
Abstract
Background:
Plasma amyloid-β (Aβ) has emerged as an important tool to detect risks of Alzheimer’s disease and related dementias, although research in diverse populations is lacking.
Objective:
We compared plasma Aβ42/40 by race with dementia risk over 15 years among Black and White older adults.
Methods:
In a prospective cohort of 997 dementia-free participants (mean age 74±2.9 years, 55% women, 54% Black), incident dementia was identified based on hospital records, medication, and neurocognitive test over 15 years. Plasma Aβ42/40 was measured at Year 2 and categorized into low, medium, and high tertile. We used linear regression to estimate mean Aβ42/40 by race and race-stratified Cox proportional hazards models to assess the association between Aβ42/40 tertile and dementia risk.
Results:
Black participants had a lower age-adjusted mean Aβ 42/40 compared to White participants, primarily among APOE ɛ4 non-carriers (Black: 0.176, White: 0.185, p = 0.035). Among Black participants, lower Aβ 42/40 was associated with increased dementia risk: 33% in low (hazard ratios [HR] = 1.77, 95% confidence interval 1.09–2.88) and 27% in medium tertile (HR = 1.67, 1.01–2.78) compared with 18% in high Aβ 42/40 tertile; Increased risks were attenuated among White participants: 21% in low (HR = 1.43, 0.81–2.53) and 23% in medium tertile (HR = 1.27, 0.68–2.36) compared with 15% in high Aβ 42/40 tertile. The interaction by race was not statistically significant.
Conclusions:
Among community-dwelling, non-demented older adults, especially APOE ɛ4 non-carriers, Black individuals had lower plasma Aβ 42/40 and demonstrated a higher dementia risk with low Aβ42/40 compared with White individuals.
INTRODUCTION
An estimated 6.5 million Americans aged 65 and older are living with Alzheimer’s disease (AD) and related dementias (ADRD) [1, 2]. The hallmark of AD pathology includes the accumulation of the amyloid-β (Aβ) plaques in the brain, which slowly begin to form many years before clinical symptoms emerge. Although cerebrospinal fluid (CSF) and PET biomarkers of Aβ are highly accurate in detecting amyloid pathology in vivo, the high cost and invasiveness limit their use in community settings [3, 4]. Plasma Aβ level has emerged as a promising biomarker of AD [5–7]. Furthermore, a lower plasma Aβ42/40 ratio has also been associated with a higher risk of mild cognitive impairment and all-cause dementia [6, 8]. With the recent Food and Drug Administration (FDA) approval of anti-amyloid drugs that may slow cognitive decline among individuals with early AD [9], using plasma Aβ to identify individuals at high risk before they develop dementia could potentially be a critical first step to ensure timely diagnosis and intervention.
ADRD disproportionately impacts Black older adults in the United States, who may be up to twice as likely to be diagnosed with ADRD compared to White older adults [2, 11]. A population-based study of non-demented elders reported that Black (versus White) older adults had greater amyloid deposition on florbetapir PET [12]. Few studies have investigated plasma Aβ markers in diverse populations, with a limited number of Black participants. While one study found differences in plasma Aβ levels by race, others did not find similar disparities [13, 14]. The study did not separate participants with and without AD, although the association between race and plasma Aβ may differ by AD diagnosis [14]. In addition, many risk factors can modulate the association between amyloid burden and cognitive outcomes, such as vascular risk factors (VRFs, including hypertension, diabetes, obesity, dyslipidemia), apolipoprotein E (APOE) ɛ4 genotype [15, 16]. These risk factors are more prevalent in Black older adults, who may also have more barriers to VRF treatment and, therefore, more uncontrolled or severe VRFs than White older adults [17–19]. The association between amyloid burden and cognitive outcomes may also be modulated by cognitive reserve that is closely intertwined with educational quality and attainment [15, 20]. Lower educational quality and attainment, which can be attributed to factors related to residential segregation and structural racism, may disproportionately affect Black older adults [21, 22]. These findings raise the question of whether the association between plasma Aβ and the risk of dementia differs by race.
In a large cohort of community-dwelling Black and White older adults without dementia, our goal was to compare the plasma Aβ42/40 by race, adjusting for potential confounders. Another goal of this study was to assess whether the association between plasma Aβ42/40 and the risk of incident dementia over 15 years differed among Black and White older adults.
