
Abstract
Background:
Microvascular dysfunction (MVD) may contribute to cognitive impairment and Alzheimer’s disease, but evidence is limited.
Objective:
To investigate the association of composite and organ-specific MVD burden with mild cognitive impairment (MCI) and cognition among rural-dwelling Chinese older adults.
Methods:
In this population-based cross-sectional study, we assessed MVD makers using optical coherence tomographic angiography for retinal microvasculature features, brain magnetic resonance imaging scans for cerebral small vessel disease (CSVD), and serum biomarkers for MVD. A composite MVD score was generated from the aforementioned organ-specific parameters. We used a neuropsychological test battery to assess memory, verbal fluency, attention, executive function, and global cognitive function. MCI, amnestic MCI (aMCI), and non-amnestic MCI (naMCI) were diagnosed following the Petersen’s criteria. Data was analyzed with the linear and logistic regression models.
Results:
Of the 274 dementia-free participants (age≥65 years), 56 were diagnosed with MCI, including 47 with aMCI and 9 with naMCI. A composite MVD score was statistically significantly associated with an odds ratio (OR) of 2.70 (95% confidence interval 1.12–6.53) for MCI and β-coefficient of –0.29 (–0.48, –0.10) for global cognitive score after adjustment for socio-demographics, lifestyle factors, APOE genotype, the Geriatric Depression Scale score, serum inflammatory biomarkers, and cardiovascular comorbidity. A composite score of retinal microvascular morphology was associated with a multivariable-adjusted OR of 1.72 (1.09–2.73) for MCI and multivariable-adjusted β-coefficient of –0.11 (–0.22, –0.01) for global cognitive score. A composite CSVD score was associated with a lower global cognitive score (β= –0.10; –0.17, –0.02).
Conclusion:
Microvascular dysfunction, especially in the brain and retina, is associated with MCI and poor cognitive function among rural-dwelling older adults.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI), as a boundary stage between normal cognitive aging and dementia, affects over one-fourth of rural-dwelling older adults in China [1]. The prevalence of MCI increases with the aging of the population, which has posed huge economic and societal burdens [2]. However, the mechanisms underlying occurrence of MCI and cognitive impairment remain poorly understood. The microvasculature is involved in many aspects of brain regulation, such as blood– brain barrier permeability, hypoperfusion, and neurovascular unit injury [3]. Evidence has accumulated in recent years that microvascular dysfunction (MVD) might be involved in the development and progression of cognitive deterioration in the elderly [3–5].
Microvascular function in various organs can be assessed using noninvasive approaches [6, 7]. For instance, markers of cerebral small vessel disease (CSVD) assessed by magnetic resonance imaging (MRI) can reflect cerebral microvascular alterations [8]. Optical coherence tomography angiography (OCTA) can provide measurements of various retinal microvascular metrics, such as retinal vascular density indices (e.g., foveal avascular zone [FAZ] area, vessel area density [VAD], and vessel skeleton density [VSD]) and retinal vascular morphology indices (e.g., fractal dimension [FD] and vessel diameter index [VDI]) [9–11]. Besides, serum soluble intercellular adhesion molecule-1 (sICAM-1) and soluble vascular adhesion molecule-1 (sVCAM-1) are well-known biomarkers for systemic microvascular injury [6]. In the past decades, the relationship of microvascular function with cognition has generated a great deal of interest. Previous studies have linked individual MVD indicators, such as CSVD, retinal microvascular parameters, and serum MVD biomarkers (e.g., sICAM-1, sVCAM-1, and E-Selectin) with poor cognition [12–14]. The composite measure of microvascular dysfunction summarized from multiple organs might better capture systemic microvascular impairment than that of using information from a single organ. The Cardiovascular Health Study has found that a greater microvascular lesion burden summarized from microvascular measures of the brain, retina, and kidney was associated with poor performance in psychomotor speed and working memory [5]. In addition, the Maastricht Study has shown that a higher composite MVD score generated from microvascular measures of the brain, retina, kidney, skin, and plasma biomarkers is associated with worse memory and processing speed in middle-aged and early older adults (40–75 years of age) who are free of dementia [6]. However, the relationship of MVD with cognitive function has not yet been investigated in rural Chinese older adults. This is important because studying association of MVD and cognitive function in an ethnically, culturally, and socioeconomically different elderly population may contribute to the generalizability of the findings. In addition, population-based studies have rarely investigated the relationships of the composite and organ-specific MVD burden with MCI and its subtypes in older adults.
Thus, in this population-based study, we sought to investigate whether the composite and organ-specific MVD burden is associated with MCI, main subtypes of MCI, and function of various cognitive domains among rural-dwelling older adults in China.
Study participants
This population-based cross-sectional study used data from the Multimodal Interventions to delay Dementia and disability in rural China (MIND-China) study, which is part of the World-Wide FINGERS Network [15]. In brief, the baseline assessments of MIND-China targeted people who were aged≥60 years by the end of 2017 and living in the 52 villages of Yanlou Town, Yanggu County, western Shandong Province, China. In March-September 2018, 5,765 participants (57.19% women) were examined for the MIND-China, as previously described [16].
