
Abstract
Background:
Alzheimer’s disease (AD) and related dementias are progressive neurological disorders with stage-specific clinical features and challenges. An important knowledge gap is the “window of time” within which patients transition from mild cognitive impairment or mild AD to moderate or severe AD. Better characterization/establishment of transition times would help clinicians initiating treatments, including anti-amyloid therapy.
Objective:
To describe cognitive test score-based AD stage transitions in Veterans with AD in the US Veterans Affairs Healthcare System (VAHS).
Methods:
This retrospective analysis (2010–2019) identified Veterans with AD from the VAHS Electronic Health Record (EHR) notes. AD stage was based on Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), or Saint Louis University Mental Status (SLUMS) Examination scores in the EHR.
Results:
We identified 296,519 Veterans with cognitive test-based AD staging. Over the 10-year study, the proportion of veterans with MMSE scores declined from 24.9% to 9.5% while those with SLUMS rose from 9.0% to 17.8%; and MoCA rose from 5.0% to 25.4%. The average forward transition times between each stage were approximately 2–4 years, whether assessed by MMSE, MoCA, or SLUMS.
Conclusion:
The average transition time for cognitive test-based assessments of initial cognitive decline, early-stage AD, and moderate/severe AD in the VAHS is 2–4 years. In view of the short window for introducing disease-modifying therapy and the significant benefits of early treatment of AD, our data suggest a critical need for treatment guidelines in the management of AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) and related dementias are progressive neurological disorders with stage-specific clinical features and challenges. Stages of AD are commonly designated early/mild, moderate, and advanced/severe [1]. Each stage is associated with typical clinical symptoms, management challenges, goals of care, and treatment options. Clarifying a patient’s stage of AD is clinically useful for patients, families/caregivers, and clinicians for making treatment decisions and better anticipating behavioral and safety challenges. In particular, treatments for early/mild-stage AD are a major research focus [2]. The United States (US) Food and Drug Administration (FDA) has now approved two anti-amyloid treatments for patients with early stage AD (i.e., mild cognitive impairment [MCI] or mild dementia stage): aducanumab (June 2021), and, more recently, lecanemab (July 2023) [3]. Thus, the establishment of clear working definitions of AD stages and how they are clinically managed is essential.
In community practice, the severity of AD or disease progression is commonly assessed using brief cognitive testing. Several studies have generated data to support quantitative assessment and designation of MCI, ‘mild’, ‘moderate’, and ‘severe’ AD, based on test results of Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and the Saint Louis University Mental Status (SLUMS) Examination [4–8]. While these instruments may neglect psychiatric and behavioral symptoms of dementia, they represent feasible and commonly used practical assessments of dementia stages that influence clinicians’ evaluation of patients’ severity [9].
Despite of a wide disparity in early stage AD diagnoses, the recent recommendations for appropriate use of aducanumab [10] and lecanemab [11] did not specify the cut/off value differentiating “MCI” from “mild AD”. Neurologists need to consider multiple factors as they assess the potential risks (i.e., complications) associated with the use of anti-amyloid treatment versus the benefits of possibly extending the time to transition from MCI/mild AD to moderate/severe AD. There is a critical need for clear treatment guidelines and increased consideration of benefits in management of AD therapy at all stages. An important knowledge gap is the “window of time” within which patients transition from MCI or mild AD to moderate or severe AD. Better characterization/establishment of transition times would help clinicians initiating anti-amyloid treatment. This study aimed to describe cognitive test score-based AD stage transitions in Veterans with AD in the US Veterans Affairs Healthcare System (VAHS). Prolongation of these transition times would serve as a clear and measurable goal for future anti-amyloid treatment.
