses were then performed to examine the interaction effects of atrophy ratios in the identified lobes and trial group (active versus placebo) on CDR_SOB at the 24-month follow-up, adjusting for demographics (age, sex, and education) and baseline CDR_SOB. All analyses were based on intention-to-treat, and all statistical tests were two-sided. p values (or Bonferroni corrected p values)<0.05 were considered statistically significant. All statistical analyses were conducted with SPSS 28.0 (IBM Corp., in Armonk, NY, USA).
RESULTS
Sample characteristics
The present study focused on non-aspirin users in the randomized trial. Table 1 shows their baseline clinical characteristics. Independent sample t-tests and chi-square tests showed no significant differences in these characteristics between all non-aspirin users in the active group and those in the placebo group (ps≥0.064; except for executive function Z score, p = 0.014), between MRI scanned non-aspirin users in the active group and those in the placebo group (ps≥0.168), between non-aspirin users who were MRI scanned and those who did not in the active group (ps≥0.049), and between non-aspirin users who were MRI scanned and those who did not in the placebo group (ps≥0.103).
Characteristics (Mean and SD) of non-aspirin users at baseline and group comparison results (p values)
CDR_SOB, Clinical Dementia Rating sum of boxes. Only subjects who underwent MRI scans had their brain atrophy measured. Chi-square tests were conducted to compare the sex ratio between groups, and independent-sample t-tests were conducted to compare the other characteristics between groups.
Effects of B vitamin supplementation on serum biochemical markers and cognition
As illustrated in Fig. 2, repeated measures ANOVAs revealed significant Time (baseline, 12 months, 24 months)×Trial (active, placebo) interaction effect on serum concentrations of active vitamin B12 [F(2, 142) = 30.386, p < 0.001, partial η2 = 0.300], folate [F(2, 142) = 49.653, p < 0.001, partial η2 = 0.412], and Hcy [F(2, 140) = 128.57, p < 0.001, partial η2 = 0.369] among non-aspirin users who received MRI scan. Follow-up simple effect analyses showed that serum active vitamin B12 and folate concentrations significantly increased and Hcy concentration significantly decreased with time in the active group, while the concentrations of all these markers remained stable in the placebo group. The interaction effect of Time×Trial was non-significant on CDR_SOB [F(2, 142) = 0.347, p = 0.707, partial η2 = 0.005], executive function Z score [F(2, 142) = 1.234, p = 0.294, partial η2 = 0.017], and memory Z score [F(2, 142) = 2.829, p = 0.063, partial η2 = 0.044]. The results showed that B vitamin supplementation effectively changed serum concentrations of B vitamins and Hcy as expected but did not affect cognition in non-aspirin using MCI patients.
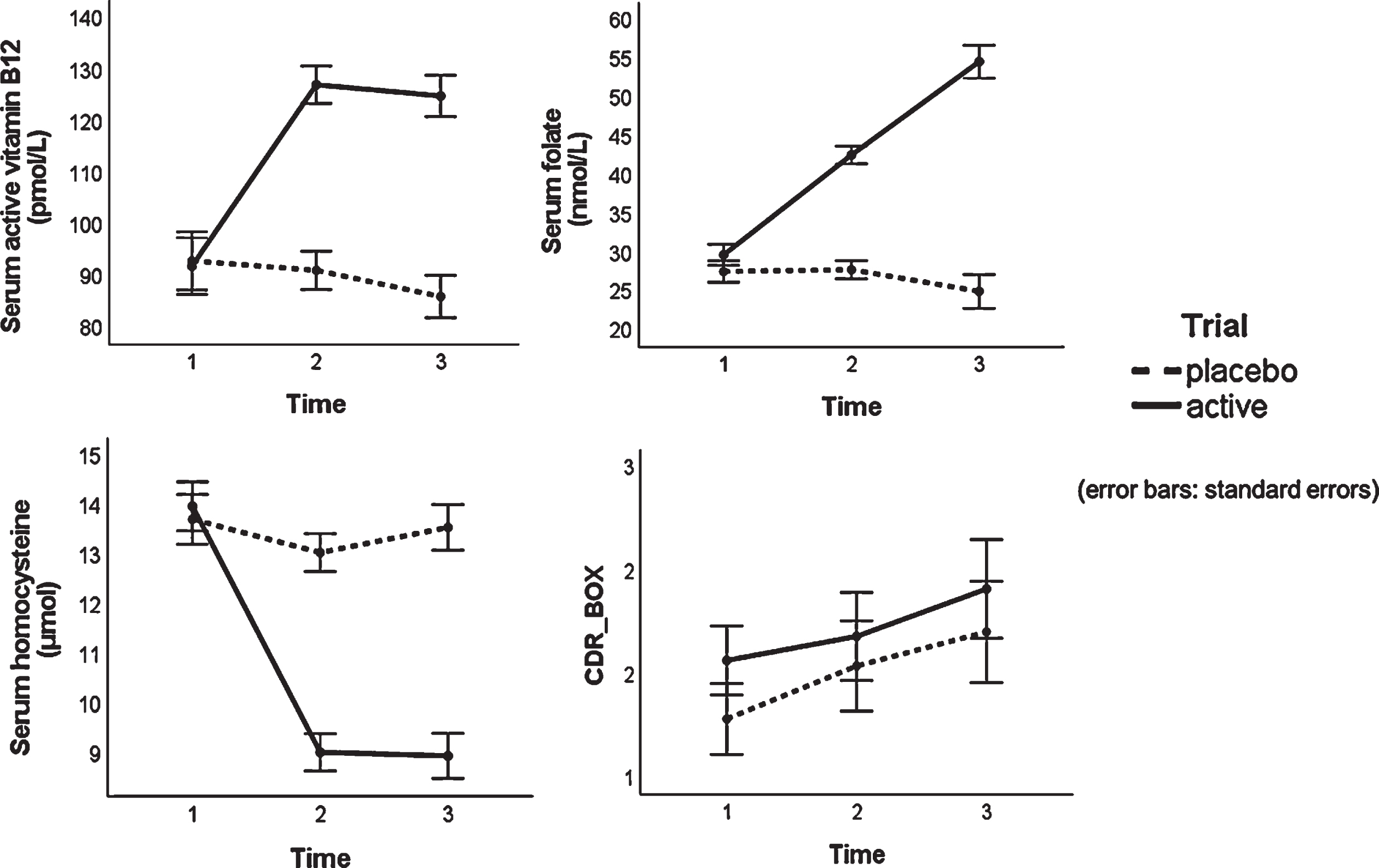
Time×Trial interaction effects on the serum active vitamin B12, folate, homocysteine, and CDR_BOX score among non-aspirin using MCI patients who received MRI scans.
Interaction effects of trial group and brain atrophy ratios on cognition
