
Abstract
Background:
Depression and dementia confer substantial global health burdens, particularly in women. Understanding the association between depression and dementia may inform new targets for prevention and/or early intervention.
Objective:
To investigate the association between depression in mid- and later-life and dementia (all-cause, Alzheimer’s disease (AD) or vascular dementia (VaD)) in women.
Methods:
A prospective study design. Nurses were followed from age 60 years or entry into the cohort, whichever came last, until date of dementia, death, emigration, or end of follow-up, whichever came first. Cox regression models with age as the underlying timeline were used to estimate the associations between time-varying depression and incident dementia.
Results:
The study included 25,651 female Danish nurses (≥45 years) participating in the Danish Nurse Cohort. During an average of 23 years of follow-up, 1,232 (4.8%) nurses developed dementia and 8,086 (31.5%) were identified with at least two episodes of treated depression. In adjusted analyses, nurses with depression were at a statistically significant 5.23-fold higher risk of all-cause dementia (aHR 5.23:95% CI, 4.64–5.91) compared to those with no history of depression. The differential effects of depression were greater for VaD (aHR 7.96:95% CI, 5.26–12.0) than AD (aHR 4.64:95% CI, 3.97–5.42). Later life depression (>60 years) (aHR 5.85:95% CI, 5.17–6.64) and recurrent depression (aHR 3.51:95% CI, 2.67–4.61) elevated dementia risk. Severe depression tripled the risk of all cause dementia (aHR 3.14:95% CI, 2.62–3.76).
Conclusion:
Both later life and severe depression substantially increase dementia risk in women, particularly VaD.
INTRODUCTION
Dementia causes a progressive deterioration in cognitive functioning leading to dependency, disability, and death. The World Health Organization estimates that over 55 million people suffer from dementia worldwide, which is moreover expected to triple by 2050 [1]. Women are disproportionally affected with a 55% higher risk from age 65 years onward compared to men, which is not fully explained by greater female longevity [2, 3]. Estrogen has been consistently identified as one potential mechanism underlying higher rates of dementia in women, and the neuroprotective mechanisms of estrogens have been demonstrated in both preclinical and clinical studies suggesting that estrogens demonstrate neuroprotective actions [4, 5]. In an aging population, prevalence and costs will escalate, unless a prevention or cure for dementia can be identified. Depression is the second leading cause of disability, affecting >300 million people worldwide (∼4%) [6]. Like dementia, depression affects more women than men [7–10] and these sex differences are apparent from puberty onwards. Similar to dementia, depression in women has been associated with times of fluctuation in sex steroid hormone concentration, such as pregnancy and menopause, suggesting that sex steroids may also contribute to vulnerability to depression in women [11].
An association between depression and dementia is suggested in at least four separate studies and independent systematic reviews with and without meta-analysis. Together, these suggest that depression is associated with a doubling in dementia risk [12–17]. However, most studies are limited by short follow-up, small sample size and uncertain ascertainment of dementia. In particular, it remains uncertain whether depression is an etiologic risk factor, a prodrome or shares genetic or other neuropathologic features with dementia [14].
Both depression and dementia have previously been associated with many of the same underlying conditions including cardiovascular disease (CVD) [18, 19], high body mass index (BMI) [20] and menopausal hormone therapy (HT) use [21–23]. However, few published studies have investigated the effect of these variables on the association between depression and dementia.
The aims of this study were to measure the prospective association between depression and dementia and determine whether this association differed by timing of depression (mid- or later-life or both) and type of dementia (all-cause, Alzheimer’s disease (AD) or vascular dementia (VaD)). Also, whether these associations were conditional on CVD, BMI, HT use or physical activity.
METHODS
Study design and data sources
A prospective cohort study within the Danish Nurse Cohort (DNC). The cohort was established in 1993 and has previously been described in detail [24]. In brief, the DNC recruited female members of the Danish Nurse Organization ≥45 years in 1993. A total of 23,170 female members were invited to participate, of which 19,898 (86%) accepted. In 1999, the cohort was expanded to include 8,833 more nurses who turned 45 years in the period since 1993 (n = 8,344) or nurses that were re-invited amongst those that did not choose to participate in 1993 (n = 489). In total, the cohort includes 28,731 nurses (Fig. 1).