MATERIALS AND METHODS
Data source and extraction
A retrospective analysis was conducted, using the VA informatics and Computing Infrastructure (VINCI) database [12], specifically Text Integration Utilities (TIU)-extracted clinical notes. An initial sample of Veterans with clinical notes in the electronic health record (EHR) was extracted using Natural Language Processing (NLP) methodology with the targeted keyword “Alz*” to identify mentions of AD diagnosis; this was followed with an iterative process with application of exclusion rules using NLP to assure a relevant analysis population. The initial data extraction to identify the eligible cohort of veterans was done from fiscal year (FY) 2010 through FY2019 (FY in our analysis was based on the US government’s accounting period, extending from October 1 and through September 30 and designated by the calendar year in which it ends). Once the cohort was established, cognitive evaluations for these Veterans were extracted from their entire available electronic record.
This study conformed with the Declaration of Helsinki and was approved by the Bedford VA Healthcare System Institutional Review Board; informed consent was not required as all data were fully deidentified before access.
Cognitive test score-based definitions of disease severity
We used scores from common cognitive tests (MMSE, MoCA, and SLUMS) to define clinical stages of AD in the clinical notations for this study. AD severity staging was based on published and publicly available standard ranges/cut-offs for test scores [4–8]. The following cutoffs were applied to classify AD severity: mild AD was defined as a score of 21–24 on MMSE and 18–25 on MoCA; moderate AD was defined as a score of 13–20 on MMSE and 11–17 on MoCA; and severe AD was defined as a score of≤12 on MMSE and≤10 on MoCA. In addition, there is no consensus about the cut-off scores to define MCI [13]; based on collective clinical experience of our research clinicians, MMSE and MoCA cutoffs for MCI were defined as 25–28 and 26–28, respectively. MMSE and MoCA scores of 29 and 30 were considered normal. SLUMS scores do not differentiate dementia severity; in this analysis, “normal” was defined as a score of 27–30, mild neurocognitive disorder (MNCD) was defined as a score of 21–26 on SLUMS, and dementia was defined as a score of≤20 on SLUMS [7]. For each FY, a Veteran’s AD stage was determined using their last cognitive test score within that year.
A validation was performed by manual chart review of 100 randomly selected notes from 100 Veterans for each cognitive test. Positive predictive values (PPV) were calculated by counting the number of notes accurately describing the test scores [14]; the PPV for MMSE, MoCA, and SLUMS were found to be 89%, 94%, and 91%, respectively; additionally, interrater reliability between 2 investigators conducting the manual chart reviews was assessed with kappa statistics of 95%, 96%, and 88% respectively.
Study endpoints
The primary study endpoint was forward transition time in years between cognitive test score-based stages of AD severity using each Veteran’s first test score for a given stage available in the VAHS. Secondarily, trends in cognitive test use and scores using each Veteran’s last test result within a FY in the VAHS over the study period (FY2010–FY2019) were examined.
Statistical analysis
Descriptive statistics were used to summarize the data. Counts and percentages were used to summarize categorical variables. Means and standard deviations were used to summarize continuous variables. Transition time was measured in years between disease stages, utilizing the date of the first cognitive test score pertaining to each disease stage. Transition times were calculated for Veterans who had cognitive test scores that were at least 30 days apart and followed forward order of disease severity progression (e.g., Normal before MCI, Mild AD before Moderate AD, etc.).
RESULTS
Study sample
We identified 296,519 Veterans with 1,580,301 clinical notes containing cognitive test scores in the entirety of their available electronic records. Veterans included in the study had a mean (SD) age of 85.9 (10.9) years and were 96.3% Male, 75.0% White, and 89.6% Non-Hispanic (Supplementary Table 1). The clinical notes ranged from FY1998 to FY2023. A total of 786,315 MMSE notes/scores from 194,977 Veterans, 450,886 MoCA notes/scores from 103,803 Veterans, and 404,062 SLUMS notes/scores from 98,232 Veterans were included in the study. When limited to FY2010–FY2019, the distribution of these Veterans and their corresponding notes by cognitive test was: MMSE, 154,062 Veterans with 560,362 clinical notes; MoCA, 95,872 Veterans with 407,886 notes; and SLUMS, 89,016 Veterans with 363,254 notes. Veterans had an average of 4 notes during the 10-year study period.
