
Abstract
Background:
Subjective cognitive decline (SCD) is considered as a preclinical hallmark of Alzheimer’s disease (AD). However, the characteristics of SCD associated with amyloid pathology remain unclear.
Objective:
We aimed to explore the associations between SCD characteristics with amyloid pathology.
Methods:
Using logistic regression analyses, we analyzed the associations between cerebrospinal fluid (CSF) amyloid pathology with AD risk factors, SCD-specific characteristics (onset of SCD within the last five years, age at onset ≥60 years, feelings of worse performance, informant confirmation of complaints, worries, other domains of cognition complaints), as well as subthreshold depressive and anxiety symptoms among individuals with SCD.
Results:
A total of 535 SCD individuals with available CSF Aβ42 information from the Chinese Alzheimer’s Biomarker and LifestylE (CABLE) study (mean age of 63.5 years, range 40 to 88 years; 47.10% female) were enrolled. The characteristics of informant confirmation of complaints (OR, 95% CI = 2.00, 1.19–3.36), subthreshold depressive symptoms (OR, 95% CI = 2.31, 1.05–5.09), and subthreshold anxiety symptoms (OR, 95% CI = 2.22, 1.09–4.51) were found to be significantly associated with pathological amyloid in multivariate analyses when adjusting for age, sex, education, and APOE ɛ4. Besides, age and females were observed risks for amyloid pathology in subscale analyses. Nonetheless, we did not find any associations of other SCD-specific characteristics with amyloid pathology in this study.
Conclusion:
Our study suggested that informant confirmed complaints and subthreshold psychiatric symptoms might be critical for discriminating AD-related SCD from non-AD related SCD.
INTRODUCTION
With the aging of population, Alzheimer’s disease (AD) has brought us many challenges: a dramatically growing prevalence, no effective targeted treatments, and a heavy societal burden [1]. The core pathology of AD is extracellular amyloid deposition, which is followed by hyperphosphorylated tau and neurodegeneration [2]. Currently, the NIA-AA Research Framework recommends the process of AD as a continuum with a biological construct and proposes a numeric scheme which separates AD continuum into six stages depend on cognitive performance [3]. With amyloid pathology yet without objective cognitive impairment, stage 1 and 2 are considered as a preclinical state, which are important stages for cognitive interventions [4–6].
Subjective cognitive decline (SCD) is defined as self-reported cognitive decline yet with normal objective cognitive performance [7]. Individuals with SCD were more likely to have amyloid pathology [8, 9]. SCD participants with abnormal amyloid pathology are considered at stage 2 of AD continuum and to had higher risks of subsequent progression to mild cognitive impairment (MCI) or AD [10–12]. Although SCD is considered as the early manifestation of AD [7, 14], most individuals with SCD would not progress to cognitive decline and AD due to various causes underlying SCD [15]. Therefore, identification SCD individuals that associated with amyloid positivity is critically important. To improve the possibility of abnormal amyloidosis in individuals with SCD, Jessen et al. proposed several characteristics known as SCD plus list in 2014 [7]. The characteristics such as APOE ɛ4, worries, and informant confirmation were demonstrated to be associated with amyloid pathology and subsequent AD in several studies [16–18]. In addition, psychiatric symptoms in SCD patients were recently revealed as important predictors for AD [19–21]. And the associations of risk factors such as sex and education with amyloid pathology are still unclear among individuals with SCD [22, 23]. Notably, the results were not always consistent due to the differences in study settings, SCD assessment methods, and characteristics of populations [24, 25]. Also, there is still no research on SCD-plus characteristics associated with amyloid pathology in China. It is necessary to report the relationships of SCD characteristics with amyloid pathology among different races and populations.
We examined the associations of amyloid pathology with general risk factors for AD (including age, gender, education, and APOE ɛ4), SCD-specific characteristics in the SCD plus list, and subthreshold depressive and anxiety symptoms among northern Han Chinese population with SCD.
