
Abstract
Background:
Assessment of motor symptoms in Huntington’s disease (HD) is based on the Unified-HD-Rating-Scale-Total-Motor-Score (UHDRS-TMS). Its categorical and rater-dependent nature reduces the ability to detect subtle changes and often placebo effects have been observed in trials. We have previously shown that impairments in isometric force matching can be detected by quantitative motor (Q-Motor) assessments of tongue protrusion forces (glossomotography) in HD.
Objective:
We aimed to investigate whether similar impairments in isometric force matching can be detected in tasks assessing hand and foot force coordination and whether correlations with clinical measures and the disease burden score can be found.
Methods:
Using a pre-calibrated force transducer, the ability of subjects to generate and maintain isometric forces at different target levels displayed on a monitor was assessed. Target forces applied in the hand were 1.5 and 5 Newton [N] and in feet 1, 5, and 10 N. Subjects with HD (n = 31) and age-matched controls (n = 22) were recruited from the HD out-patient clinic.
Results:
All paradigms distinguished controls from HD. The static coefficient of variability (%) was the most robust measure across all matching tasks. Correlations with clinical measures, such as the UHDRS-TMS, TFC, and the DBS were found.
Conclusions:
Assessment of hand and foot force matching tasks was feasible and provided quantitative objective measures for severity of motor phenotype in HD. Since both upper and lower extremity motor function are relevant for everyday activities, these measures should be further assessed as candidates for developing functionally meaningful quantitative motor tasks.
INTRODUCTION
Huntington’s disease (HD) is a hereditary, autosomal-dominant neurodegenerative disorder resulting in motor, behavioral, cognitive and psychiatric impairments [1, 2]. Progression of motor symptoms is a well-recognized feature of HD [3] with known impacts on global and functional measures [4]. Besides the involuntary choreatic movements [5, 6], the clinical hallmark of HD, deficits of voluntary motor control are a well-recognized features of HD [7]. While no disease modifying therapy is established in HD, symptomatic therapies are available for chorea [8–10] and behavioral symptoms [11], albeit often with limited efficacy and side effects. Thus, motor symptoms remain a target of several new therapeutic approaches and could serve also as endpoint to assess progression of HD in clinical trials [12, 13].
The most commonly used measure to assess the severity and progression of motor symptoms in HD is the Unified-Huntington’s-Disease-Rating-Scale-Total-Motor-Score (UHDRS-TMS) [14]. The UHDRS-TMS is a categorical clinical scale assessing a wide range of motor symptoms (31 sub-items covering, e.g., eye movements, hand function, dystonia, chorea, gait and balance) ranging from 0 to 124 points (not to most severely affected). Although a high degree of internal consistency was suggested [15], the UHDRS remains a subjective measure with intra- and interrater variability, errors and limited sensitivity due to its categorical nature [16]. In spite of a globally applied online training and certification for raters in clinical trials [16], recent trials still revealed relevant variability and sizeable placebo effects in the UHDRS-TMS [17].
In contrast, novel quantitative motor (Q-Motor) measures exhibited less variability, higher sensitivity and no placebo effects compared to the UHDRS-TMS, e.g., in a trial with the mGlu5-receptor antagonist AFQ056 (sponsored by Novartis) [17], and two large multinational clinical trial with the dopamine-receptor antagonist pridopidine (PRIDE-HD – sponsored by Teva) and the pd10a-inhibitor PF-02545920 (AMARYLLIS – sponsored by Pfizer) [18]. The higher sensitivity may be explained by the rater-independent standardization across sites and the quantitative quality of the measures [16]. Guided by these results, we decided to explore further quantitative motor measures, which may supplement the assessments established so far [16] and assist in future clinical developments in HD and possibly other movement disorders [13].
We previously established a Q-Motor task assessing the ability of HD patients to match a force displayed on a monitor by protruding their tongue on a force transducer for defined periods (glossomotography) [19]. Tongue force variability was increased in symptomatic and even in premanifest HD gene carriers compared to controls; correlation was seen with the UHDRS-TMS, the disease burden score (DBS, based on the subjects CAG repeat size and age) [19] and with volumetric changes in caudate volume [20]. Similar observations were seen in patients with multiple sclerosis in correlation to a clinical score (EDSS) and disease burden as assessed by changes in brain diffusion tensor imaging [21]. The task has been successfully applied in HD in multicenter settings in a clinical trial [17] and in the biomarker study TRACK-HD, where is detected deficits in premanifest HD gene carriers [22] and progression of motor deficits in symptomatic HD patients [3, 23]. The variability of tongue motor output in HD is known clinically as “motor impersistency” and underlying the clinical phenomena called “chameleon-tongue”.
