
Abstract
Background:
Transcranial alternating current stimulation (tACS) could improve cognition in patients with Alzheimer’s disease (AD). However, the effects of tACS on brain activity remain unclear.
Objective:
The purpose is to investigate the change in regional neuronal activity after tACS in AD patients employing resting-state functional magnetic resonance imaging (rs-fMRI).
Methods:
A total of 46 patients with mild AD were enrolled. Each patient received 30 one-hour sessions of real or sham tACS for three weeks (clinical trial: NCT03920826). The fractional amplitude of low-frequency fluctuations (fALFF) and the regional homogeneity (ReHo) measured by rs-fMRI were calculated to evaluate the regional brain activity.
Results:
Compared to baseline, AD patients in the real group exhibited increased fALFF in the left middle frontal gyrus-orbital part and right inferior frontal gyrus-orbital part, as well as increased ReHo in the left precentral gyrus and right middle frontal gyrus at the end of intervention. At the 3-month follow-up, fALFF increased in the left superior parietal lobule and right inferior temporal gyrus, as well as ReHo, in the left middle frontal gyrus and right superior medial frontal gyrus. A higher fALFF in the right lingual gyrus and ReHo in the right parahippocampal gyrus were observed in the response group than in the nonresponse group.
Conclusions:
The findings demonstrated the beneficial effects of tACS on the neuronal activity of the prefrontal cortex and even more extensive regions and provided a neuroimaging biomarker of treatment response in AD patients.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia worldwide, but until recently, efficient strategies to slow or prevent clinical cognitive progression were poorly understood. 1 It is anticipated that the worldwide prevalence of dementia due to all causes will rise from 50 million cases in 2010 to 113 million cases by 2050. 2 The prototypical patients with AD exhibit progressive cognitive deficits in working memory, language, executive function, and even more cognitive function. 2 AD involves a prolonged clinical phase during which amyloid-β (Aβ) and tau protein clump together, causing various degrees of structural and functional alterations in the brain that lead to measurable cognitive impairment. 3 Although the present outcomes of pharmaceutical therapy are encouraging, great challenges remain in the treatment and management of AD. Assessment in brain activity may potentially help to shed light on the pathophysiological processes that underlieAD. 4
Transcranial alternating current stimulation (tACS) is a prevalent and non-pharmacological approach to improving symptoms in multiple cognitive domains in AD patients. 5 A small but growing number of studies have shown that tACS with multiple sessions has the potential for therapeutic benefit in episodic memory and language function impacted by AD.6,7, 6,7 Through an entrainment mechanism, tACS modulates endogenous cortical oscillations that apply sinusoidal alternating current with a specific frequency to target brain functional regions utilizing electrodes attached to the scalp, and then regulates and improves brain communication.8,9, 8,9 Evidence of tACS-induced cognitive improvements in AD patients is particularly associated with gamma stimulation, a special frequency range with significant involvement in hippocampal-mediated memory processes that is typically impaired in the early stages of the disease.10,11, 10,11 While the noninvasiveness of tACS is a methodological benefit in clinical settings, it brings difficulties for cognition-related research projects seeking to comprehend tACS mechanisms at an optimal level that can only be attained through animal trails or human brain imaging. 12 A previous study provided direct evidence that tACS procedures could deliver electrical currents to deep brain tissues, paving the way for the modulation or treatment of neuropsychiatric disorders associated with hippocampus, insula, and amygdala. 13 Clinical evidence has demonstrated 40 Hz tACS effectively improved short-term memory and verbal learning performance in patients with AD. 7 Modulating gamma neuronal activity with 40 Hz stimulation is a novel non-pharmacological approach to treat AD patients. 14 Twice-daily 15 mA tACS was expected to become a unique protocol for rapid physical neuromodulation. 15 In clinical practice, improvements in cognitive function, behavioral symptoms, and even reduction of pathological proteins in AD patients after tACS often benefit from repetitive brain stimulation. 6 The cumulative effects over time between changes in neuronal activity and received tACS should be taken into account. 16 Most previous studies have shown that transcranial electrical stimulation with the duration from two to four weeks could effectively improve cognitive impairment and balance neuronal activity in AD patients.17,18, 17,18 Accounting for the cumulative effects of multiple sessions and the tolerance for prolonged hospital stays, we opted for 30 sessions over 15 days as the treatment period. Therefore, the twice-daily sessions for three weeks were chosen for safety and efficacy. However, the cumulative effects of repetitive tACS with multi-session remain largely unknown, and there is still a need to characterize the long-term benefits of stimulation.
Resting-state functional magnetic resonance imaging (rs-fMRI) is a viable option for assessing regional brain function effectively and without complex experimental designs and procedures, making it easily applicable to patients with neuropsychiatric disorders. 19 Specifically, the fractional amplitude of low-frequency fluctuation (fALFF), a measure assumed to capture regional spontaneous neuronal activity, has been demonstrated to correlate with local brain glucose metabolism.20,21, 20,21 The alteration in fALFF is helpful in elucidating the physiology of AD from a neuroimaging point of view, revealing intrinsic disturbance of the network, and serving as an accurate marker of AD-related neurodegeneration. 22 Regional homogeneity (ReHo) was proposed as another measure that can effectively evaluate resting-state brain activity. 23 ReHo is introduced to reflect the regional homogeneity of neural activity between adjacent voxels. Some previous studies have reported that the prefrontal cortex, hippocampus, posterior cingulate cortex, precuneus, and temporal lobe were among the primary cognition-related regions that have been identified and recognized as being implicated in the pathophysiology of AD.24,25, 24,25 These two voxel-based measures provide distinct perspectives on neurological features and demonstrate a progressive relationship that enhances the sensitivity of identifying regional abnormalities. Generally, patients with AD showed extensive abnormal alterations in fALFF and ReHo values. 26 However, no consensus has been reached on alterations of these indexes and their relationship with cognitive performance changesin AD.