From June 2019 to November 2020, 284 participants accomplished both the structural brain MRI scan and the OCTA examination in Southwest Lu Hospital, Shandong province. The cluster (village)-randomized sampling approach was used in the selection of participants for the brain MRI and OCTA substudies within the MIND-China, as previously described [16]. Of the 284 participants, 10 were excluded due to missing data on cognitive function (n = 7), the 15-item Geriatric Depression Scale (GDS-15) (n = 1), apolipoprotein E (APOE) genotype (n = 1), and serum inflammatory biomarkers (n = 1), leaving 274 persons for the current analysis. Of these, data were available in 273 participants for serum biomarkers of MVD, in 259 participants for brain MRI data, and in 248 participants for retinal microvascular features (26 participants were excluded due to poor quality of OCTA images). Finally, data on composite MVD indicator were available in 233 participants who had complete data on all cognitive tests, individual MVD measures, and potential confounders. Figure 1 shows the flowchart of the study participants.
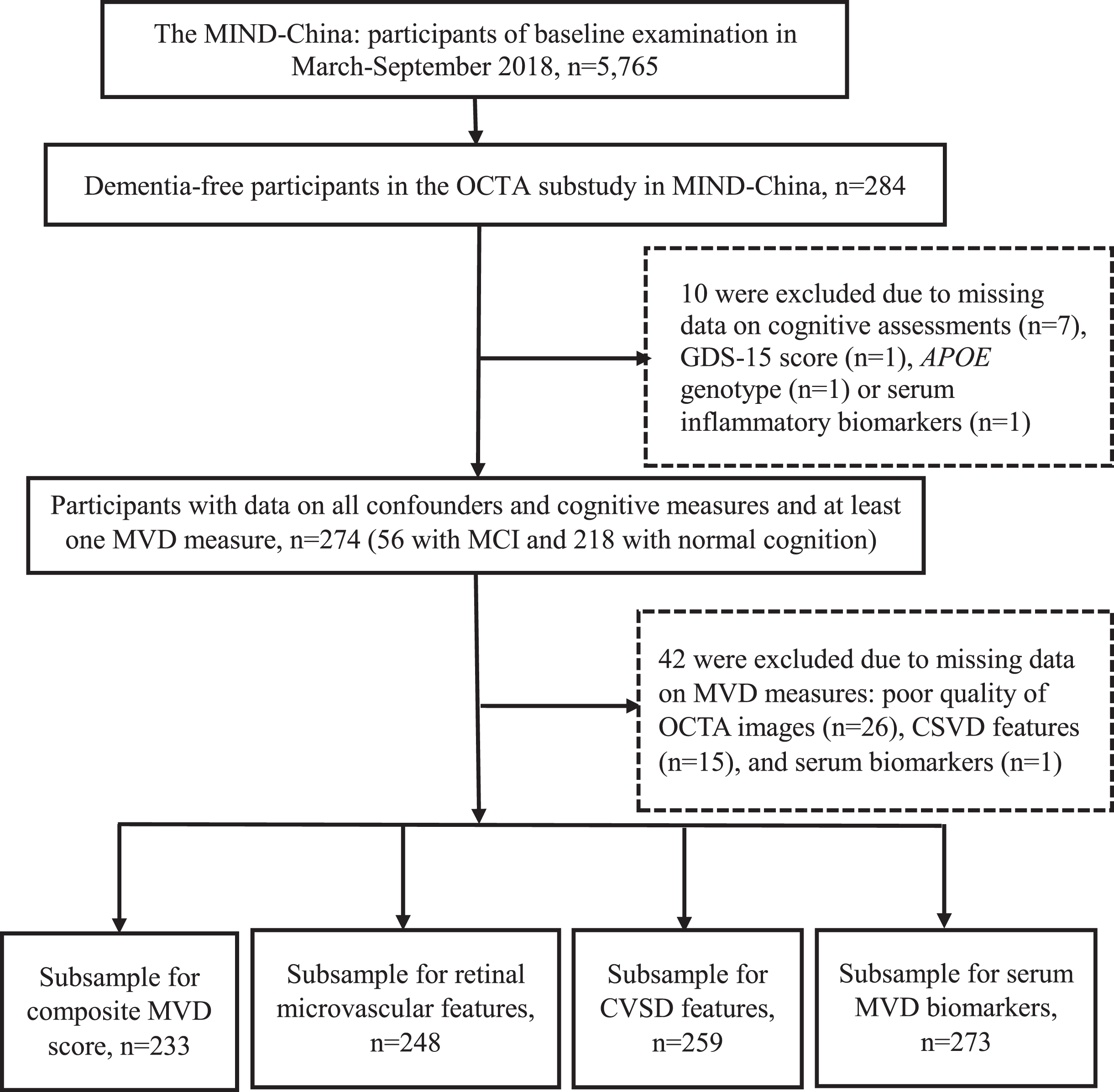
Flowchart of the study participants. APOE, apolipoprotein E; CSVD, cerebral small vascular disease; GDS-15, the 15-item Geriatric Depression Scale; MIND-China, the Multimodal Interventions to delay Dementia and disability in rural China; MCI, mild cognitive impairment; MVD, microvascular dysfunction; OCTA, optical coherence tomographic angiography.
