
Abstract
BACKGROUND:
Despite advances in managing nonimmune hydrops fetalis (NIHF), perinatal mortality is still significant. Fetal cardiac failure eventually occurs regardless of etiology. However, no previous study has addressed NIHF from fetal cardiologists’ perspective. Therefore, we evaluated etiology and management of a NIHF cohort requiring fetal cardiologist consultation in a developing country.
METHODS:
A single-center retrospective cohort study of 70 cases with NIHF that were referred to a fetal cardiology unit over four years was performed. Demographics, etiologic diagnosis, and outcomes of the cases were assessed. Antenatal management was evaluated using cardiovascular profile score (CVPS).
RESULTS:
The most frequent diagnosis was Idiopathic hydrops 42(62.6%), followed by hydrops due to cardiac diseases 19(28.4%), and 3 dead fetuses were detected at the first fetal echocardiography. Treatment of fetal tachyarrhythmia (n = 7) had 100% success rate in terms of antenatal hydrops resolution. Digoxin was used in cases of structural heart diseases, twin- twin transfusion syndrome, and dilated cardiomyopathy with perinatal mortality occurring in all cases (n = 9). In cases of idiopathic hydrops, 14 fetuses received digoxin with intrauterine hydrops resolution in 2/14 (14%) while non-treated cases had intrauterine or early neonatal death.
CONCLUSION:
Nonimmune hydrops is the worst complication of diverse etiologies. Limitations in resources for advanced investigations in developing countries increase the possibility of categorizing NIHF as idiopathic. Tachyarrhythmia induced hydrops can be entirely reversed with antenatal therapy while non-tachyarrhythmia fetal cardiac disease outcomes are unfavorable regardless of therapy. On the other hand, idiopathic hydrops shows a limited potential response to digoxin in utero.
Introduction
Hydrops fetalis can be defined as abnormal fluid accumulation within at least two extravascular fetal compartments as generalized skin thickening, pericardial effusion, pleural effusion, and ascites. In the past, immune hydrops was the most frequent type of hydrops fetalis, but with the well-established routine immunization of Rhesus-negative mothers, nonimmune hydrops fetalis (NIHF) makes up 90% of hydrops cases [1]. However, despite massive improvements in diagnostic techniques and management methods for NIHF, the associated morbidity, and mortality remain significant. The perinatal mortality rate was reported to be as high as 72–78% in some series [2, 3]. NIHF may result from diverse etiologies such as genetic, metabolic, and inflammatory causes; associated malformation; or even idiopathic factors. Whatever the causative factor, a decline in cardiac reserve, and fetal heart failure prior to fetal demise is the usual scenario. Nevertheless, the pathogenesis can vary according to the etiology. High-output heart failure might occur in cases of anemia or arteriovenous fistula, low output failure in great arterial obstruction, or myocardial dysfunction, inadequate diastolic filling in arrhythmias, and venous return obstruction in intra-thoracic or intra- abdominal tumors [4, 5].
Over the last couple of decades, several studies have reported the success of utilizing antenatal therapies to manage certain etiologies of NIHF like fetal tachyarrhythmias [6, 7]. Additionally, digoxin has been used as an antenatal treatment for hydrops resulting from different structural and functional heart failure causes [8]. In the current work; we attempted to retrospectively assess the etiologic categories, antenatal management, and outcomes of a NIHF cohort in a developing country from the perspective of fetal cardiologists. Moreover, we tried to determine the success of fetal therapies with a specific emphasis on the use of digoxin in idiopathic hydrops.
Methods
Study design
The study was designed as a single-center retrospective cohort analysis that included the antenatally detected NIHF cases referred to Mansoura University Children's Hospital (MUCH) for fetal cardiology assessment between April 2012 and April 2016. This study was approved by the institutional review board (IRB) of Mansoura Faculty of Medicine, Mansoura University, Egypt. Hydrops was defined as an excessive accumulation of fluid in two or more fetal body compartments, including ascites, pleural effusion, pericardial effusion, and skin edema with a skin thickness >5 mm [9].