To date, a few relevant studies have examined the changes in regional brain activity after short-term tACS treatment in AD patients. However, randomized clinical trials employing rs-fMRI to explore the effect of tACS in the cognitive intervention of AD are still insufficient. Moreover, the evaluation of limited sample sizes has led to inconsistent conclusions. Therefore, we proposed the hypothesis that the cognitive performance of AD patients could be improved after tACS, and there may be a relationship between the relief in cognitive symptoms and the alteration of regional brain activity.
MATERIALS AND METHODS
Procedure
A randomized, double-blind, placebo-controlled, parallel-group, and 3-week study was conducted and included two groups: a real group and a sham group. The study has been registered in advance (NCT03920826, Registration date: April 19, 2019) and approved by the Ethics Committee at Xuanwu Hospital, Capital Medical University. Outcomes were assessed at baseline, at the end of the 3-week intervention, and at the 3-month follow-up.
Participants and eligibility criteria
We recruited patients with mild AD between September 2019 to April 2022 from Xuanwu Hospital, Capital Medical University, China. All included patients provided written informed consent. The inclusion criteria were as follows: 1) age range of 45–75 years, right-handed, Chinese origin; 2) a minimum of 6 years of education was necessary; 3) diagnostic criteria were according to the National Institute on Aging and the Alzheimer’s Association (NIA-AA) guidelines; 27 4) the initial score on the clinical dementia rating was 1.0; 5) reduced levels of cerebrospinal fluid or positive findings from positron emission tomography for Aβ; 6) a cholinesterase inhibitor (e.g., rivastigmine, donepezil) at a set dosage was administered consistently for at least 6 weeks, and the dosage was maintained fixed across the intervention and follow-up. The exclusion criteria were as follows: 1) other neurological diseases (e.g., stroke, hemorrhage, tumor) and other serious illnesses of the body that might impact cognitive function, either present or past; 2) other types of neurodegenerative diseases (e.g., Parkinson’s disease, frontotemporal dementia); 3) severe psychiatric disorders (e.g., anxiety, depression); 4) patients who exhibited contraindications for MRI and tACS; 5) aberrant state of the brain as determined by structural MRI; 6) patients who could not complete cognitive tests due to vision or hearing impairments.
tACS intervention
A previous study from our research center has indicated that twice-daily 15mA tACS, a unique form of noninvasive brain stimulation, offers an acute effective intervention. 15 Due to the refractory nature of AD, we hypothesized that more sessions of tACS may effectively treat AD. Accounting for the cumulative effects of multiple sessions and the tolerance for prolonged hospital stays, we opted for 30 sessions over 15 days as the treatment period. Each patient received real or sham tACS intervention with 30 one-hour sessions during 3 consecutive weeks using the tACS stimulator (Nexalin ADI). Three electrodes were applied to the predefined scalp: one electrode placed over the forehead and two electrodes placed over the mastoid areas. A 15 mA current level with a gamma frequency of 40 Hz was applied in the real group. Patients in the sham group were addressed using a sham specific stimulator, which has the same appearance as real stimulus machines and there was no active current flow through the cerebral cortex. The remaining treatment parameters were the same in the two groups. The participants could not discern whether the stimulator was real based on its appearance or patients’ feelings.
Neuropsychological tests
Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog), Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), World Health Organization-University of California Los Angeles (WHO-UCLA) Auditory Verbal Learning Test (AVLT), Trail Making Test (TMT), and Boston Naming Test (BNT) were employed to evaluate cognitive function. Assessors and patients were blinded to group assignments.
Imaging acquisition
Imaging data was acquired using a 3.0 T MR scanner (GE, Premier). The rs-fMRI data were obtained using an echo planar imaging sequence sensitive to BOLD contrast (repetition time = 2000 ms, echotime = 30 ms, flip angle = 90°, matrix size = 64×64, resolution of axial slice = 3.0×3.0 mm2, slice thickness = 3 mm, 240 time points. Sagittal three-dimensional magnetization prepared rapid gradient echo (3DMPRAGE) sequence was used to obtain T1-weighted images.
Imaging preprocessing
The data was processed using Data Processing Assistant for Resting-State fMRI (DPARSF 4.5, https://www.nitrc.org/projects/dparsf) with the following steps: 1) conversing format and removing the first 10 time points; 2) slice timing; 3) head motion correction; 4) spatial normalization to the Montreal Neurological Institute space; 5) spatial smoothing with a 8 mm full-width half-maximum Gaussian filter; 6) eliminating the linear trend of the time course; 7) regression of head motion effect, gray matter, white matter, and cerebrospinal fluid signals; and 8) bandpass filtering (0.01 ∼ 0.08 Hz). Participants with head motion > 2 mm or rotation > 2° were excluded.
fALFF calculation
After data preprocessing, the time course of each voxel was transformed into the frequency domain using a fast Fourier transform and the power spectrum was subsequently obtained. The square root was calculated at each frequency of the power spectrum, and the average square root was obtained as the ALFF value between 0.01 and 0.08 Hz for each voxel, which was divided by the global mean ALFF value of each patient. Finally, the ratio between the ALFF and the power spectrum of the entire frequency range was calculated to obtain the fALFF measurements. For the purpose of standardization, the fALFF maps were obtained through the fALFF of each voxel divided by the global mean fALFF value.
ReHo calculation
A single ReHo map was generated by calculating the Kendall’s coefficient of concordance of the time series of a given voxel and its nearest neighbor (26 voxels) in a voxel-wise way. For standardization, the ReHo value of every voxel was divided by the global mean ReHo of each individual. The spatial smoothing was conducted after the ReHo calculation.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science version (SPSS 24.0). Between-group comparisons were tested by t test for age, education, and neuropsychological scores, while χ 2 test was used for sex. Linear mixed-effects models for repeated-measures data were used to examine the effects of tACS on neuropsychological scores over time with a random effect for patients.
