
Abstract
Background:
Il Paese Ritrovato is an Italian nursing home founded in 2018, it is based on the Alzheimer village model and admits people with mild-to-moderate dementia.
Objective:
Describe the impact of the SARS-CoV-2 pandemic on people living at Il Paese Ritrovato through a Comprehensive Geriatric Assessment (CGA) regularly administered prior to and during the pandemic.
Methods:
We explored the effects of a person-centered approach. We assessed 64 subjects (enrolled and followed between June 2018 and December 2020), who underwent at least 18 months of observation prior to the pandemic. Each subject was evaluated using a CGA on admission time (T0) and at defined time-points: T6, T12, T18. One last CGA evaluation was performed during the SARS-CoV-2 pandemic (TCovid-19). Temporal trends during T0–T18, and differences between T18 and TCovid-19 were calculated.
Results:
The mean age was 82 years with a prevalence for females (77.0%) and Alzheimer’s disease diagnosis (60%). Psychiatric and behavioral disorders were the most common conditions (80%). We utilized a nonpharmacological approach aimed at promoting the residents’ overall wellbeing and observed satisfactory performance during the first 18 months. In comparison with the pre-pandemic period, TCovid-19 enlightened +11.7% use of antidepressants and a decline of Mini-Mental State Examination mean values (not statistically significant), while engagement in activities dropped.
Conclusions:
The pandemic may have disrupted the existing model of care, but at the same time, it confirmed that the Il Paese Ritrovato approach, which encompasses symptoms improvement and multicomponent support, is in fact beneficial.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a common type of dementia, with a prevalence of 4.4% in Italians over age 65; furthermore, AD prevalence increases as the population ages and in the female subgroup [1]. For instance, AD prevalence among females aged 65–69 is 0.7%, but increases precipitously to 23.6% among females ≥90 years. Males, on the other hand, have a prevalence of 0.6% and 17.6% respectively, for the same age groups [2]. Because dementia includes a number of chronic disorders with currently irreversible progression, treatment must therefore focus on the individual’s quality of life (QoL) [3, 4].
In this context, uncontrolled behavioral and psychological symptoms of dementia (BPSD) often represent a determinant for nursing home new admissions [5, 6] According to the DSM-5, BPSD commonly include many disturbances that range from apathy to severe agitation and combativeness. Such disturbances are frequent among community-dwelling subjects with dementia, impairing their QoL and representing a burden for caregivers and family members. Although psychoactive medications may cause adverse drug reactions, they are still commonly prescribed when facing BPSD [7]. Non-pharmacological approaches may represent a more suitable strategy to follow when caring for AD or other dementias. To this end, approaches such as the person-centered care (PCC) have been developed with the aim of recognizing the uniqueness of each person with dementia, their unmet needs, and factors that trigger BPSD in order to adjust the care and support strategies [8]. The available literature has already proven the significant benefits of PCC versus usual care when treating persons with cognitive impairment, in terms of better symptoms control and QoL [9–11]. However, studies that explored how COVID-19 affects the PCC model are still limited.
The Alzheimer village Il Paese Ritrovato is an innovative care model that focuses on the unmet needs of people with mild-to-moderate AD (or other dementias). In this facility, PCC is integrated with other interventions that are crucial for promoting QoL in dementia, such as movement stimulation, personalized and significant activities, and social inclusion [12–14].
This prospective observational study was performed at Il Paese Ritrovato with the aim of underlining the influence of the care setting on the patient with cognitive frailty. We investigated the temporal trend of our Comprehensive Geriatric Assessment (CGA) before the SARS-COV-2 pandemic to see whether there were some potential benefits of this environment towards the well-being of the person with dementia. As a secondary aim, we evaluated the impact of the pandemic and its containment measures on the evolution and adaptation of the care setting, comparing pre- and during-pandemic CGA values [15].
METHODS
Setting
Il Paese Ritrovato was inaugurated at the beginning of 2018 by Cooperativa La Meridiana (Monza, Italy). This facility was built as a community neighborhood and represents the first experience of an Italian Alzheimer’s village. Its buildings are easily recognizable by the residents, just like in any neighborhood. This aspect allows them, even in a context of cognitive impairment, to move freely and to actively conduct their daily life based on their own rhythms and choices. The purpose of Il Paese Ritrovato is to promote the social inclusion of persons with dementia and to improve their QoL, minimizing the discomfort or the need for intervention that can be expressed by the onset of BPSD [16].