The MIND-China protocol was reviewed and approved by the ethics committee at Shandong Provincial Hospital in Jinan, Shandong, China. Written informed consent was collected from all participants or proxies. This study was carried out in accordance with the ethical principles expressed in the Declaration of Helsinki. The protocol of MIND-China was registered in the Chinese Clinical Trial Registry (ChiCTR, https://www.chictr.org.cn; registration no.: ChiCTR1800017758).
Data collection
Trained medical staff collected data on potential confounding factors through face-to-face interviews, clinical examinations, neuropsychological testing, and laboratory tests, as previously reported [16]. These factors included demographics (e.g., age, sex, and education), lifestyles (e.g., smoking, alcohol consumption, and body mass index [BMI]), medical history (e.g., hypertension, diabetes, dyslipidemia, coronary heart disease, and stroke), and APOE genotype. The GDS-15 score was used to assess the presence of depressive symptoms [17]. Serum inflammatory biomarkers, including interleukin-6, interleukin-8, and tumor necrosis factor-α, were determined as described previously [16]. Cardiovascular multimorbidity was defined as concurrently having two or more of the five chronic cardiovascular health conditions, i.e., hypertension, diabetes, dyslipidemia, coronary heart disease, and stroke [18].
Assessment of retinal microvascular features
Macular OCTA images of 6 mm×6 mm areas centered at the fovea were acquired with the commercially Spectralis HRA+OCT (Software Version 1.10.2.0; Heidelberg Engineering, Inc., Heidelberg, Germany) prototype. The OCTA algorithm and image processing technique have been described in previous studies [19, 20]. In brief, OCTA images underwent quality control procedure to exclude poor images with artifacts, severe motion, or retinopathy [21]. Then, a custom semi-automated algorithm was developed using MATLAB (R2019b, Math Works, Inc.) to process raw angiography images and to extract and calculate retinal microvascular parameters, including FAZ area, VAD, VSD, FD, and VDI [10, 11]. Briefly, VAD and VSD were calculated as the retinal area density and skeleton density of superficial networks except the FAZ area. FD represents the complexity of capillary network. Thus, smaller VAD, VSD, and FD represent more severe microvascular impairment. FAZ area, which is defined as the area of avascularity, is particularly vulnerable to microvascular injury. VDI, which is the average of vascular caliber diameter, reflects vascular dilation. Therefore, higher FAZ area and VDI represent loss of capillaries [9, 20]. A detailed description of the OCTA protocol and the definitions of the microvascular parameters is provided in Supplementary Material 1. The current study used blood flow data from the retinal superficial vascular plexus. The OCTA images of the right eye were analyzed in most cases, and images of the left eye were used in case the right eye images were not available or of suboptimal quality.
Assessment of cerebral microvascular features
The structural brain MRI scans were performed from June 2019 to November 2020 in the Southwest Lu Hospital (Philips Ingenia 3.0T, The Netherlands). The core protocol of structural brain MRI scans mainly included the three-dimensional T1-weighted, T2-weighted, and fluid-attenuated inversion recovery sequences [16]. We evaluated four CSVD markers, i.e., total brain parenchymal volume, white matter hyperintensity (WMH) volume, the number of lacunes, and the number of enlarge perivascular spaces (EPVS) [22]. Total brain parenchymal volume and WMH volume were determined semi-automatically, as previously described [23, 24]. EPVS and lacunes were assessed and counted manually by two trained raters (M.Z. and J.W.) who were blinded to the participants’ clinical information under the supervision of an experienced clinical neurologist (L.S.) [25, 26]. In this study, we only counted EPVS in the basal ganglia because EPVS in this region were specifically associated with CSVD [26]. We used the following scale to grade EPVS in the basal ganglia [26]: 0 = no EPVS, 1 = 1–10 EPVS, 2 = 11–20 EPVS, 3 = 21–40 EPVS, and 4 =≥40 EPVS. A detailed description of the MRI parameters and the definitions of the CSVD features is provided in Supplementary Material 2.
Assessment of serum biomarkers for MVD
After an overnight fast, peripheral blood samples were drawn into a tube with 2 ml ethylenediaminetetraacetic acid, and serum samples were stored at –80°C for future analysis, as described previously [16]. Two serum biomarkers for MVD, sICAM-1 and sVCAM-1, were measured using commercial kits (Meso Scale Discovery [MSD] V-PLEX Assays). For biomarker assays, the intra- and inter-assay coefficients of variation were less than 15%.