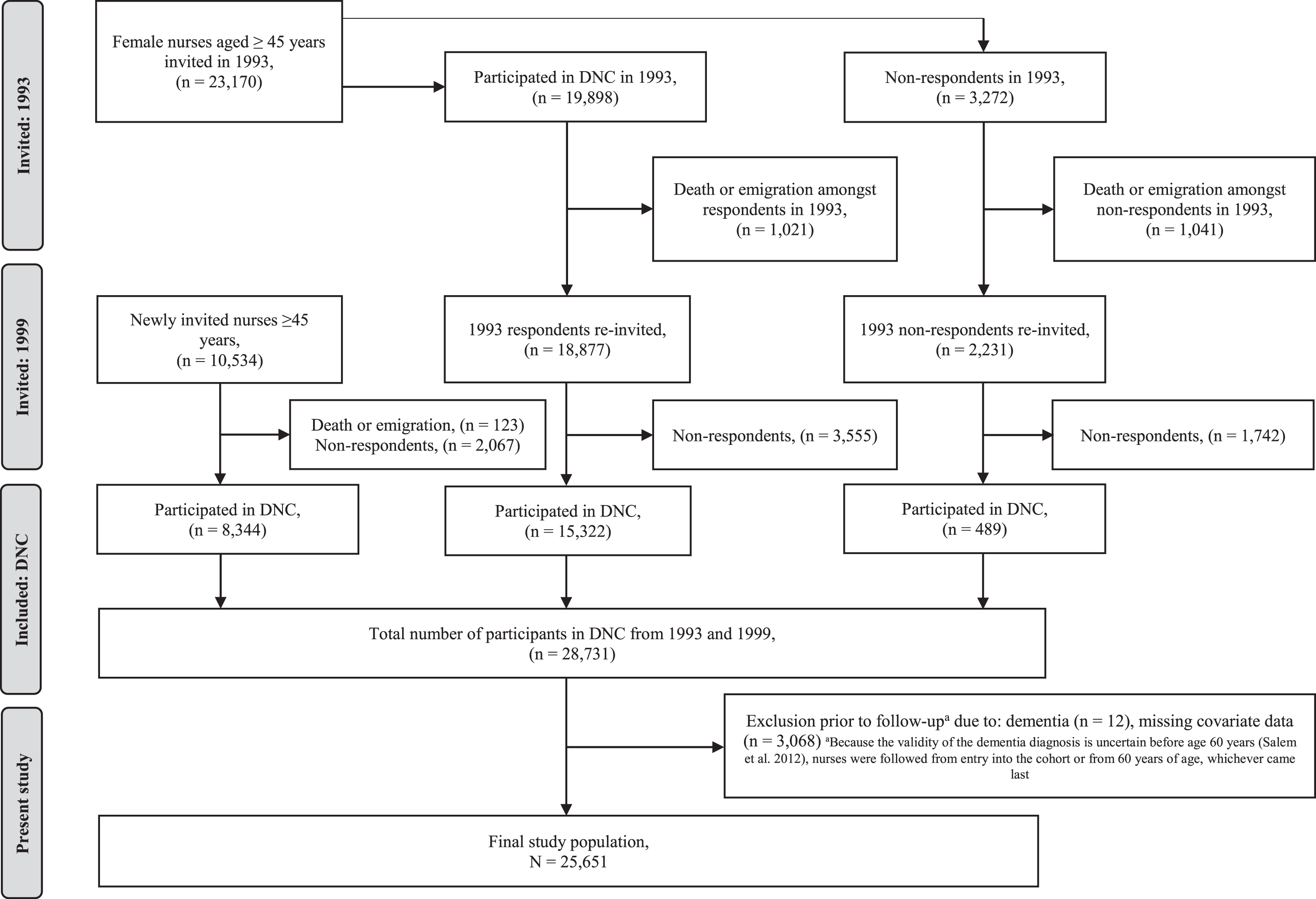
Population of nurses participating in the Danish Nurses Cohort (n = 28,731) and final study population (n = 26,651) after exclusions during follow-up.