A similar clinical sign in HD, the “milkmaid’s grip”, i.e., the varying intensity of grip strength during a handshake, has also been detected by a Q-Motor assessment of grasping and lifting an object (manumotography) [7, 24]. Variability of isometric grip forces was increased in premanifest and symptomatic HD gene carriers and deficits in symptomatic HD progressed over time [3, 25]. Similarly, deficits in Q-Motor finger tapping measures (digitomotography) exhibited higher tap variability [26]. These motor deficits in the upper extremity were complemented by impairments found in the lower extremity, which were depicted by increased variability in the coordination of posture [27] and gait [28, 29], eventually resulting in falls and loss of mobility [30]. In summary, both upper and lower extremity motor symptoms contribute to relevant loss in every day function in HD [2].
The sensitivity of quantitative motor assessments in previous studies supports the development and exploration of novel tasks that might be easily applicable in the clinic and linked to relevant functional limitations in HD patients. Therefore, this study investigated, whether assessing force variability in the upper and lower extremities under well-controlled conditions, using target force reproduction tasks similar to those applied in glossomotography, allows to detect motor deficits in subjects with HD in hands and feet. In addition, we assessed whether these deficits correlate to the severity of HD as assessed by 1) the UHDRS-TMS, measures of function such as 2) the UHDRS Total Functional Capacity (TFC), 3) the UHDRS Functional Assessment Scale (UHDRS-FA) and 4) the Disease Burden Score (DBS).
METHODS AND SUBJECTS
Subjects
We included 31 symptomatic subjects with HD (18 male and 13 female participants, mean age 47.2±12.5 years). 29 of the patients had genetically confirmed HD, the other two had a diagnostic confidence level of 4 and a positive family history for HD. Four patients were left-handed and 27 right-handed. Twelve patients received small doses of neuroleptic medication, specifically tiapride [4], sulpiride [5] tiapride and sulpiride [1], and amisulpride [1]. Other neurological diseases or orthopedic conditions potentially interacting with the motor assessment were excluded. The control group consisted of 22 age matched subjects without neurological conditions (9 males and 13 females, mean age 43.9±12.3 years), 5 left-handed and 17 right-handed.
All HD subjects were clinically assessed by a physician well-experienced in HD, who conducted all UHDRS assessments. The study was approved by the Institutional Review Board of the University of Muenster and all subjects gave their informed consent in accordance with the declaration of Helsinki. Subjects were naïve regarding the aims of the study.
Methods
A pre-calibrated and temperature controlled force transducer (Mini40, ATI Automation, Apex, NC, USA) was used for both the hand and foot force matching tasks [16]. A monitor providing visual feedback was placed on a table in front of the subjects. The force exerted on the force transducer was displayed on the monitor as a moving red line scaled to vertically display levels of force. Subjects were asked to match a pre-defined target force, which was displayed as a straight black line on the monitor. The target force had to be matched as exact as possible for 20 seconds. Each trial was initiated and terminated by a cueing tone. Analysis of all measures was conducted within a 15-second “static-phase” starting 5 seconds after initiation of the trial to avoid variability in the initial force generation and matching period. Every subject performed a practice trial in each condition before recording started. Five trials were completed in each condition. Data was recorded, stored and analyzed using the WINSC/WINZOOM software (Department of Physiology, University of Umeå, Sweden) on a laboratory computer. Analysis was performed automated after visual quality control of each trial.
Hand force matching task
The hand matching task was performed using the grip device previously used for assessing grip forces and their variability (manumotography) during grasping and lifting an object [7, 24]. The force transducer was mounted vertically onto the grip device on the side of the thumb – see Fig. 1A. Subjects were instructed to sit comfortably upright on a chair, resting their hand on the edge of the table in front of them. In order to achieve well-controlled conditions and, e.g., avoid interference from object movements, the grip device was firmly fixed on the surface of the experimentation table in front of the subject within easy reach. The subjects were instructed to use the precision grip (i.e., thumb and index finger) to grasp the object and were not allowed to rest the elbow on the table. Two target force levels, 1.5N and 5N, were assessed. The task was performed with the non-dominant hand as previous data suggested higher sensitivity of quantitative motor tasks in HD in the non-dominant hand [7, 26].