Statistical Parametric Mapping (SPM 12.0, http://www.fil.ion.ucl.ac.uk/spm) was employed to analyze rs-fMRI data based on a generalized linear model. fALFF and ReHo maps were compared at baseline and after treatment, respectively. The gaussian random field (GRF) was applied to correct for multiple comparisons with significance set at voxel-level p value < 0.01, cluster-level p value < 0.05, and cluster size > 10. Pearson correlation was calculated to measure the association between the mean fALFF and ReHo values and neuropsychological scores. Additionally, in order to further evaluate whether the changes in brain function activity were related to efficacy, AD patients in the real group were divided into the response and nonresponse groups based on ADAS-Cog. A reduction of 4-score was used as the judgment standard for clinical efficacy. 28 The changes in fALFF and ReHo between the two groups before and after treatment were compared.
RESULTS
Demographics
A total of 46 patients with mild AD were included in the analysis (Fig. 1). No significant difference in age, sex, and education was observed between the real group and the sham group (p > 0.05)(Table 1).
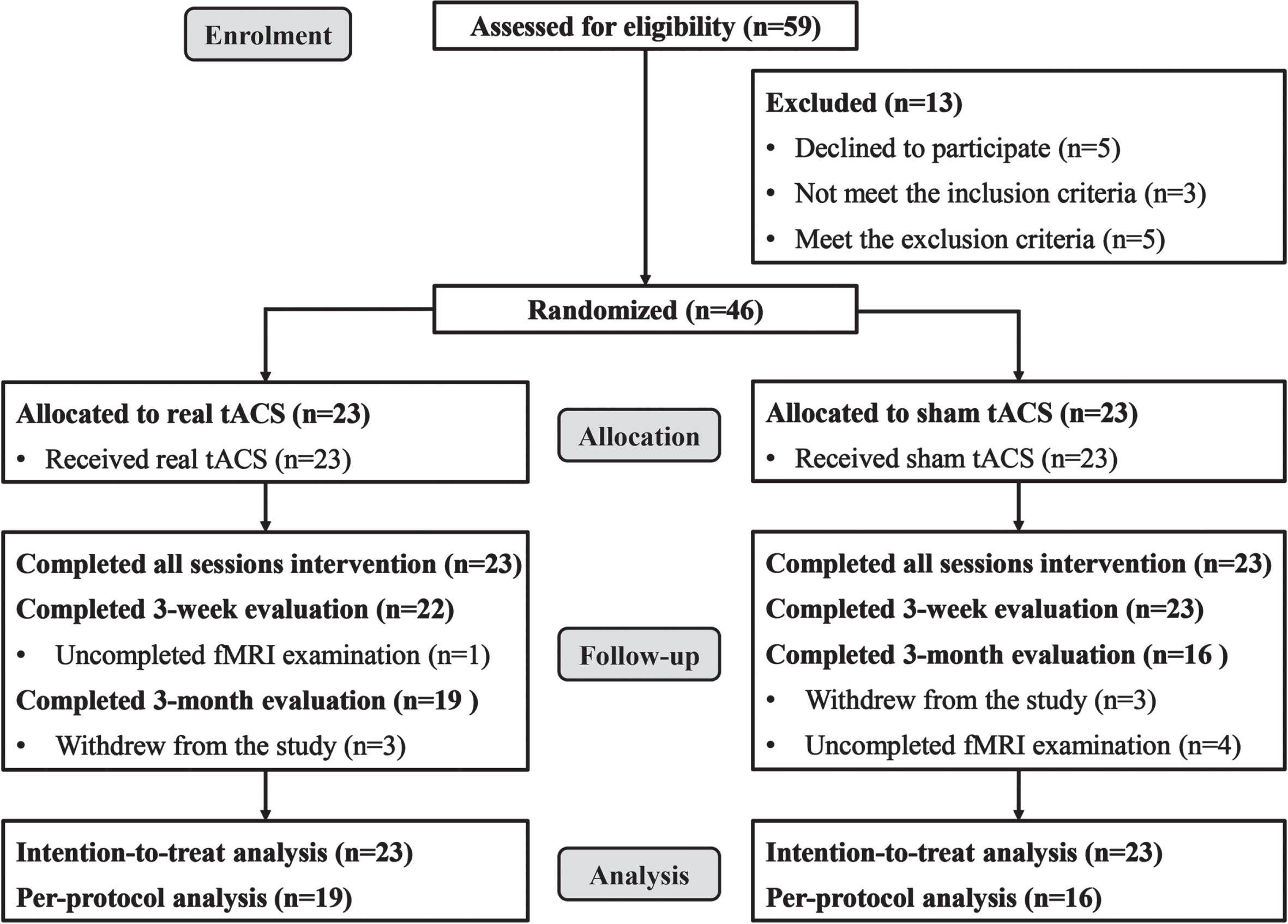
CONSORT diagram of study flow.
Sample Characteristics at Baseline
Frequency and percentage are provided for categorical variables; mean and standard deviation are provided for continuous variables. χ 2 test was used for sex and two sample t test for age and education.
Neuropsychological assessment
No difference was found between the real group and the sham group at baseline (p > 0.05). There was a significant group (real versus sham)×time (baseline versus after tACS) interaction effect in MMSE, MoCA, and AVLT at the end of intervention (p < 0.05), while there was no significant difference at the 3-month follow-up (p > 0.05) (Supplementary Table 1).
Changes in fALFF
AD patients in the real group showed increased fALFF in the left middle frontal gyrus-orbital part and right inferior frontal gyrus-orbital part at the end of intervention, and in the left superior parietal lobule and right inferior temporal gyrus at the 3-month follow-up. Conversely, fALFF was decreased in the right thalamus at the end of intervention, and in the right inferior frontal gyrus-pars opercularis and left middle cingulate gyrus at the 3-month follow-up in the sham group (Fig. 2, Supplementary Table 2).