Information on lifestyle factors, parity, age at menarche, oral contraceptive use, HT use, and self-reported height and weight was retrieved from baseline questionnaire data. Data from the DNC were linked to the Danish Civil Registration System to obtain individual demographic data such as emigration and death [25, 26] using unique national identification numbers. Identification numbers were linked to diagnoses, procedures and prescriptions using the National Patient Registry, the Psychiatric Central Research Registry and the National Prescription Registry [27–29].
Study population
The sample population were 28,731 nurses from the DNC (Fig. 1). A total of 3,080 nurses were excluded due to dementia before follow-up (n = 12) or missing covariate data (n = 3,068). In total, 25,651 nurses were included for complete case analysis.
Depression (exposure) ascertainment
Depression was defined by the date of the first of at least two retrieved prescriptions for antidepressants (from the National Prescription Registry) and multiple prescription retrievals were recorded in both mid- and later-life. Nurses with antidepressants use prior to start of follow-up entered the model as exposed. Nurses with no prior antidepressants use were the reference group. The potential association between depression and dementia were considered overall and stratified based on nurses age when she retrieved her antidepressant prescription.
Incident severe depression was identified independently by the first date of depression diagnosis recorded in the National Patient Register and Psychiatric Central Research Registry using International Classification of Disease (ICD [8/10] codes [hospital admission]). The association between severe depression and dementia was assessed independently. Details of codes are included in the Supplementary Material.
Dementia (outcome) ascertainment
Incident dementia was identified as the date of the first diagnosis recorded in the National Patient Register or the Psychiatric Central Research Registry using the ICD (8/10) or as the date of the first filled dementia medication prescription in the National Prescription Registry, whichever came first. Hospital admission dementia diagnosis ICD codes in National Patient Register / Psychiatric Central Research Registry enabled ascertainment of dementia subgroups including AD, VaD, and other (frontotemporal, unspecified and Lewy body) dementia. Details of diagnosis and prescription codes are included in the Supplementary Material. As the validity of the dementia diagnosis is uncertain before age 60 years [30], all 25,651 nurses were followed from entry into the cohort or from 60 years, whichever came last. Follow-up continued until date of incident dementia, death, emigration, or December 31, 2018, whichever came first.
Covariates
Potential confounders and key covariates were identified a priori based on known risk factors for depression and dementia [31]. Baseline confounder data from DNC included BMI (underweight (<18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), obese (≥30 kg/m2)); physical activity (low [sedentary], moderate [light exercise ≥4 h/week], high [frequent elite sports or heavy lifting]); smoking status (never, previous, current); alcohol consumption (none, <7, 7–14, ≥14 units); use of oral contraceptives (never, ever); and use of HT at baseline (never, ever). Both age at menarche (≤12, >12 years of age); and parity (nulliparous, parous) were also included as potential confounders since previous studies have reported that risk of both depression and dementia may be affected by these factors [32–35]. Nurses who had undergone hysterectomy or oophorectomy were identified using hospital ICD-procedure codes recorded in the National Patient Register. Incident CVD was defined from ICD-8 and ICD-10 codes in the National Patient Register. Types of CVD included hypertensive heart disease, ischemic heart disease, stroke, cardiac arrest infarction and other.
Statistical methods
Descriptive statistics were calculated for all included variables stratified according to exposure (antidepressants use) and outcome (incident dementia) separately. Between group differences for categorical variables were tested with Pearson’s chi-square test.
In our main analyses, we applied Cox proportional hazards regression models to investigate the association between depression (ascertained by antidepressant use) and risk of dementia. Results were expressed as hazard ratios (HRs) with 95% Wald-type confidence intervals (CI) of incident dementia (all-cause, AD, VaD, and other) following depression and compared to referent nurses. The association between depression and all-cause dementia was classed as midlife (<60 years), later life depression (≥60 years), or recurrent (both mid- and later-life). Model 1 was adjusted for age as an underlying timeline and calendar period. Model 2 was further adjusted for BMI, physical activity, CVD, alcohol consumption, smoking status, age at menarche, parity, oral contraceptives, HT, hysterectomy status, oophorectomy status. To address times since depression onset, we included depression treatment onset in all models as a time-varying categorical variable. In supplementary analysis, we repeated the main analyses and measured the association between incident severe depression (hospital admission) and dementia (all-cause, AD, VaD, and other). We were unable to stratify by age at diagnosis in these analyses due to power constraints.