Cognitive test-related trends in the VAHS
Over the 10-year study period, the proportion of Veterans with cognitive test scores from MMSE declined from 24.9% in FY2010 to 9.5% in FY2019 (Fig. 1A). In contrast, the proportion of Veterans with scores from the other cognitive tests rose from FY2010 to FY2019: the proportion with a SLUMS score rose from 9.0% to 17.8%; the proportion with a MoCA score rose most markedly from 5.0% to 25.4%. When the proportion of electronic clinical notes with scores from these cognitive tests was examined, similar trends of a decline in MMSE, but rise in SLUMS and MoCA were observed from FY2010 to FY2019 (Fig. 1B).
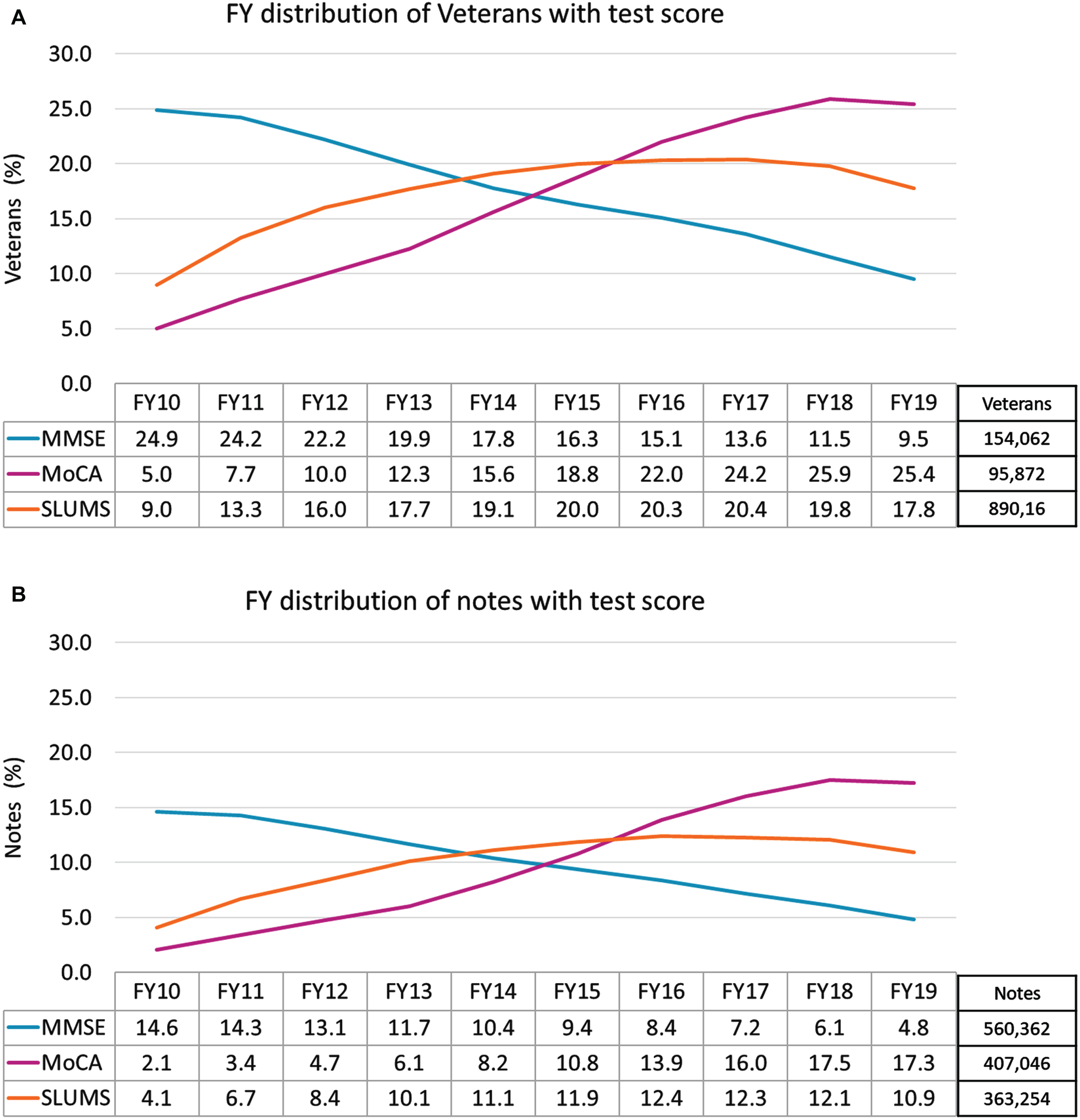
Distribution of cognitive tests over time (years) in the VAHS A) proportion of Veterans with MMSE, MoCA, or SLUMS scores; and B) proportion of notes with MMSE, MoCA, or SLUMS scores. FY, fiscal year; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment (MoCA); SLUMS, Saint Louis University Mental Status Examination; VAHS, Veterans Affairs Healthcare System.
