
Abstract
It is a common disease of abnormal early pregnancy in obstetrics and gynecology. Inside them, abortion and hydatidiform mole are two common types, which seriously threaten the life safety of pregnant women. To evaluate the diagnostic value of transvaginal ultrasound and serum-HCG in hydatidiform mole and missed abortion. This article introduces the application of transvaginal ultrasound in disease diagnosis. An edge detection algorithm based on multiplicative gradient was proposed: normal pregnant women and abnormal pregnant women were selected as the research objects. According to the pathological examination results of abnormal pregnancy, all pregnant women were divided into two groups: hydatidiform mole group and abortion group. The level of serum β-HCG was measured and its diagnostic value was analyzed. Transvaginal ultrasound combined with serum beta-hcg confirmed the diagnosis of β-HCG.
Keywords
Introduction
In the common abnormal diseases of early pregnancy, hydatidiform mole and missed abortion are two high incidence diseases. The incidence in China is 0.1-0.2%. Hydatidiform mole may develop into malignant cell tumor. Once diagnosed, it should be solved immediately [1]. Leakage abortion is a special way of abortion in clinic. Dead embryonic tissue may enter the mother, causing coagulation dysfunction, threatening the safety of the mother’s life and property. In recent years, the incidence of both diseases has increased significantly, so the value of early diagnosis is very high. However, the clinical manifestations of the two are similar, both of them are vaginal bleeding, the pathology is complex, and the differential diagnosis is difficult. In the current diagnosis technology, ultrasound diagnosis method is simple, noninvasive and widely used. Ultrasound can be used to observe the development and survival of embryo, and can be combined with the history of ectopic pregnancy to predict the development of disease. It is also important for the choice of clinical treatment methods [2]. In the diagnosis of hydatidiform mole and missed abortion, the atypical manifestations may be misdiagnosed, only some data can be obtained from ultrasound. Therefore, it is difficult to rely on image features alone. In the diagnosis of hyddiform mole and miscarriage, it is of great practical significance to apply the multiply gradient based ultrasound image edge detection algorithm in the combination of vaginal ultrasound and serum β – hCG monitoring to improve the diagnostic level of the two diseases.
State of the art
Ultrasound technology is widely used in early pregnancy examinations. It can directly observe the presence or absence of pregnancy, implantation site, and embryonic development. At the same time, it should be combined with medical history to observe whether there is miscarriage [3]. In the diagnosis of ectopic pregnancy, it can show the situation of hemoperitoneum in the pelvic cavity, which has a great effect on predicting the progression of the disease. The current clinical common early pregnancy diseases mainly refer to hydatidiform mole and missed abortion [4]. The pregnant sac of missed abortion is shorter than that of menopause and abnormal in shape. Observation of the morphology of yolk sac is helpful to change the outcome of pregnancy. Many scholars at home and abroad have comparatively analyzed the role of conventional ultrasound, high frequency ultrasound and vaginal ultrasound in the diagnosis of missed abortion, and found that the diagnostic rate of vaginal ultrasound and high frequency color ultrasound have been greatly improved compared with conventional ultrasound. Moreover, the diagnosis can be stopped 1 2 weeks earlier, but the operation of high-frequency ultrasound is more convenient and the patients are more easily accepted. [5]. Color Doppler ultrasound can obtain more hemodynamic parameters and find early pregnancy based on expired abortion resistance index [6]. In the ultrasonic diagnosis of hydatidiform mole, the most typical ultrasonographic feature is that it automatically increases obviously, the wall of the uterus is not homogeneous, and the continuity is complete [7]. In the diagnosis of hydatidiform mole, some scholars find that there are abundant blood flow signals in the uterine wall, increasing resistance index of uterine artery and more abundant blood flow signal in the muscle wall of atypical hydatidiform mole [8].