METHODS
Study population
We studied participants from the Health, Aging, and Body Composition (Health ABC) study, a prospective cohort of community-dwelling Black and White participants aged 70 to 79 years at baseline (1997–1998) who lived in Memphis, Tennessee, or Pittsburgh, Pennsylvania. Participants were recruited from a random sample of Medicare-eligible adults living within the designated zip codes. Eligible older adults were those who reported no difficulties performing activities of daily living or with mobility. Participants also had to be free of life-threatening cancers and planned to remain in the study area for at least three years. Details of the Health ABC study have been described previously [23, 24].
Standard protocol approvals, registrations, and patient consents
All participants provided written informed consent. The study was approved by the institutional review boards of the University of Pittsburgh, the University of Tennessee, Memphis, the coordinating center, and the University of California, San Francisco.
Plasma amyloid-β
Among the 3,075 participants enrolled in the Health ABC study, a random sample of 997 sex- and race-stratified participants with cognitive measures at baseline and ≥1 follow-up visit had plasma Aβ42 and Aβ40 measured from stored plasma obtained at Year 2 [15]. Plasma was stored at –70°C at Fisher BioServices, Inc. Laboratories and shipped directly to the analytical laboratory at the Mayo Clinic, Jacksonville, Florida. In 2010, plasma Aβ was measured using INNO-BIA assays (Innogenetics, Ghent, Belgium). The INNO-BIA assay is a fluorometric bead-based (xMAP microspheres) immunoassay that simultaneously measures Aβ40 and Aβ42. The sample analyses used a non-simultaneous measurement approach due to a large number of samples. To ensure standardization, the lab utilized aliquots from common specimens on every plate, which allowed for plate-to-plate comparison and helped maintain consistency across the assay runs. The detection limit for this assay was 12 pg/mL for Aβ40 and 5 pg/mL for Aβ42, with mean inter-assay coefficient of variation 9.9% for Aβ40 and 9.3% for Aβ42 and mean intra-assay coefficient of variation 3.5% for Aβ40 and 2.3% for Aβ42. We categorized low (<0.159), medium (0.159–0.1939), and high (≥0.194) Aβ42/40 levels based on tertile in the overall sample, which is similar to tertile by race.
Dementia incidence
During baseline and follow-up at Years 1, 3, 5, 8, 10, and 11, participants underwent the Modified Mini-Mental Status Examination (3MS), a test that measures global cognitive function by assessing orientation, attention, praxis, language, and memory, with scores ranging from 0 to 100 [25]. Participants were interviewed every 6 months about possible hospitalizations, and hospital records would be requested if any were reported. At each annual clinic visit, participants were asked to bring their medication, which was then documented by the study staff. Incident dementia over 15 years was determined if a participant met any of the following criteria: 1) a record of hospitalization with dementia listed as a primary or secondary diagnosis, 2) a documented prescription for dementia medication, or 3) ≥1.5 standard deviations (SD) decline in 3MS from baseline to last visit compared with the mean 3MS change of the race-matched peers within the cohort [26–28]. The time to dementia incidence was calculated as the duration between baseline and the date on which a participant first met the incident dementia criteria.
Covariates
Demographic information (age and sex) and education were obtained from self-report at baseline. Race was determined by participant self-identification as either Black or White [23]. We considered baseline VRFs (hypertension, diabetes, high cholesterol, obesity, and current cigarette smoking) and comorbid conditions (stroke and myocardial infarction) determined based on self-report, physician diagnoses, medication use, and laboratory exam. Body mass index (BMI, kg/m2) was calculated from direct height and weight measured at baseline, and obesity was defined as BMI > 30. We also considered baseline behavior factors from self-report, including heavy alcohol drinking (>1 drink per day) and physical activity (total kcal expended per week walking and exercising) [29]. Depression was assessed using the 20-item Center for Epidemiologic Studies Depression (CESD) Scale, with a score of ≥16 indicating the presence of depression [30]. Serum creatinine was determined using standard techniques. Genotyping was performed at baseline and APOE was determined directly using polymerase chain reaction on coded DNA samples [31, 32]. In our analyses, APOE was categorized as ɛ4 carriers and non-carriers.