METHODS
Study participants
All participants were enrolled from the Chinese Alzheimer’s Biomarker and LifestylE (CABLE) study, an ongoing large-scale cohort since 2017, which aimed to explore risk factors and biomarkers of AD in the northern Chinese Han population aged from 40 to 90 years old [26]. The current study was cross-sectional and all subjects were consecutive through face-to-face interviews. Participants were recruited from Qingdao Municipal Hospital, Shandong Province, China, and through both advertising and clinical practice, and most were not from memory clinic. Neurology outpatients and participants using lumbar anesthesia for surgical treatment of noninflammatory diseases were the main sources, including benign prostatic hyperplasia, stress incontinence, varicose veins of the lower limbs, and rectal polyps. The exclusion criteria are as follows: (a) infection of the central nervous system, epilepsy, head trauma, and major neurological disorders; (b) major psychological disorders; (c) severe systemic diseases (e.g., malignant tumors); (d) family history of genetic diseases. All individuals experienced comprehensive clinical, psychiatric, and neuropsychological evaluations via face-to-face interviews and collections of biological samples (blood and CSF sample). We inquired about the baseline information of age, sex, and education years at study entry. And the questionnaire of SCD was assessed according to SCD-I and SCD plus recommendations [7]. We used the Chinese-modified Mini-Mental State Examination (CM-MMSE) for cognitive test, the 17-item version of the Hamilton Depression Rating Scale (HAMD) for depression evaluation, the Hamilton Anxiety Rating Scale (HAMA) for anxiety assessment, and the basic Activities of Daily Living score (ADL) for assessment of activities of daily living.
1,730 individuals were recruited in total. Among them, 947 were cognitively normal, 210 were objectively impaired, and 38 had significant depressive (HAMD score ≥7) or anxiety (HAMA score ≥7) symptoms, which were excluded due to eligibility criteria. A total of 535 subjects who had subjective cognitive complaints but no objective impairment (CM-MMSE: ≥27 for >6 years of education, ≥23 for 1∼6 years of education, ≥20 for 0 years of education) [27] were finally enrolled. Participants with a HAMD or HAMA score of 0–6 were considered as having subthreshold depressive or anxiety symptoms. Written informed consent was obtained from all subjects or their proxies. The CABLE study was approved by the Ethics Committee of Qingdao Municipal Hospital and conducted following the Declaration of Helsinki.
Diagnostic criteria and characteristics of SCD
The questionnaires were used to assess the subjective cognitive function and the characteristics of SCD. Firstly, individuals were asked, “Do you think your memory is declining compared to what it used to be?”. If their answers were “yes”, they were considered as having SCD. Then, the data on the characteristics of SCD in the SCD-plus list were collected via the following questions: (a) How long has memory decline been around? (b) Are you worried about your memory decline? (c) Is there any decline in other cognitive domains such as language, organizing/planning, and attention/concentration? (d) Do you have a worse memory performance than your peers? (e) Has your SCD ever been perceived by your caregivers or proxies (yes/no/unclear)? In the end, professional investigators confirmed whether SCD was caused by drug and substance abuse such as alcohol, or other severe medical conditions.
Based on these questionnaires, we obtained the SCD-specific characteristics: onset of SCD within the last 5 years, age at onset ≥60 years, feelings of worse performance, informant confirmation of complaints, worries about the complaints, complaints in other domains of cognition, language-specific complaints, planning-specific complaints, attention or concentration-specific complaints.
CSF amyloid assessment
Amyloid pathology was measured by CSF amyloid-β (Aβ), which was extracted with a standard lumbar puncture after discarding the first 1–2 ml. CSF samples were processed within two hours, including being centrifuged at 2000×g for 10 min and being stored in an enzyme-free EP (Eppendorf) tube at –80°C. The maximum times of thaw/freezing cycle were two. CSF Aβ42 was assessed by professional experimenters using ELISA kits (Innotest β-AMYLOID (1–42) [catalog number: 81583]; Fujirebio, Ghent, Belgium). Also, phosphorylated tau (p-tau) levels were measured by PHOSPHO-TAU (181p) [catalog number: 81581] (Fujirebio, Ghent, Belgium). We used a single lot of antibodies and plates to eliminate variation. Besides, the within-batch coefficient of variation (CV) was <5%, and the inter-batch CV was <15%.