In general, the village has been structured into 8 apartments, each consisting of 8 single rooms with bathrooms. The total area of Il Paese Ritrovato is 3,360 square meters and it can accommodate a maximum of 64 guests with each space properly furnished. The everyday activities are part of the experimental therapy used to stimulate the residents’ cognitive functions and provide them with a satisfying QoL. Each room is customizable to prevent spatio-temporal orientation loss and BPSD. The whole space is considered Ambient Assisted Living (AAL), and it uses technologies such as an adapted lighting system, air handling units and user-friendly small appliances [17]. For example, room lighting optimizes the circadian rhythm using sensors that adjust brightness based on real-time external conditions and ensures orientation in various spaces. This enables residents to live safely, while safeguarding their residual capacity and supporting their integration with the community and caregivers. The modular furniture has easy openings and presents graphic symbols to communicate precise information. The educational activities are offered both in the apartments and mainly at the “Central Pole”, or central square of Il Paese Ritrovato. This Centrale Pole consists of communal and gathering spaces including workshops, a movie theater, beauty salon, bar, minimarket, gymnasium, and church. People may access these places freely either spontaneously or by invitation.
Cohort selection
The 91 subjects admitted to Il Paese Ritrovato from June 2018 (i.e., when the facility was opened) to December 2020 (i.e., nearly one year after the SARS-COV-2 pandemic outbreak) were recruited in the study. All these subjects were diagnosed with dementia according to the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) [18], confirmed by a specialist in neurology or geriatrics [19]. In order to be admitted to Il Paese Ritrovato, each subject should have a Clinical Dementia Rating scale (CDR) value ranging between 0.5 (questionable dementia) and 2 (moderate cognitive impairment) and should be able to walk independently [20]. The presence of BPSD, even severe ones, and incontinence did not constitute exclusion criteria. Each cohort member was followed-up from the date of admission to Il Paese Ritrovato until the earliest date among discharge for any reason (e.g., death, emigration, etc.) from the facility or December 31, 2020.
Among the 91 subjects admitted to the facility between 2018–2020, 76 subjects experiencing a minimum follow-up period of 18 months were identified. For each cohort member a Comprehensive Geriatric Assessment (CGA) was administered at established time-points (T0, T6, T12, T18, and TCovid-19). In particular, T18 was the latter time-point of CGA evaluation before the SARS-COV-2 pandemic, whereas at TCovid-19 corresponds the evaluation performed in July 2020, after the pandemic outbreak. During the follow-up period, a multidisciplinary team, including a geriatrician, psychologists, occupational therapists, nurses, educators, and social workers, monitored the cohort members and assessed every six months the residents’ health status through the same validated tests proposed at the baseline (excluding demographic information, which is collected at baseline only). The CGA was then performed at T0, T6, T12, T18 (before the SARS-COV-2 pandemic), and TCovid-19 (July 2020, during the pandemic). For the purposes of the study, the subjects who did not receive a CGA at TCovid-19 were excluded from the analysis. The remaining 64 patients represented the final study cohort, as depicted in Fig. 1.