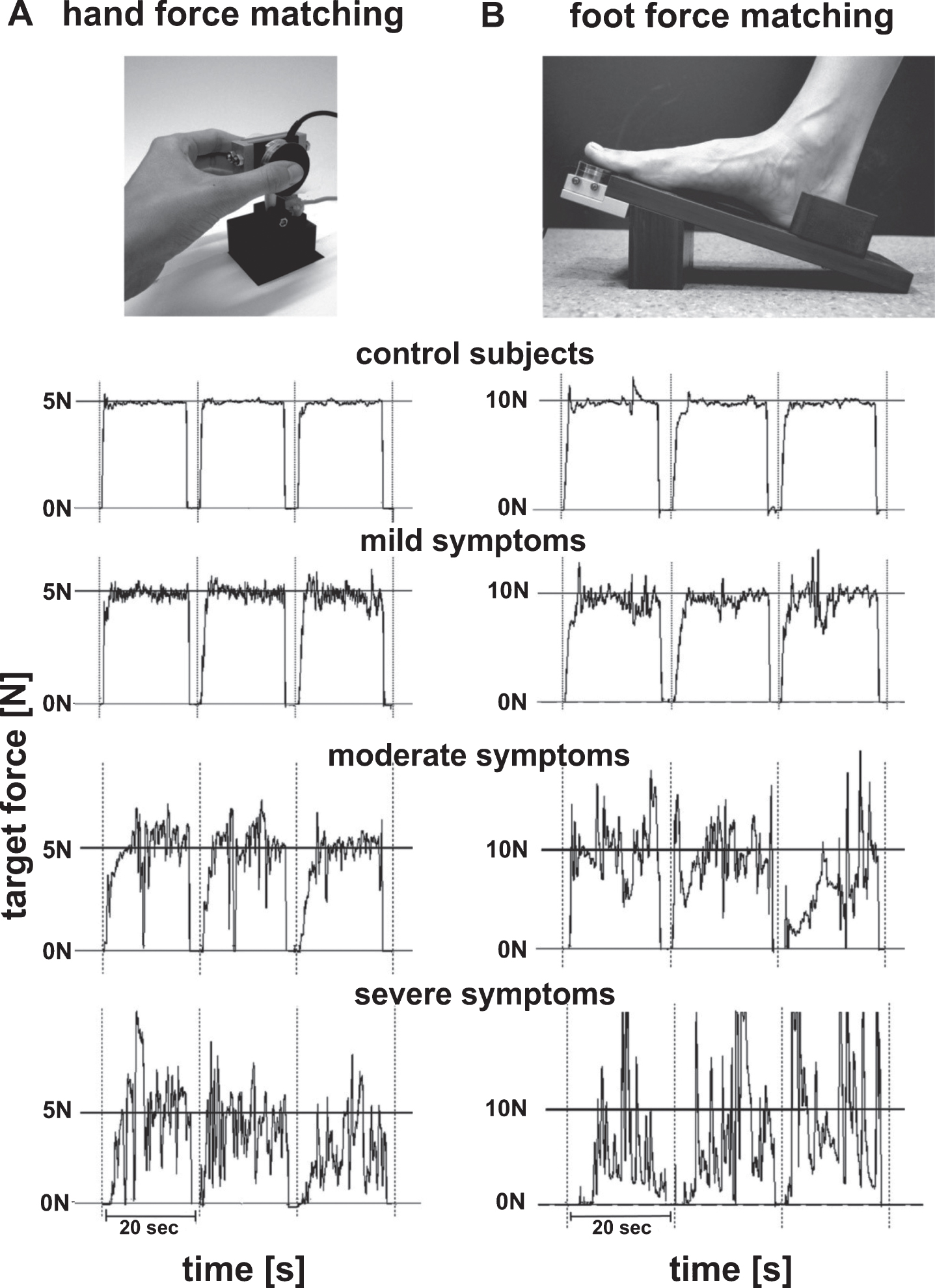
Experimental setup and sample curves. Setup of hand force matching device and foot force matching device. Representative recordings of a control subject and patients with mild, moderate, and severe impairments performing the 1.5 hand force matching task [A – left] and the 10N foot force matching task [B – right]. Note: although the last sample curve was not displayed fully, all ranges of measures were captured and used in the analysis.
Foot force matching task
For the foot matching tasks, the force transducer was mounted on the top end of a foot device used for foot force assessments (pedomotography) – see Fig. 1B. A pedal was fixed in a 17° angle from the horizontal plane. The transducer position was adjustable and positioned under the big toe depending on which foot was assessed. An adjustable heel rest provided optimal support for feet of different sizes, ensured a comfortable fit, and proper placement of the big toe for each subject. For hygiene purposes a disposable plastic cover was applied to cover the force transducer for each individual subject. Subjects were instructed to sit upright on the chair and rest their heel on the device placing their big toe above the force transducer. Three target force level, 1N, 5N, and 10N, were assessed. As no previous data about foot motor coordination in quantitative motor assessments was available we assessed the dominant and non-dominant foot separately and the mean of the two. Foot dominance in this case was assumed to be the same as handedness.