After screening for the outside 3 standard deviation (SD) values, the participants within the lowest tertile of CSF Aβ42 (<189.5 pg/mL) in the CABLE study were defined as having Aβ pathology. 189 (35.33%) of the SCD participants were thought to have amyloid pathology. The proportion was in accordance with that of the DELCODE study [12].
APOE ɛ4 genotyping
DNA was extracted from fasting blood samples, and then the extracted DNA was separated and stored in an enzyme-free EP tube at –80°C until the APOE genotyping. APOE SNPs (rs7412 and rs429358) were genotyped using restriction fragment length polymorphism technology. Individuals with one or two copies of APOE ɛ4 alleles were defined as APOE ɛ4 carriers.
Statistical analyses
Participant characteristics were illustrated using descriptive statistics. Differences between amyloid positive group and amyloid negative group were analyzed using the t-test (for continuous variables) and chi-square test (for categorical variables). Logistic regression models were applied to investigate the associations of independent variables including AD risk factors, SCD-specific characteristics, and subthreshold neuropsychiatric symptoms with the dependent variable of amyloid pathology: firstly, univariate logistic regression analyses were employed to determine the significant factors (Analysis 1); secondly, the significant SCD-characteristics, age, sex, years of education, and APOE ɛ4 were combined in one multivariate logistic regression model (Analysis 2); thirdly, we investigated the effects of remaining variables which were not significant in Analysis 1 on amyloid pathology by adding them one by one in the model used in Analysis 2 (Analysis 3). Besides, we tested the interaction effects of age, sex, and APOE ɛ4 on the correlation between all the variables and amyloid pathology in the models applied in Analysis 2 and 3. The cross product was used to judge for p value. For any significant strata effect (p < 0.1), subgroup analyses according to age (≥60 or <60), gender and APOE ɛ4 were conducted. Sensitivity analysis was explored to further adjust for hypertension, diabetes, smoking, stroke, and coronary heart disease in Analysis 2. A two-tailed p value <0.05 was considered significant. All statistical analyses were performed using the package “car”, “lm”, “forestplot” in R 4.0.3 software.
RESULTS
Participant characteristics
We included a total of 535 participants with SCD, ranging in age from 40 to 88 years, with a mean age of 63.5 (SD = 9.70). Among them, 252 (47.10%) participants were female; 72 (15.45%) participants were APOE ɛ4 carriers. The mean MMSE score was 28.16 (SD = 1.87). Participant characteristics in amyloid positive group and amyloid negative group were shown in Table 1. There were no differences in age, sex, years of education, APOE ɛ4, and p-tau levels between the two groups. Participants with amyloid pathology were more likely to have subthreshold depressive or anxiety symptoms, and their memory complaints were also more likely to be confirmed by informants, compared with amyloid negative group.
Population characteristics based on amyloid status
The statistically significant results have been bolded. SD, standard deviation; APOE, apolipoprotein E; P-tau, phosphorylated tau 181. *The difference among groups was examined by the t test. †The difference among groups was examined by the chi-square test.
Associations between SCD characteristics and amyloid pathology
In univariate analyses, informant confirmation of complaints, subthreshold depressive symptoms, and subthreshold anxiety symptoms were suggested to be significantly associated with amyloid pathology in SCD population (Fig. 1). The associations of general AD risk factors and other SCD-specific characteristics with amyloid pathology were not recorded. In Analysis 2, the associations of amyloid pathology with informant confirmation of complaints (OR, 95% CI = 2.00, 1.19–3.36), subthreshold depressive (OR, 95% CI = 2.31, 1.05–5.09), and anxiety symptoms (OR, 95% CI = 2.22, 1.09–4.51) remained significant when we added age, sex, years of education, and APOE ɛ4 to one logistic regression model (Fig. 2). The remaining SCD-specific features including onset of SCD within the past 5 years, age at onset of SCD ≥60 years, feelings of worse performance, worries about the complaints, and subjective decline in other cognitive domains were not related to amyloid pathology in Analysis 3 (Fig. 2).