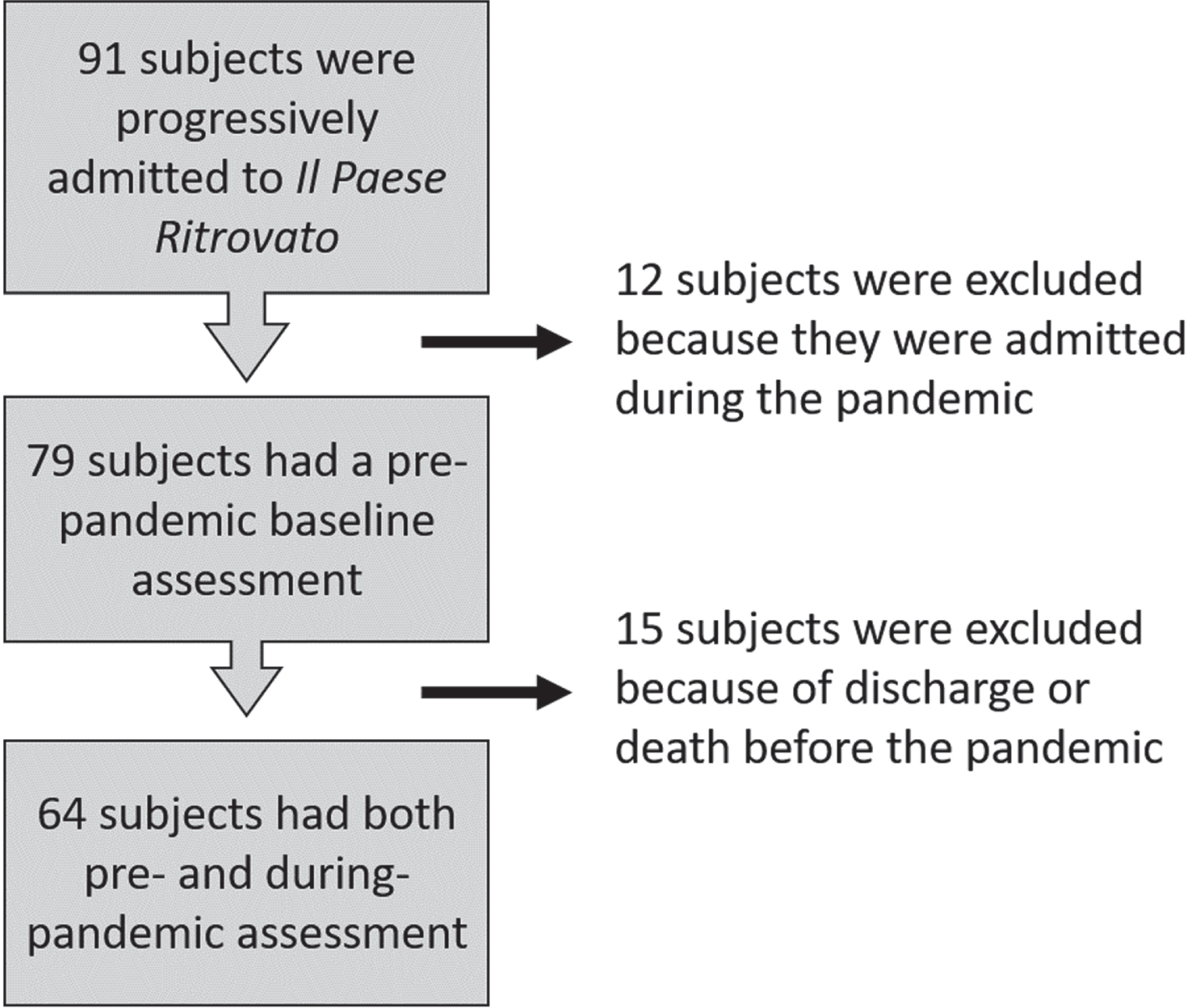
Flow chart of the selection process.
General assessment
The variables describing participants’ socio-demographic characteristics were age, sex, and living status (i.e., home situation of origin). This information was assessed at the baseline (i.e., the date of admission to the facility). Other characteristics assessed at the baseline included the CIRS tool (Cumulative Illness Rating Scale) [21], through which we were able to calculate severity and comorbidity indexes. As for medications, psychopharmacological therapy related to AD and to the management of BPSD were of particular concern. Thus, we collected information regarding antidepressant drugs, benzodiazepines (BDZ), typical and atypical antipsychotics, and antiepileptics.
Functional level and other clinical domains (behavior, cognition, physical status) were collected. Researchers involved in this study focused on single domains, e.g., geriatricians focused on health status and cognition, occupational therapists focused on the engagement in the activities, and physical therapists assessed functional status. Each researcher performed the same tests at each time point according to their competence, being blinded to the assessment performed by the others.
Comprehensive geriatric assessment (CGA)
For the aims of the study, the CGA evaluation values considered were those related to the following variables: MMSE, Barthel Index, NPI score, Cornell score, ISE score, Tinetti scale, CDR scale, and BMI.
With more detail, the CGA consisted in a battery of tests evaluating cognitive functions, behavioral disorders, the residents’ QoL, functional and nutritional status, risk of falling, engagement in occupational therapy and socio-recreational interventions, and the caregivers’ level of stress.
