
Abstract
OBJECTIVE:
To measure patient safety climate and the associated factors from the perspective of the multiprofessional team.
METHOD:
This was an analytical cross-sectional study, developed in a medium-sized hospital in the Southern region of Brazil. The Safety Attitudes Questionnaire (SAQ) was used as the data collection tool and applied to 199 workers of the multiprofessional and support team between November 2017 and February 2018. Data analysis was descriptive and analytical. A positive score was considered when ≥75.
RESULTS:
The overall SAQ score was positive (75.1). The domain Satisfaction at Work was the one with the highest score (88.7), while Stress Perception showed the worst score (59.1). It was observed that professionals without a College/University degree better evaluated the domains Satisfaction at Work, Management Perception and Working Conditions, whereas the ones with a College/University degree had better stress perception. Medical doctors showed better Stress Perception when compared to the other health professionals.
CONCLUSION:
There is a positive safety climate in health organizations from the perspective of the multiprofessional team. However, the domains Safety Climate, Working Conditions and Stress Perception constitute areas that need improvement in terms of patient safety in the institution.
Introduction
Patient safety, one of the attributes of the health service quality, is currently defined as the absence of damages to patients in health institutions during care processes [1]. Despite all efforts, adverse events (AE) continue to occur in all health care settings [2].
A study published in 2013 estimated that deaths associated with preventable damages affect more than 400,000 people per year and approximately 4 to 8 million individuals suffer serious damages, which means that, on average, 1,096 deaths and 10,949 to 20,918 serious damages occur daily [3]. A report published in Brazil in 2016 identified that 2.47 Brazilians die in a public or private hospital every three minutes as a consequence of AE related to the care provided to the patient. The report also estimates there are at least 104,187 to 434,112 possible deaths associated with hospital adverse events per year [4].
In this context, the promotion of patient safety culture, an essential requirement to attain the reduction of adverse events through proactive learning based on errors and redesigns of care processes, stands out among the strategies used worldwide in health organizations focused on patient safety [5].
The safety culture is defined as a set of values, attitudes, skills and behaviors that determine commitment with health and safety management, replacing guilt and punishment by the opportunity to learn from failures and improve health care. By measuring the safety climate in health institutions, it is possible to make a diagnosis of the current culture, as well as to identify the potentialities and weaknesses of institutions [6,7].
It is important to note that, when questionnaires are used to study levels of perceptions within a group, the most appropriate term to be used is “safety climate”, since surveys are not able to measure all aspects of the culture, such as behaviors, values and skills [7].
In Brazil, there is a scarcity of safety climate studies covering the multiprofessional team and support professionals in all hospital sectors. Overall, studies assess the safety culture of a specific occupational category, i.e., nurses, physicians, or a specific sector, i.e., the Intensive Care Unit [8–13]. Therefore, it is necessary to carry out more studies that evaluate the issue from the viewpoint of these professionals.
In view of the above, it is important to assess the attitudes and perceptions of safety from the perspective of all workers, considering that patient safety is associated with all professionals involved and all levels of care. Moreover, this diagnosis provides indicators that can be used by the decision-makers when planning actions to promote the safety culture.
This way, frontline health and senior management professionals can both participate in the provision of care without damages. Thus, the objective of this study was to measure the patient safety climate from the perspective of all professionals in the multiprofessional and support teams.
Methods
This was an analytical cross-sectional study developed in a medium-sized general hospital (124 beds) that treats low and medium-complexity cases, located in the Southern region of Brazil.
The following professionals were invited to participate in the research: nurses, nursing technicians, physicians, other health professionals (social workers, pharmacists, nutritionists, psychologists, pharmacy assistants, radiology technicians), and support staff (cleaning and hygiene services, kitchen and catering services, maintenance service, doormen, administrative managers, stockroom service, secretaries, telephone operators, receptionists and others). The professionals who accepted to participate in the study signed the Free and Informed Consent Form.
A total of 199 workers participated in the study, which corresponds to a response rate of 89.6% of the institution’s entire staff (Fig. 1). Therefore, it was consistent with adequate response rates for climate surveys, which should be between 65% and 85% of the studied population [14].
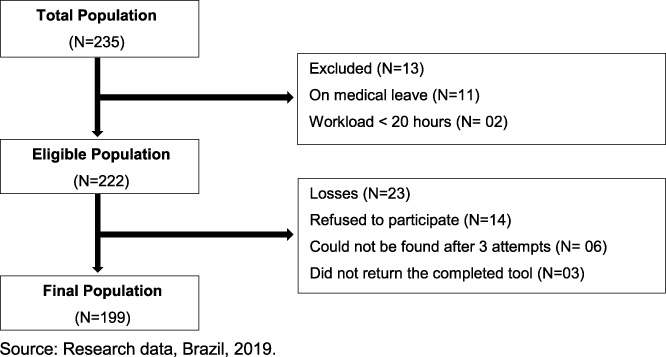
Population selection among the workers of the general hospital, Brazil, 2019.