Statistical analysis
Statistical analysis was performed using SPSS (version 20). Because of the relatively small number of subjects, data was not normally distributed within groups. Thus, we applied non-parametric tests. Group comparisons were done using Wilcoxon-Mann-Whitney-Tests; correlations of Q-Motor measures with clinical data was achieved using Spearman-Rho tests. Clinical data used for correlations was the UHDRS-TMS, a lower extremity motor score called “GAIT” (consisting of the gait, tandem gait and retropulsion test sub-items of the UHDRS-TMS), the disease burden score (DBS = [CAG-repeat-35.5]*age) [31], the UHDRS-Total-Functional-Capacity (TFC) and the UHDRS-Functional-Assessment (FA). Statistical significance was assumed at the p≤0.05 level. All analyses were exploratory and no corrections for multiple comparisons were applied.
RESULTS
Between group comparisons
Between group comparisons revealed increased variability in quantitative motor measures in both hand and foot force matching tasks in HD subjects – see Table 1. This was seen for variability as assessed by standard deviation (SD) and by the coefficient of variation (CV). All measures discriminated between symptomatic HD patients and controls with p≤0.001 with the exception of one measure with p≤0.01. Representative box-plots are shown in Fig. 2 for hand force matching and Fig. 3 for foot force matching tasks.