As already detailed, we used the CDR scale to describe the pathological stage of dementia. For the screening of cognitive status, we adopted the Mini-Mental State Examination (MMSE) [22]. To explore the resident’s well-being and QoL we performed the Quality VIA interview [23]. This interview is intended for people with MMSE scores up to 13 and allows the assessment to be quantified in a numerical score, the variations of which can be monitored at repeated intervals over time. Functional status was assessed through the following measures: Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL) [24–27] and modified Barthel Index scale [28]. We adopted the Neuropsychiatric Inventory (NPI) both for clinical purposes, to assess the presence of BPSD, and to evaluate the stress load to which family members, caregivers and professional staff are subjected [29, 30]. Depressive symptoms were evaluated through the Cornell Scale for Depression in Dementia (CDS) [31], while the effectiveness of socio-recreational interventions was assessed using the ISE tool (Index of Social Engagement) [32]. We measured commitment to social and individual activities with a numeric scale, graded from 0 (no commitment) to 6 (maximum commitment). The Tinetti balance and Gait Scale is an easy-to-use, widespread and validated tool that has proven to be a good predictor of falling. It is widely used within our facility for its accuracy in evaluating motor functions such as subjects’ mobility, balance, and gait. The cut-off for low versus high risk of falling was set at 20: the lower the score, the higher the risk. The Conley scale, when combined with the Tinetti scale, offers a good prediction of the risk of falling. The Conley score ranges from low risk (0 points) to maximum risk (10 points), with a cut-off at 2 for identifying an increased risk of falling [33]. To assess the caregivers’ stress, we used the Caregiver Burden Inventory (CBI) because of its capability of analyzing its multidimensional aspect among the caregivers of people suffering from AD and other dementias [34]. To account for comorbid conditions, we adopted the Modified CIRS, through which we calculated two indices: one to measure the comorbidity level and one for the severity. CIRS considers 14 classes of conditions and assigns a score from 0 to 5 based on the severity of each condition. In the calculation of the CIRS comorbidity and severity indices, psychiatric pathologies and neurodegenerative dementias are excluded, except in the case in which dementias have a vascular basis. In that case, they fall under the section of “neurological pathologies”.
Statistical analysis
Data was collected in an ad hoc database and managed anonymously, with access allowed exclusively to healthcare professionals. To preserve privacy, personal details were deleted, and identification code was automatically anonymized.
Continuous variables were described as mean±standard deviation (SD), whereas absolute frequencies and percentages were reported for categorical variables.
To evaluate the temporal trend of the considered CGA evaluations, before the SARS-COV-2 pandemic outbreak (T0–T18), a Joinpoint regression analysis (JPA) [35] was performed. Values of CGA at T0, T6, T12, and T18, were considered. Only the CGA indexes without missing values at each time-point were considered in the analysis. JPA is usually applied to study varying trends over time to identify the time point(s) in which the trend significantly changes. This analysis allows to identify inflection point(s) (called “joinpoint(s)”) at which there are significant changes in the linear slope of the trend. The number and location of significant joinpoint(s) for each considered CGA index were determined using a log-linear model. We estimated the annual percent change (APC) and corresponding 95% confidence intervals (CI) to describe the magnitude of the slope change for each temporal segment identified by the joinpoint(s) in the period T0–T18. Then we calculated the average annual percent change (AAPC) for the overall period (T0-TCovid-19) in trends of each CGA scale. Further details on the JPA to evaluate temporal trends have been previously reported by Rea et al. [36].
To evaluate the impact of the SARS-COV-2 pandemic on the evolution of the residents’ health status, a comparison between the values assessed in the CGA before (T18) and during (TCovid-19) the pandemic was performed. The T-test for paired data [37, 38] and its non-parametric equivalent, the Wilcoxon signed-rank test [39, 40], were used to assess whether statistically significant differences existed between the pre-pandemic and during-pandemic CGA scores, taking into account the non-independence of CGA assessments within each subject. Considering the distribution of the CDR values and its categorical ordinal nature, we used the Stuart-Maxwell test for marginal homogeneity [41–43] to compare the values before and during the pandemic.
Excel Software (from the Microsoft Office Personal Productivity Software Suite, Version 2019 16.0.6742.2048), Joinpoint regression software (version 4.8.0.1; Surveillance Research Program, USA National Cancer Institute, Bethesda, MD, USA), SAS Software (version 9·4; SAS Institute, Cary, NC, USA), IBM SPSS software (Version 24.0; IBM Corp., Armonk, NY, USA) and the R software (version 4.1.3/2022, R Foundation for Statistical Computing, Vienna, Austria) were used to perform all the analyses. For all hypotheses tested, two-sided p-values were used to evaluate the statistical significance, and all p-values less than 0.05 were considered significant.
