
Abstract
OBJECTIVES:
Efavirenz therapy plays an important role in controlling the progression of HIV/AIDS. However, efavirenz often causes short-term side effects for the central nervous system, and it remained controversial as to whether efavirenz leads to depression or even suicidal attempt when applied for a longer period of time. The purpose of this study is to determine the association between the use of efavirenz and depressive disorders.
METHODS:
This study explored the use of efavirenz on HIV-infected patients using National Health Insurance Research Database (NHIRD) in Taiwan by Bayesian survival analysis and investigated whether the use of efavirenz has the risk of depressive disorders. To reduce the dependence of statistical modeling assumptions, this study applied propensity score matching to research data.
RESULTS:
Based on the result of this study, it can be found that the use of efavirenz (HR = 1.009, 95% CI=–0.505 0.554), gender (HR = 0.324, 95% CI = –2.544 0.381) were not significantly associated with the occurrence of depressive disorders, whereas age of HIV diagnosis (HR = 1.021, 95% CI = 0.011 0.055) was significantly associated with the occurrence of depressive disorders. This study concludes that the use of efavirenz does not in-crease the risk of depressive disorders among HIV-treated patients.
CONCLUSIONS:
For the care of HIV-infected patients (especially the older ones), the psychological harm from society, such as lack of social support, social stigma or unemployment is higher than the harm of medicine.
Keywords
Introduction
Human immunodeficiency virus (HIV) is a virus that destroys the immune system, and it is a kind of retroviridae virus. Acquired Immunodeficiency Syndrome (AIDS) is a disease that human beings have acquired various diseases due to the reduction of body resistance due to HIV infection. There were approximately 36.7 million people living with HIV at the end of 2016 with 1.8 million people becoming newly infected in 2016 globally. HIV is a major global public health issue, having claimed more than 35 million lives so far. In 2016, 1 million people died from HIV-related causes globally [1]. HIV is transmitted through humoral exchange. There are three types of infections: sexual behavior, blood contamination or sharing of needles, and mother-to-child transmission.
The origin of HIV is a non-human primate simian virus, probably passed from chimpanzees to human via bush hunters. HIV develops a number of mechanisms to escape immune control and has thereby prevented effective control of the epidemic. The AIDS was first recognized in 1981 [1]. HIV is present in blood, semen and other body fluids such as breast milk and saliva. Exposure to infected fluid leads to a risk of contracting infection, which is dependent on the integrity of exposed site, the type and volume of body fluid, and the viral load. HIV can enter either as free virus or within cells.
Two types of HIV, HIV-1 and HIV-2, have been identified with HIV-1 being the primary source of infection worldwide [2]. HIV attacks and destroys CD4 + T cells in the blood which interrupts the normal functioning of the immune system. When an individual’s CD4 + T cell count drops below 200 and/or the person develops certain opportunistic infections, HIV has progressed to AIDS. This condition progressively reduces the effectiveness of the immune system and leaves individuals susceptible to opportunistic infections [3].
At the beginning of the 21st century, the international community faced formidable health and development challenges, none more so than countries in the poorest region of the world: sub-Saharan Africa. A rapidly expanding HIV epidemic was already dramatically reversing decades of progress on key development indicators, such as infant mortality and life expectancy [4]. Although the global incidence of HIV infection had peaked in the mid-1990 s, more than 3 million people were being newly infected per year, AIDS had become one of the leading causes of adults dying in sub-Saharan Africa and the full onslaught of the epidemic would not be felt until 2006, when more than 2.2 million people died each year from AIDS related causes [5].
AIDS was first recognized by the U.S. Centers for Disease Control and Prevention in 1981 and in 1983, scientists in United States and France independently identified a virus that causes AIDS and named it HIV [6]. Although the infection of HIV/AIDS has existed for about 30 years, the damage it has made to mankind is appalling and overwhelming.
The first effective drug was introduced in 1985, 4 years after HIV was identified; however, not until 1996 was highly active antiretroviral therapy (HAART) proposed and the mortality of people living with HIV got decreased greatly afterward [7]. The main concerns of the use of HAART turn to be the long-term effects associated with these drugs since these drugs are supposed to be applied for lifelong time. Various drug classes were invented for treating HIV infection, such as protease inhibitors, reverse transcriptase inhibitors, integrase inhibitor or even co-receptor inhibitors. With the effectiveness of HAART which has been well established in various clinical trials, post-market surveillance and clinical practices all over the world, HIV infection has become a chronic disease.