Effect modification: The modifying effects of CVD, BMI, HT, or physical activity on the association between depression treatment and all-cause dementia were estimated by comparing all-cause dementia risk in nurses with and without depression within the levels of each effect modifier using the likelihood ratio test for interaction in model 2, but without adjustment for the interaction variable.
Kaplan-Meier plots illustrate time course free of all dementia, using age (years) as the horizontal (x) axis and probability of not being diagnosed with dementia (proportion without dementia) as the vertical (y) axis, according to overall depression treatment (yes, no). All statistical analyses and graphical presentations were produced in R version 4.0.3 (R Core Team, 2016), using the following packages: dplyr, stats, survival, splines, mets, gplots, plotCI, and Hmisc. All statistical tests were two-sided, and p-values <0.05 were considered statistically significant.
The manuscript follows the Enhancing the Quality and Transparency of Health Research (EQUATOR) reporting guidelines for observational studies (STROBE).
Ethical considerations and data protection
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and the Helsinki Declaration. The nurses included in the DNC provided informed consent and recruitment into the cohort was approved by the local Danish Ethical committee (J. nr. BFH-2019-001, suite nr. 06102). The study was approved by the Danish Protection Agency (J.nr. VD-2018-451, suite nr. 06707).
RESULTS
Basic characteristics
In total, 8,086 (31.5%) nurses receiving at least two prescriptions for antidepressants were identified. Characteristics of the study population stratified by retrieval of antidepressants are presented in Table 1. At baseline, nurses who retrieved antidepressants were slightly more likely to be overweight to obese (BMI ≥25 kg/m2), current cigarette smokers, either non-drinkers or heavy drinkers, physically inactive, nulliparous, HT users with hysterectomy/bilateral oophorectomy, and previous hospital CVD admission compared to nurses with no record of antidepressant use. Hospital admission for major depression was more prevalent amongst nurses who had retrieved antidepressants (n = 1,073, 13.3%) compared to nurses with no such record (n = 47, 0.3%).
Person-related characteristics of 25,651 female nurse (Danish Nurse Cohort) stratified by depression
Depression identification was based on prescription retrieval. Depression was a time-varying exposure, midlife only (<60 years, n = 1,462), later life only (≥60 years, n = 4,506). aIncluding beer (regular and strong), wine (red and white) and liquor. bBased on all incident cases ascertained at age ≥60 years in the Danish Hospital (ICD codes) and National Prescription (Anatomical Therapeutic Chemical Classification codes) Registry, whichever came first. cDiagnosed ≥60 years and based on ICD codes in the Danish Hospital Registry only. dIncluded frontotemporal dementia, unspecified dementia, and Lewy bodies. *p < 0.05, Pearson’s chi-squared test of homogeneity in strata of depression.
A total of 1,232 (4.8%) nurses developed dementia during follow-up. Where the type of dementia was known (based on hospital admission records), 726 (58.9%) had AD and 132 (10.7%) had VaD (Table 1). Nurses with dementia were more likely to be overweight (BMI: 25–29.9 kg/m2) and be previous smokers, non-alcohol drinkers, inactive, and HT users with a previous hospital admission for CVD, compared to nurses with no dementia record (Supplementary Table 1). Overall, the 3,148 excluded nurses were slightly younger at baseline than the 25,651 included nurses with comparable baseline characteristics (Supplementary Table 2).