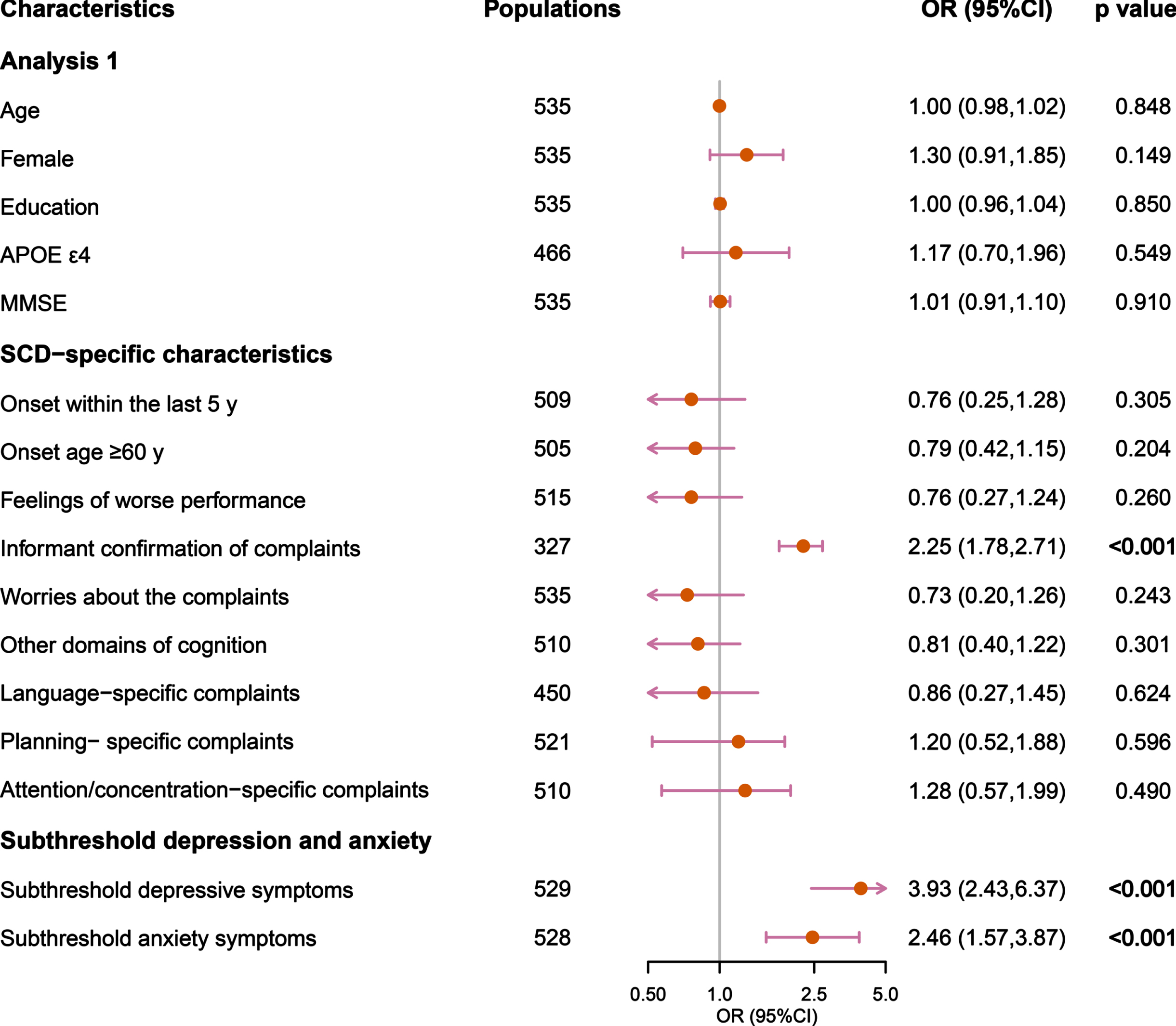
Analysis 1 for associations of SCD characteristics with amyloid pathology. In Analysis 1, univariate logistic regression models were used to investigate the associations between variables with amyloid pathology. p-value <0.05 was considered significant. OR, odds ratio; 95% CI, 95% confidence interval.