Assessments of cognitive function and diagnosis of MCI, aMCI, and naMCI
Cognitive function was assessed using a neuropsychological test battery, as previously described [1, 16]. Specifically, subjective cognitive decline was assessed using three questions of memory problems the participants experienced in the past year, i.e., difficulty remembering (do you feel that in the past year you had difficulties in remembering things?), forgetting what had been planned (do you feel that in the past year it was easier than before to forget things?), and worry about memory decline (do you worry about your memory that has been getting worse in the past year?). The Clinical Dementia Rating scale was used to assess participants’ cognitive changes. The Chinese version of Activities of Daily Living Scale to evaluate self-care and instrumental activities of daily living. For function of specific cognitive domains, we assessed memory function using the Auditory Verbal Learning Test-immediate recall, long-delayed free recall, and long-delayed recognition. Verbal fluency was assessed using the Verbal Fluency Test-categories of animals, fruits, and vegetables. Attention was assessed using the Digit Span Test-forward and Trail Making Test A. Executive function was assessed using the Digit Span Test-backward and Trail Making Test B. The raw score of each test was standardized into z-score using the age- and education-specific means and standard deviations, derived from all dementia-free participants in MIND-China. Because all cognitive domains were assessed using more than one test, we created the composite z-score for each of the cognitive domains by averaging the z-scores of the tests for that domain. The composite z-score for global cognition was estimated by averaging the composite z-scores of the four cognitive domains. Objective cognitive impairment was defined as scoring≥1.0 SD below the age- and education-specific mean among dementia-free participants in MIND-China in any of the four cognitive domains.
Diagnosis of MCI, amnestic MCI (aMCI), and non-amnestic MCI (naMCI) in MIND-China has been described previously [1]. In brief, MCI and its subtypes were diagnosed by senior neurologists via neuropsychological and clinical assessments according to the Petersen’s criteria that were operationalized as in the Mayo Clinic Study of Aging [27]: 1) subjective cognitive concern by the subject (responded “Yes” to any of the three questions of memory problems above), informant or physician (Clinical Dementia Rating≥0.5); 2) objective cognitive impairment evidenced in at least one of the four cognitive domains (from cognitive test battery); 3) essentially preserved function of daily activities (from the Activities of Daily Living); and 4) absence of dementia diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria. MCI was then categorized into aMCI if the memory domain was impaired or naMCI if there was no impairment in memory.
Statistical analysis
We presented mean (standard deviation, SD) or median (interquartile range, IQR) for continuous variables and frequencies (%) for categorical variables. Characteristics of the study participants by MCI were compared using Mann-Whitney U test for skew distributed continuous variables, the t test for normal distributed continuous variables, and Chi-square test for categorical variables.
For the calculation of composite score for MVD, we inversed VAD, VSD, FD, and total brain parenchymal volume (i.e., multiplying it by –1) to reflect MVD [4, 22]. WMH volume, EPVS count, and number of lacunes were log-transformed to reduce skewed distribution. We standardized all 11 individual MVD measures (e.g., 5 retinal microvascular markers, 4 CSVD imaging markers, and 2 serum biomarkers) into z-scores. Then, we averaged these z-scores into the composite MVD score. The composite MVD score was calculated only among participants with data available for all individual MVD measures. Similarly, we calculated the organ-specific composite MVD scores for the retinal microvascular features, and serum MVD biomarkers separately, by averaging the z-scores of MVD measures for that organ [28]. The composite CSVD score was calculated from multiple MRI markers following the methods as previously described [22, 29]. One point for each of the following four CSVD markers was assigned: the first quartile of total brain parenchymal volume, the fourth quartile of WMH volume, the presence of lacunes, and the EPVS grading score≥2 (i.e., EPVS number≥11) in the basal ganglia of one hemisphere. The total composite CSVD score ranges 0–4. In addition, we analyzed retinal microvascular density features (i.e., retinal microvascular density) = (z-score FAZ area + z-score VAD + z-score VSD)/3 and retinal microvascular morphology features (i.e., retinal microvascular morphology) = (z-score FD + z-score VDI)/2, respectively [10, 11].
Linear regression models were used to estimate the β coefficient and 95% confidence interval (CI) of cognitive z-score associated with MVD measures. Binary and multinomial logistic regression models were used to investigate the odds ratio and 95% CI of MCI and the main subtypes of MCI associated with MVD measures. We reported the main results from two models: Model 1 was adjusted for age, sex, and education; and Model 2 was further adjusted for smoking, alcohol consumption, BMI, APOE genotype, GDS-15 score, serum inflammatory biomarkers, and cardiovascular multimorbidity [14, 30]. In addition, we also examined the associations of individual MVD measure with cognitive function, MCI, aMCI, and naMCI. Because microvascular function deteriorates with age and is accelerated by vascular risk factors [3, 31], we further examined the statistical interaction of the composite MVD score with age, sex, education, APOE genotype, and cardiovascular multimorbidity on global cognitive z-score.
IBM SPSS Statistics for Windows, Version 26.0. (Armonk, NY: IBM Corp) was used for all the analysis. A two-tailed p < 0.05 was considered to be statistically significant.