Hazard ratios of dementia
The main regression analyses are presented in Tables 2, 3, and Fig. 2. In fully adjusted analyses, depression (prescription retrieval) was associated with an over five-fold increased risk of all-cause dementia (aHR 5.23:95% CI, 4.64–5.91), compared to nurses with no antidepressant prescription retrieval. The differential effects were more elevated for VaD and other dementia (aHR 7.96:95% CI, 5.26–12.0 and aHR 6.54:95% CI, 5.19–8.22) than for AD (aHR 4.64:95% CI, 3.97–5.42) (Table 2). Depression in later-life only (>60 years) (aHR 5.85:95% CI, 5.17–6.64) and recurrent depression (both mid- and later-life) (aHR 3.51:95% CI, 2.67–4.61) were associated with statistically significant increased dementia risk, while midlife depression only (<60 years) was not (aHR 1.24:95% CI, 0.68–2.28) (Table 3). In supplement, severe depression based on hospital admission, was associated with a statistically significant increased risk of all-cause dementia, but of a lower magnitude (aHR 3.14:95% CI, 2.62–3.76). The differential effects were similarly more elevated for VaD and other dementia (aHR 4.27:95% CI, 2.66–6.85 and aHR 4.10:95% CI, 3.06–5.52) than for AD (aHR 2.01:95% CI, 1.53–2.65) (Table 2).
Hazard ratios (HR) and 95% confidence interval (CI) of all-cause dementia, Alzheimer’s disease, vascular dementia, and other dementia in nurses (followed ≥60 years) from the Danish Nurse Cohort (n = 25,651) with depression treatment compared with referent women with no prescription retrieval for depression
*Depression exposure status based on age at prescription retrieval (ascertained in the Danish National Prescription Registry based on Anatomical Therapeutic Chemical Classification codes) entered the Cox model as time-varying variable. **Depression exposure status based on hospital admission for severe depression (ascertained in the Danish Patient Registry based on ICD diagnosis codes) entered the Cox model as a time-varying exposure. aAdjusted for attained age as the underlying timeline and attained calendar period. bAs for model 1, with further adjustment for cardiovascular disease (ever/never), body mass index (underweight, normal, overweight, obese), smoking status (never, previous, current), alcohol consumption (none, low, moderate, high), physical activity (low, moderate/high), age at menarche (≤12, >12 years of age), parity (nulliparous, parous), oral contraceptives (never, ever), hormone therapy (ever, never), hysterectomy (yes, no), any oophorectomy (yes, no).
Hazard ratios (RR) and 95% confidence interval (CI) of all-cause dementia in nurses (followed ≥60 years) from the Danish Nurse Cohort (n = 25,651) with depression treatment (mid-, later-, and recurrent [mid/later life]) compared with referent women with no depression treatment
Depression exposure status based on age at prescription retrieval (ascertained in the Danish National Prescription Registry based on Anatomical Therapeutic Chemical Classification codes) entered the Cox model as a time-varying variable. aAdjusted for attained age as the underlying timeline and attained calendar period. bAs for model 1, with further adjustment for cardiovascular disease (ever/never), body mass index (underweight, normal, overweight, obese), smoking status (never, previous, current), alcohol consumption (none, low, moderate, high), physical activity (low, moderate/high), age at menarche (≤12, >12 years of age), parity (nulliparous, parous), oral contraceptives (never, ever), hormone therapy (ever, never), hysterectomy (yes, no), any oophorectomy (yes, no).