Ethical issues
This research, with all of the methods and tests included in the CGA, was carried out as part of the routine evaluations at Il Paese Ritrovato. The Ethics Committee of Cooperativa La Meridiana (Monza, Italy) approved the administration of each test. The study design and methods comply with the standards of the Helsinki II Declaration.
With more detail, the choice to enter Il Paese Ritrovato as a resident is made in agreement with one’s family members/caregivers of reference. If the eligibility criteria are met, the subject is asked to sign an informed consent form in which he/she certifies: 1) acceptance of the care path shared with family members and the professionals of Il Paese Ritrovato; 2) acceptance to undergo regular assessments by the professionals through validated scales that explore different healthcare domains; 3) acceptance of the collection and processing of data, both for audit and research purposes, according with the Italian law “Personal Data Protection Code” (Legislative Decree n. 196, 30/06/2003, available at https://www.gazzettaufficiale.it/dettaglio/codici/datiPersonali). The family member/caregiver also signs the informed consent form, since this path is shared. The consent forms are archived at Cooperativa La Meridiana (Italy).
As already mentioned, the care path provides that every activity can be chosen freely, but always with the supervision or support of trained professionals who operate daily in all areas of the facility. Moreover, each resident undergoes regular interviews that aim to monitor cognition, mood, engagement in the activities, and QoL (the latter is also assessed among family members).
The administration of validated scales is part of the routine assessment of nursing homes in Italy, although there is no fixed protocol for the time-points of these assessments or restrictions in terms of the adopted scales. Furthermore, professionals working in nursing homes usually care for people with different kind and degrees of disability or dementia, for which they follow recognized treatment guidelines. Otherwise, Il Paese Ritrovato hosts a more homogeneous population, since its residents fulfil specific criteria for dementia (CDR 0.5 to 2) and are able to walk independently. For this reason, through the free choice to attend different activities and by stimulating the residents’ residual cognitive abilities, follow-ups are carried out regularly with the aim of monitoring the progress of quality of life, cognition, functional status and management of any behavioral disorders, for which professionals are specifically trained in the preferential use of non-pharmacological strategies.
To summarize, Il Paese Ritrovato adopts scales and methods that can be considered as “routine” in nursing home practice. The real difference of this model lies in how spaces are conceived, in the freedom of action of each resident within the facility (always with supervision), and in the systematic use of the assessment scales to monitor the residents’ well-being and for audit/research purposes.
RESULTS
As shown in Table 1, the subjects enrolled in the study are aged between 49 and 93 years old, with a mean age of 82 years (SD = 9.4). They are mostly females (77%), with AD being the most prevalent diagnosis (61%). Vascular dementia and dementia of mixed etiology was the other prevalent main diagnosis (7.8% and 15.6%, respectively). At the time of the admission to Il Paese Ritrovato, more than a half of the subjects were assisted by a caregiver and/or by a family member.
General baseline characteristics at admission of the 64 subjects living at Il Paese Ritrovato and included in the study cohort
AD, Alzheimer’s disease; CDR, Clinical Dementia Rating scale; CIRS, Cumulative Illness Rating Scale; CIRS-CI, CIRS Comorbidity Index; SD, standard deviation; ENT, ear, nose, and throat; GI, gastro-intestinal.
Comorbidity
The mean value of the CIRS severity index was 0.57±0.31, while the mean value of the CIRS comorbidity index was 0.97±0.94. Of the 64 admissions, 48 were followed by home care, while 12 came from a nursing home. In the analyzed period, the outcomes of the study participants showed that 7 of them were transferred to nursing home due to a clinical-functional evolution of the disease; 1 was transferred to hospice, 1 was transferred to an Alzheimer’s core.
Among the residents, 5 had a diagnosis of mental retardation, 39 had a diagnosis of AD including 1 with parkinsonism, 6 had dementia of vascular etiology, 9 had mixed dementia (neurodegenerative and vascular), 4 had frontotemporal dementia, and one had Lewy body dementia. Among the psychiatric-behavioral disorders, 10.4% of subjects had a history of depressive syndrome, while 1% had a psychotic syndrome. The remaining developed BPSD.