In Taiwan, the first HIV case who was a foreigner in transit was identified in December 1984. Taiwan CDC report on HIV/AIDS showed that from 1984 to 2016 about 31,620 Taiwanese and 1,020 foreigners were identified as HIV positives [8]. Of all HIV infections, 58.90% were homosexual contact, 17.74% were heterosexual contact and 21.87% were injecting drug users [8]. To deal with this situation the emphasis has been put on HIV prevention and treatment with overall objectives to limit the spread of HIV efficiently, prevent the uninfected population from HIV, and make sure the infected people have received proper medical treatment such as HAART. As expected, the development of HAART has been associated with a dramatic decline in HIV-associated morbidity and mortality and increased the life expectancy of HIV positive patients. In addition, the medical expenses of HIV patients are paid by the Bureau of National Health Insurance.
HIV infection and depressive disorders
AIDS, depression and cancer are listed by the World Health Organization as the three major diseases of the 21st century. When AIDS and depression are coexisting at the same time, it cannot be ignored. HIV-infected individuals have been found to have a higher prevalence of psychiatric disorders, with rates exceeding those of the general population. Depression is one of major challenges facing people living with HIV [9]. Depression also reduces adherence to treatment, leading to disease progression and mortality [10].
Depression is often triggered by a sense of loss, including death or separation from people, loss of body parts, stress and negative life events, loss of self-esteem, money, loss of dreams, and negative emotional reactions. Depression is a negative mood, and it includes low mood, no hope for the future, self-blame, retreat or restlessness, slow thinking, lack of concentration, poor appetite, and sleep disorders.
Many factors are related to depression, and the influence of personal attributes on depression is also mentioned in many previous studies. However, studies have different results on the impact of gender and age on the quality of life of HIV infected people.
Based on the result of Vosvick, Martin, Smith, and Jenkins’ study [11], men with depression after HIV infection may be accompanied by distraction, social condemnation, and less expression while women are more subject to social condemnation. Penzak, Reddy, and Grimsley declared that women have higher rates of depression than men, but the cause of depression is not related with HIV serostatus [12]. Briongos-Figuero, Bachiller-Luque, Palacios-Martín, De Luis-Román, and Eiros-Bouza conducted a cross-sectional study over 150 HIV-outpatients with Beck Depression Inventory Second Edition inventory, and the results of their study showed that the degree of depression in female is higher than male [13]. Besides, Babowitch, Vanable, and Carey concluded that depressive symptoms may be a more powerful sexual risk factor among women relative to men [14].
Sherr, Fishbein, Spire, Moatti, Shishana, Prince, Catalan, Hedge, and van den Boom indicate that young HIV-infected people are more likely to suffer from depression than older ones [15]. Briongos-Figuero, Bachiller-Luque, Palacios-Martín, De Luis-Román, and Eiros-Bouza conducted a cross-sectional study over 150 HIV-outpatients with Beck Depression Inventory Second Edition inventory, and the results of this study showed that there was no difference in the age and degree of depression of the HIV infected person [13]. Among adolescents living with HIV in sub-Saharan Africa, Ashaba, Cooper-Vince, Vořechovská, Maling, Rukundo, Akena, Tsai declare the incidence of depressive disorders has been increased with age and over calendar time among people living with HIV [9].
Adewuya, Afolabi, Ola, Ogundele, Ajibare, Oladipo, and Fakande explored the association between depression and quality of life in 87 HIV-infected people and found that those with low living standards and low socioeconomic status were more depressed [16]. Kaharuza et al. (2006) measure the depressive symptoms of 1017 HIV-infected people in Uganda using the Center for Epidemiologic Studies Depression Scale, and they found 47% of them had depressive symptoms. HIV infected people who do not have a fixed source of income are more likely to have depression [17]. Song, Lee, Seo, Kim, Noh, Baek, Cheong, and Kim used a Beck Depression Inventory scale for 82 HIV infected people in South Korea. The study found that 21% of the HIV infected people had a prevalence of depression, and a higher level of depression is seen among those who are unemployed or have low social status [18].
Social support is defined as the social resources that persons perceive to be available or that are provided to them. These resources can be instrumental, emotional, or informational, all of which have unique associations with various physical and mental health outcomes [19]. Social support is considered a protective factor for maintaining good health and quality of life in HIV infected people [20]. People with better social support were also more likely to develop more positive health behaviors and adherence to medical treatment [21]. It is not known whether infecting HIV leads to development of depressive disorders, or depressive disorders facilitate the acquisition of HIV. On the other hand, socioeconomic disadvantage has been noted to increase the risk for depression among certain HIV population [22].