Methodology
Subject investigated
Pregnant women who are admitted to a department of gynecology and obstetrics department in a hospital are studied. The menopause time is 8 10 weeks, including 50 normal pregnant women and 120 abnormal pregnant women. Patients with abnormal pregnancies are diagnosed according to their medical history and clinical manifestations. There are some differences in patient performance. Some patients have vaginal bleeding and some patients have lower abdominal pain and vomiting. The pathological diagnosis results are grouped into 50 cases of hydatidiform mole and 70 cases of missed abortion. Normal maternal age is (26.3±2.6) years, menopause is (60.3±3.8) days. The hydatidiform mole ages are (27.5±2.6) years, menopause is (61.8±3.2) days, missed abortion group ages are (26.8±2.6) years, menopause is (60.8±3.7) days, and there is no significant difference in basic data between the three groups of pregnant women
All the rules of menstruation before admission for pregnant women are naturally conceived and they are singletons. Excluding assisted reproductive technology pregnancy, multiple complications, genital malformations, and radiological exposure to pregnant women.
Research methods
Serum β-HCG levels are measured in all pregnant women included in the study and vaginal ultrasound is used.
Determination of serum β-HCG levels: All pregnant women take 3 ml of venous blood on the day of admission and measured by chemiluminescence analysis. The instrument used is Bayer automatic biochemical analyzer, the system is 180-system, which can be measured automatically. The concentration of β-HCG monoclonal antibody is diluted to 5μg/ml. The concentration of β-HCG monoclonal antibody is washed three times with normal saline. The sealing solution of 350ul is added to each hole for 2 hours at room temperature. The concentration of β-HCG is frozen and dried. Alkaline phosphatase markers are prepared by modified glutaraldehyde method, 4 mg monoclonal antibody and 2 mg alkaline phosphatase are accurately weighed, washing with normal saline, mixing evenly, the final volume is controlled at 0.5 ml, magnetic stirring, and glutaraldehyde is added. Stir for 15 minutes at room temperature, avoid light for 4 hours, and add ethanolamine, then reaction at room temperature for 2 hours, add dialysate, and change three times. Prepare calibrators, use human β-HCG standards to measure the quality, horse serum standards to dilute, package and save. The microporous plate containing antibodies is added to the serum to be tested, and the antibody is labeled with 100ul alkaline phosphatase. The antibody is oscillated evenly and incubated in a water bath at 37°C for half an hour. Washing solution is used for 4 times, and the paper is sucked dry. Then add 50ul alkaline phosphatase fifth, room temperature dark reaction half an hour, and then determine the luminescence intensity. Transvaginal Ultrasonography: Vaginal ultrasound is performed using a Doppler ultrasound system (Voluson E8, manufactured by GE) and the transvaginal probe frequency is 5 to 9 MHz. For all pregnant women diagnosed, if there is vaginal bleeding, anti-inflammatory hemostasis is performed first, followed by vaginal ultrasound. If the ultrasound image diagnosis prompts intrauterine early pregnancy, review after 1 week. Before vaginal ultrasonic examination, asking the pregnant woman to empty the bladder, take the lithotomy position, lie on his back in the examination bed, apply the coupling agent on the vaginal probe, cover the condom, after preparing enough, put the probe out of the posterior vagina fornix, and scan the multi-cut plane continuously. The measurement of sonographic features. Observing the size and echo of the uterus, focusing on scanning the gestational sac and the yolk sac, and measure the suspicious lesions in the uterus to observe the internal and echogenic lesions. Color Doppler flow is used to observe the distribution of blood flow within the mass and to determine the resistance index and data, and to store rabbit food. If it is found that the uterine cavity is unclear, the pregnant woman will make a fist on the buttocks and use similar methods to explore the attachment area.
Diagnostic criteria and data analysis
Diagnostic criteria for missed abortion: Ultrasonographic diagnosis of pregnancy is less than postmenopausal time, irregular shape, diameter of fetal sac over 2 cm, germ invisible, and no obvious changes in sonographic examination within one week of cardiac tube pulsation. The standard reference range for serum β-HCG values is between 50,000 and 100,000 mIU/ml. This value may also be lower than normal pregnancy levels. Therefore, it is necessary to combine pathological diagnosis.
Hydatidiform mole diagnostic criteria: Ultrasound image examination of the uterus is greater than the time of menopause, intrauterine measurement shows uneven density echoes, and accompanied by large night dark areas. The vesicular echoes appearing in the placenta and the embryonic tissues can be seen. At the same time, serum β-HCG values are above 100,000 mIU/ml, and the levels are consistently high without reduction.