Cognitive and functional features
The MMSE scale reports unchanged data from the trend assessed prior to the pandemic. Data resulting from the comparison of the MMSE test score between T pre -Covid-19 (18.1±3.1) and the TCovid-19 (15.9±3.5) did not show a statistically significant difference. There seems to be a decreasing trend, despite it not being statistically significant, but we have to consider the normal course of cognitive decline, which is progressive.
Furthermore, as shown in Table 2, the CDR scores reported during the pre-pandemic period and those reported during the pandemic period were not significantly different. However, as reported in Table 3, from the results of the JPA, during the pre-pandemic period, CDR score increased significantly between T0 and T12 and decreased significantly between T12 and T18 (annual percent change, APC, equal to 8.7 and – 14.3, respectively, both statistically significant).
Analysis of the indexes included in the Comprehensive Geriatric Assessment and their evaluations at different time-points
Values are expressed as means±SD, and relative frequencies, unless otherwise specified. MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; ISE, Index of Social Engagement; BMI, body mass index; CDR, Clinical Dementia Rating. (1)Wilcoxon Signed-Rank Test; (2)T Test for paired samples; (3)Stuart-Maxwell test for marginal homogeneity; *Statistical significance at an alpha level of 0.05.
Joinpoint regression analysis of the average temporal trend of the various indexes evaluations included in the Comprehensive Geriatric Assessment
AAPC, Average Annual Percent Change; APC, Annual Percent Change; CI, Confidence Interval; NPI, Neuropsychiatric Inventory; CDR, Clinical Dementia Rating; BMI, body mass index; *p < 0.05 for significant change in trend.
There was a significant difference regarding Barthel Index values between T pre -Covid-19 (68.0±18.7) and TCovid-19 (61.0±19.7). As shown in Table 3, during the observation period (T0 – TCovid-19), a statistically significant decreasing trend was observed (AAPC = –7.2 (95% CI: –11.8, –3.9), i.e., the values of the Barthel index showed an average decreasing trend of 7.2% for each temporal period considered in the analysis). In particular, there was a significant decrease from period T0 to period T6 and from T6 to T18, with APCs of –0.6% (–0.3%, –0.9%) and –9.2% (–9.1%, –9.4%), respectively.
Behavioral and psychological symptoms
The evaluation of behavior disorders (NPI) and mood (Cornell scale) documented a worsening at TCovid-19 compared to the last monitoring prior to the pandemic. The trend of the NPI scale was similar to that of the Cornell scale, with the difference that latter showed a significant worsening from T pre-Covid-19 to TCovid-19 (p < 0.0001), whereas the variation from Tpre-Covid-19 to TCovid-19 was not statistically different from 0 for NPI. NPI and Cornell scales, however, showed decreasing trends during the pre-pandemic period (see Table 3).
Social engagement
As reported in Table 2, the mean values of ISE, an indicator of the residents’ engagement and involvement in social-recreational activities, showed a worsening from 3.4 at T18 to 3.1 at TCovid-19. The mean ISE values prior to the pandemic were significantly different from the values at TCovid-19 .
Mobility features
The mean score of the Tinetti scale, which initially maintained a certain stability so as to confirm the efficacy of a rehabilitative approach and active lifestyle, showed a significant decrease during the pandemic period (p-value <0.0001 from the relative T-test for paired data). However, we have to consider the natural course of AD and other dementias during the observation period.
Evaluation of caregiver distress
There are no results from the CBI scale as it was altered by the excessive emotional stress of the family members who, during the pandemic, were prevented from entering the facility and meeting the residents. The last monitoring of the scale was performed at T18, with a positive outcome regarding itsprogress.
Psychopharmacological therapy
No major changes were observed in the use of psychoactive medications, except for an 11.7% increase in the use of antidepressants (against a 1.7% reduction prior to the pandemic). We observed minor changes, such as a 5% increase in the use of atypical antipsychotics, a 1.7% increase in the use of benzodiazepines (BDZ) (with no reduction from the previous trend), and a similar trend for typical antipsychotics. As for the use of acetylcholinesterase inhibitors (AChE-i), there was no change at TCovid-19 compared to the pre-pandemic period, while the use of memantine increased 1.7% compared with the stability that emerged over the previous months.