Highly active antiretroviral therapy and depressive disorders
There is still no way to cure AIDS and viral infections. However, a variety of antiretroviral drugs can effectively inhibit the number of HIV and enhance human immunity against other opportunistic infections. Combination antiretroviral therapy regimens that were able to suppress viral replication were developed in the late 1990 s and transformed HIV from a progressive illness with a fatal outcome into a chronic manageable disease. After the initiation of antiretroviral therapy, the plasma viral load decreases to concentrations below the lower limit of detection of available commercial assays in most people, usually within 4–6 months. The recovery of CD4 + T cells in individuals on antiretroviral therapy is variable.
Antiretroviral therapy (ART) are divided into five different categories: Nucleoside reverse-transcriptase inhibitors (NRTIs), Nonnucleoside reverse-transcriptase Inhibitors (NNRTIs), Protein per unit inhibitor (PIs), Integrase inhibitors (INIs), and Entry inhibitors. NRTIs is Act on DNA Chain of terminators, inhibition of viral RNA genome reverse transcription into DNA, and this process in the virus life cycle early is a very important event. NNRTIs is binding and inhibition of reverse transcriptions, and this virus enzyme will lead to reverse transcription. PIs is the main role in the virus protease. The enzyme is required to cut the precursor protein so that it is assembled when the inner core of the virus particles is assembled. INIs is to block the action of integrase, a viral enzyme that inserts the viral genome into the DNA of the host cell. Since integration is a vital step in retroviral replication, blocking it can halt further spread of the virus. Entry inhibitors can prevent HIV virions from penetrating its target cells.
The standard treatment consists of a combination of at least three drugs (highly active antiretroviral therapy; HAART), which are used to reduce the likelihood of the virus developing resistance. ART has the potential to reduce mortality and morbidity rates among HIV-infected people, and to improve their quality of life [23].
Efavirenz is one of the most popular medicine used in HAART. It is a selective inhibitor of HIV, and it func-tions as reverse transcriptase non-nucleoside analogues and noncompetitive inhibitors. Efavirenz was introduced to the market in 1998 and it was one of the regimen of choice for treatment-naïve patients recommended by medical personnel [7]. With the introduction of HAART, HIV infection has transformed into a disease for which lifelong medication is necessary for disease control and better survivals. However, the long-term use of HAART might lead to problems of the central nervous system and psychiatric disorders. Efavirenz is now widely used, but its association with depression or suicidality remains controversial.
Some studies indicated that patients taking efavirenz might be at increased risk of developing depressive symptoms, including suicidal idea and attempt. Gutiérrez’s study also indicates that efavirenz increases the possibility of depression [24]. Mollan points out that the risk of suicidality of HIV-infected patients on efavirenz therapy was 2-fold of the risk of HIV-infected patients on non-efavirenz therapy [25]. In Lochet’s study, a significant percentage of HIV-infected patients reported suicidal intentions at the time of the study after one month of efavirenz therapy [26]. After a systematic review, Drury, Ware, Gilfillan, and Ahrens indicated that 60% of HIV-infected patients with efavirenz therapy may experience some form of neuropsychiatric side effects [27].
Efavirenz is now widely used, but its relationship with depression or suicide is still controversial. The utilization of anti-depressants was not significantly different between patients taking efavirenz and those without taking such drug in a nationwide 14-year follow-up study in Denmark [28]. Another Spanish cohort didn’t conclude the positive association of efavirenz with increased risk of clinically significant depression, including depression requiring drug therapy and suicide attempt, instead, the study argued that the use of HAART, no matter what kinds of HAART regimens, would significantly decrease the incidence of such depressive disorders [29]. Some studies were in line with the studies that claim that there was no difference in depressive disorders between HIV-infected patients with efavirenz therapy and those without, and these studies point out that the main effect for HIV-infected patients on depressive disorders is alcohol usage [30] or unemployment [31].
Based on these studies, it can be found that the relationship between the use of efavirenz and the occurrence of depressive disorders among HIV-treated patients has not been determined. Some studies [24–27] indicate that the use of efavirenz boosts the occurrence of depressive disorders among HIV-treated patients. On the other hand, other studies [22, 31] point out that unemployment, alcohol usage and insufficient social sup-port are the main factors that influence the occurrence of depressive disorders among HIV-treated patients.
Objectives of the study
The advantage of Bayesian statistics over classical statistics lies in its comprehensive description of parameters uncertainty [32]. While classical statistics may give the most probable position of the change point, Bayesian methods provide a full posterior probability distribution of its position. The posterior probability distribution can for instance be skewed and/or multimodal. It thus provides much more information than a simple estimation and a credibility interval as usually obtained with classical methods.