The distribution of score-based disease staging was generally consistent over time within each cognitive test type (Fig. 2). However, the distribution of stages between test types varied. For MMSE, the distribution of mild, moderate, and severe AD was approximately 19%, 21%, and 18%, respectively in FY 10 and approximately 19%, 20%, and 23% in FY19 (Fig. 2A). For MoCA, the distribution of mild, moderate, and severe AD was approximately 42%, 27%, and 19%, respectively in FY 10 and approximately 42%, 28%, and 19% in FY19 (Fig. 2B). Notably, in each FY, the proportion of Veterans identified as having mild AD based on MoCA scores was more than double that based on MMSE scores. Although the SLUMS exam does not differentiate between dementia stages, we observed that the distribution of MNCD and dementia in SLUMS was approximately 24% and 67%, respectively in FY 10 and 26% and 64% in FY19 (Fig. 2C). The proportion of Veterans with scores in the normal range varied widely among cognitive tests: In FY19, approximately 13% of Veterans had an MMSE score≥29, 2% had a MoCA score≥29, and 11% had a SLUMS score≥27. The proportions of Veterans who had MCI based on MMSE (25–28) and MoCA (26–28) were approximately 26% and 9%, respectively in FY19 (Fig. 2).
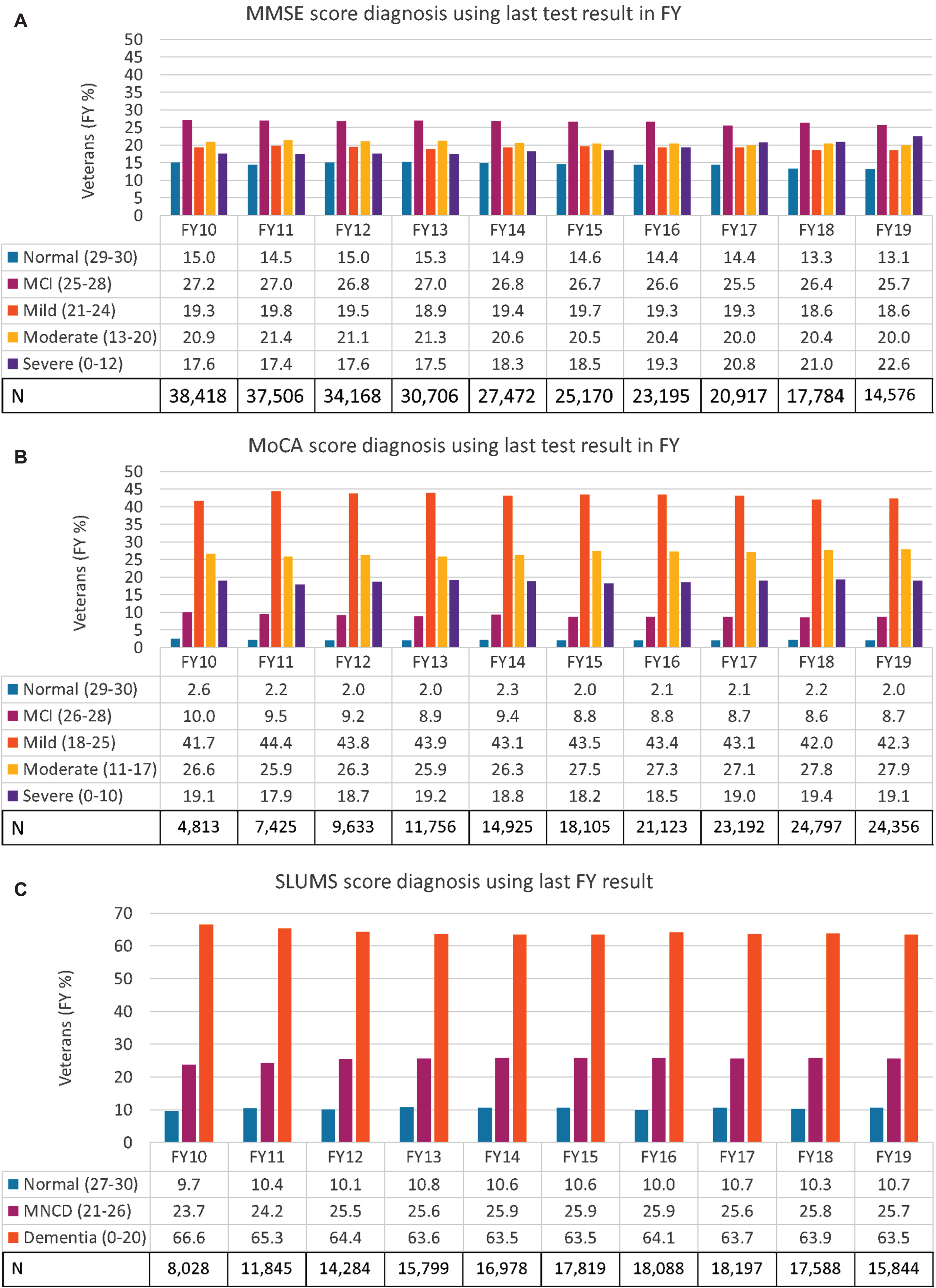
Distribution of cognitive tests score-based AD stages in Veterans over time (years) in the VAHS A) MMSE; B) MoCA; C) SLUMS. FY, fiscal year; MNCD, mild neurocognitive disorder; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; SLUMS, Saint Louis University Mental Status Examination; VAHS, Veterans Affairs Healthcare System.