DISCUSSION
The results of the comparison between the pre-pandemic and the TCovid-19 assessments show the effects of the preventive measures dictated by the pandemic. According to the restrictions, the use of public areas, which comprised both outdoor and indoor environments at Il Paese Ritrovato, was indeed discouraged [44]. A synopsis of the professionals’ roles and tasks are reported in Supplementary Tables 1 and 2, as well as the full-text document that describes the preventive measures adopted by Il Paese Ritrovato (Supplementary Material). In general, the pandemic-related policies determined huge problems by interrupting social and recreation activities for all nursing home residents. A recent survey described a number of interventions that were adopted to mitigate social isolation and loneliness of the residents in different US facilities [45]. Overall, nursing homes responded with measures and attempts to use technology (tablets, smartphones) and by increasing the time that professionals spend with the residents to make them feel less lonely and more cared for. These efforts were perceived as useful and helped in promoting QoL in nursing homes despite overall staffing issues and limitations dictated by the structures [45]. To the best of our knowledge, there are no studies investigating the impact of COVID-19 on models that match Il Paese Ritrovato, because Alzheimer villages are rare worldwide. However, the impact of the pandemic on the PCC approach in nursing homes has been recently investigated by Morgan et al. [46]. This survey showed that many pandemic-related barriers to delivering PCC emerged and contributed to exacerbate pre-existing challenges such as increased workloads, staff shortage, and consequent stress and burnout of the professionals. However, COVID-19 also created positive opportunities such as team strengthening, experience sharing, training and emotional support, and availability of protective resources, which overall acted as facilitators for maintaining different PCC approaches [46].
We speculate that, despite the pandemic-related limitations, a dedicated setting can still be helpful in promoting the QoL of its residents.
Our analysis showed that COVID-19 does not appear as an aggravating factor per se in the MMSE scores, but rather it seems to accentuate an already downward trend observed at the previous time-points. However, the monitoring performed at TCovid-19 records a CDR scale that seems to mirror an acceleration of the cognitive worsening, as resulted from the analysis on trend, showing a significant decrease during time, with a clear-cut major reduction when considering the COVID-19 period (Table 3). In this context, COVID-19 acts as an accelerator of a process that remained almost stable for the previous 12 months. The CDR is a clinical scale with a consolidated diagnostic utility and classification of severity which has a strong point global approach, and not only focused on the definition of the cognitive profile. By assessing cognitive performance against the habitual functioning in daily activities and in the context of the environment, the CDR could indicate how the Alzheimer’s village model of care can contribute to a better cognitive function beyond the cognitive efficiency assessed with the MMSE alone [20].
The decreasing trend in Barthel index scores is basically ascribable to the natural evolution of the disease. With the advent of the pandemic, the gradual worsening trend has not stopped its mostly steady descent, so that the COVID-19 factor does not seem to have significantly affected the scores.
The results of the NPI scale reveal a deterioration potentially due to the forced lack of participation in daily activities, consequent to isolation and to the absence of freedom of movement in the public areas of Il Paese Ritrovato. The assessments prior to TCovid-19 follow a more intense and clear reduction trend (from APC = –28.9 to APC = –6.5) and demonstrate the validity of the interventions adopted in the facility, i.e., an improvement in behavioral issues during the pre-pandemic full activity phase.
The analysis of data that emerged from the Cornell scale is similar. Prior to COVID-19, a statistically significant decrease emerged from the T12–T18 comparison, thus delineating an improvement ascribable to the model of care at Il Paese Ritrovato, which relies on the influence of its supportive environment and promotes the social engagement. The analysis of the results at TCovid-19 showed that there is evidence of a statistically significant worsening of the Cornell scale.
The ISE indicator highlights the steady participation of residents in socio-recreational activities in the pre-pandemic period, with reversal of the trend at TCovid-19. Indeed, the reported variation is slight and significant.
Pertaining the number of falls, we confirmed a finding already observed before the pandemic in our study population, i.e. that the bedroom is the environment where most falls occur. The increase showed at TCovid-19 likely reflects the fact that the residents spent most of the time in their own rooms compared to the pre-pandemic period. It can be inferred that frail people fall more during the period of isolation, in which sedentariness, decreased freedom of movement and lower activity levels affected their motor performance [47, 48]. The internal and external spaces at Il Paese Ritrovato are designed to reduce the risk of falling, which is an important measure to adopt in healthcare facilities. However, despite interventions to modify the settings in order to reduce the number of accidents and promote independent living, the risk of falling cannot be fully eliminated even in the best designed facilities. To maximize the risk reduction, we believe that multi-component preventive strategies should be pursued and implemented, especially in times such as the pandemic, possibly combining protective equipment with a greater staff time to spend with the residents. This latter aspect, considering the burden placed upon the healthcare professionals during the pandemic, has already emerged as a crucial barrier to the implementation of such measures [45].