Medians, upper and lower quartiles (in parentheses) of grip and foot force measures
C, controls; HD, HD-patients; N, Newton; GFV-C, Grip force variability-coefficient of variation; GFV-SD, Grip force variability-standard deviation; FFV-C, Foot force variability-coefficient of variation; FFV-SD, Foot force variability-standard deviation; P, pooled analysis; D, Dominant foot; ND, Non-dominant foot. *p≤0.05, **p≤0.01, ***p≤0.001.
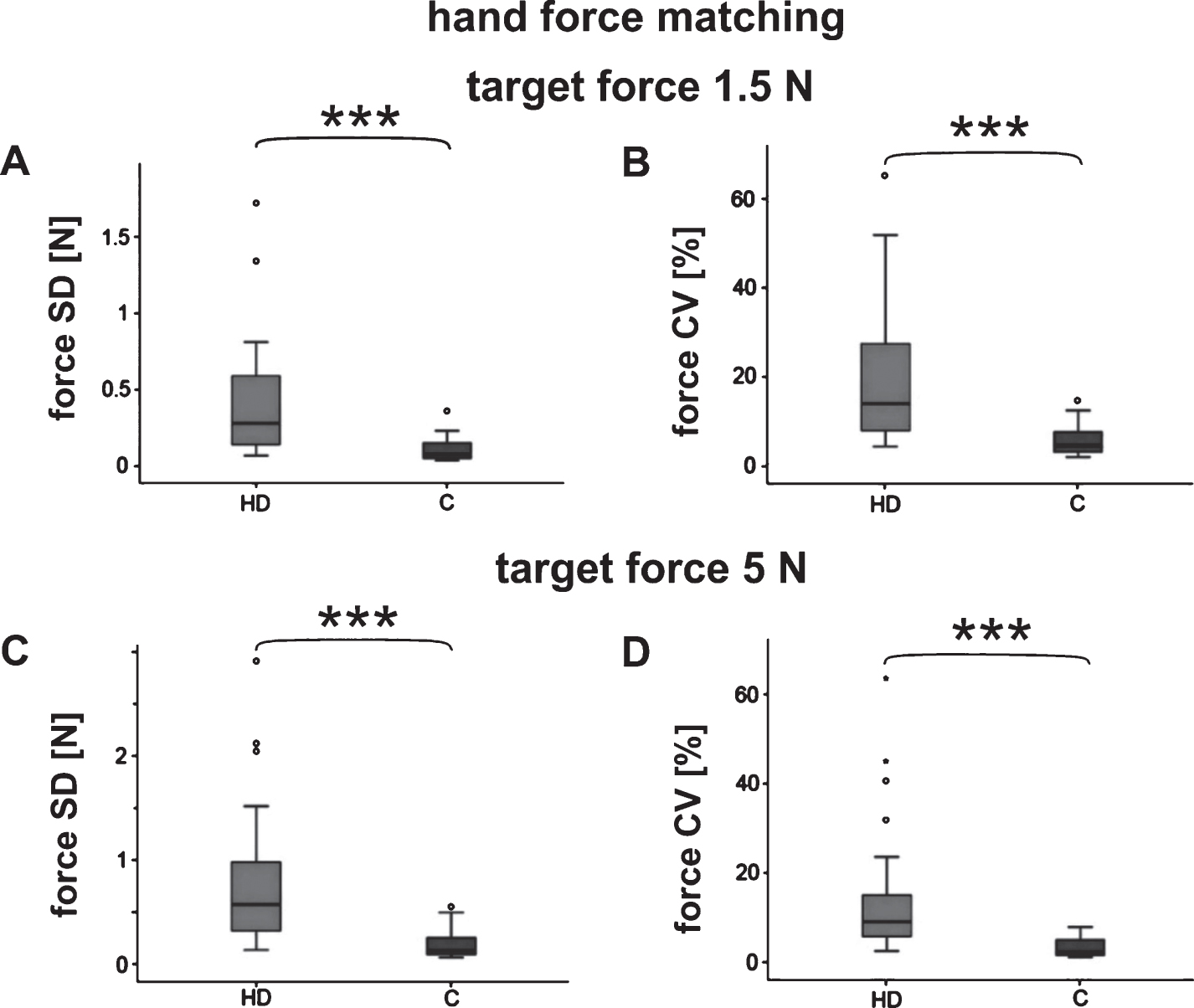
Group comparisons hand force matching. Box-whisker plots of the median, quartiles and range showing grip force variability assessed as standard deviation (SD) and coefficient of variation (CV) as a measures of motor impersistency. Group comparison between HD patients (HD) and Controls (C) for the target forces 1.5N [A, B] and 5N [C, D] (*p≤0.05, **p≤0.01, ***p≤0.001).
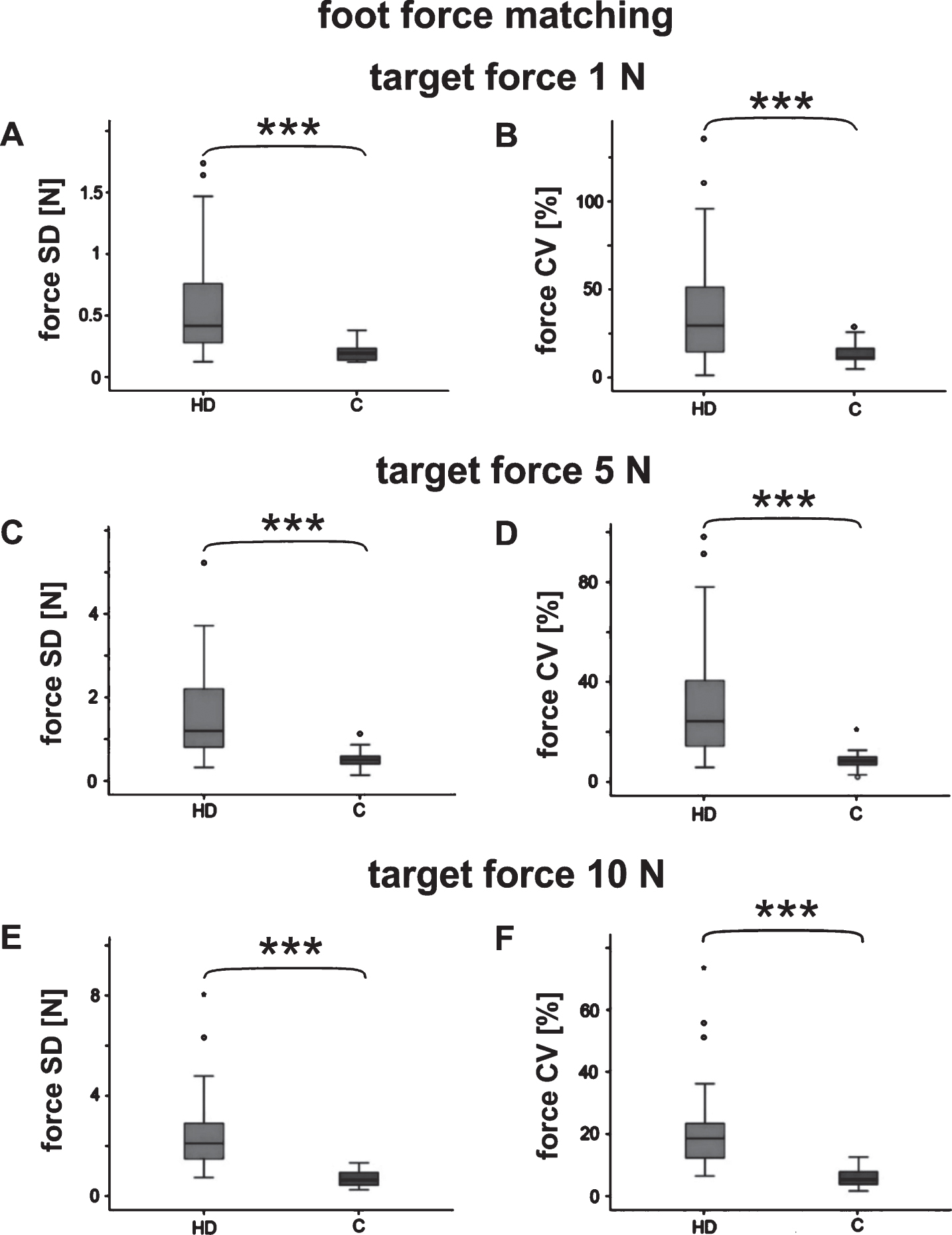
Group comparisons foot force matching. Box-whisker plots of the median, quartiles and range showing Foot force variability assessed as standard deviation (SD) and coefficient of variation (CV) as a measures of motor impersistency. Group comparison between HD patients (HD) and Controls (C) for the target forces 1N [A, B], 5N [C, D] and 10N [E, F] (*p≤0.05, **p≤0.01, ***p≤0.001).