Depression also reduces adherence to treatment, and impairs the effectiveness of ARTs, leading to disease progression and mortality [10]. The use of efavirenz is a main treatment method for HIV patients, so understanding the side effects of efavirenz is very important for the use of efavirenz. Anxiety, depression, and suicidal attempts with the use of efavirenz have been reported in some studies, but it remained controversial concerning whether efavirenz may cause neuropsychiatric deficits when being applied for a longer period of time [33]. To reduce the dependence of statistical modeling assumptions, this study applied matching process to research data [34]. The purpose of this study is to examine the association between the use of efavirenz and the occurrence of depressive disorders among HIV-treated patients with Bayesian statistics.
Materials and research method
The purpose of this study is to explore the relationship between the use of efavirenz and the occurrence of depressive disorders among HIV-treated patients with the data obtained from NHIRD by using the Bayesian Cox proportional hazard model.
Research data
The research data of this study was obtained from Taiwan’s National Health Insurance Database (NHIRD), which contained a series of population-based longitudinal databases that covered approximately 99% of the 23 million people living in Taiwan and included 99% of the hospitals and clinics under a mandatory single-payer health insurance system [35]. The NHIRD included the original medical and pharmacy records of all patients.
Data for the HIV-infected patients were identified by the International Classification of Diseases version 9 (ICD-9) codes (042, 043, 044, V08) on the original claim files from 1998 to 2010. Patients that are gender un-known, aged below 20 (in 1998), had HIV or depressive disorder before 1998 were excluded. The total number of objects was 790, and they were divided into two subgroups: patients who were efavirenz-treated and patients who were not. Patients with depressive disorders were defined as having two outpatient records or one hospitalization record. There were 103 patients on efavirenz therapy and 687 patients on non-efavirenz therapy. All patients were followed up until 2010 to discuss whether they had depressive disorders. It has been found that there were 77 patients with depressive disorders and 713 patients without depressive disorders.
In this study, the confirmatory method of depressive disorders patients is to check whether their medical records were recorded in the depressive disorders-related disease codes (ICD-9-CM). The depressive disorders-related disease codes include 296.2 (major depressive disorder, single episode), 296.3 (major depressive disorder, recurrent episode), 300.4 (neurotic depression), 309.0 (brief depressive reaction), 309.1 (prolonged depressive reaction), and 311 (depressive disorder, not elsewhere classified). The remaining patients who had been prescribed efavirenz were classified into the efavirenz-treated group while patients who had never been prescribed efavirenz during the study period were classified into the non-efavirenz-treated group.
Data analysis
Bayesian approach has become a reliable alternative to frequentist statistical inference. There is rich literature concentrated on Bayesian application in biostatistics [36]. Bayesian inference is a statistical inference in which evidence or observations is used to update or to newly calculate the probability of a hypothesis being true. The fundamental concept of Bayesian analysis is that the plausibility of alternative hypotheses is represented by probabilities, and inference is performed by evaluating those probabilities [37].
Survival analysis is wildly used nowadays in survival territories. It is not only used for comparing new medication with old treatments for chronic diseases but also used for immunological experiments. Basically, models that can be used to analyze survival data include non-parametric, semi-parametric and parametric models. Except for the non-parametric model, every model has its unique statistical assumptions. For example, proportional hazard is used in the semi-parametric models. And for the parametric models, exponential, lognormal or Weibull distribution is often used for the statistical distributions of observed survival time. In the semi-parametric models, these assumptions are needed for making statistical prediction on the application purposes in this study. R 3.6.2 with spBayesSurv package was used to analyze data in this study.
The proportional hazards (PH) model is widely used in survival analysis (or the analysis of time-to-event data) [38]. The survival function of PH model is defined as Equation (1), and the density function of PH model is defined as Equation (2).
β ∼ N p (β0, S0)
S0 (·) |α, θ ∼ TBP L (α, S θ (·)), α ∼ Γ (a0, b0), θ N2 (θ ; 0, V0)
(v1, ⋯ v m ) T |τ ∼ IID (τ2), τ-2 ∼ Γ (a τ , b τ )
where β = (β1, … . βp)T is a vector of regression coefficients, vi is an unobserved frailty associated with si, and S0(t) is the baseline survival with density f0(t) corresponding to xij = 0 and vi = 0. Let Gamma(a, b) denote a gamma distribution with mean a/b and Np(μ, Σ) a p-variate normal distribution with mean μ and covariance Σ.