RESULTS
Characteristics of study participants
The mean age of the 274 participants was 68.3 (SD = 4.0) years, 57.7% were female, 34.3% had no school education, and 56 (20.4%) were diagnosed with MCI, including 47 (17.2%) with aMCI and 9 (3.3%) with naMCI. Compared with cognitively normal participants, those with MCI were older, more likely to be female, and less likely to drink alcohol, and had a higher composite score of MVD, retinal microvascular morphology, and serum MVD biomarkers, as well as higher VAD, FAZ area, VDI, sICAM-1, and sVCAM-1, and lower total brain parenchymal volume (p < 0.05) (Table 1). The two groups showed no statistically significant differences in the distributions of the other examined factors in Table 1 (p > 0.05).
Characteristics of study participants by mild cognitive impairment
APOE, apolipoprotein E gene; BMI, body mass index; CSVD, cerebral small vascular disease; EPVS, enlarge perivascular spaces; FD, fractal dimension; FAZ, foveal avascular zone; IQR, interquartile range; GDS-15, 15-item Geriatric Depressive Scale; MVD, microvascular dysfunction; SD, standard deviation; sICAM-1, serum soluble intercellular adhesion molecule-1; sVCAM-1, soluble vascular adhesion molecule-1; VAD, vessel area density; VSD, vessel skeleton density; VDI, vessel diameter index; WMH, white matter hyperintensity. aData were mean (standard deviation), unless otherwise specified. bOf the 274 participants, data were available in 273 individuals for serum MVD biomarkers; in 259 individuals for MRI markers of CSVD; in 248 individuals for OCTA markers of retinal microvascular; and in 233 individuals for the composite MVD measures from all organs.
Associations of MVD with MCI, aMCI, and naMCI
A higher composite MVD score was statistically significantly associated with a higher likelihood of MCI and aMCI in both the demographic-adjusted and fully-adjusted models (Table 2). A higher composite score of retinal microvascular features was statistically significantly associated with a higher likelihood of MCI after adjusting for age, sex, and education, but the association became statistically non-significant in the fully-adjusted model. A higher composite score of retinal microvascular features was statistically significantly associated with naMCI, particularly in the fully-adjusted model. A higher composite score of retinal microvascular morphology features was statistically significantly associated with a higher likelihood of MCI, aMCI, and naMCI after adjusting for age, sex, and education, and the association with MCI and naMCI remained statistically significant after further adjusting for additional potential confounding factors. There was no statistical association of composite scores of retinal microvascular density, CSVD features, and serum MVD biomarkers with MCI and its subtypes (Table 2).
Association of composite measures of microvascular dysfunction with mild cognitive impairment and its subtypes
CI, confidence interval; CSVD, cerebral small vascular disease; MVD, microvascular dysfunction; SD, standard deviation. aThe odds ratio (95% confidence interval) of mild cognitive impairment or its subtypes was estimated in association with per 1-SD or per 1-point increase (CSVD score) in microvascular dysfunction score. bModel 1 was adjusted for age, sex, and education; and Model 2 was further adjusted for APOE genotype, smoking, body mass index, alcohol consumption, 15-item Geriatric Depressive Scale, serum inflammatory biomarkers, and cardiovascular multimorbidity. When we analyzed associations of microvascular dysfunction with amnestic mild cognitive impairment and non-amnestic mild cognitive impairment, we used multinomial logistic regression models, in which smoking was not included in model 2 due to lack of cases with non-amnestic mild cognitive impairment in the smoking group. *p < 0.05, †p < 0.01, ‡p < 0.001.
We also examined the associations of individual MVD measure with MCI, aMCI, and naMCI. Higher z-scores of FAZ area, VSD, and VDI, and EPVS grade score were statistically significantly associated with a higher likelihood of MCI and its subtypes in both the demographic- and fully-adjusted models (p < 0.05) (Supplementary Table 1). We found no statistically significant associations of z-scores of sICAM-1, sVCAM-1, VAD, FD, total brain parenchymal volume, and WMH volume, and the presence of lacunes with MCI and its subtypes (p > 0.05) (Supplementary Table 1).
Association of MVD with cognitive function
Higher composite scores of MVD, retinal microvascular morphology, and CSVD features were statistically significantly associated with a lower global cognitive z-score in both the demographic- and fully-adjusted models (p < 0.05) (Fig. 2).
For the cognitive subdomains, a higher composite MVD score was associated with lower z-scores of memory, verbal fluency, and executive function in both the demographic- and fully-adjusted models (p < 0.05) (Fig. 2). Higher composite scores of retinal microvascular features, retinal microvascular morphology, and CSVD features were statistically significantly associated with lower z-score of memory after adjusting for age, sex, and education. Higher composite scores of retinal microvascular morphology and CSVD features were associated with lower verbal fluency z-score in both the demographic- and fully-adjusted models. A higher composite score of CSVD features was also statistically significantly associated with a lower z-score of executive function in both models. A higher composite score of serum MVD biomarkers was associated with a lower z-score of verbal fluency in the fully-adjusted models. No statistically significant association was found between the composite score of retinal microvascular density with z-scores of global cognition and various cognitive domains (Fig. 2).