CBI was not administered at TCovid-19 as a result of distance from families. This would have reported altered data due to high emotional stress on the families who were prevented from entering Il Paese Ritrovato and meeting residents during the pandemic. The last monitoring of the scale was obtained at T18, with a positive outcome regarding its performance. The statistical significance highlights the validity of this model of care and its extent, given that the pathology has the ability to involve the entire family of the subject with dementia [15, 49].
Finally, the comparison of psychopharmacological therapy in the period before and during the pandemic did not show significant changes, except for a modest increase in the use of antidepressants derived from a monitoring of depressive symptoms by the treating team. Interestingly, there was no significant increase in the use of antipsychotic medications at TCovid-19 despite the increase in the NPI score.
This study has several limitations. First of all, it is a single-center study performed on a relatively small sample, which does not allow us to generalize our findings. Second, we have to mention that the study population was selected according to specific criteria, which accounts for a potential selection bias, so that our sample is not representative of the general population or the typical nursing home population. Finally, since this was basically an observational study where each resident underwent a multi-component PCC, we have to account for information bias because of the potential inaccuracies in reporting the measurements [50].
Conversely, strengths of this work included the facility, which was specifically designed for promoting the QoL of subjects with dementia, and the CGA that was performed according to validated scales and conducted by trained specialists in their respective fields. The PCC itself, which by definition does not entail the same schedule and choices for the residents, integrates several strategies with the aim of maintaining their residual abilities for as long as possible. We speculate that Il Paese Ritrovato could represent an example to follow for developing non-pharmacological approaches that will contribute to changing the paradigm of the traditional nursing home care for people with dementia.
CONCLUSION
When considering chronic progressive disorders such as dementia, the main goal of care is to act against the modifiable risk factors that negatively affect QoL. Il Paese Ritrovato offers to its residents the opportunity of being active and moving freely in a familiar environment, where each person can be protagonist of their choices despite the presence of cognitive impairment. Trained professionals of Il Paese Ritrovato perform a PCC that is individualized for each resident, shifting the paradigm of traditional nursing home care with the aim of maintaining the highest possible level of autonomy [51–56].
Overall, from the analysis of the pre-pandemic period, a good efficacy of the care model of Il Paese Ritrovato emerges with respect to the resident’s well-being, expressed directly by the reduction of BPSD. We observed a sort of cognitive stability over an 18-month follow-up, with no change in the AChE-i therapy. We speculate that this effect is ascribable to cognitive, social, and motor stimulation offered by the facility in a dedicated environment.
The SARS-CoV-2 pandemic may have disrupted the existing organization in terms of model of care, with an orientation predominantly toward the preventive measures of isolation and social distancing of the residents. This generated a sudden hiatus in social relationships, free mobility, and in providing formal and informal cognitive stimulation. However, at the same time it confirmed the benefits of this approach in terms of symptoms improvement and multicomponent support.
Indeed, even though we observed a decline of MMSE and Barthel Index scores, these changes can be partially explained by the natural progression of dementia. With regard to the CDR, worsening from the pre-pandemic assessment may likely be attributable to changes in environmental and relational factors, and thus essentially to the discontinuation of all that we might call the “Il Paese Ritrovato approach” and its promotion of QoL in dementia subjects [57, 58].
In conclusion, although SARS-CoV-2 infection has brought great inconvenience to the management of our residents, it seems to indirectly demonstrate the validity of a model of care that is still scarcely adopted by specialized dementia centers, and that should be fervently promoted.
Footnotes
ACKNOWLEDGMENTS
The authors express sincere appreciation to the entire team of professionals of Il Paese Ritrovato, and also to all volunteers that contribute daily to promote the well-being and QoL of its residents. Last but not least, sincere thanks to Justin S. Brathwaite, MSc, for his contribution in editing the English language of this manuscript.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
Patrizia Mecocci is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
Information and data collected at Il Paese Ritrovato are not publicly available according to the Italian privacy regulations. Specific information can be made available for research purposes upon inquiry.