A wide variety of Bayesian nonparametric priors is used in S0(·) model in semiparametric survival analysis. The transformed Bernstein polynomial (TBP) prior is attractive in that it is centered at a given parametric family and it chooses only smooth densities. For a fixed positive integer L, the TBP is defined as Equation (3).
wL∼Dirichlet(α,..., α),
where wL=(w1,..., wL)T is a vector of positive weights, I(·|a, b) denotes a beta cumulative distribution function (cdf) with parameters (a, b), and {S θ (·) : θ ∈ Θ} is a parametric family of survival functions with support on positive reals R + .
For non-spatial data, the independent Gaussian prior IID (τ2) is defined as
Markov chain Monte Carlo (MCMC) is carried out through an empirical Bayes approach coupled with adaptive Metropolis samplers [39, 40]. Recall that wj = 1/L implies the underlying parametric model with S0(t)=S θ (t). Thus, the parametric model provides good starting values for the TBP survival model. The likelihood function for (wL, θ, β, v) is given as Equation (4).
In general, the advantage of Bayesian estimation is that you can incorporate the use of a prior, or assumed knowledge about the current state of “beliefs”, and how the evidence might update those beliefs.
A total of 688 HIV-infected patients were extracted from NHIRD from 1997 to 2010. This study was an established cohort by using the patients from 1999 to 2007 to ensure that all the patients were observed for more than three years.
Of the 688 patients, 128 (18.60%) was given efavirenz at least once as part of HAART, and they were categorized as the efavirenz-treated group. The other 560 (81.40%) patients who never used efavirenz were categorized as non-efavirenz-treated group. The detailed demographic characteristics are listed in Table 1. In both groups, around 85.61% of patients were male, and most of them were under 49 years old.
Demographic characteristics of HIV-infected patients with and without efavirenz treatment, 1998–2010