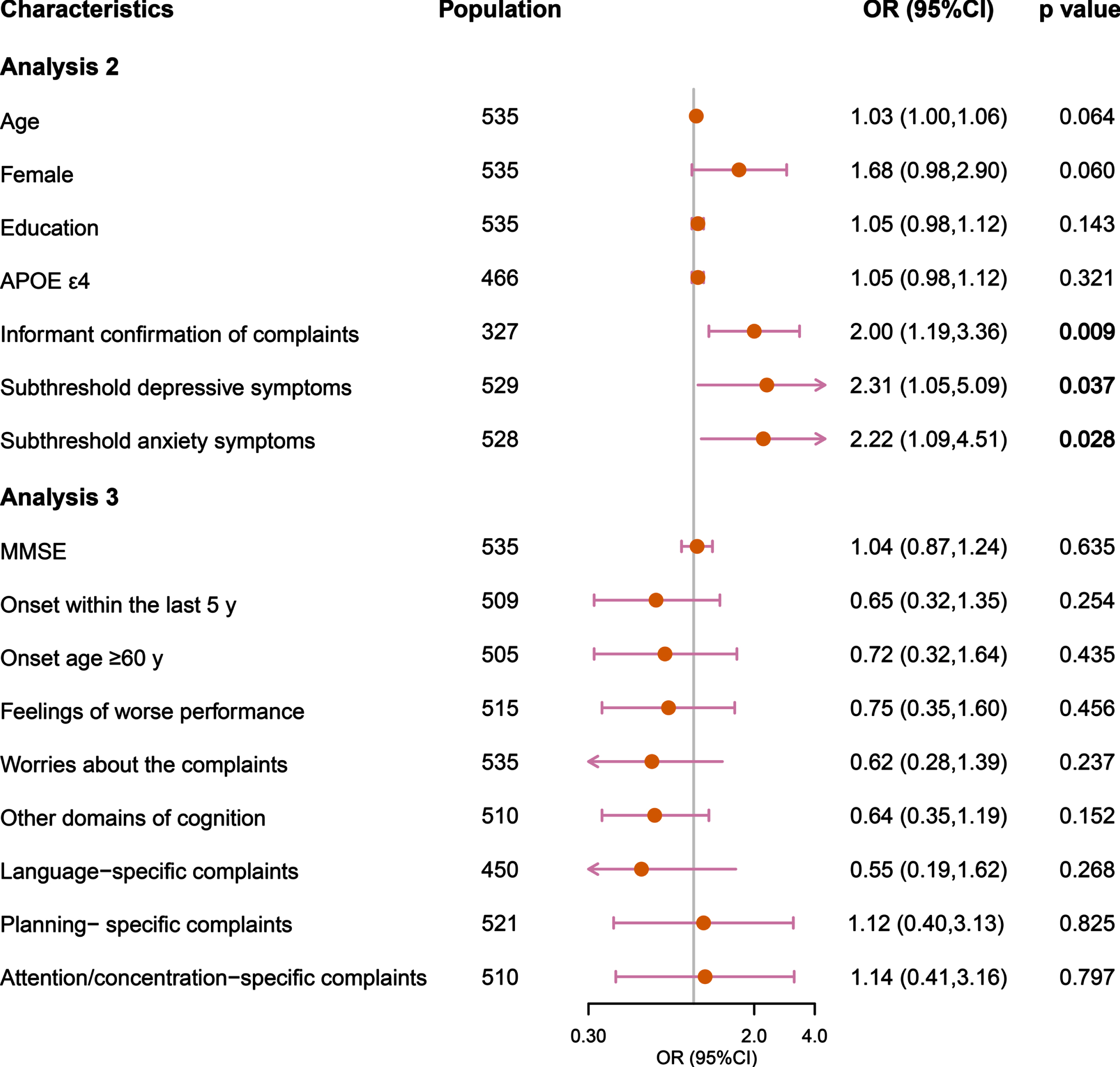
Analysis 2 and 3 for associations of SCD characteristics with amyloid pathology. In Analysis 2, multivariate logistic regression models were used to investigate the associations between age, sex, education, APOE ɛ4, informant confirmation, subthreshold depressive and anxiety symptoms with amyloid pathology. In Analysis 3, the remaining variables were added one-by-one individually to analysis 2. p-value <0.05 was considered significant. OR, odds ratio; 95% CI, 95% confidence interval
Interaction and subgroup analyses
Interaction between age and APOE ɛ4 (p = 0.0592), and interactions of sex with subthreshold depressive (p = 0.0797) and anxiety symptoms were revealed ((p = 0.0319) (p < 0.1, Supplementary Table 1). Subgroup analyses stratified by age, sex, and APOE ɛ4 were subsequently conducted. Informant confirmed complaints was suggested to be risk factor for amyloid pathology only in the elderly, yet not in the middle-age. Subthreshold depressive and anxiety symptoms were associated with amyloid pathology in females but not in males. Moreover, among APOE ɛ4 carriers and males, age was significantly associated with amyloid pathology. In middle-age individuals, female was suggested risk for amyloid pathology (Fig. 3). No relationships of amyloid pathology with other SCD characteristics in subgroup analyses were found (Supplementary Figure 1).
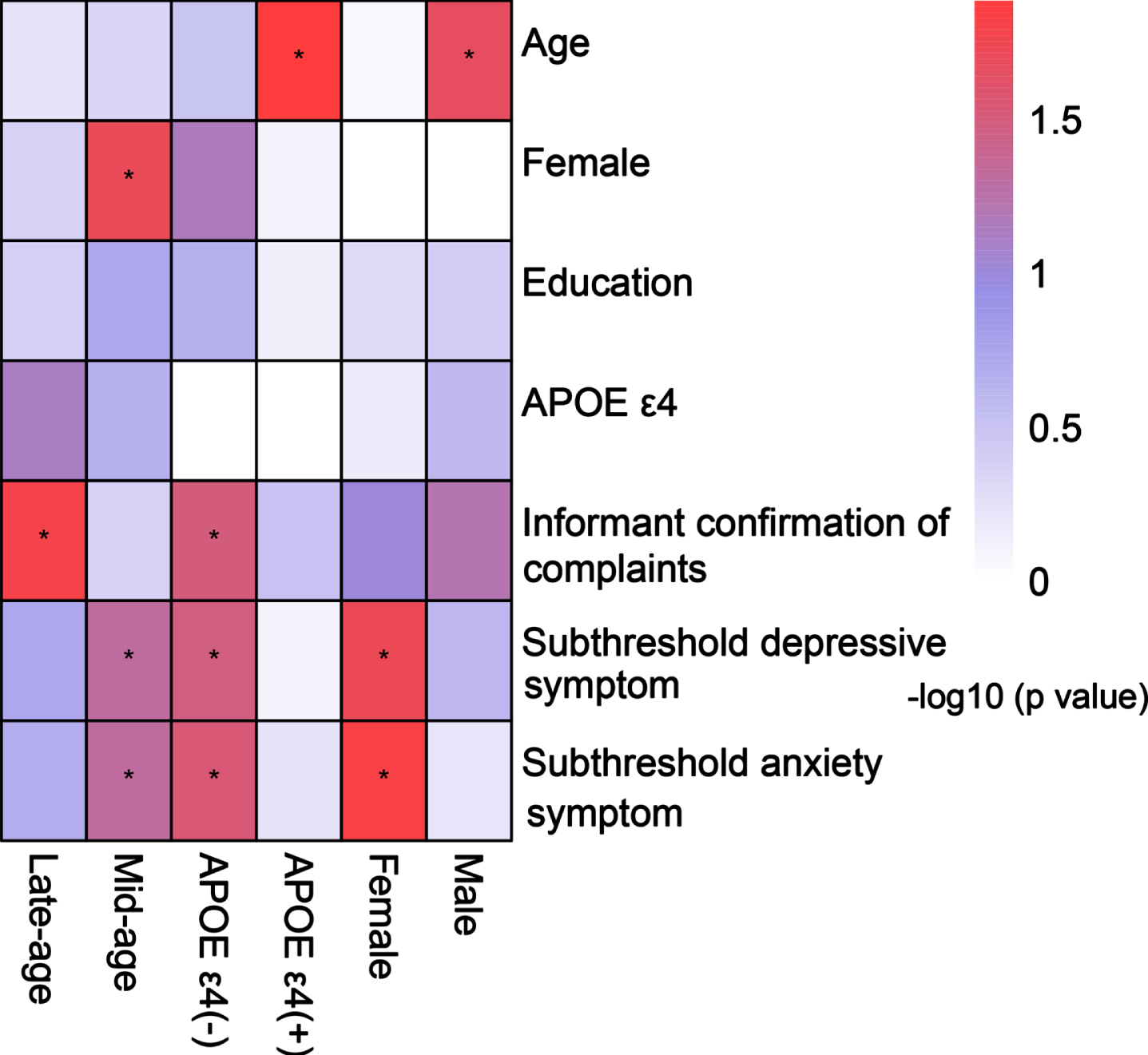
Subgroup analyses of associations between SCD characteristics with amyloid pathology in Analysis 2. Subgroup analyses were conducted according to late age (≥60 years) or middle age (<60 years), APOE ɛ4 status, and genders. In Analysis 2, multivariate logistic regression models were employed to investigate the associations of age, sex, education, APOE ɛ4, informant confirmation, subthreshold depressive and anxiety symptoms with amyloid positivity. Asterisks represents statistical significance (*p < 0.05).