Statistical analysis
Descriptive statistics were used to compare the baseline characteristics between Black and White participants and by Aβ42/40 tertile within each race using Mann-Whitney U tests, Kruskal-Wallis tests, and Chi-Square tests as appropriate. We used linear regression to model natural log-transformed plasma Aβ42/40 by race with and without adjusting for potential confounders. The estimated marginal means for the plasma Aβ42/40 levels by race were presented by exponentiation of the natural log-transformed plasma levels (back-transformed from the log scale). We selected potential confounders a priori based on previous studies, which included demographics, behavioral and VRFs, renal function, and depression [8, 34]. Given the important role of APOE ɛ4 in Aβ metabolism and its different prevalence by race, we also adjusted for and stratified our analysis by APOE. We then conducted race-stratified analyses using Cox proportional hazards models to assess, within each race, the association between Aβ42/40 tertile and the risk of dementia with and without adjusting for the above potential confounders, education, baseline cognition, and APOE ɛ4 [8, 35], with censoring at dementia, death, or their last study visit (whichever occurred first). Additional detail on the potential confounders and effect modification in our conceptual model was included in Supplementary Figures 1 and 2. The results were reported as hazard ratios (HR) with 95% confidence intervals. We tested the interaction between race and Aβ42/40 by tertile. A p < 0.05 was considered statistically significant in all other analyses. Statistical analyses were conducted with SAS (version 9.4).
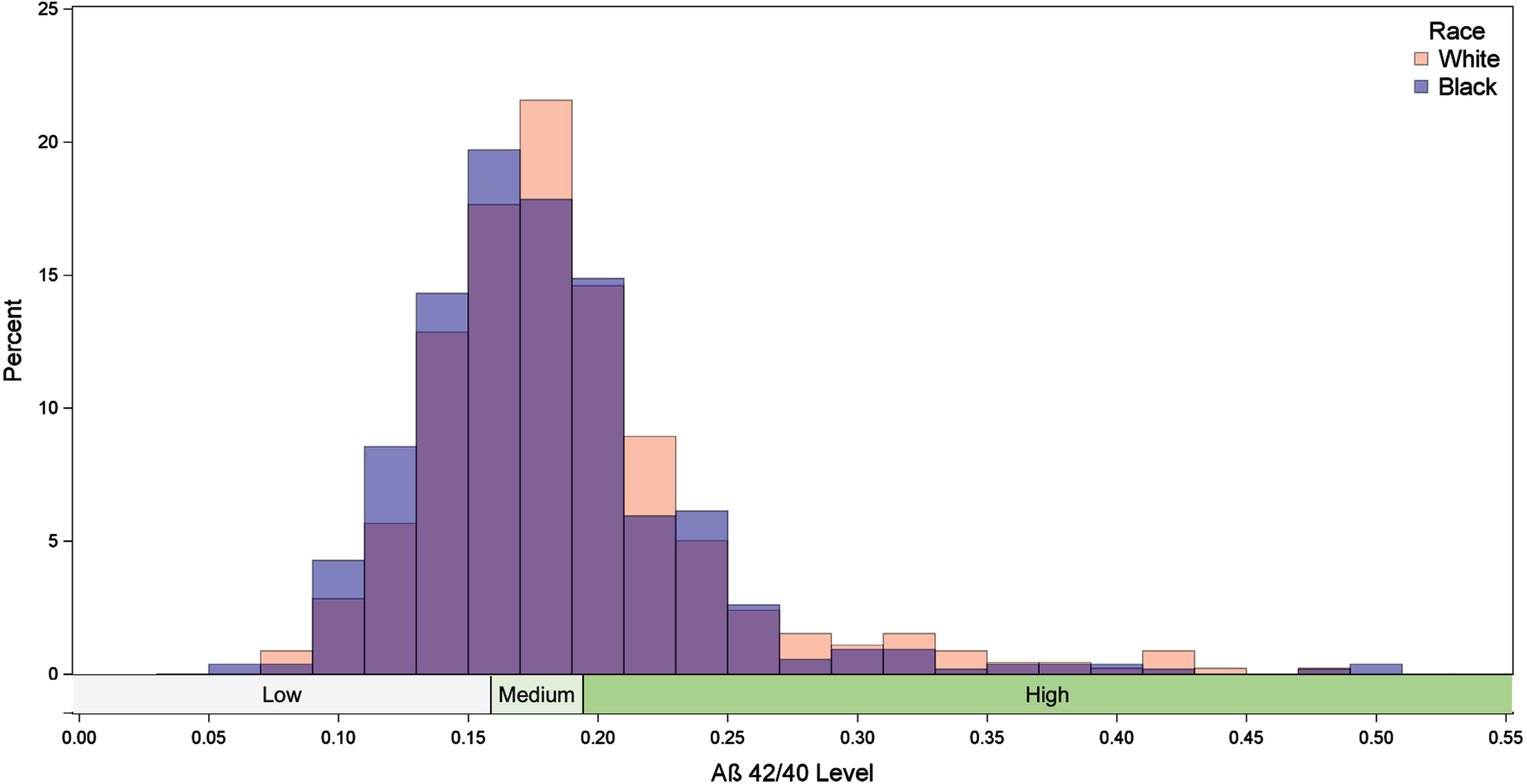
The distribution of amyloid-β (Aβ) 42/40 level by race.