The following were established as the inclusion criteria: working in the same area at the institution for at least one month; and workload of at least 20 hours a week. These criteria were used because after one month of work and with a minimum workload of 20 hours a week in the same unit, the professionals can perceive the individual and group values, attitudes, perceptions and skills that determine commitment, style and proficiency, regarding the patient safety issues in the health institution [7]. Workers who were on medical leave and on vacation during the data collection period were excluded.
Data collection was carried out between November 2017 and February 2018, using the Safety Attitudes Questionnaire (SAQ) [7], a validated tool for the Brazilian context [10] with good psychometric properties.
The tool consists of two parts: the first one includes questions that assess the team’s attitudes and perceptions, related to the domains Teamwork Climate; Safety climate; Work satisfaction; Stress Perception; Management Perception and Working Conditions; and the second part, which aims to characterize the study subjects. The answer to each of the questions follows a five-point Likert scale: I totally disagree (0 point), partially disagree (25 points), neutral (50 points), partially agree (75 points), totally agree (100 points) and does not apply (X). The final score ranges from 0 to 100. The climate is considered positive for scores ≥75 [7]. The data were organized using the program Epi-Info® 6.04, with double independent typing. The analysis was performed using the Statistical Package for Social Sciences, version 20.0 for Windows (SPSS Inc., Chicago, IL, USA, 2010). The demographic variables comprised gender, age range, level of schooling. Work variables comprised work position, work shift at the institution, other employment bonds, working directly with the patient and time working at the institution.
The level of significance considered for the study was 0.05. Descriptive statistics were analyzed through central tendency (mean) and variability (standard deviation) measurements. Student’s t test was used for the independent groups when comparing the SAQ domain scores between them. When the comparison of the scores involved three or more independent groups, the Analysis of Variance (ANOVA) one-way post-hoc Scheffé test was used. The hypothesis of homogeneity of variance was verified using Levene test and, when rejected, the Brown-Forsythe-Post Hoc Scheffé correction was used.
The study was approved by the Research Ethics Committee under CAAE number 75925417.7.0000.5350 and was in agreement with Resolution N.466/2012 [15].
A total of 199 workers, predominantly females (146, 73.4%), working the day shift (138, 69.3%), without a College/University degree (142, 71.3%) and who had direct contact with the patient (147, 73.9%) participated in the study.
There was a predominance of the nursing team professionals (111; 55.9%), followed by physicians (16; 8%); (1; 0.5%), nutritionist (1; 0.5%), psychologist (1; 0.5%), pharmacists (2; ; 1.0%), pharmacy assistants (5; 2.5%), radiology technicians (3; 1.5%); and support staff (59, 29.6%), namely: cleaning and hygiene services (10; 5%), kitchen staff (12.6%), doormen (7; 1%), maintenance staff (2; 1%); service management (3; 1.5%) and administrative support (28; 14.2%).
The Cronbach’s alpha of the general questionnaire score was 0.85, considered a satisfactory one. The overall SAQ mean was 75.1 ± 10.4, thus showing a positive safety culture. Regarding the domains, the positive evaluation was observed for Work satisfaction (88.7 ± 13.5), Teamwork climate (78.8 ± 14.2), Unit Management Perception (77.1 ± 17.8) and Hospital Management Perception (75.4 ± 18.4). The negative scores were observed for the domains Safety Climate (72.7 ± 15.1), Working Conditions (71.7 ± 27.6) and Stress Perception (59.1 ± 27.1). Table 1 shows the SAQ domains related to variables: work shift, level of schooling and direct/indirect contact with the patient. The results show that the night shift professionals showed the lowest scores (p < 0.001) in relation to the Stress Perception. The opposite was observed in the Working Conditions domain, where the night shift professionals showed a higher score (p = 0.012). Regarding the level of schooling, the Stress Perception showed a higher score (p = 0.007) among the professionals with a degree. Professionals without a degree had significantly higher mean scores in the domains: Work Satisfaction; Hospital and Unit Management Perception and Working conditions.
Bivariate analysis of the SAQ domains regarding work shift, having a degree, and direct contact with the patient, among general hospital employees, Brazil, 2019
Bivariate analysis of the SAQ domains regarding work shift, having a degree, and direct contact with the patient, among general hospital employees, Brazil, 2019
§ Student’s t test for independent groups assuming homogeneity of variances; ¥ Student’s t test for independent groups assuming heterogeneity of variances; Source: Research data, Ijuí, RS, Brazil, 2019.