To assess possible inter-trial learning or fatigue effects an additional analysis comparing the first and last trial of every subject and task was performed (data not shown). No significant difference between the first and last trial was detected in HD subjects or controls. Three patients could not complete the 10N foot matching task due to insufficient muscle strength.
Genotype-phenotype correlations
Multiple correlations were observed between clinical measures and the quantitative motor assessments – see Table 2 and Fig. 4. In the hand force matching tasks correlations to the TMS and the FA score were seen at 1.5N target force, but not in the 5N condition. No significant correlations were found with the TFC and DBS scores. Correlations were slightly stronger with the coefficient of variation (CV) than with the standard deviation (SD).
Correlation of force variability measures to motor phenotype and genotype
Gait, TMS for gait and tandem gait; TMS, Unified Huntington’s disease rating scale-total motor score; TFC, Total functional capacity; FA, Functional assessment; DBS, disease burden score; N, Newton; GFV-C, Grip force variability-coefficient of variation; GFV-SD, Grip force variability-standard deviation; FFV-C, Foot force variability-coefficient of variation; FFV-SD, Foot force variability-standard deviation; P, pooled analysis; D, Dominant foot; ND, Non-dominant foot. *p≤0.05, **p≤0.01, ***p≤0.001.
In foot force matching, the strongest correlations were also seen in the lowest force level, i.e., 1N, which revealed correlations with the TMS including the gait-mean sub-score, the TFC, FA and DBS. No other assessment in the study exhibited a TFC correlation. The highest target force of 10N also revealed robust correlations with TMS including gait, FA and DBS.
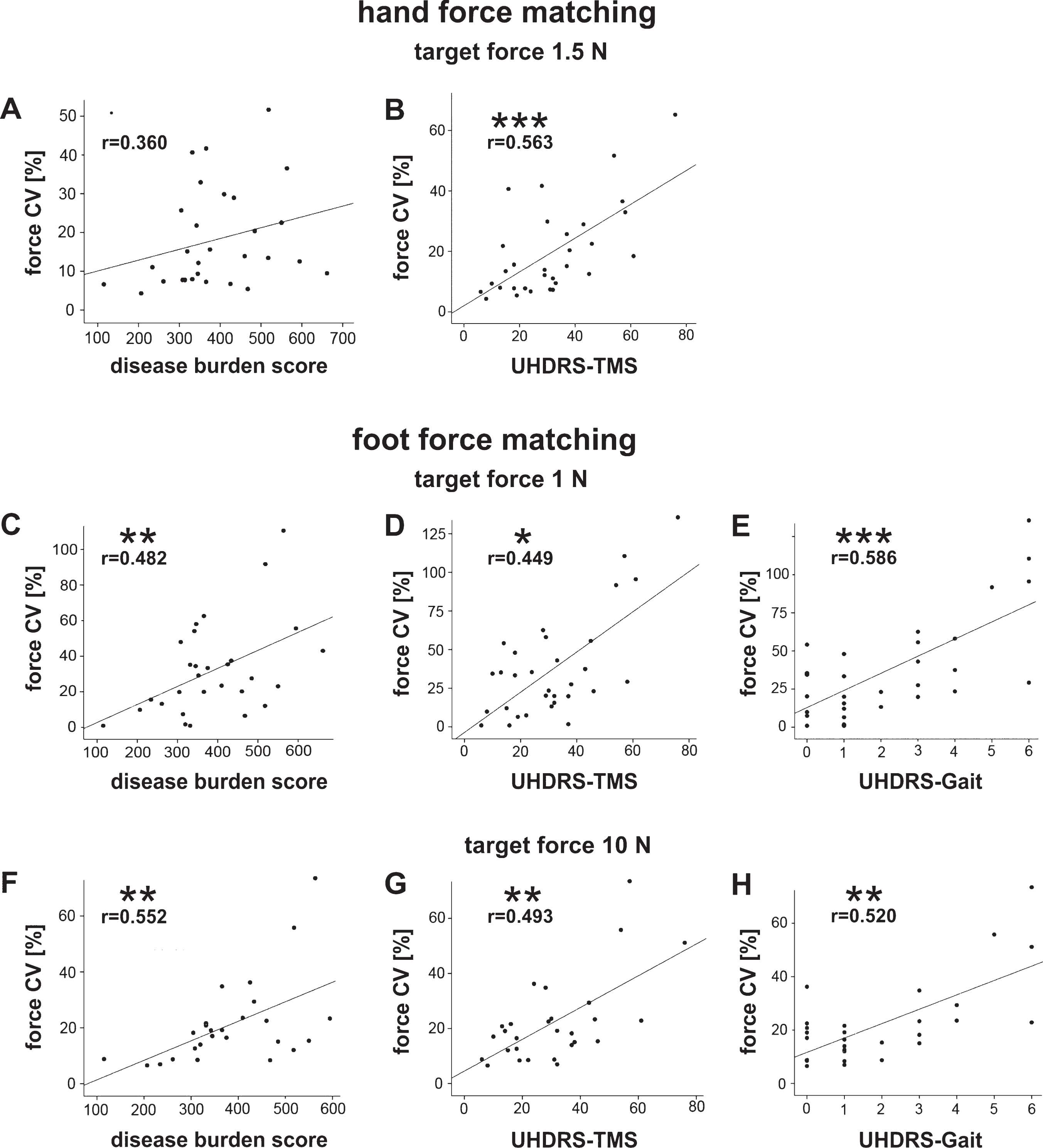
Genotype phenotype correlation. Correlation of hand force matching coefficient of variation (CV) for the target force 1.5N with UHDRS-TMS and disease burden score [A, B] and correlation of foot force matching coefficient of variation (CV) for the target forces 1N [C, D, E] and 10N [F, G, H] with UHDRS-TMS, UHDRS-gait score, and disease burden score. r = correlation coefficient (*p≤0.05, **p≤0.01, ***p≤0.001).