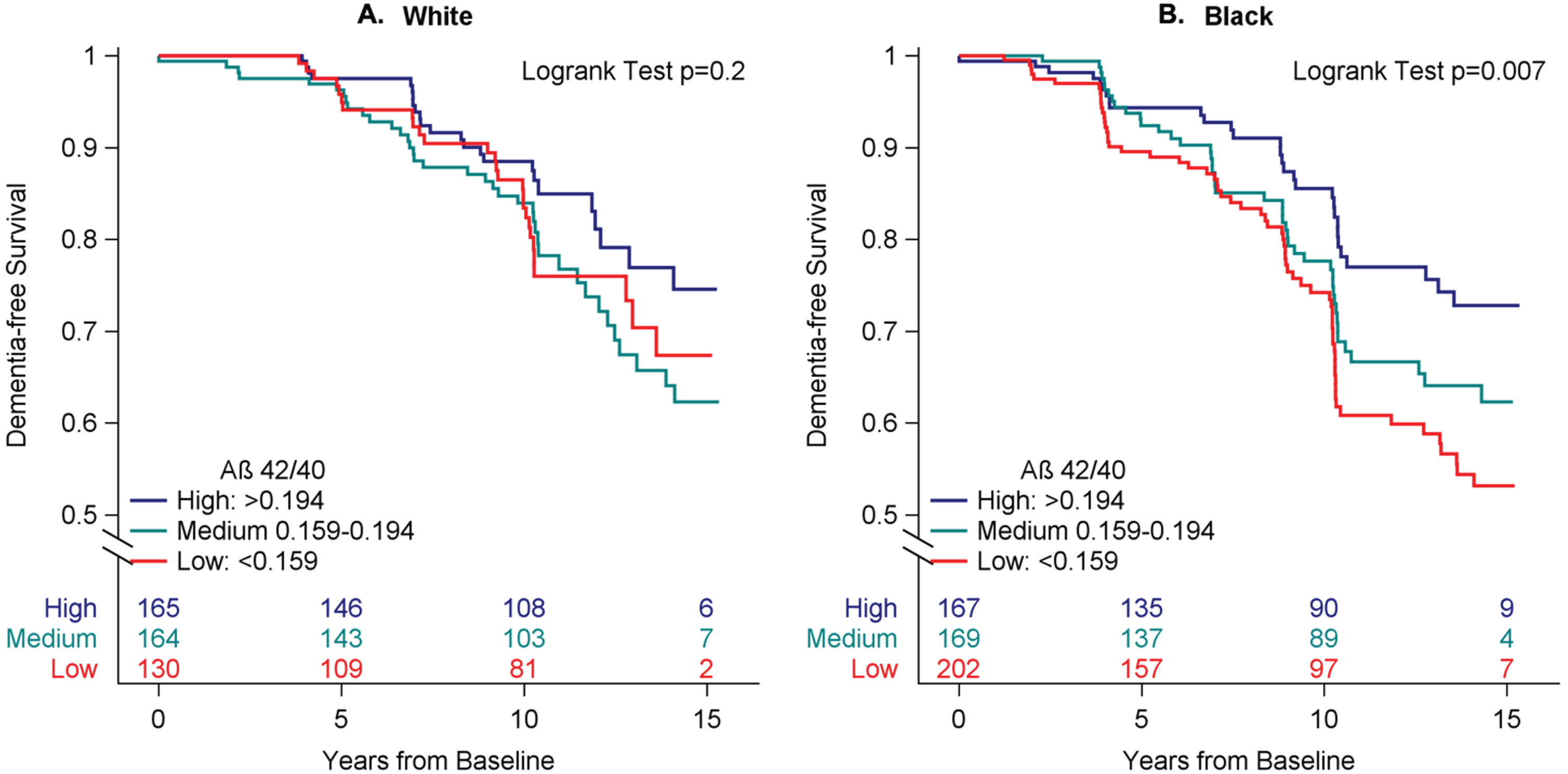
Kaplan-Meier curves of dementia-free survival by amyloid-β (Aβ) 42/40 tertile among 997 Black and White participants. Annotations denoting the number of participants at risk at 0, 5, 10, and 15 years.