Transition times between AD stages in VAHS
Half of the Veterans with any cognitive test scores recorded met the criteria for assessment of transition times (i.e., 2 scores from a given cognitive test at least 30 days apart), while just over 40% of these Veterans only had cognitive assessment documented during a single date in the EHR. Among Veterans included in the transition time analysis, the average duration of time for any of the stage-to-stage transitions assessed in our study was approximately 2 to 4 years on average (1.2 to 3.4 by median), whether assessed by MMSE, MoCA or SLUMS (Table 1 and Supplementary Table 2). The overall range of transition times was < 1 to 22 years for MMSE and < 1 to 15 years for both MoCA and SLUMS.
Transition Times Between Cognitive Test Score-Determine AD Stages in the VAHS
AD, Alzheimer’s disease; MCI, mild cognitive impairment; MNCD, mild neurocognitive disorder; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment (MoCA); SLUMS, Saint Louis University Mental Status Examination; SD, standard deviation; VAHS, Veterans Affairs Healthcare System. aBased on the first cognitive test score pertaining to each disease stage category being assessed. bVeterans with cognitive test scores that were at least 30 days apart. cCognitive test scores corresponding to “Normal” for MMSE and MoCA were 29 or 30. dCognitive test scores corresponding to “MCI” for MMSE and MoCA were 25–28 and 26–28, respectively.