Sensitivity analysis
Sensitivity analysis was performed. When additionally adjusted for hypertension, diabetes, smoking, stroke, and coronary heart disease, the informant confirmation of complaints and subthreshold anxiety symptoms were still significantly associated with amyloid pathology in Analysis 2 (Supplementary Figure 2). Besides, the association between age with amyloid pathology was observed (Supplementary Figure 2).
DISCUSSION
The present study investigated whether SCD characteristics had associations with amyloid pathology in the CABLE study. We found that informant confirmation of complaints, subthreshold depressive and anxiety symptoms were significantly associated with amyloid pathology in univariate and multivariate analyses. Age and female were suggested risks for amyloid pathology in subgroup analyses as well. Our findings help to identify individuals at AD risk among those with SCD.
As an important characteristic of SCD, informant confirmation of complaints can better reflect SCD, compared with subjective cognitive decline. Informant confirmation was suggested as a predictor of lower gray matter volumes in AD-related brain areas of SCD individuals from the ALFA cohort [28]. Studies from Germany and Spain also showed that informant confirmation was related to amyloid pathology [18, 29]. Janssen et al. analyzed the data from 20 cohorts within a research setting, suggesting a significant association between informant confirmation and amyloid positivity in SCD individuals [23]. Similarly, in our CABLE study using a convenient sample, we found that informant confirmation of complaints was significantly related to amyloid pathology. Moreover, we noticed that above relationship only existed in the elderly rather than middle-aged participants, which is consistent with the finding from Cacciamani et al.’s study that informant-reported SCD was an important indicator of preclinical AD