DISCUSSION
In this study we report novel objective and quantitative measures that detect deficits in motor coordination as expressed by motor impersistency in hands and feet of HD compared to control subjects using isometric force matching tasks. The study shows that assessment of force matching tasks is feasible in HD and that both upper and lower extremity are amenable to such assessments.
Discrimination between HD subjects and controls was achieved by all measures. Correlations with clinical measures were observed particularly in the low target forces for both hand and foot tasks. This observation is consistent with earlier findings of lighter objects [25, 33] and lower target forces [19] to be more sensitive in detecting motor deficits. This may be explained partially by lower sensory input at lower target forces. It has been shown that HD patients suffer from a dysfunction in error-feedback control due to disrupted cortical feedback [34]. Impairment of sensory input in HD patients was described in several studies. It is assumed to be a consequence of abnormal gating by the basal ganglia [33]. Accordingly, recent studies demonstrated substantial striatal and white matter pathology [3, 22].
Foot task measures exhibited correlations with the mean gait score derived from the TMS. It is known that abnormalities in gait velocity, stride length and its variability [35] and a significantly greater trunk sway are very common in HD [29] and might be predictive of falls [30], all contributing to functional impairment in HD [2]. Further studies should evaluate whether motor impersistency of the lower extremities could be used as an easy to apply surrogate measure to assess gait and postural stability in out-patient settings. Some correlations of hand and foot force measures with functional disability as assessed by the UHDRS-FA checklist was also seen in both these conditions while a correlation with TFC scores was less frequent and only seen in the foot assessment. The lack of correlation with the TFC may be due to the relatively small range of TFC scores in this group. The foot measures also revealed correlations with the disease burden score (DBS) albeit the sample size of this study was small.