The results also show that professionals who did not have direct contact with the patient showed a higher score regarding Stress Perception (p = 0.001). The opposite was observed for the Working Conditions domain (p = 0.043), indicating that professionals who had direct contact with the patient had a higher mean. There was no statistical difference in the means obtained for the SAQ domains in relation to gender, age, other employment bonds and time working at the institution.
As shown in Table 2, regarding the occupied position, there was a significant difference in the domain of Stress Perception (p = 0.001), in which the physicians’ scores (72.7 ± 25.9) were higher when compared to the scores of the nursing staff (52.5 ± 27.2, p < 0.01) and other health professionals (63.0 ± 27.2; p < 0.05). Also, it was observed that the support team’s score (67.1 ± 24.2) was significantly higher than the nursing team’s score (p < 0.05).
Mean and standard deviation of the SAQ domains, according to the grouped positions performed by the workers of a general hospital in the State of Rio Grande do Sul, Brazil, 2019
£: Test of Analysis of Variance (One Way) – Post Hoc Scheffée, where averages followed by equal letters do not differ at a significance of 5%; Source: Study data, Brazil, 2019.
Regarding the Working Conditions, the nursing team’s score was higher (p = 0.030) than the scores of all the other positions. The other health professionals of the multiprofessional team had a higher score compared to physicians’ scores (p < 0.05).
Evaluating and understanding the culture of safety in healthcare facilities is essential and, ideally, this assessment should be performed prior to planning actions that aim to provide safe care. One of the key benefits of this type of evaluation is to obtain a concrete indicator of the current state of the safety culture [10].
The overall reliability of the tool, assessed using Cronbach’s alpha, gives the data credibility. Similar results were found in other studies using the same tool [16–20].
This research showed a high rate of responses to the SAQ, probably due to the data collector’s commitment, who approached the workers individually and remained in the collection field for the various work shifts. Moreover, she waited for the answers to be returned and clarified possible doubts regarding its completion.
The broad adherence of the multiprofessional team to the research should be seen as beneficial, since the improvement of the safety culture requires the involvement and dedication of all the professionals related to the process of care and management of health institutions [5,6].
As for the characterization of the study participants, the female gender and the nursing staff predominated. In the Brazilian hospital institutions, the nursing team represents the largest professional group, and it is often the profession with the highest percentage of female professionals [21–23].
As for the level of schooling, professionals with high school education predominated, followed by professionals with a College/University degree. When comparing the SAQ domains with the College/University degree or no degree variable, it was observed that the ones with a degree evaluated the institution’s safety climate more judiciously, showing significant differences in the domains Satisfaction at Work, Stress Perception, Unit and Hospital Management Perception and Working Conditions.
In this sense, the variable education can be considered a positive factor for patient safety, since professional qualification contributes to a more coordinated, articulated and good-quality care, aiming to minimize risks due to stressors that interfere in the provided care [23].
As for having another job or not, it was shown that 138 (69.7%) of the employees worked exclusively at the institution being assessed. This result should be considered a positive one, since having a different employment bond is directly related to the quality of care. This is due to the fact that long working hours can trigger physical and mental fatigue, decrease the time spent on self-care and leisure, and contribute to a greater susceptibility to stress. Moreover, it can trigger problems related to patient safety and the safety of the professionals themselves [24].
In the SAQ overall evaluation, the mean score obtained was 75.1, which translates into a positive safety climate [7], differing from other studies that used the same tool in Brazil [17,18,22,25,26]. Health organizations with a positive safety culture facilitate the implementation of patient safety interventions, which leads to the reduction of the risks of iatrogenic events related to the therapeutic process. Additionally, they aim to guide the arbitrary behaviors of health professionals towards safe care, as a priority in daily practice [27,28].
The professionals’ perception of the safety climate varied in relation to the domains evaluated individually. The domain Teamwork Climate, considered as the quality of the relationship and the collaboration among the members of a team, showed a positive score. This indicates that the workers of this hospital satisfactorily perceived a good collaboration among the members of the multiprofessional team. This result is relevant for the institution, since a well-connected and coordinated team leads to mutual collaboration among professionals, resulting in safe care with fewer chances of harm to the patient [29].
The Safety Climate domain obtained an overall average below the recommended one (72.7). This information suggests that the institution’s organizational commitment, focused on patient safety, is still incipient. This result shows the need to improve error management, promote discussions and organizational learning, and to encourage colleagues to report concerns about patient safety. Moreover, it is important for the institution to disclose the appropriate means to address issues related to patient safety risks and failures [30]. These measures can be effective in reducing AE and thus contribute to improving the safety climate among team members.