Demographic characteristics of HIV-infected patients with and without efavirenz treatment, 1998–2010
This study implements the suggestions of Ho, Imai, King, and Stuart [34] for improving parametric statistical models and reducing model dependence by preprocessing data with semi-parametric and non-parametric matching methods. The ratio of efavirenz to non-efavirenz is 1 : 1. R 3.6.2 with MatchIt package was used in this process. Demographic characteristics of HIV-infected patients with and without efavirenz treatment after matching process in this study is as Table 2.
Demographic characteristics of HIV-infected patients with and without efavirenz treatment after propensity score matching in this study
Table 3 shows the Bayesian Cox proportional hazard model for depressive disorders. Use of efavirenz (HR = 1.009, 95% CI = –0.505 0.554), and gender (HR = 0.324, 95% CI = –2.544 0.381) were not significantly associated with the occurrence of depressive disorders. Age of HIV diagnosis (HR = 1.021, 95% CI = 0.011 0.055) was significantly associated with the occurrence of depressive disorders. Lower age has lower odds of getting depressive disorders. One more year of age increases the risk of the occurrence of depressive disorder by 2.1%. The survival curves for male patients with using efavirenz at 25, 55, and 75 years old is shown in Figure 1, and we can find that older HIV-patients’ risk of occurrence of depressive disorders is higher the younger patients.
Bayesian Cox proportional hazard model for depressive disorders onset among HIV-infected patients (n = 256)
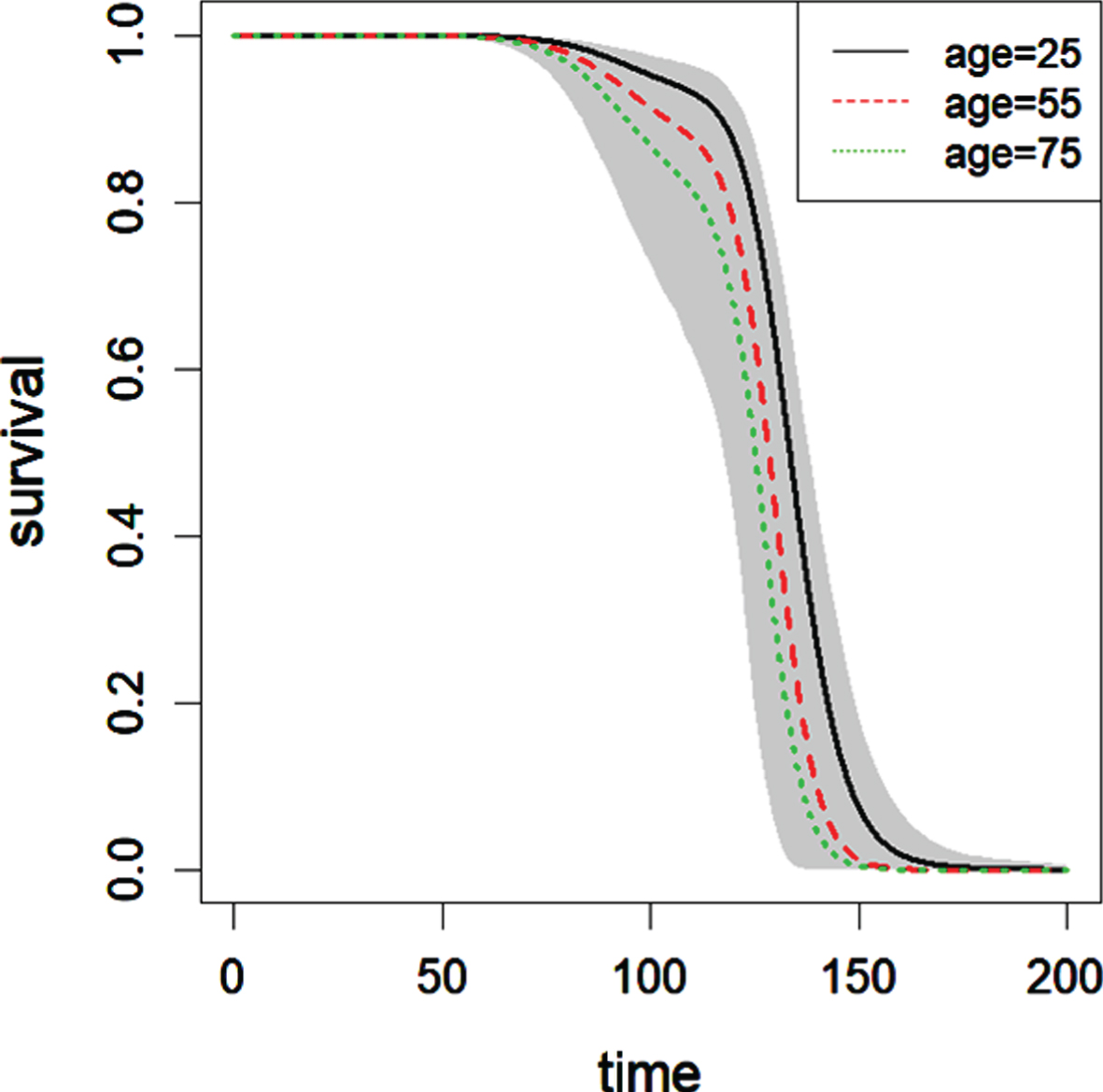
Survival curves with 95% credible interval bands for male patients with the use of efavirenz at different ages. The unit of time is month.