The mean (SD) transition times from Normal to MCI based on MMSE was 2.8 (2.9) years (median 1.7 years) and 2.0 (1.9) years (median 1.4 years) based on MoCA; the mean (SD) transition from Normal to MNCD/MCI based on SLUMS was 2.2 (2.1) years (median 1.5 years). The mean (SD) transition time from MCI to mild AD based on MMSE was longer than that based on MoCA: 2.6 (2.5) years (median 1.8 years) and 2.1 (1.9) years (median 1.5 years), respectively. The mean (SD) transition times from mild to moderate AD were comparable for MMSE score-based assessments (2.2 [2.2] years) and MoCA score-based assessments (2.1 [1.8] years); median transition was 1.5 years for MMSE and 1.6 years for MoCA. Mean (SD) transition from moderate to severe AD was longer when based on MMSE (2.1 [2.0] years, median 1.4 years) than when based MoCA (1.6 [1.5], median 1.2 years).
Mean (SD) transition times from normal or mild AD to severe AD was longer than transition to moderate AD for both MMSE and MoCA. Normal to moderate and severe AD transition according to MMSE was 4.2 (3.3) years (median 3.4 years) and 3.6 (3.3) years (median 2.5 years), respectively. Mild AD to moderate and severe AD transition according to MMSE was comparable. Transition from MCI to moderate and severe AD according to MoCA was 2.8 (2.1) years (median 2.4 years) and 2.3 (2.1) years (median 1.7 years), respectively. Transition from normal to moderate and severe AD via MoCA were comparable.
DISCUSSION
This analysis of cognitive test scores of nearly 300,000 Veterans in the VAHS found that the average transition time from early-stage AD (mild AD) to moderate or severe AD was approximately 2 to 4 years. These data are based on the time elapsed between the first documentation of a test score indicating early AD and first documentation of a test score indicating progression to a later disease stage.
The combined duration of MCI plus early-stage dementia presents a critical window of opportunity to address risk factors, safety issues and treatment options for patients with AD. It is during this window of time, on average, that early AD can be identified and screened for potential treatment with disease modifying therapy. Prior studies have demonstrated clinical and economic benefits from anti-amyloid therapies that slow progression [15–17], emphasizing the importance of early identification and treatment of AD.
Our overall data on duration of AD stages is consistent with prior studies of AD progression. Previous studies have demonstrated an average rate of progression of approximately 3 points per year on MMSE [18]. This would imply MCI duration of around 2 years (MMSE 22–28) and mild AD duration of around 2 years (MMSE 21–24). Our measurement of MCI and mild AD is consistent with these data. Differences might be expected based on variation in testing between the VAHS and community care, differences in patient populations, or changes in testing over time. Our transition data include the available EHR that spans approximately 20 years and includes cognitive test scores for a wide variety of clinical environments within the VAHS. The good agreement between our data and prior research [18] suggests that our EHR analysis accurately reflects the rate of disease progression.
We observed longer transition, up to six months, from Normal or MCI to moderate AD compared to severe AD. We know that, by definition, the disease must progress from MCI to mild to moderate to severe AD. It is therefore biologically impossible for a cohort to progress more rapidly from mild to severe AD than from mild to moderate AD. These results may be impacted by the frequency of cognitive testing at various stages of the disease as well as provider/patient decision-making to take a test. Specifically, Veterans may decide to delay subsequent cognitive testing unless they observe a noticeable decline, hence the longer intervals between tests and the increased severity that may not follow typical staged progression (e.g., jump from mild to severe AD). Additionally, calculating transition based on the first occurrence of a test score within an AD severity range may not accurately estimate transition time. This is of particular importance when a Veteran scores around the break point between two AD severities (e.g., score around moderate and severe AD cutoff). A “stable” state that requires at least two tests within a stage could be established and/or performing a longitudinal analysis may yield a more accurate estimate of transition, but the sample size would be negatively impacted.