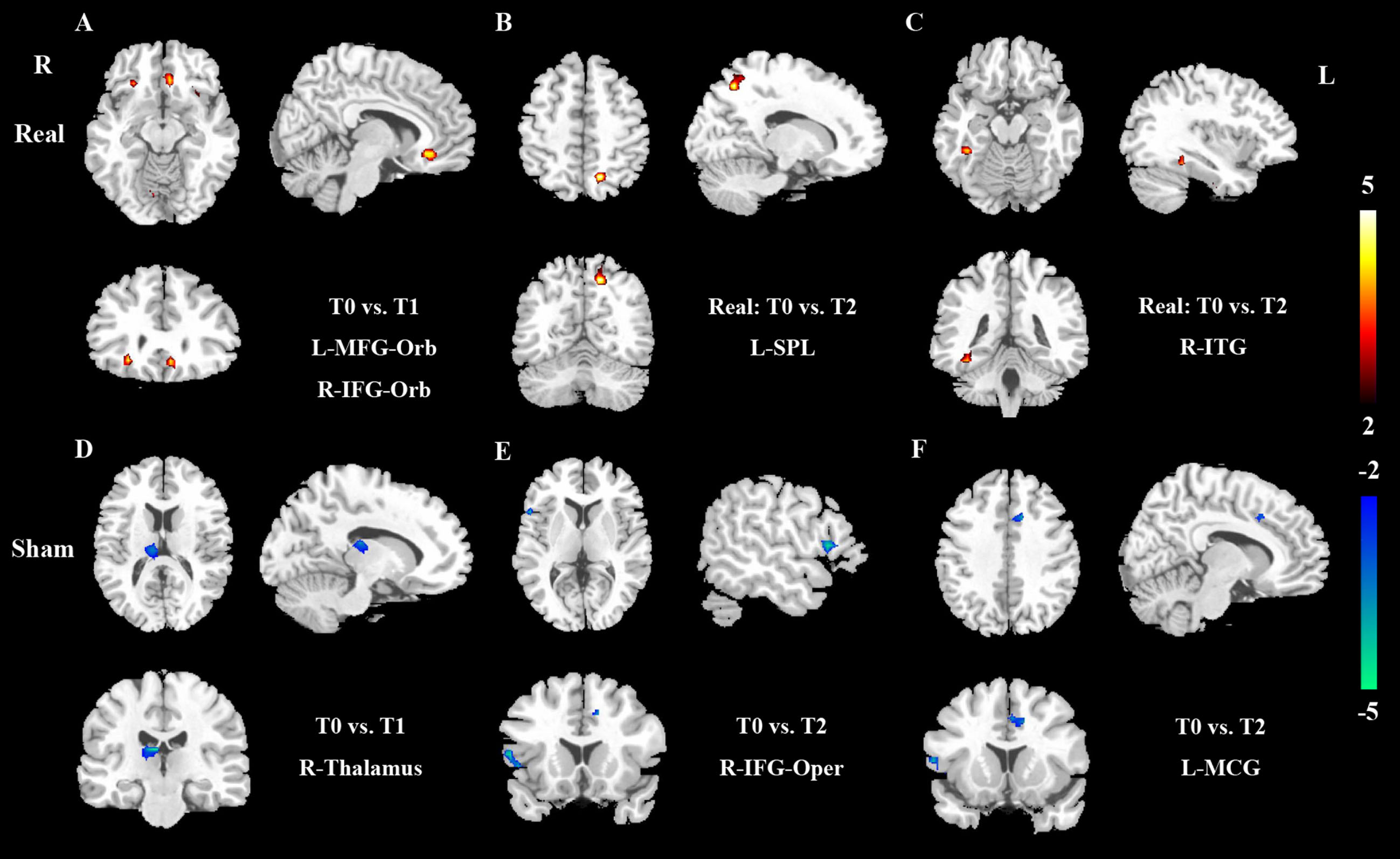
Changes in fractional amplitude of low-frequency fluctuation after intervention in the real group (A–C) and sham group (D–F). Warm colors represent increases, while cool colors represent decreases; T0, baseline; T1, immediately after treatment; T2, 3-month follow-up; L, left; R, right; MFG-Orb, middle frontal gyrus-orbital part; IFG-Orb, inferior frontal gyrus-orbital part; SPL, superior parietal lobule; ITG, inferior temporal gyrus; IFG-Oper, inferior frontal gyrus-pars opercularis; MCG, middle cingulate gyrus.
Changes in ReHo
Following 3 weeks of intervention, ReHo increased in the left precentral gyrus and right middle frontal gyrus in the real group. At the 3-month follow-up, the patients exhibited higher ReHo in the left middle frontal gyrus and right superior medial frontal gyrus. In contrast, there was a decreased ReHo in the left superior medial frontal gyrus at the end of intervention and in the right superior frontal gyrus-orbital part at the 3-month follow-up (Fig. 3, Supplementary Table 3).