The Log pseudo marginal likelihood (LPML), Deviance Information Criterion (DIC), and Watanabe-Akaike information criterion (WAIC) are –212.591, 421.0286, and 425.1785, respectively. The trace plots for β (use of efavirenz, gender, and age of HIV diagnosis) is shown in Figure 2. The Cox-Snell plots with 10 posterior residuals is in Figure 3.
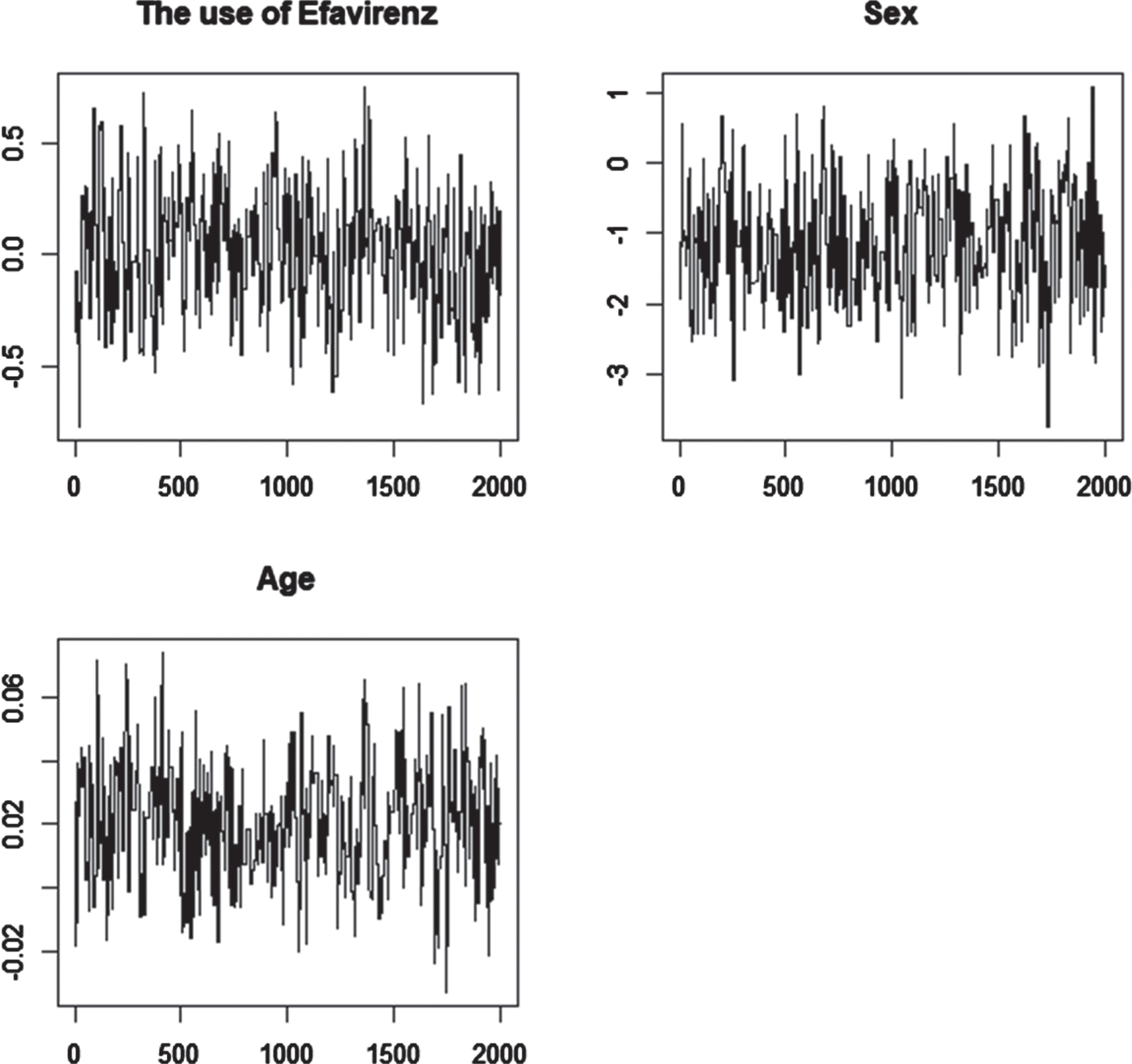
Trace plots for using efavirenz, gender, and age of HIV diagnosis in this study.
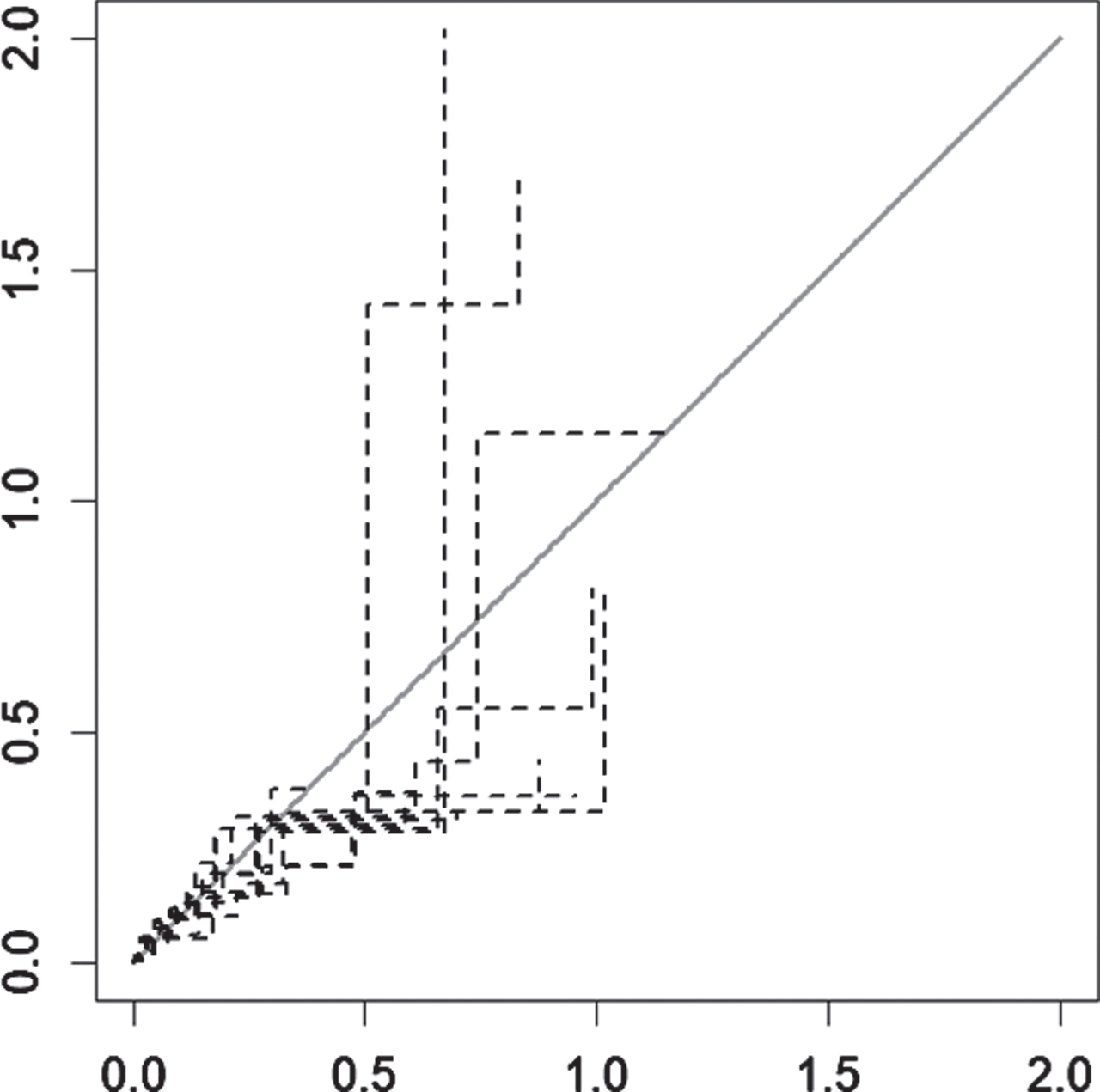
Cox-Snell plot with 10 posterior residuals in this study.
Efavirenz has been widely used in the treatment of HIV, and clinicians are aware of its direct side effects on the central nervous system. However, opinions about the relationship between the use of efavirenz and depression are varied. It makes clinicians unsure whether or not to use efavirenz, and it also makes some HIV-infected patients have doubts in using efavirenz.
The result of previous studies that detect the effect of using efavirenz on the occurrence of depressive disorders among HIV-treated patients are not the same. This study explores the relationship between using efavirenz and the occurrence of depressive disorders among HIV-treated patients with a new technique –Bayesian survival model. The Bayesian analysis differs from the classical method for inference in its use of a prior probability and a posterior probability to express the uncertainty before and after seeing the data respectively. This study was a population-based study that covered nearly 5% of HIV-infected patients in Taiwan. A large administrative claim data spanning 13-year period was used to examine the associations between the use of efavirenz and the occurrence of depressive disorders. With this long observational period, the occurrence of depressive disorders could be detected in a greatest extent, fully addressing the long-term effects of efavirenz.