All study data are included in the EXCEL form, and statistical software is used for analysis. α = 0.05 is used as the test standard. P < 0.05 indicates that the difference is statistically significant.
Image processing
Compared with other medical images, ultrasound images are harmless, inexpensive, and have great potential for development. However, ultrasound images have certain deficiencies, the internal structure of biological tissues is complex, and the contours in ultrasound images are not complete. In ultrasound images, the signal-to-noise ratio is relatively low, and the gray difference between different tissues is very small, and the distribution is relatively uneven. [9] Therefore, an accurate target edge processing algorithm is proposed.
In the previous edge detection, the level set method is used, and the curve structure is formed into a higher level set of the dimensional surface, and the topological change of the adaptive curve is obtained [10]. The high-dimensional function is the level set function expressed as Φ (x, y, t). The zero level is used (Φ (x, y, t) =0) to represent the curve C0 (p), and the level set function evolution equation can be expressed as:
In the expression, F denotes the speed function of surface discovery, which mainly realizes the control of the surface, and covers the terms related to the shape of the product set of the image. There are many applications in image segmentation. In order to improve the algorithm, some scholars put forward a function-based segmentation algorithm. It is assumed that the image has a background region and an object region, and the average gray scale is represented by c, and the energy functional function can be expressed as:
Where L represents the length of the closed contour, A represents the area of the interior region, u and v are greater than zero, and λ represents the energy term weight coefficient, which is also greater than zero. When the curve is listed on the boundary line, the value of the function can be guaranteed to be the smallest, so the image segmentation problem is converted into the minimum value of the calculation E.
According to equation (2), the Euler-Lagrangian equation is used for parsing to obtain the partial differential equation of the level set function, expressed as:
The function is normalized and expressed as:
However, the definition of this function is relatively narrow, and there is a deficiency in detecting the overall situation. In order to better detect the edge of the ultrasound image, the edges are correctly identified. The average edge energy is used to monitor the level of zero-level set surfaces close to the edge of the image. The formula is expressed as:
At this point, the level set function can be further evolved. Using this algorithm to adjust the ultrasound image, the image can be accurately observed and the result is more accurate.
Ultrasound image performance
Ultrasound images of normal pregnant women can be seen that the yolk sac is consistent with the embryo, size and other homogeneity, and the embryo does not appear cardiac tube pulsation.
The missed abortion sonogram show that most of the patients have small gestational sac, accompanied by clutter echo, and the echogenicity of the gestational sac is smaller than the corresponding gestational age. The shape is irregular. Figure 1 shows the diagnosis of missed abortion ultrasound. The light spots of varying sizes can be seen in the uterine cavity, accompanied by sacral echoes, and there is an echo-free area at the bottom of the uterine cavity. In one case, the internal echo is irregular and uneven. In 22 cases, the echo of uterine cavity is disorderly and no gestational sac echo is found.
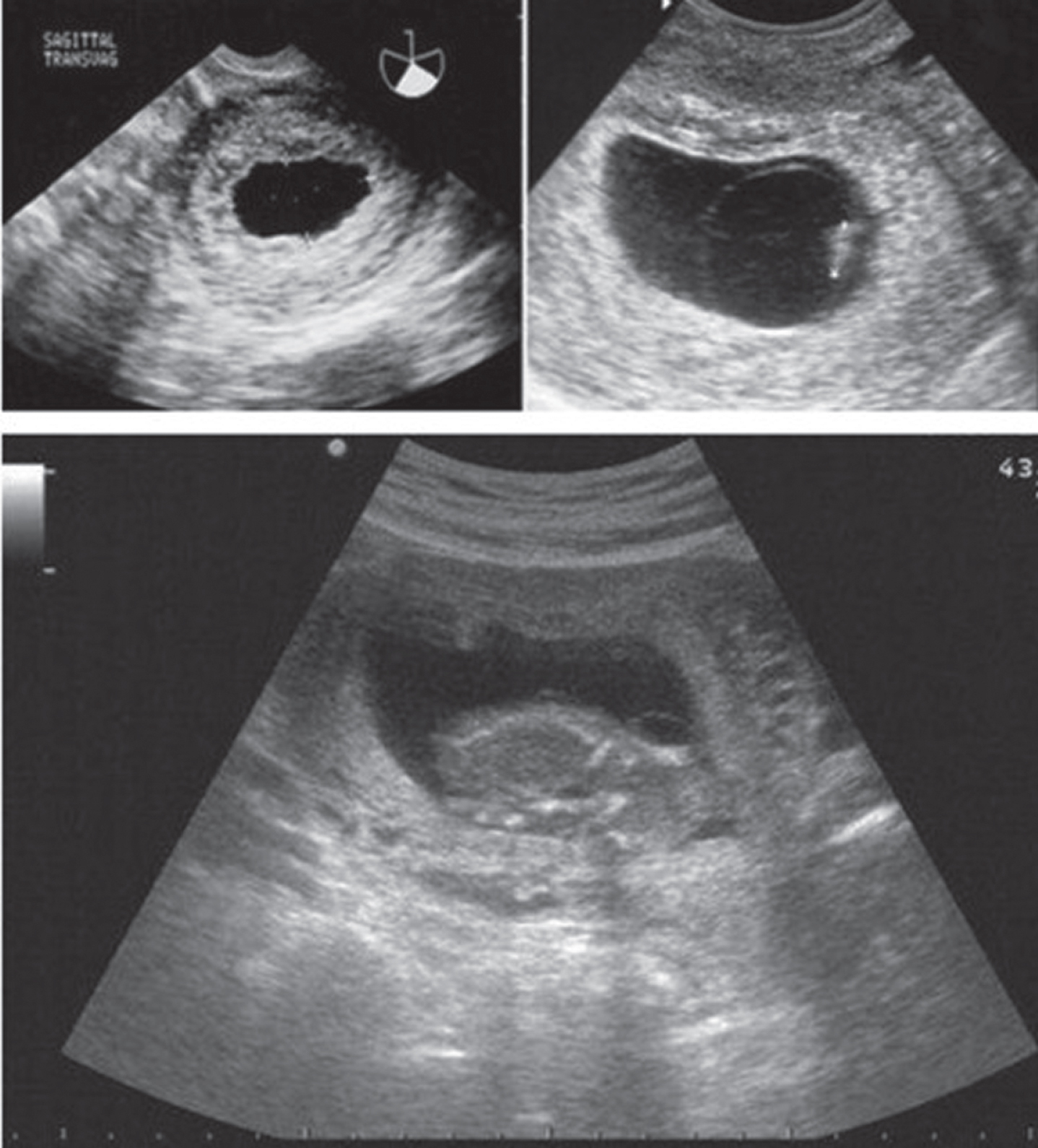
Ultrasonic image diagnosis of abortive abortion.
There are some deficiencies in the ultrasonic image of hydatidiform mole, and Fig. 2 is the ultrasonic image of mole. 15 cases of intrauterine echo disorder appear uneven spot of light, partial ectopic area is uneven, uterine wall blood flow is normal. The echo area is uneven in some areas and the uterine wall blood flow is normal. In 22 cases, embryo tissue is not seen in uterine cavity, irregular echo is observed in some cases, and missed abortion is diagnosed in part, which is misdiagnosed as uterus enlargement. The most obvious manifestation of echo disorder is in 2 cases with embryo in pregnancy sac, with a few enhanced echoes.