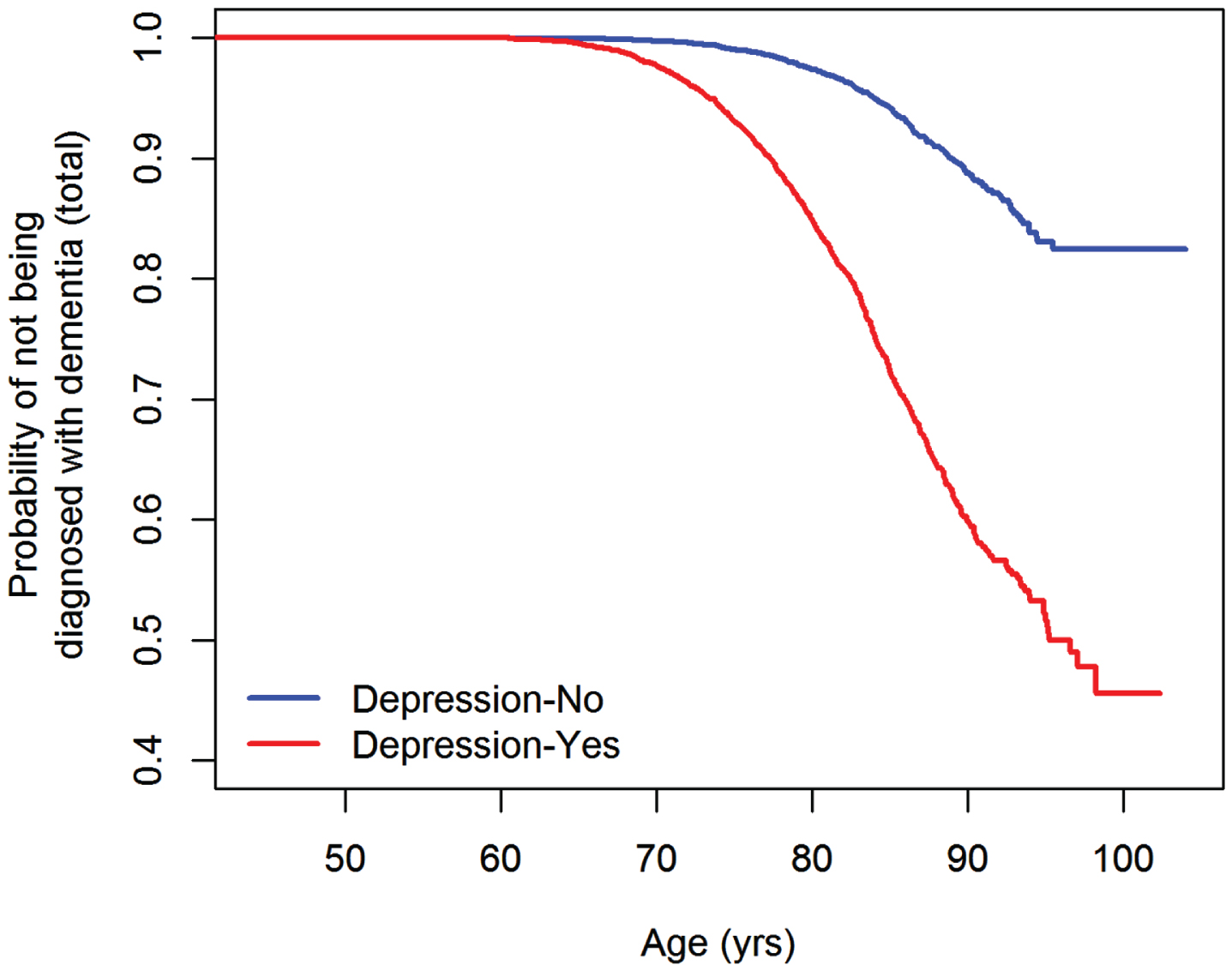
Kaplan Meier plots for time course free of all-cause dementia.
The time course to all-cause dementia is illustrated in Kaplan Meier plots according to prescription retrieval/no prescription retrieval for antidepressants (main exposure) (Fig. 2). The oldest diagnosis of dementia was made at age 96 years. Figure 2 shows that nurses treated for depression followed a strikingly different time course for all-cause dementia compared to nurses not treated for depression, confirming our estimates.
Effect modification
Effect modification analyses applying the main adjusted model are in Table 4. The effect modification of HT use was statistically significant (pinteraction = 0.02). Although associations were strong in both strata, the association between depression and dementia was greater in non-HT users (aRR 5.72; 95% CI, 4.90–6.67) versus HT users (aRR 4.60; 95% CI, 3.78–5.58) with only a small overlap in confidence intervals. Depression was associated with a statistically significant increased risk of dementia within all strata of other effect modifiers, including CVD (yes versus no), BMI (≥25 kg/m2 versus <25 kg/m2) and physical activity (moderate/high versus low), but without significant interaction between the strata (pinteraction ≥0.18), and with similar effect sizes for strata within different modifiers.