Our examination of trends in cognitive testing over the 10-year study period revealed a > 50% decline in the proportion of Veterans assessed by MMSE while the proportion assessed by MoCA more than quintupled over the same period. The finding that the proportion of Veterans identified as having mild AD based on MoCA scores was more than double that based on MMSE scores, is consistent with prior data suggesting that MoCA may be a more sensitive test for detecting early-stage disease [19]. Our finding that less than 50% of these Veterans had evidence of a cognitive score in their EHR with a frequency of more than once per year suggests a suboptimal cognitive assessment rate that could be related to a perceived lack of treatment options or other provider and/or healthcare system-related factors. For a condition expected to progress over 2 years, annual assessment is not sufficient to detect progression and implement treatments appropriately.
Limitations
Our method of AD severity identification relied on cognitive test scores extracted from clinical notes since mild, moderate, and severe AD staging information cannot be discerned from traditional structured data. Natural language processing enables efficient extraction of key data from large volume databases where manual chart review would not be feasible; however, there is the potential for information to be mis-identified. Nonetheless, our validation via direct chart review of a random selection of notes found approximately 90% accuracy of test scores extracted from clinical notes. While progressive decline gives the best indication of disease progression, the low frequency and temporal non-uniformity of test scores would likely be insufficient to take into considerations of baseline differences of individual MMSE and MoCA scores. Of note, assessments of later (moderate and severe) stages of dementia may be complex and difficult to measure. Cognitive instruments may be inaccurate due to ceiling effects. Further, cognitive assessments for moderate and severe AD are far less frequent in the more advanced stages of disease as they are clinically less useful. This may be due to lack of need for diagnosis, more difficulty getting patients to cooperate or even attend to testing in these advanced stages; there may also be provider and/or healthcare system-related barriers. Also, the duration of these stages of AD may depend on type and availability of care. Patients living at home may be more likely to receive anti-psychotic drugs for behavior management, due to lack of skilled non-pharmacological interventions, and they are less likely to benefit from an enriched social environment. There are also significant differences in risk of infectious disease between home-bound and institutionalized patients. It is likely that our measurements include a wide variety of clinical populations that could be distinguished by a more refined study to avoid the large range of transition times. For all these reasons, we suspect that the estimated duration of later stages of AD in this analysis may not be reliable.
Another important consideration is that transitions between stages of AD are not discrete; therefore, our transition times may be underestimated. Our study did not capture data in Veterans who used clinical services outside of the VAHS. Finally, our population of Veterans may not be generalizable to the current US population at risk for AD as the VAHS population is predominantly male and the requirements to receive VA healthcare (e.g., income restrictions and service-related disability). Nevertheless, we identify trends that are likely to be relevant to both individual patients with AD and to the diverse AD population.
CONCLUSION
In summary, our data identify a window of opportunity, based on clinical notations of objective cognitive assessments, for intervention in progression of early-stage AD. In view of the significant individual and societal benefits of early treatment of AD, our data suggest a critical need for treatment guidelines and more active involvement of subspecialty providers in the management of AD.
Footnotes
ACKNOWLEDGMENTS
The views expressed in this article are those of the authors and do not represent the views of the US Department of Veterans Affairs and the US Government. Editorial assistance and medical writing support in the preparation of this article was provided by Kulvinder Katie Singh, PharmD, of KK Singh LLC (Branchburg, NJ, USA).
FUNDING
This study was supported by Eisai Inc. and National Institute on Aging RF1 AG063913 (WX).
CONFLICT OF INTEREST
Amir Abbas Tahami Monfared, Raymond Zhang, and Quanwu Zhang are employees of Eisai, Inc. All other authors have no conflict of interest to report. The funders had no decisional role in study design, data collection and analysis, or the decision to present or publish the manuscript.
Weiming Xia is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions and government regulations. Request for accessing available data will be submitted for approval by the Department of Veterans Affairs. All data are fully de-identified before access.