We acknowledge several limitations of this exploratory study besides the sample size. Some patients were taking small doses of neuroleptic medication, which might have influenced motor performance. However, since we aim to develop assessments applicable in clinical trials, exploring performance of these measures under representative conditions including co-medication may be advantageous. Sensitivity of other quantitative motor measures to assess stage and progression of HD subjects was demonstrated in other settings in spite of medication [3, 22]. Task performance may be limited in advanced stages of HD with higher levels of dystonia and parkinsonism, however, most clinical trials are currently conducted in HD stages 1-2 where task performance is not problematic. We also acknowledge limitations of the measures used for correlation analyses: in case of the DBS, the CAG-repeat is not the only determinant of phenotypic variability; the TMS lacks objectivity and has considerable intra- and inter-rater variability and placebo effects [36]. In spite of these limitations the cross-sectional sensitivity of the measures described to discriminate between HD and controls and the multiple correlations observed are encouraging.
Quantitative motor measures were sensitive in assessing severity of HD motor deficits in cross sectional and longitudinal settings in HD biomarker studies [3, 22]; deficits observed were correlated to imaging changes, UHDRS-TMS and the DBS [20, 26]. Q-Motor measures in randomized clinical trials detected central drug effects, while clinical measures did not [17, 37]. The lack of placebo response and rater-dependent bias observed in Q-Motor measures in these trials support a further exploration of these measures to improve the assessment of drug effects in future clinical trials. While several tests have been established [16], novel assessments to measure lower extremity function, are warranted.
In conclusion, isometric force matching tasks are applicable in HD patients, reliably detect a phenotype and display multiple correlations with clinical assessments. The results of this study therefore support a further evaluation of these easy to apply assessments in larger and longitudinal studies, possibly extending to prodromal and premanifest HD.
CONFLICTS OF INTEREST
S. Medzech conducted this project as part of her dissertation and has no other disclosures. C. Sass is a former postdoctoral research fellow of the George-Huntington-Institute and was involved in the TACK-HD and TRACK-ON-HD Q-Motor data analysis. He has no other disclosures. S. Bohlen is an employee of the George-Huntington-Institute and was involved in the TACK-HD and TRACK-ON-HD Q-Motor data analysis. He has no other disclosures. H.W. Lange is an employee of the George-Huntington-Institute and was involved in several projects and publications with Q-Motor assessments. He has no other disclosures. R. Koch has no disclosures. E.B. Ringelstein has no disclosures. R. Reilmann is founding director and owner of the George-Huntington-Institute, a private research institute focused on clinical and preclinical research in Huntington’s disease, and QuantiMedis, a clinical research organization providing Q-Motor (quantitative motor) services in clinical trials and research. He holds appointments at the Dept. of Radiology of the University of Muenster and at the Department of Neurodegenerative Diseases and Hertie-Institute for Clinical Brain Research, University of Tuebingen. Dr. Reilmann serves as elected member of the Steering Committees of the European Huntington Disease Network (EHDN) and the Huntington Study Group (HSG), co-chair of the Task Force on Huntington’s disease and member of the Task Force on Technology of the International Parkinson and Movement Disorder Society (IPMDS). He has provided consulting services, advisory board functions, clinical trial services, quantitative motor analyses, and/or lectures for Actelion Pharmaceuticals, Amarin Neuroscience, AOP Orphan Pharmaceuticals, Cure Huntington Disease Initiative Foundation (CHDI), Desitin, Hoffmann-La Roche, IONIS Pharmaceuticals, Ipsen, Lundbeck, Link Medicine, MEDA Pharma, Medivation, Mitoconix, Neurosearch, Novartis AG, Omeros, Pfizer, Prana Biotechnology, Raptor Pharmaceuticals, Siena Biotech, Temmler Pharma, Teva Pharmaceuticals, uniQure, Vaccinex, Wave Life Sciences, and Wyeth Pharmaceuticals. He has received grant support from the Bundesministerium für Bildung und Forschung (BMBF), the Cure Huntington Disease Initiative Foundation (CHDI), the Deutsche Forschungsgemeinschaft (DFG), the Deutsches Zentrum für Neurodegeneration und Entzündung (DZNE), the European Union 7th Framework Program (EU-FP7), the European Huntington Disease Network (EHDN), the High-Q-Foundation, and the National Science Foundation (NSF).R Schubert is an employee of the George-Huntington-Institute and is involved in Q-Motor analysis of different projects and development of novel tasks supported by the European Union (EU-FP7 program) consortium REPAIR-HD. He has no other disclosures.
Footnotes
ACKNOWLEDGMENTS
This study was supported by donations from HD families and resources available to RR from clinical trial revenues.
We acknowledge the support of all patients and families that volunteered to participate in this study.