Effect modification of the association between depression (prescription retrieval) and dementia by hormone therapy (HT), body mass index (BMI), physical activity (PA) and cardiovascular disease (CVD). Female nurses with no depression (prescription retrieval) served as reference group
aAdjusted for attained age as the underlying time-line and attained calendar period, cardiovascular disease (ever/never), body mass index (underweight, normal, overweight, obese), smoking status (never, previous, current), alcohol consumption (none, low, moderate, high), physical activity (low, moderate/high), age at menarche (≤12, >12 years of age), parity (nulliparous, parous), oral contraceptives (never, ever), hormone therapy (ever, never), hysterectomy (ever, never) and any oophorectomy (ever, never). But with no adjustment for the interaction variable. *Test of the null hypothesis that the Hazard Ratios are identical, from likelihood ratio test for interaction.
DISCUSSION
In this large, national prospective registry-based cohort study of 25,651 nurses we found a statistically significant five-fold increased risk of dementia in nurses with later life depression (>60 years) versus those with no previous depression history. This was moreover greater for VaD than AD. These observations are consistent with a 2022 systematic review and meta-analysis of 33 studies measuring the association between depression and risk of dementia, which reported a doubling in risk for all-cause dementia in those with previous depression (pooled relative risk [RR] 1.96:95% CI, 1.59–2.43) with strongest associations for later-life depression [36]. The relatively larger risk estimate found in our present study may reflect the longer follow-up period enabling ascertainment of more dementia as well as varying methods for classifying depression.
Some previous studies have reported that severe depression confers a greater risk of dementia, although severity was defined in different ways [36]. Among women defined with depression based on a hospital admission diagnosis for depression, we did not find an increased dementia risk. However, only 1,120 nurses were hospitalized for depression in our study, around eight-times fewer than those treated with antidepressants.
Our study addresses limitations of previous research in this field. It is the largest study of women uniquely adjusted for reproductive health, HT use, included dementia subtype and applies a long follow-up of 23 years. Only one previous study has applied a follow-up of more than two decades [37, 38]; however, that study only considered effects of depression on AD. Other studies of depression and VaD have had less than a decade of follow-up [12]. We found that only later life and recurrent depression increased dementia risk. Since the prodrome for dementia can be up to 25 years, our findings may indicate that depression is a prodrome for dementia [39]. However, nurses were recruited to the cohort aged ≥45 years and 1,462 were then diagnosed with midlife only depression, compared to 4,506 diagnosed in later life only, decreasing statistical power to detect an effect of midlife depression alone. Unlike some previously published studies, we did not observe an increased risk of dementia with recurrent depression. This differs from longitudinal data from 13,500 members of Kaiser Permanente, which reported a three-fold increased risk of dementia in those with both mid and later life depression [38]. Likewise, the Baltimore Longitudinal study of Aging followed women from midlife for up to 50 years and reported that one depressive episode conferred an 87–92% increase in dementia risk, while at least three episodes nearly doubled the risk, with each additional episode conferring a 14% increased risk of dementia [37].
Only one other prospective study of a 6-year follow up included a larger number of incident VaD cases [38]. It also used medical records for diagnoses, and similarly found a far stronger risk associated with VaD than AD with depression [38]. These findings are also consistent with cross-sectional data showing that depressive symptoms are more common in VaD than AD [36] and are consistent with a recent meta-analysis showing that the risk of VaD associated with depression is larger than the risk of AD [36]. They strengthen the view that incident later life depression shares vascular origins with vascular cognitive impairment, potentially via the psycho-immune-neuroendocrine network [40].
Both depression and dementia are associated with CVD [18, 19]. We observed that nurses with dementia were more likely to smoke and have a high BMI, determinants that are common risk factors for both depression, dementia, and CVD [20]. However, the association between treated depression and dementia was not conditional on CVD. This is not consistent with the Framingham Heart Study which reported that non-stroke CVD at age 65 years was a risk factor for later-life dementia [41]. However, only 57% of the Framingham study were female which limits direct comparisons.
Whether HT increases or decreases dementia risk is extensively debated [21–23]. We observed a stronger association between depression and dementia in non-HT users suggesting a potentially protective effect. However, HT-users may be more engaged with the healthcare system such that risk factors for dementia (such as hypertension) were more likely to be treated.