among the elderly population aged 70 to 80 [30]. This age difference might be explained by the worse cognitive compensation in the elderly, which makes their cognitive decline easier to be detected by informants. Notably, the informant confirmation was examined by one question rather than a detailed questionnaire, and the number of informants was limited, which need further exploration.
In the current study, we excluded the population with significant depressive and anxiety symptoms to avoid confounding causes of SCD. However, subthreshold depressive and anxiety symptoms in individuals with SCD were still demonstrated to be risk factors for amyloid pathology, suggesting the importance of monitoring the psychological status of SCD individuals even below the threshold. In individuals with SCD, neuropsychiatric symptoms have been demonstrated as important indicators of preclinical AD, and they are associated with incident cognitive decline and AD [19, 21]. Also, Liew et al. found that SCD and anxiety were independently related to the risk of neurocognitive disorders, and both constructs were helpful for identifying individuals at high risk [20]. Moreover, interaction effects of sex on subthreshold depressive and anxiety symptoms were revealed in our study. Stratified analyses suggested that in the population with SCD, these associations of amyloid pathology with subthreshold depressive and anxiety symptoms remained significant only in females, but not in males. And both female and subthreshold psychiatric symptoms were suggested risks for amyloid pathology in middle age. This gender difference can be explained by the fact that females are more susceptible to being influenced sex hormones. The changes of hormones could further affect emotions and even depression and anxiety symptoms of female, which might aggravate AD pathology [31, 32]. More longitudinal studies with large samples are expected in the future.