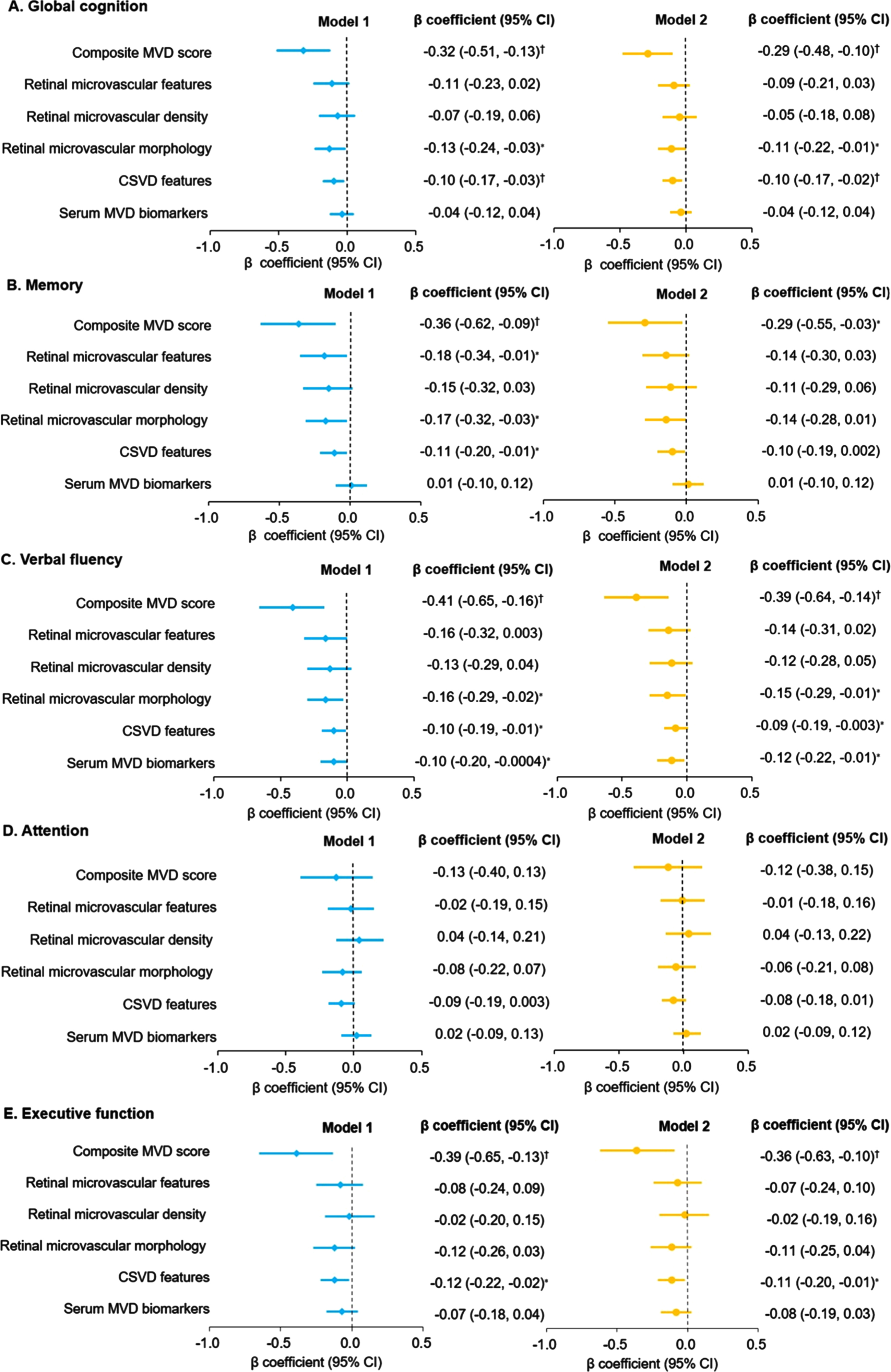
Associations of microvascular dysfunction parameters with cognitive function (N = 274a). A) Global cognition. B) Memory. C) Verbal fluency. D) Attention. E) Executive function. aOf the 274 participants, data were available in 273 individuals for serum MVD biomarkers; in 259 individuals for MRI markers of CSVD; in 248 individuals for OCTA markers of retinal microvascular; and in 233 individuals for the composite MVD measures from all organs. CI, confidence interval; CSVD, cerebral small vascular disease; MVD, microvascular dysfunction. The β coefficient (95% CI) of cognitive z-score was estimated in association with per 1-SD or per 1-point (CSVD score) increase in microvascular dysfunction score. Model 1 was adjusted for age, sex, and education; and Model 2 was further adjusted for APOE genotype, smoking, body mass index, alcohol consumption, 15-item Geriatric Depressive Scale score, serum inflammatory biomarkers, and cardiovascular multimorbidity. *p < 0.05, †p < 0.01, ‡p < 0.001.