RESULTS
Among the 997 participants (mean age 74±2.9 years), 538 (54%) were Black, and 550 (55%) were female. Table 1 shows the baseline characteristics of Health ABC participants by race. Compared to White participants, Black participants were more likely to be female and APOE ɛ4 carriers, drank less alcohol, had higher serum creatinine and greater VRFs, and had lower education, physical activity, and baseline 3MS score. Baseline characteristics were also compared by Aβ42/40 tertile among White and Black participants in Table 2. Those with lower Aβ42/40 levels were more likely to be APOE ɛ4 carriers.
Baseline Characteristics of the 997 Health ABC Participants by Race
SD, standard deviation; 3MS, Modified Mini-Mental State Examination. *Chi-square tests for categorical variables and Mann-Whitney U tests for continuous variables. Number of participants with missing information: APOE 58 (6%), cholesterol 36 (4%), myocardial infarction 15 (2%), stroke 12 (1%), depression 10 (1%).
Baseline characteristics by Aβ42/40 tertile in the 997 black and white participants
Aβ, amyloid-β; SD, standard deviation; 3MS, Modified Mini-Mental State Examination. *Chi-square test for categorical variables and Kruskal-Wallis tests for continuous variables. Participants with missing information: APOE 58 (6%), cholesterol 36 (4%), myocardial infarction 15 (2%), Stroke 12 (1%), Depression 10 (1%).
Race disparities in Aβ
The overall mean of plasma Aβ42/40 level was 0.186 (standard deviation [SD] = 0.07). The distribution of Aβ42/40 was right-skewed and had a heavier left tail for Black participants compared to White participants (Fig. 1). Table 3 shows the unadjusted and adjusted marginal mean of plasma Aβ42/40 by race. Compared with White participants, Black participants had slightly lower age-adjusted Aβ42/40 (White, mean = 0.181, 95% CI 0.176–0.186; Black, mean = 0.174, 95% CI 0.17–0.178), and this difference remained after adjusting for APOE ɛ4 (White, mean = 0.179, 95% CI 0.174–0.184; Black, mean = 0.172, 95% CI 0.168–0.177). After stratifying by APOE, the age-adjusted difference in Aβ42/40 by race was significant only among APOE ɛ4 non-carriers (White, mean = 0.185, 95% CI 0.179–0.191; Black, mean = 0.176, 95% CI 0.171–0.182), but not among APOE ɛ4 carriers (White, mean = 0.172, 95% CI 0.163–0.182; Black 0.169, 95% CI 0.161–0.176). The results were not attenuated after additional adjustment for sex, vascular and behavioral risk factors, serum creatinine, and depression.
Comparing Estimated Mean Amyloid-β 42/40 Level by Race
LS Means, Least Squares Means of amyloid-β 42/40 level; CL, confidence interval; *Multivariable-adjusted model adjusted for age, sex, APOE ɛ4 (except stratified-models), vascular and behavioral risk factors, serum creatinine, and depression.
Aβ42/40 and incident dementia in Black and White older adults
After up to 15 years of follow-up (mean follow-up of 9.7±3.8 years), 230 (23.1%) participants developed incident dementia, which occurred in 19.4% of White (N = 89) and 26.2% of Black (N = 141) participants. The proportion of participants meeting the specific criteria for incident dementia is included in Supplementary Table 1. Black participants had slightly lower proportions of dementia hospitalization and medication use but a greater proportion of having ≥1.5 SD decline in 3MS compared to White participants.