Based on the result of this study, the use of efavirenz was not significantly associated with the occurrence of depressive disorders, which is consistent with many previous studies [28]. The risk of the occurrence of depressive disorders among HIV-treated patients was not significantly different between using efavirenz and not using efavirenz. Gender was not significantly related to the occurrence of depressive disorders. The risk of the occurrence of depressive disorders among HIV-treated patients was not significantly different between male HIV-infected patients and female HIV-infected patients. Age of HIV diagnosis was significantly related to the occurrence of depressive disorders, which is consistent with many previous studies [9]. As age increases, patients are at higher risk of depressive disorders. One more year of age increases the risk of depressive disorders by 1.031 times. The risk of the occurrence of depressive disorders of older HIV-treated patients was higher than that of younger HIV-infected patients.
Conclusion
In conclusion, in this population-based study over a 13-year period among HIV-infected patients, it can be found that efavirenz use did not increase the risks of depressive disorders among these patients. The psychological harm from society, such as lack of social support, social stigma and unemployment is higher than the harm or side effect of medicine, such as efavirenz. Therefore, in order to prevent depression, more social support should be provided so that HIV-infected patients would develop a higher self-esteem and a better adherence to medical treatment.
Footnotes
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the National Health Insurance Administration, Ministry of Health and Welfare and managed by National Health Research Institutes (NHRI). The interpretation and conclusions contained herein do not represent those of National Health Insurance Administration, Ministry of Health and Welfare or National Health Research Institutes. The author declare that he has no competing interests, and this study is not funded by any organization.