In addition, we also examined the associations of individual MVD measure with cognitive function. Higher z-scores of sICAM-1, sVCAM-1, FAZ area, VAD, VDI, total brain parenchymal volume, and WMH volume, and the presence of lacunes, but not VSD, FD, and EPVS, were statistically significantly associated with lower z-scores of global cognitive function and cognitive subdomains (Supplementary Table 2).
We detected no statistical interaction of the composite MVD score with age, sex, education, APOE genotype, serum inflammatory biomarkers, and cardiovascular multimorbidity on global cognitive function (p for interaction > 0.05) (data not shown).
DISCUSSION
In this population-based cross-sectional study of rural-dwelling dementia-free Chinese older adults, we found that a greater MVD load was associated with an increased likelihood of MCI, aMCI, and poor function in multiple cognitive domains. Specifically, a greater burden of retinal microvascular lesion markers, especially retinal microvascular morphology features, was associated with a higher likelihood of MCI, aMCI, and naMCI as well as poor performance in global cognition, memory, and verbal fluency function. The increased load of CSVD was associated with poor global cognitive function, memory, verbal fluency, and executive function. The increased load of serum MVD biomarkers was associated with poor verbal fluency function.
The associations of MVD burden with MCI and its main subtypes have not yet been reported in the literature of population-based studies. In our population-based study of rural older adults, we generated a composite MVD measure that integrated MVD features of retinal microvascular lesions, CSVD, and serum biomarkers. We found that a heavier load of MVD, especially the burden of retinal microvascular morphology features, was associated with a higher likelihood of MCI and aMCI. However, the Eye Determinants of Cognition substudy (n = 480) within the Atherosclerosis Risk in Communities of middle-aged biracial cohorts found no associations of retinal microvascular parameters (e.g., retinal vascular density and FAZ area) with MCI [32]. Differences in characteristics of the study sample (e.g., age, sex, and race) and fundus imaging techniques might partly contribute to the discrepant findings across studies. Compared to the traditional fundus photography [33, 34], OCTA can quantitatively detect the movement of red blood cells at capillary-level resolution and offer quantitative index for retinal microvascular signs [35]. Several OCTA-based case-control studies showed retinal microvascular loss in patients with MCI or aMCI [36, 37], which was in agreement with our results. The finding of association of MVD burden with aMCI supports the potential involvement of MVD in the pathophysiology of Alzheimer’s disease because aMCI, as the most common subtype of MCI in our sample, involves impairment in episodic memory that is more likely to progress to typical Alzheimer’s disease [1]. We further revealed that a greater burden of retinal microvascular morphology features was associated with a higher likelihood of naMCI. Non-amnestic MCI has more vascular components than aMCI [38] and might represent prodromal stage of dementia subtypes such as vascular dementia, Lewy body dementia, and Parkinson’s disease dementia [1, 39]. Retinal morphological parameters assessed with OCTA, which reflected the overall complexity and ischemia of the retinal vasculature at the micrometer level [35], were associated with cognitive impairment [20, 40]. Taken together, our study supports the hypothesis that MVD may be involved in the development of MCI. MVD, especially retinal microvascular morphology features detected with OCTA, could be valuable retinal markers for MCI in older adults. However, future prospective cohort study is needed to further clarify the potential causal relationship of MVD with MCI inolder adults.
Population-based studies have rarely examined the associations of MVD burden with global and domain-specific cognitive function among older adults. Our study showed that a higher load of MVD was associated with poor cognitive performances independent of sociodemographic, behavioral, clinical, and genetic factors. This was in line with reports from the US Cardiovascular Health Study and the Maastricht Study in the Netherlands, which showed the correlation of the higher MVD load with lower cognitive function in older adults [4, 5]. Furthermore, we also found that features of retinal microvascular morphology and CSVD were associated with poor function in multiple cognitive domains (e.g., memory, verbal fluency, and executive function). This was consistent with two population-based studies from UK and Italy, which suggested correlations of heavy CSVD burden and retinal vascular network loss with poor cognitive function [41, 42]. However, the Maastricht study found that the higher composite scores of CSVD features and plasma MVD biomarkers, but not of retinal arteriolar and venular dilation responses, were associated with worse cognitive function. This indicates that retinal arteriolar and venular dilation responses may mostly reflect a more subtle form of endothelial dysfunction [4]. It is well known that microvasculature in the retina and brain is anatomically and physiologically homologous [43, 44], and neuropathological studies have demonstrated amyloid-β deposition in cerebral and retinal capillaries [45, 46]. MVD of the brain and retina may lead to neuronal ischemia, dysfunction, and cell death, which contributes to cognitive impairment [3, 48]. Circulating MVD biomarkers indicate systemic microvascular injury. Previous studies have yielded mixed results regarding the relationship between circulating MVD biomarkers and cognitive function. For instance, the Hoorn Study found that higher serum sICAM-1 and sVCAM-1 were associated with worse cognitive performances on information-processing speed, attention, and executive function [14]. By contrast, the Australian Imaging Biomarkers and Lifestyle Active study and the Epidemiology of Hearing Loss Study found no associations of plasma sVCAM-1 and sICAM-1 with cognitive function after controlling for demographics and depressive symptoms [49, 50]. Our study showed that a high burden of serum MVD biomarkers was only associated with poor verbal fluency. In support of our finding, a previous case-control study showed that higher levels of serum sVCAM-1 and sICAM-1 were associated with altered cortical vasoreactivity and atrophy in multiple brain regions associated with language function (e.g., temporal and parietal) [51]. Taken together, these results suggest that the burden of MVD could be valuable markers for MCI and cognitive impairment in older adults.