The evaluation of Satisfaction at Work shows the positive assessment of the professionals about their workplace. In our study, this domain received the highest score (88.7). The scores were positive for all positions, being higher for the nursing staff, followed by physicians, support staff and other health professionals.
A study showed there was an association between accessibility, visibility, inclusion of team workers in the unit decisions, managers who offer support, recognition and who are flexible with their team and the increase in the professionals’ satisfaction at work [31].
Stress recognition is the only factor in the SAQ that is put in terms of self-behavior of the respondents. The highest mean score of Stress recognition shows evidence of the awareness of workers about the effect of stressors on their performance [20]. In our study, this was the domain that obtained the lowest mean (59.1), corroborating other studies that used the same tool [18,20].
Lack of stress recognition has been related to increased patient and nurse harm [32]. To address this safety issue we need systemic approaches that grapple more effectively with the stress that working conditions in acute care settings pose for staff and patients, especially in low income countries, such as unmanageable workloads and unaddressed dangers.
We observed that professionals with a College/University degree who worked the day shift had a better perception of stress. Having a higher level of schooling provides a more critical view of the processes and thus, leads to greater responsibilities [16,33]. In our study, the physicians showed a better perception of stress, when compared with the nursing team and the other health professionals.
Factors related to human resources, such as professionals’ fatigue due to excessive workload, lack of human resources, communication barriers, non-effective interpersonal relationships, distractions and the professionals’ emotional factor are closely associated to stress recognition. Therefore, they may adversely affect the development of safe care [34].
The domain Unit and Hospital Management Perception was positive, which means that employees usually approve management decisions related to the staff, patient safety, leadership, and human resources management. Contrasting our results, in national and international studies, the domain Management Perception is often evaluated negatively by workers in different hospital institutions [19,22,35]. The positive scores found in this area suggest that the institution’s efforts to improve safety should be maintained, given that managers have an important role in driving, monitoring, and encouraging a safety culture [36].
The Working Conditions domain showed a mean of 71.7. This indicates a negative climate environment. It is important for the institution to recognize the need for improvement in this area, aiming to providing a safer and practice-friendly environment. In this domain, the nursing team showed the highest average, 76.8, which indicates greater satisfaction in relation to the other professionals in the study. This result differs from that of the study carried out with surgical center professionals [25], where the average of nursing professionals was 34.6. It is believed that the stress conditions, widely associated with the surgical center, justify this difference found by the study. Overall, working conditions related to an understaffed institution, work overload, scarce resources, lack of materials, supplies and provisions compromise the quality of care [30].
Also, in our study, professionals without a College/University degree who worked the night shift better evaluated the Working Conditions, with a statistically significant difference. This can be explained by the low expectations that individuals with the lowest level of education have in relation to the ideal working conditions.
The results found in our study contribute to more assertive decision-making in the managerial context of hospital organizations, aiming to promote a culture of patient safety. However, new studies with all Brazilian hospital workers are required to determine whether the safety climate found in this study can be generalized. For these reasons, we suggest for future studies, the analysis of safety culture in an integrated manner using mixed methods, for example. This kind of studies provides useful, contextualized data for management and policy makers in developing and implementing effective strategies to improve patient safety. Furthermore, this study also shows the need for further research in the area, making it possible to explore the phenomenon in different contexts.
From a policy or practice perspective, this study provides important information for managers in that these methods may be useful in the implementation of strategies to consolidate a safety culture in health care institutions.
Conclusion
We found a positive safety climate in the health institution, from the perspective of the multiprofessional team. However, the domains Safety Climate, Working Conditions and Stress Perception comprise areas that need improvement, aiming to improve patient safety in the institution.
The data from this study show that the professionals with a College/University degree showed a better perception of stress, while professionals without a degree better evaluated the management perception, working conditions and job satisfaction. Day-shift professionals perceived stress better, while those working the night shift were more satisfied with working conditions.
Also, the physicians showed better stress perception in comparison to the nursing team and other professionals of the multiprofessional team. The working conditions were better evaluated by the nursing team when compared to the other health professionals and physicians.
The results allowed the diagnosis of the professionals’ attitudes and perceptions regarding the safety culture. It was possible to identify the domains that need improvement. Therefore, they can be used by the assessed institution’s managers and leaders in the planning and implementation of effective strategies to improve patient safety, focusing on attitudes that did not reach positive scores.
Footnotes
Conflict of interest
None to report.