Among all participants, after adjusting for demographics, education, behavioral and VRFs, serum creatinine, depression, and baseline 3MS score, lower Aβ42/40 was associated with an increased risk of dementia (28% in low [HR 1.72, 95% CI 1.21–2.44] and 25% in medium Aβ42/40 tertile [HR 1.52, 95% CI 1.06–2.18] compared with 16% in high Aβ42/40 tertile). The association was attenuated but remained significant after additional adjustment for APOE ɛ4: low versus high tertile (HR 1.46, 95% CI 1.01–2.11) and medium versus high tertile (HR 1.45, 95% CI 1.0–2.1). The Kaplan-Meier curves in Fig. 2 demonstrate differences in dementia risk between high and low Aβ42/40 tertile among Black and White participants.
In race-stratified analysis, lower Aβ42/40 was associated with an increased risk of dementia among Black participants (33% in low [HR 1.77, 95% CI 1.09–2.88] and 27% in medium Aβ42/40 tertile [HR 1.67, 95% CI 1.01–2.78] compared with 18% in high Aβ42/40 tertile). The association among White participants was weaker but in the same direction (21% in low [HR 1.43, 95% CI 0.81–2.53] and 23% in medium Aβ42/40 tertile [HR 1.27, 95% CI 0.68–2.36] compared with 15% in high Aβ42/40 tertile). The interaction between Aβ42/40 tertile and race did not reach statistical significance (interaction p = 0.21).
DISCUSSION
In a large prospective cohort of dementia-free adults aged 70–79, we found that Black older adults have lower age-adjusted plasma Aβ42/40 than White older adults. The higher prevalence of APOE ɛ4 carriers among Black older adults did not explain much of the disparity in plasma Aβ42/40, which was primarily driven by the Aβ42/40 difference among APOE ɛ4 non-carriers. Furthermore, demographics, vascular and behavioral risk factors, renal function, and depression did not explain the difference in Aβ42/40 by race. Interestingly, the association between lower plasma Aβ42/40 and dementia risk over 15 years was found to be stronger among Black older adults.
Despite the recent advances in research on plasma AD biomarkers, including Aβ42/40, significant gaps remain in the study of plasma Aβ and the association with incident dementia among diverse communities. Prior reports regarding Aβ42/40 levels in Black and White adults are conflicting. Results from the Washington Heights-Inwood Columbia Aging Project (WHICAP) found that Aβ42/40 level did not differ among 113 autopsied and 300 clinically evaluated Black, White, and Hispanic participants with and without AD, but the study may have had limited power [14]. Among a diverse cohort of 1,428 participants (mean age 63–69, 10% Black) from the Health and Aging Brain Study-Health Disparities (HABS-HD), higher Aβ42/40 was reported for Black compared to White older adults [13]. Heterogeneity in age and sample size, especially for Black participants, and the inclusion of participants with AD may contribute to the discrepancies in findings compared to ours. Previous studies comparing Aβ42/40 across racial groups are also limited by the lack of adjustment for age and APOE ɛ4, two important factors of plasma Aβ that are likely to vary by race [36].
We found evidence of a racial disparity in plasma Aβ42/40 between Black and White older adults without dementia, which aligned with the prior study on Florbetapir PET Aβ burden among non-demented older adults in the Atherosclerosis Risk in Communities - Neurocognitive Study (ARIC-NCS) [12]. Our finding on the racial difference in plasma Aβ42/40 existing primarily among the APOE ɛ4 non-carriers is novel and has important implications for the underlying mechanisms contributing to the racial disparity in dementia risk. Despite an observed stronger association between lower Aβ42/40 and dementia risk in Black than White participants, the interaction did not meet statistical significance. This finding is similar to that from the ARIC study, which showed that the associations between late-life plasma Aβ measures and cognitive outcomes did not differ by race [8].
The mechanisms for disparities in plasma and brain Aβ deposition are unclear. APOE ɛ4, a genetic risk factor of AD with an important role in Aβ metabolism, is more prevalent in Black than White individuals, but most studies showed that the association between APOE ɛ4 and dementia risk is weaker in Black than in White older adults [37–39]. Our findings suggest that differences in APOE ɛ4 prevalence did not appear to be the major factor, and the Aβ difference by race may be primarily driven by differences in Black and White older adults among APOE ɛ4 non-carriers. While we did not find that VRF or other comorbidities explained the difference in plasma Aβ42/40 by race, it is possible that disproportionate exposure to long-term VRF burden by race, which can start from midlife, may still contribute to this disparity. In addition, the possibility that differential social and structural factors by race may contribute to the disparity of Aβ42/40 by race invites future studies in diverse communities [40, 41].