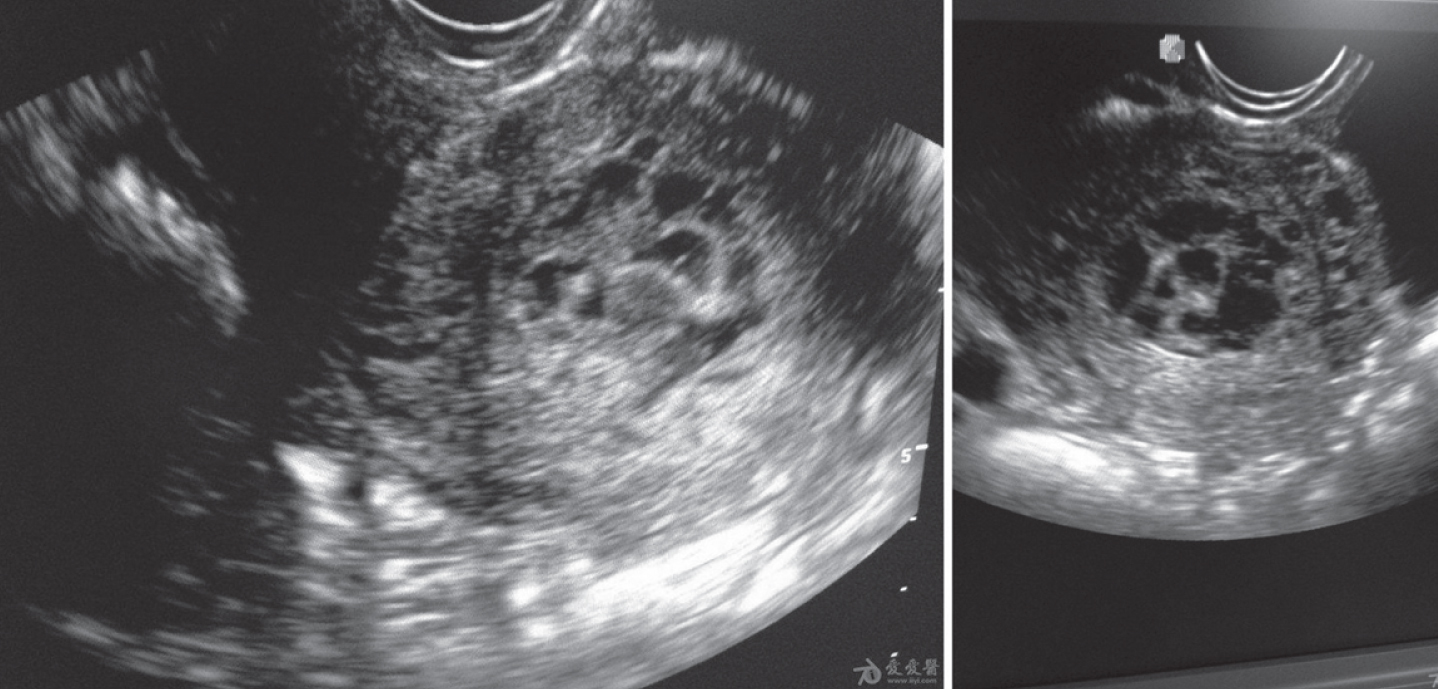
Ultrasonic image of hydatidiform mole.
There are many common characteristics between hydatidiform mole and missed abortion, among which the serum β-HCG level is the most obvious, and in many cases the serum β-HCG content is increased. Hydatidiform mole may cause the increase of serum β-HCG level because of the proliferation of daughter cells, so the serum β-HCG level will exceed the index of normal pregnancy. Missed abortion refers to the cessation of embryo development, so the serum β-HCG level drops, even to zero, which is often used in differential diagnosis.
The serum β-HCG level of the three groups is compared. Table 1 is the result of the measurement. From the table, it can be seen that the serum β-HCG level of the three groups of pregnant women is very different. The β-HCG level in the atypical mole group is significantly higher than that in the other two groups, and the β-HCG level in the missed abortion group is the lowest. The results are consistent with previous studies. Some pregnant women with missed abortion have β-HCG levels in the normal range, so if only rely solely on this β-HCG level to judge, there will be missed diagnoses.
Comparison of serum beta-HCG in 8 weeks less than 9 weeks of pregnancy (mIU/ml)
Comparison of serum beta-HCG in 8 weeks less than 9 weeks of pregnancy (mIU/ml)
Vaginal ultrasound images and serum β-HCG are used to diagnose missed abortions, respectively, to determine the diagnostic value. Table 2 shows the results. It can be seen from the table that the combined diagnosis of vaginal ultrasound images and serum β-HCG can improve the diagnostic accuracy of missed abortion, which is significantly higher than that of a single diagnosis method.