Strengths and limitations
This prospective longitudinal study utilized a large and well-defined national cohort. The cohort has well characterized baseline data, a long follow-up period and objectively ascertained exposures and outcome through unique linkage to Danish national registries. All Danish female nurses were invited to participate in this cohort, reducing potential selection bias, and the excluded nurses in the present study were comparable to the included. Data quality and validity is high as reporting to the registries is compulsory in Denmark [42] and because Danish health care is fully reimbursed, socioeconomic factors play a limited role in healthcare-seeking compared to countries where healthcare is charged at the point of delivery. In contrast to many previous studies, the DNC is particularly homogenous regarding educational and socioeconomic factors, reducing potential confounding by socio-economy. In our present study, nurses were followed for dementia after age 60 years, and this limited uncertainty about the validity of the diagnosis before age 60 years [30]. We could ascertain the type of dementia based on both hospital record registries and prescription redemption, allowing inclusion of participants in the community and in hospital. This reduces differential misclassification of nurses as non-cases which occurs in studies predicated on hospitalization.
Among study limitations, we acknowledge that the ascertainment of depression was based on retrieving at least two antidepressant prescriptions, which may underestimate the prevalence of depression which is often unrecognized and untreated. In addition, as depression was ascertained by antidepressant use, we were unable to determine whether the increased dementia risk was due to depression or to antidepressant use. Importantly, depression can cause cognitive impairment which may be misdiagnosed as dementia [43], which could imply potential exposure and outcome misclassification. Moreover, antidepressants can also be used to help treat other mental health conditions, including anxiety, obsessive compulsive disorder, panic, bulimia, post-traumatic stress disorder, as well as treatment of menopausal vasomotor symptoms; none of which we were able to confirm, implying the potential of some exposure misclassification. Potential surveillance bias may have been implied, as it is possible that people with depression are more closely surveilled for all mental health diagnoses including dementia, and this might partly explain the large effect sizes detected in our present study.
Although we adjust our statistical models for several important confounders, we recognize that both depression and dementia are multifactorial and heterogeneous conditions and anticipate that causal factors will be inherently complex. For example, antidepressants may cause weight gain and we cannot quantify how this might affect our estimates. Moreover, given this multifactorial complexity it is important to note that the detected associations in our present study do not imply causality.
Our finding that HT modified the association between depression and dementia should be interpreted with care as HT reporting was limited to baseline use which may have changed throughout follow-up. Also, we do not know the type or dose of HT used which may have influenced our outcomes [44]. Use of HT was not randomized, and HT users may be more likely to seek health care which might influence both outcomes and exposures. We further acknowledge that the findings from the present study are not necessarily generalizable to all other populations. The included population was predominantly Caucasian and representative of the general Danish female nurses at that time, but we expect ethnicity in other populations may play a role and sex differential effects would be expected in a male population.
In this large prospective cohort study of female nurses with an average of 23 years of follow up, later life but not midlife depression was associated with a five-fold increased risk of all-cause dementia, with a stronger effect seen for VaD. Future research should aim to elucidate the mechanisms that mediate these associations.
Footnotes
ACKNOWLEDGMENTS
We are extremely grateful to the nurses who took part in this study and the Danish Nurse Cohort Team for cohort coordination and data collection. We thank the Danish Nurse Cohort steering group for approving our access to the data.
FUNDING
The research being reported in this publication was funded by The Health Foundation of Denmark (Helsefonden, Grant no. 19-B-0077). The funding covered salaries for Trine Koch Hueg and Elvira Bräuner. Martha Hickey is supported by a NHMRC Investigator Grant (ID number 1193838). Kaarin Anstey is supported by ARC Laureate Fellowship FL190100011. The funding bodies played no role in the design, collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
CONFLICT OF INTEREST
Kaarin J. Anstey is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
Data used in the present study is governed and maintained centrally by the Danish Data Health Authority and data access is regulated by European Union General Data Protection Regulations. Data are not publicly available and anonymized data can only be accessed after approval by the Danish Data Health Authority and the Danish Data Protection Agency.