Zero-order correlations were calculated to identify brain lobes whose atrophy ratios were associated with the subsequential changes in the primary cognitive outcome (ΔCDR_SOB score) and the secondary cognitive outcomes (ΔExecutive function Z score and ΔMemory Z score) among the MRI-scanned non-aspirin users in the placebo group. We focused specifically on the frontal lobes, temporal lobes, cingulate cortex, and insula because B vitamins have particularly significant effects on these frontal regions (or the frontal parts of these regions) [20, 27]. Subjects in the active group were excluded from these correlation analyses because B vitamin supplementation might have ameliorated cognitive decline and thus would disguise the zero-order correlations between the atrophy ratios of brain lobes and cognitive changes. As displayed in Table 2, the atrophy ratios in the left frontal lobe, left temporal lobe, left insula, and right cingulate cortex at baseline were significantly associated with increases in subsequential CDR_SOB, namely decreases in cognitive function (p < 0.006, the threshold p value was Bonferroni adjusted for multiple testing).
Correlations (r and p) between atrophy of brain lobes at baseline and follow-up changes in cognition and brain among MRI-scanned non-aspirin users in the placebo group (n = 42)
L, left; R, right; AR, atrophy ratio; Δ, change from baseline to 24 months after baseline. Significance threshold was adjusted to p = 0.05/8 = 0.006 using Bonferroni correction. Significant correlations are highlighted in bold.
By linear regression analysis, we next investigated whether the baseline atrophy ratios in the five lobes identified above moderated the effect of B vitamin supplementation on cognition. Specifically, the interaction effect of Trial (active versus placebo)×Atrophy Ratio of a specific brain lobe (as a continuous variable) on CDR_SOB at the 24-month follow-up was examined, adjusting for demographics (sex, age, educational level) and baseline CDR_SOB. The results showed a significant interaction of Trial×Atrophy Ratio in the left frontal lobe (b = –0.109, β= –0.183, SE = 0.038, t = –2.879, p = 0.005), but no significant interactions of Trial×Atrophy Ratio in the other lobes (ps≥0.193). The interaction effect of left frontal atrophy on CDR_SOB at month 12 was not significant (b = –0.025, β= –0.051, SE = 0.031, t = –0.796, p = 0.429).
Further exploratory regression analyses showed no significant main or interaction effects of Trial×Atrophy Ratio on executive function Z score or memory Z score, adjusting for baseline cognitive Z score and demographics (ps≥0.261). The interaction effects on the whole brain atrophy rate (% per year) and the changes in the lobes’ volumes/atrophy ratios during the trial were also not significant (ps≥0.106).
To decompose the interaction effect of left frontal atrophy ratio, subjects were divided into two groups (i.e., the high and the low frontal atrophy groups) by the median value of atrophy ratio in the left frontal lobe (53.05), and then the predictive effect of Trial on CDR_SOB at the 24-month follow-up was examined separately for the two groups. Results showed that the supplemented subjects had significantly lower CDR_SOB at the 24-month follow-up in the high frontal atrophy group (b = –0.529, β= –0.164, SE = 0.223, t = –2.372, p = 0.023) but not in the low frontal atrophy group (b = 0.243, β= 0.069, SE = 0.344, t = 0.708, p = 0.484), with demographics and baseline CDR_SOB being adjusted.