The mechanisms underlying the association of MVD with cognitive impairment in older adults are not fully understood and can only be speculated. Previous studies have linked Alzheimer’s disease and cognitive impairment with blood-brain barrier leakage, impaired neurovascular unit, and decreased capillary density, which may be the consequences of MVD [3, 52]. Both MVD and cognitive decline are accelerated by vascular risk factors [3, 54]. However, we detected no statistical interaction of MVD measures with cardiovascular multimorbidity (i.e., hypertension, diabetes, dyslipidemia, coronary heart disease, and stroke) on global cognitive function. Other biological mechanisms (e.g., oxidative stress and dysfunction of coagulation pathway) may underlie both MVD and poor cognitive function [55]. However, we were not able to explore this pathway because data on biomarkers of oxidative stress and coagulation were not available in our study. Further studies are needed to clarify the mechanisms underlying the association of MVD load with cognitive impairment in old age.
The major strengths of our study refer to the population-based design that targeted rural-dwelling older adults, and MVD markers in multiple organs that were assessed using the state-of-the-art techniques (e.g., 3T MRI scans and non-invasive OCTA), which can provide high-quality images of cerebral microvascular lesions and retinal microvascular network from multiple metrics. However, our study also has limitations. First, this cross-sectional study cannot provide evidence for any causal relationships. Second, we had a relatively small sample size and the participants were relatively younger and more educated compared to the MIND-China total sample (mean age, 68.3 versus 70.9 years, p < 0.05; primary school or above, 65.7% versus 59.4%, p < 0.05). Third, we did not have proper MVD markers from relevant organs such the heart and kidney, which might underestimate the association of MVD load with cognitive outcomes in older adults [31, 56].
Conclusion
In summary, our population-based study shows that a greater MVD load, especially in the brain and retina, is related to poor cognitive performance and an increased likelihood of MCI and aMCI in older adults. Our results support the hypothesis that MVD might be involved in the pathophysiology of cognitive impairment and Alzheimer’s disease. Noninvasive measurements of microvascular abnormalities may be useful clinical markers for cognitive dysfunction. Future prospective cohort studies are warranted to further evaluate their potential causal relationship and the underlying biological mechanisms linking MVD with cognitive phenotypes in the elderly. This will further facilitate the development of potential preventive and therapeutic interventions to delay cognitive impairment and its progression to dementia and Alzheimer’s disease by targeting microvascular pathways.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all the participants of the MIND-China Project and the staff of the Yanlou Town Hospital as well as Shandong Provincial Hospital who were involved in the data collection and management.
FUNDING
MIND-China was financially supported in part by grants from the National Natural Science Foundation of China (grants no.: 82171175, 81861138008, and 81772448), the Alzheimer’s Association Grant (grant no.: AACSFD-22-922844), the National Key R&D Program of China Ministry of Sciences and Technology (grant no.: 2017YFC1310100), the Natural Science Foundation of Shandong Province (grant no.: ZR2021MH005), the Academic Promotion Program of Shandong First Medical University (2019QL020), the Integrated Traditional Chinese and Western Medicine Program in Shandong Province (YXH2019ZXY008), and the Brain Science and Brain-like Intelligence Technology Research Projects of China (2021ZD0201801 and 2021ZD0201808). L Cong received grants from the Shandong Provincial Key Research and Development Program (grant no.: 2021LCZX03). C Qiu received grants from the Swedish Research Council (grants no.: 2017-05819 and 2020-01574), the Swedish Foundation for International Cooperation in Research and Higher Education (grant no.: CH2019-8320), and Karolinska Institutet, Stockholm, Sweden. The funding agency had no role in the study design, data collection and analysis, the writing of this manuscript, and in the decision to submit the work for publication.
CONFLICT OF INTEREST
Yongxiang Wang and Yifeng Du are Editorial Board Members of the Journal of Alzheimer’s Disease but they were not involved in the peer-review process nor had they access to any information regarding its peer-review. All other authors have no conflict of interest to report.
DATA AVAILABILITY
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request and approval by the Steering Committee of MIND-China at the Department of Neurology, Shandong Provincial Hospital.