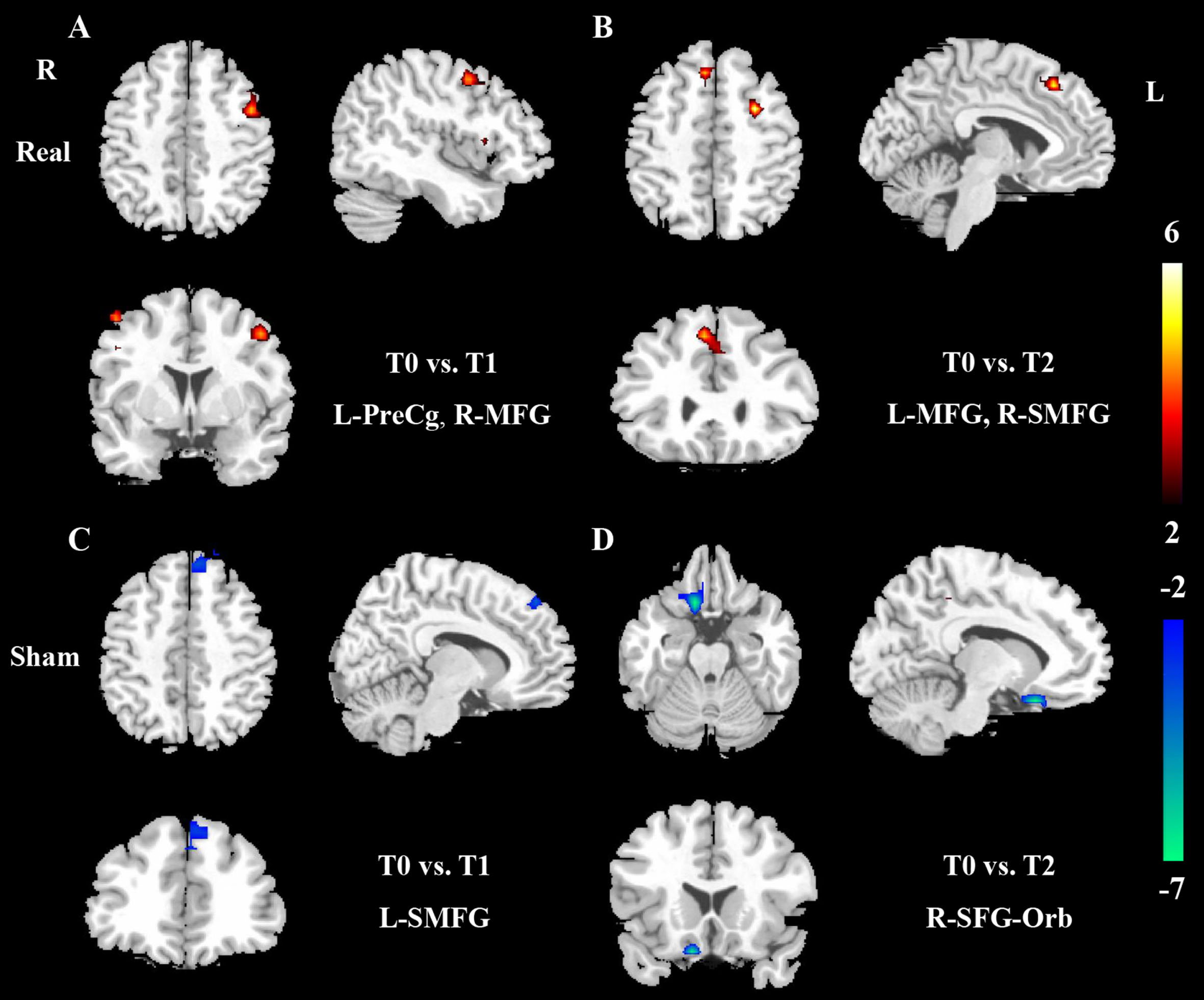
Changes in regional homogeneity after intervention in the real group (A, B) and sham group (C, D). Warm colors represent increases, while cool colors represent decreases; T0, baseline; T1, immediately after treatment; T2, 3-month follow-up; L, left; R, right; PreCg, precentral gyrus; MFG, middle frontal gyrus; SMFG, superior medial frontal gyrus; SFG-Orb, superior frontal gyrus-orbital part.
Correlation analysis
No significant correlation was observed between the change of rs-fMRI (fALFF and ReHo) and neuropsychological scores at the end of intervention. However, the increased fALFF in the left superior parietal lobule at the 3-month follow-up was significantly and positively related to the increased MoCA (r = 0.603, p = 0.006) (Fig. 4A). There was a significant positive correlation between the change of ReHo in the left middle frontal gyrus and the increase of AVLT-immediate recall at the 3-month follow-up (r = 0.594, p = 0.007) (Fig. 4B).
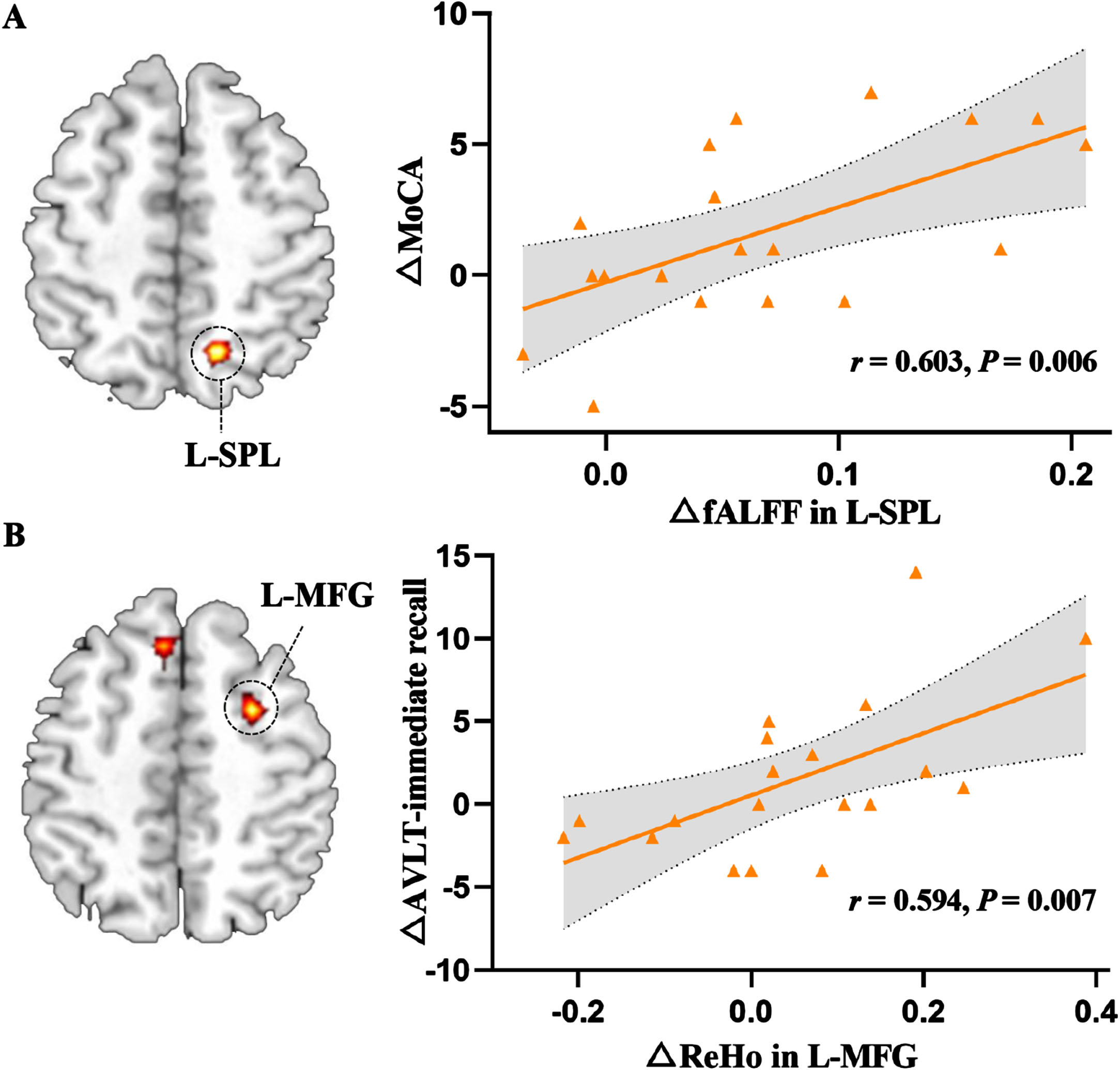