Comparison of three diagnostic methods for missed abortion
Comparison of three diagnostic methods for missed abortion
According to different performances of missed abortion measurement, there will be some differences in the ultrasound diagnosis results. For the withered gestational sac type missed abortion, ultrasound diagnosis is very effective and can be basically diagnosed. If the embryonic tissue can be seen in the uterine cavity mass, fluctuations does not be seen in the heart tube, the embryonic development ceases, there is no natural discharge, and it can be diagnosed as missed abortion. If the uterine cavity mass does not see embryonic sheep tissue, it is generally a hydatidiform mole. The part of missed abortion is cluttered in uterine cavity, and often surrounding the blood clot around the gestational sac. The image is more complicated and difficult to differentiate diagnosis. Other images, such as color Doppler ultrasound, are needed for image diagnosis.
Vaginal ultrasound images and serum β-HCG are used to diagnose hydatidiform moles, and the diagnostic value is judged. Table 3 shows the results. It can be seen from the table that the combined diagnosis of vaginal ultrasound images and serum β-HCG can improve the diagnostic accuracy of hydatidiform mole, which is significantly higher than that of a single diagnosis method. In the diagnosis of hydatidiform mole, there are generally echo-intensive honeycomb structures, relatively uniform rear echo, and the surrounding tissue is relatively clear. The sonogram of early hydatidiform mole shows no specificity and the sonogram is not typical enough to be misdiagnosed as missed abortion. This is because the characteristics of the early hydatidiform mole are not obvious enough and only mildly cluttered villous edema can be detected.
Comparison of three diagnostic methods for atypical hydatidiform mole
Comparison of three diagnostic methods for atypical hydatidiform mole
From the data analysis, it can be seen that the diagnosis of hydatidiform mole and missed abortion, the use of ultrasound diagnosis all appear missed diagnosis, this is because the missed diagnosis of pregnant women with very small lesions, the examination is not careful, such as abortion lesions, most of the lesions are below 15 mm, occasionally there will also be uterine hemorrhage and fluid confusion. In addition, there are some special cases, such as pregnancy stop development and the presence of hydatidiform mole, it is more difficult to distinguish. Therefore, in ultrasonic examination, the detected area can be pressed with a little force, and can be diagnosed with color Doppler ultrasound at the same time.
Single TVS and β-HCG are used to differentiate the two diseases, and the sensitivity and positive predictive value are measured. Table 4 shows the results of ultrasonic differential diagnosis of two diseases. It can be seen from the table that the accuracy of TVS in the differential diagnosis of hydatidiform mole and missed abortion is above 82.5%, the positive predictive value of hydatidiform mole is about 77%, and the positive predictive value of missed abortion is more than 90%.
TVS for the differential diagnosis of two diseases
TVS for the differential diagnosis of two diseases
The diagnostic value of the joint diagnosis for the two diseases is analyzed. Table 5 is the measurement result. When combined diagnosis can be seen from the table, the sensitivity of the two diseases is high, can reach more than 98%, and the positive predictive value reaches 100%.
Evaluation of two combined differential diagnosis of two diseases
In recent years, influenced by environment, living habits and other factors, the incidence of hydatidiform mole and miscarriage has increased gradually, so it is necessary to carry out early diagnosis. In the diagnosis of hydatidiform mole abortion, the edge detection algorithm of Obstetrics and Gynecology ultrasound image based on multiplicative gradient was used to combine the vaginal ultrasound image with the serum β – hCG monitoring. Clinical research methods: normal pregnant women and 120 abnormal pregnant women were selected as the research objects. Pregnant women with abnormal pregnancy were divided into hydatidiform mole group and abortion group. Transvaginal ultrasonography and β – hCG diagnosis. The diagnostic coincidence rate was calculated. The results showed that transvaginal ultrasound and single diagnosis of β – hCG were two better diagnostic methods, and the diagnostic accuracy was high. The combined diagnosis of transvaginal ultrasound and β – hCG can improve the coincidence rate of missed abortion and hydatidiform mole. The diagnostic sensitivity of the two diseases was higher than that of the single diagnosis method. The positive predictive value was more than 98%, and the positive predictive value was 100%. It should be noted that due to the differences of individual factors, the level of β – hCG in patients will be very different, and there will be differences in different gestational weeks and diseases, so the threshold cannot be determined. Therefore, the sample size of this study is small, it is necessary to expand the sample size for further in-depth study.
Footnotes
Acknowledgments
The study was supported by “Science and Technology Project of China Railway Corporation, China (Grant No. 1341324011)”.