As major risk factors of AD, age and APOE ɛ4 have been suggested to be associated with amyloid pathology in individuals with SCD [16, 34]. With a larger sample size, Janssen et al. observed the relationships of age and APOE ɛ4 with amyloid positivity as well [23]. Although we observed significant association between age with amyloid pathology in sensitivity analysis, we did not record the association in the analyses of total population. Also, we did not find the association between APOE ɛ4 with amyloid pathology. That might be due to the younger sample and limited number of APOE ɛ4 carriers in our study, as we revealed the interaction between older age with APOE ɛ4. Our subgroup analyses showed older age was associated with amyloid pathology in the subgroup of APOE ɛ4 carriers. Zhang et al.’s study revealed that APOE ɛ4 was a risk factor for amyloid positivity in the elderly with SCD (60 to 90 years) [35]. This might be because that the effect of APOE ɛ4 on the pathology of AD accumulates with age. However, given the limited number of APOE ɛ4 carriers in our study, further discussions are required.
The remaining SCD-specific characteristics in SCD plus list were not significantly associated with amyloid pathology. The DELCODE study with older populations from a memory clinic showed that onset of SCD within 5 years and decline-related worries were associated with amyloid pathology by assessing different cognitive domains [18]. However, it has two limitations. Its sample size was small. And the study included not only individuals with SCD but also healthy controls and first-degree relatives of AD patients (AD relatives). Also, another study from a memory clinic, the SCIENCe study, showed that onset age ≥60 and decline-related worries rather than other SCD features in the list were associated with preclinical AD [17, 34]. What’s more, Janssen et al. revealed that the relationship between the feeling of worse performance with amyloid pathology was only significant in older participants [23]. Our study was based on a convenient sample from hospitals rather than memory clinics. The population was relatively young, which might explain the negative associations between SCD-plus characteristics (except informant confirmation) and amyloid pathology. Considering the complexity of participant population and SCD assessments, more detailed studies are needed in the future.
We explored the associations of SCD characteristics with amyloid pathology in a large SCD population from the CABLE study. Nonetheless, some limitations should be noted. Firstly, the study was conducted in China, which should be cautious for generalizing the results. Besides, SCD is a clinical concept with heterogeneity, and we used only the MMSE to detect objective cognitive impairment, which could not exclude participants with MCI. The frequency of amyloid positivity varies widely, and the actual cut-off value of amyloid pathology in our cohort needs to be confirmed by subsequent outcomes. In addition, since this was a cross-sectional study, the results require longitudinal follow-up validation in the future.
In conclusion, the characteristics of informant confirmed complaints, subthreshold depressive and anxiety symptoms may be helpful for targeting population with amyloid pathology in individuals with diagnosis of SCD, who are supposed to benefit from further follow-up and intervention against AD. Still, more well-designed studies are warranted in the future.
Footnotes
ACKNOWLEDGMENTS
The authors thank all participants of the present study as well as all members of the CABLE study for their efforts in data collection.
FUNDING
This study was supported by grants from the Science and Technology Innovation 2030 Major Projects (2022ZD0211600), the National Natural Science Foundation of China (82071201, 91849126), the National Key R&D Program of China (2018YFC1314702), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01) and Zhangjiang Lab, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University.
CONFLICT OF INTEREST
Jin-Tai Yu and Lan Tan are Editorial Board Members of this journal but were not involved in the peer-review process nor had access to any information regarding its peer-review. The authors have no conflict of interest to report.
DATA AVAILABILITY
In the current study, the datasets used and analyzed are available from the corresponding author on reasonable request.