Correlation between the change of fALFF in L-SPL and MoCA (A), and between the change of ReHo in L-MFG and AVLT-immediate recall (B) at the 3-month follow-up after intervention. MoCA, Montreal Cognitive Assessment; fALFF, fractional amplitude of low-frequency fluctuation; L, left; SPL, superior parietal lobule; AVLT, Auditory Verbal Learning Test; ReHo, regional homogeneity; MFG, middle frontal gyrus.
Differences between the response and nonresponse group
The patients in the real group were divided into the response (n = 9, 40.91%) and nonresponse (n = 13, 59.09%) group. No significant changes were found in fALFF and ReHo between the two groups before treatment. Compared with the nonresponse group, increased fALFF in the right lingual gyrus (cluster size = 61, t = 5.37) and ReHo in the right parahippocampal gyrus (cluster size = 117, t = 4.49) after intervention were observed in the response group (Fig. 5).
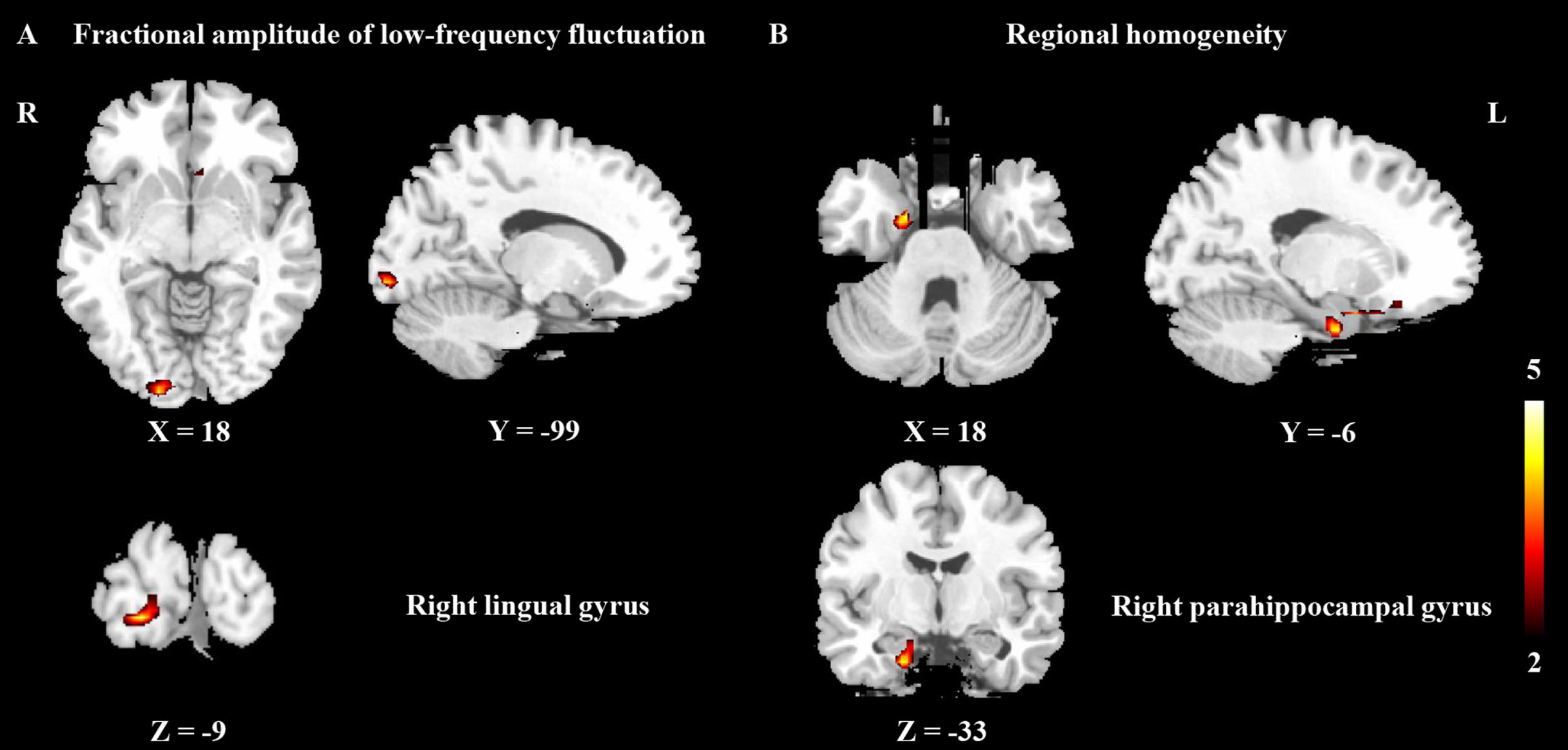
The differences between the response group and nonresponse group after intervention. Warm colors represent increases, while cool colors represent decreases; L, left; R, right.