In order to examine the potential association between the left frontal atrophy ratio and the severity of AD, further correlation analyses were performed on baseline cognitive scores and hippocampal volume ratios (left and right) in all included trial subjects at baseline. Left frontal atrophy correlated significantly with age (r = 0.375, p < 0.001), CDR_SOB (r = 0.243, p = 0.027), memory Z score (r = –0.318, p = 0.004), but not with hippocampal volume ratios (r = 0.006, p = 0.954). Left frontal atrophy ratio did not correlate significantly with serum homocysteine (r = 0.169, p = 0.127), vitamin B12 (r = –0.034, p = 0.761), or folate (r = 0.069, p = 0.537). Prospectively, left frontal atrophy correlated significantly with whole brain atrophy rate (partial r = 0.512, age-adjusted p = 0.002) among placebo group subjects.
DISCUSSION
This post hoc analysis showed that B vitamin supplementation attenuated cognitive decline (indicated by CDR_SOB score) in older MCI patients with more atrophy in the left frontal lobe, but not in those with less frontal atrophy.
There is evidence that brain atrophy precedes changes in cognitive functioning. This may explain the correlations between brain atrophy in regions (e.g., the temporal, insula, and cingulate lobes) commonly affected by AD and changes in cognitive functioning as estimated by CDR_SOB [28]. Interestingly, only left frontal lobe atrophy correlated significantly with whole brain atrophy rate which is a recognized marker of the progression of AD. Neurodegeneration in AD usually starts in the hippocampus and the temporal lobe. Frontal lobe atrophy is a relatively late phenomenon [29, 30]. This finding suggested that AD progresses more rapidly once the frontal lobe became involved. The asymmetry of the significance of frontal lobe atrophy is also noteworthy. Similar findings have been reported previously [31, 32]. It is as yet unexplained why AD appears to involve the left brain earlier than the right.
The subjects of this trial had significantly elevated serum homocysteine at baseline, and the B vitamins were effective in lowering it to below 10μ#x03BC;mol/L which is probably a safe level for cognition [33]. As the trial excluded those with low serum active vitamin B12 and folate, the cognitive effects of B vitamins in this trial were therefore probably not due to the correction of the deficiency of these vitamins. Therefore, the cognitive effects of B vitamins were attributed to the lowering of homocysteine which may exacerbate AD and cerebrovascular disease. As the MCI trial subjects were selected for the amnesic type and the burden of small vessel disease on MRI was low, the cognitive effects of B vitamins were likely to be mediated through their effects on AD changes. This is consistent with a post hoc analysis of the VITACOG trial, which showed that B vitamins slowed MCI patients’ cognitive decline by reducing AD-related brain atrophy [28]. This is somewhat consistent with the findings of the metabolomics analysis of the responders to B vitamins in this trial, in which there was clear evidence of the activation of the Warburg effect pathway [18]. This pathway is an abnormal aerobic glycolysis pathway adopted by defective neurons in an attempt to stave off apoptosis [34].
The key finding of this analysis is that B vitamins improved cognitive functioning in those with more left frontal atrophy, the interaction term being highly significant. One possible explanation for this finding is that B vitamins were only effective in improving cognitive functioning when the AD was at its later stage when the frontal lobe became involved. The significant correlations of left frontal atrophy with greater age and CDR_SOB scores and lower memory Z scores at baseline, and with whole brain atrophy rates prospectively were consistent with that.
However, it was somewhat unexpected that left frontal atrophy was not associated with hippocampal volume ratio. This may be attributed to our selection of subjects with higher serum homocysteine. There is some evidence that the frontal lobe may be more susceptible to the detrimental effects of homocysteine. For example, a sizeable cross-sectional study found that moderately elevated plasma homocysteine was associated with AD-related atrophy of white matter in brain regions, including the frontal and other lobes, in MCI patients [35]. Myelin damage is one of the recognized features of hyperhomocysteinemia [36]. The maintenance of myelin health may therefore be an important element of the therapeutic effect of B vitamins in older people with MCI. In the post hoc analysis of the VITACog trial, the positive cognitive and brain atrophy responses to B vitamins appeared to be confined to those with high baseline serum omega3 [14], and there is experimental evidence that omega3 can repair myelin damages [37]. Taken together, B vitamins may benefit brain health by facilitating myelin repair from omega3.
Aspirin users were excluded from data analysis because two randomized trials of B vitamins in older people with MCI found a negative interaction effect between aspirin use and B vitamin supplementation on brain atrophy and cognitive functioning [3, 13]. There is some evidence that aspirin inhibits dihydrofolate reductase (DHFR) which is essential for the slow conversion of folic acid to active forms of folate [13, 39]. The importance of DHFR in the cognitive responses to B vitamins was supported by the interaction effect of DHFR gene polymorphism on the cognitive responses to B vitamins [16].
A limitation of this study is the relatively small sample size and short trial duration. Another limitation is that the present study only included MCI patients. Future studies could also examine the effects of B vitamin supplementation in other populations, e.g., normal-aging older adults.
Despite these limitations, the present study provides novel evidence showing that the effect of B vitamin supplementation varies with brain atrophy conditions: The supplementation may be particularly effective in slowing down cognitive decline in MCI patients with more atrophy in the (left) frontal lobe. The study contributes to a better understanding of B vitamins’ effects on the brain and cognition.