Although the difference in plasma Aβ42/40 by race was statistically significant in our study, it is important to note that the mean difference was small. Nonetheless, previous studies have demonstrated similarly small but significant differences in mean plasma Aβ42/40 between amyloid PET negative and positive individuals [42], suggesting that even subtle variations in Aβ42/40 ratios may indicate differences in underlying brain amyloidosis. The potential disparities in amyloid pathology between Black and White older adults may contribute to the disparities in dementia risk by race, particularly when combined with other risk factors, such as VRFs, which have a disproportional impact on different racial groups [16]. In addition, although we adjusted for baseline cognitive function, unaccounted differences in pathologies and brain aging at baseline may still play a role in the observed differences by race, which invites future studies.
Despite the fact that the interaction between race and Aβ42/40 in association with the risk of dementia was not significant, we had limited power. Nevertheless, our findings suggest that Black older adults may be at a higher risk for dementia compared to White older adults with similar plasma Aβ levels. Emerging evidence now supports the notion that plasma Aβ42/40 is a sensitive early indicator of dementia risk, preceding amyloid PET [43]. Further research is necessary to better understand the potential benefits of utilizing plasma Aβ42/40 as a screening tool for early detection in different racial groups, with the goal of lessening racial disparities in dementia risk.
Our study has a number of strengths, including the prospective study design with up to 15 years of follow-up for incident dementia. Plasma biomarkers have now emerged as inexpensive and minimally invasive tools to predict AD risk, and we measured plasma Aβ in a community-based cohort with a large number of Black older adults. This study fills the gap in understanding the racial disparity in plasma Aβ and the association with dementia risk among non-demented Black and White older adults. We were able to control for numerous potential confounders, including those that were included in previous studies. There are some limitations to our study. Dementia diagnosis used in our study is likely less accurate than the diagnosis using comprehensive clinical evaluation, but the misclassification of dementia diagnosis should not differ by Aβ42/40 tertile. We also did not have information on the etiology of dementia. We used Innogenetic INNO-BIA assays, an immunoassay-based method, to quantify plasma Aβ in a community-based cohort, similar to the ARIC study and the Framingham Heart Study [8, 35]. However, the precision of immunoassay-based methods may not be as sensitive as those obtained by newer mass spectrometry-based methods, such as the immunoprecipitation-mass spectrometry (IP-MS) [44]. Ongoing investigations using more precise assays (e.g., Simoa) to evaluate racial or ethnic differences in plasma Aβ42/40 are underway [13]. Future studies employing newer and more precise methods are warranted to confirm our findings. The long-term stability of plasma Aβ when frozen for up to 10 years remains to be determined and merits thorough evaluation [45]. Unmeasured confounding from sociocultural and structural factors, VRFs earlier in life, and other comorbid conditions may also contribute to the racial differences in plasma Aβ42/40. Although we have a large study sample, we may still be underpowered to detect an interaction by race in the association between Aβ42/40 and dementia risk, the confirmation of which may require a larger study.
In conclusion, non-demented, community-dwelling older Black adults have lower plasma Aβ42/40 levels than White adults, particularly among APOE ɛ4 non-carriers. Additionally, lower Aβ42/40 levels are associated with a higher risk of dementia over 15 years, with a stronger association seen among Black participants. These findings suggest a potential explanation for the existing disparity in dementia risk among Black and White older adults and highlight a need for further research on the underlying mechanism of Aβ disparity by race.
AUTHOR CONTRIBUTIONS
Xiaqing Jiang (Conceptualization; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Amber L. Bahorik (Formal analysis; Methodology; Writing – review & editing); Neill R. Graff-Radford (Data curation; Writing – review & editing); Kristine Yaffe (Conceptualization; Data curation; Funding acquisition; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The Health, Aging, and Body Composition Study was supported by NIA Contracts N01-AG-6-2101; N01-AG-6-2103; N01-AG-6-2106; NIA grant R01-AG028050, and National Institute of Nursing Research grant R01-NR012459. This research was funded in part by the Intramural Research Program of the NIH, NIA.
FUNDING
This work was supported by the National Institute on Aging (NIA) at the National Institutes of Health (NIH) R35AG071916 and T32AG049663.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.