Safety
During the course of the study, one patient in the real group reported a tingling sensation during the first two sessions, while another in the sham group reported transient itching at the first session. No serious adverse events were observed in either group. There was also no side-effect related injury on structural MRI.
DISCUSSION
In this study, we reported that 40 Hz tACS could effectively improve cognitive impairment in patients with mild AD. Although the effect size of improvement in cognitive scores retracted at the 3-month follow-up, the change of fALFF and ReHo in the real group after tACS was encouraging. We observed a marked increase in neuronal activity of the prefrontal cortex in the real group at the end of the intervention, and the beneficial effect after tACS extended to temporal and parietal regions at the 3-month follow-up. Furthermore, our study provided some evidence that the increased fALFF in the right lingual gyrus and ReHo in the right parahippocampal gyrus may serve as a neuroimaging predictor for the treatment response of tACS in AD patients.
In our study, the frontal lobe was revealed to be the primary brain area where alterations in regional neural activity were noticed after tACS treatment. The frontal lobe is crucial for cognitive control and emotion processing.29,30, 29,30 AD is frequently accompanied by pathologic alteration and dysfunction in the frontal lobe, which is identifiable at the onset of the disease. 31 For the treatment of AD patients, noninvasive brain stimulation frequently targets the frontal lobe, either directly or indirectly.17,32,33, 17,32,33 Three premade electrodes were placed on the individual’s scalp with the current passing through the frontal cortex, so that tACS with specific frequencies could selectively correct neural oscillations in the target area to achieve cognitive improvement in AD patients. Increased fALFF was observed in the left middle frontal gyrus-orbital part and right inferior frontal gyrus-orbital part at the end of the intervention in the real group in this study. Previous clinical research has also demonstrated the benefits of increased neuronal activity in the frontal lobe for the restoration of cognitive impairment, albeit with various intervention modalities.34–37 Part of the prefrontal cortex, the orbitofrontal cortex is primarily engaged in cognitive function, and individuals rely on the orbitofrontal cortex to make decisions and avoid risks.38,39, 38,39 Support for relevant cognitive activity has been revealed in previous research on the orbitofrontal cortex, which serves as a cognitive map of pertinent environmental states.40,41, 40,41 An animal experiment has shown that the orbitofrontal cortex and hippocampus share striking cognitive and functional similarities. 42
In a further 3-month follow-up study, we found that significantly increased fALFF was mainly located in the left superior parietal lobule and right inferior temporal gyrus. Longitudinally, the modulatory effect of tACS on the frontal lobe was reduced, but it seemed to extend to farther-off parietal and temporal regions. The left superior parietal lobule, an important component of the left frontoparietal network, plays a key role in cognitive and behavioral control in AD. 43 Prior research has noted that significantly severe hypoperfusion and decreased brain activity were observed in the lateral parietal lobe of AD patients, especially in the left superior parietal lobule.44,45, 44,45 This finding provided evidence that AD pathogenesis may be linked to hypoperfusion in the left superior parietal lobule. Additionally, correlation analysis in our study showed that the change of fALFF in the superior parietal lobule was significantly and positively related to the increased score in MoCA. It supported the idea that activation of the left superior parietal lobule implied better global cognitive function after tACS. Although MoCA score retracted at 3-month follow-up after tACS, it showed an increasing trend compared with baseline. On the other hand, the changes in regional neuronal activity and clinical cognitive scores after the intervention were not completely matched to some extent. Therefore, it is insufficient to evaluate efficacy just based on cognitive scores in the clinical management of AD. Consistent with our findings, prior studies have reported that hyperactivation in the superior parietal lobule could potentially reflect protective brain plasticity in individuals with AD. 46 Moreover, the activation in the right inferior temporal gyrus after tACS intervention is also worth considering. The findings are in line with an earlier investigation. 47 Lower brain activity in the inferior temporal gyrus, a crucial brain region involved in memory, auditory cognition, and semantics, could be affected soon after the onset of AD and observed in AD patients when compared to normal controls.48,49, 48,49
Remarkably, in our study, ReHo significantly increased after tACS in multiple regions, including the left precentral gyrus, bilateral middle frontal gyrus, and right superior medial frontal gyrus. The findings also corroborated the modulation of tACS on neuronal activity in the prefrontal cortex. The precentral gyrus, a cortical motor region located in the frontal lobe responsible for voluntary movement control, predominantly receives proprioceptive input from the contralateral skeletal muscles and joints. The precentral gyrus is essential for clear communication and has been identified to participate in language and memory function. 50 The enhanced neuronal activity observed in the precentral gyrus of individuals with AD has been recognized as a positive modulatory mechanism to attenuate memory impairment associated with AD.51,52, 51,52 Our study revealed a spatial shift in the ReHo effect of tACS on the middle frontal gyrus, transitioning from the right to the left hemisphere. The middle frontal gyrus, located mainly in the lateral prefrontal cortex, is an essential component of the executive control network and is associated with episodic memory and emotional processing.53,54, 53,54 A decreased ReHo in the middle frontal gyrus has been reported in patients with amnestic mild cognitive impairment, a prodromal stage of AD.55,56, 55,56 Consequently, the increase in ReHo after tACS intervention indicated an enhancement in regional spontaneous neural activity, which was advantageous for mitigating cognitive decline. This finding also accords with earlier observations. 18
Correlation analysis in our study indicated a positive association between enhanced ReHo in the middle frontal gyrus and improved memory function. There were also some differences between the pattern of change in ReHo and cognitive scores after tACS. Meanwhile, there has been evidence of aberrant brain activity in the medial frontal cortex in AD patients, which is associated with executive function.49,57, 49,57 Atrophy and hypometabolism in the medial frontal cortex contribute to behavioral abnormalities in AD.58,59, 58,59 A prior study confirmed that patients with multi-domain amnestic mild cognitive impairment had decreased activation in the right superior medial frontal when performing an encoding task. 60 It was presumed that the improved cognitive performance after tACS observed in our study may be attributed to enhanced neural activity in the right superior medial frontal cortex.
Some decreased fALFF and ReHo brain regions were observed after intervention in the sham group, which indicated worsened cognitive function without effective intervention. Another observation was that patients in the response group showed higher fALFF in the right lingual gyrus and ReHo in the right parahippocampal gyrus than those in the nonresponse group. Increased neuronal activity in the lingual gyrus may help to enhance cognitive function in AD patients, based on previous studies.61,62, 61,62 However, current investigations were unable to reach a consensus on whether AD patients exhibit increased or decreased activity in the parahippocampal gyrus compared with that in normal control subjects. 63 Therefore, the clinical effect caused by increased ReHo in the parahippocampal gyrus remains uncertain.
The neurophysiological mechanisms underlying tACS are still not well understood but deserve attention. Neurophysiological effects of tACS could alter brain oscillatory power, frequency, and phase connections to modulate the neuronal activity and influence behavioral processes and cognitive performance, enabling therapeutic applications in AD.12,64,65, 12,64,65 The aforementioned cognitive benefits were supported by rs-fMRI alterations observed after 40 Hz tACS stimulation in AD patients, may resulting from entrainment of gamma frequency. 7 Actually, beyond reestablishing neural plasticity, tACS might enhance cortical oscillation synchronization.66,67, 66,67 A previous study on animals has shown that tACS serves as a noninvasive method for neuronal rehabilitation by ameliorating abnormal gamma oscillation in the hippocampal-prefrontal circuit. 68 In addition, tACS with gamma frequency could restore cholinergic transmission, increase blood perfusion, and even reduce Aβ and tau burden in AD patients.7,69,70, 7,69,70
To sum up, employed for the therapeutic effect evaluation of tACS, rs-fMRI provided accurate and impartial neuroimaging evidence, which subsequently aided neurological specialists in precisely identifying and localizing alterations in brain activity related to the therapy and management of AD. On the other hand, rs-fMRI could reveal the differences in the therapeutic response of AD patients after tACS, which could be beneficial in the subsequent individualized and precise localization of stimulation targets. Therefore, it is necessary to fully consider changes in functional imaging during AD clinical practice and therapeutic response evaluation.
There are some limitations. First, the sample size was relatively small and inadequate for stratified analysis. In the future, we will conduct randomized controlled trials with larger samples and more centers to enhance the accuracy and robustness of the research results. Potential variables (e.g., age, sex, duration of disease) impacting the therapy response will be considered. Second, more analyses of follow-up information were limited by insufficient follow-up time. Given that AD is a neurodegenerative disease that progresses slowly with a lengthy course, longer-term follow-up (e.g., from three to five years) is required for further study. Long-term follow-up will help to better understand and validate the efficacy response of tACS. Third, only one stimulation protocol was selected in this study for the treatment of AD based on earlier research. For short-term or long-term cognitive interventions, optimal protocols in AD clinical practice remain unknown. Optimal and individualized stimulation protocols should be the focus in the future AD research, even although multiple intervention options have been demonstrated to be effective. Fourth, evaluation of pathological protein alterations before and after tACS is lacking. The effects of tACS treatment on Aβ plaque reductions in the brain measured by PET will be evaluated further in the near future on the going clinical studies.
Conclusion
Our fMRI findings indicated that tACS may be an appropriate and effective therapeutic strategy for AD patients. The enhancement in cognitive performance may be attributed to modifications in the neuronal activity of the prefrontal cortex. It advanced understanding of the efficacy response to tACS and increased confidence in nonpharmacologic therapies in AD patients. Future studies can utilize PET to explore the longitudinally altered patterns of glucose metabolism and pathological protein in the cerebral cortex of AD patients after tACS.
AUTHOR CONTRIBUTIONS
Tao Wang (Conceptualization; Data curation; Methodology; Software; Writing – original draft); Shaozhen Yan (Data curation; Methodology; Software; Writing – original draft); Yi Shan (Data curation; Formal analysis; Methodology; Software); Yi Xing (Data curation; Methodology; Resources); Sheng Bi (Data curation; Methodology; Software); Zhigeng Chen (Data curation; Formal analysis; Software); Hanyu Xi (Formal analysis; Investigation; Methodology); Hanxiao Xue (Methodology); Zhigang Qi (Formal analysis; Investigation; Methodology; Validation); Yi Tang (Investigation; Methodology; Resources; Supervision; Writing – review & editing); Jie Lu (Conceptualization; Funding acquisition; Investigation; Methodology; Supervision; Validation; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This study was supported by the National Key Research and Development Program of China (No. 2022YFC2406900 and No. 2022YFC2406904), and National Natural Science Foundation of China (No. 62333002).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article.