Fetal echocardiographic examination
For each case in our study, we collected the gestational age at the first fetal echocardiographic examination. Details of the fetal echocardiography in which a full assessment of cardiovascular structural anatomy and function was performed according to the American Institute of Ultrasound guidelines [10]. The following echocardiography machines were used: (1) the Philips Sonos 5500 (Philips Medical Systems, Andover, Massachusetts 2004) equipped with a C3540 or C5 MHz transabdominal curvilinear Transducer, or (2) Philips iE33 X matrix (Philips Medical Systems, Bothell, WA, USA 2012) equipped with C5-1 MHz transabdominal curvilinear transducers, and (3) the Philips Epiq C7 (Philips Medical Systems, Bothell, WA, USA 2014) equipped with C5 MHz transabdominal curvilinear transducers.
Assessment of the cardiovascular profile score (CVPS) as described by Huhta [11].
The score was determined in the first visit to provide a baseline value and two weeks after therapy for indicated cases with treatments. Evaluation of 5 items was mandatory to calculate the score that included the hydrops compartments, venous Doppler data (umbilical vein and ductus venous), arterial Doppler data (umbilical artery), cardiac size and function (fractional shortening and atrioventricular valves regurgitation).
The idiopathic hydrops diagnosis
After a full echocardiographic examination, middle cerebral artery peak systolic velocity (MCA-PSV) of less than 1.5 multiple of mean to exclude fetal anemia, TORCH screening, maternal blood grouping, Rh analysis, comprehensive ultrasound screening to exclude associated extracardiac anomalies and genetic counseling.
For indicated cases, antenatal therapy consent had to be given in addition to an assessment of the maternal cardiac status by reviewing her history and basal ECG as well as her baseline electrolyte measurements to exclude contraindications for the use of digoxin or antiarrhythmics.
Antenatal treatments
Oral digoxin tablets were prescribed to the mothers at a loading dose of 0.50 mg/12 hr for two days, then a maintenance dose of 0.25 mg/12 hr. For tachyarrhythmias, sotalol tablets might be given at a dose of 80–160 mg twice daily in, and the oral flecainide dose was given at 150–300 mg daily in 3 divided doses. Follow-up of the cases receiving treatment was planned on a weekly basis and was carried out by fetal echocardiography, maternal ECG, and assessment of the serum level of digoxin.
Outcomes
The outcomes were divided into elective pregnancy termination, intrauterine death (stillbirth), premature delivery with live birth, prematurity with neonatal death (early or late neonatal death), full-term with neonatal death (early or late neonatal death), full-term live birth beyond the neonatal period, or loss to follow-up.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 21 (SPSS, Inc, an IBM Company, Chicago, IL, USA). Descriptive statistics were used to describe the characteristics of the patient groups. Continuous variables were compared using Student’s t-test, while categorical variables were compared using the chi- square test. A P-value <0.05 was considered significant.
Results
The study population included 70 pregnant women who were diagnosed as having fetuses with NIHF and who were referred for further fetal cardiology evaluation. Fetal demise was detected at the time of fetal echocardiography in 3 hydropic fetuses that were excluded from further analysis. The median gestational age at the initial diagnosis of the included cases was 28±8 weeks, and the mean maternal age was 26.67±6.43 years. Notably, parental consanguinity was high among our hydrops cohort 41(58.6%). Moreover, most of the referred fetuses had three compartments affected by hydrops accumulation (46.2%), with the most prevalent combination being ascites, pleural effusion, and pericardial effusion 28/67 (28.2%).
The diagnosis was achieved successfully for 25/67 (37.4%) cases, and 42/67 (62.6%) cases were labeled as idiopathic NIHF. Comparisons between the basic characteristics of the NIHF cases with confirmed etiologic diagnoses and the idiopathic groups are shown in Table 1. No statistically significant differences were detected between the groups regarding maternal age, gestational age at the time of first fetal echocardiography, or parental consanguinity. However, the median CVPS of the cases with a confirmed etiology was significantly lower than that of the cases with idiopathic hydrops. In addition, the median frequency of follow-up using fetal echocardiography was higher for fetuses with an identified diagnosis.
Comparison of the basic characteristics of the NIHF cases in the confirmed etiologic diagnosis group with those of the idiopathic group
Comparison of the basic characteristics of the NIHF cases in the confirmed etiologic diagnosis group with those of the idiopathic group
CVPS: cardiovascular profile score, GA: gestational age. *Data expressed as the mean±SD or median (interquartile range) or n (%) according to the variable. **p-value is significant if <0.05.
The fetuses were further divided into different etiologic categories, as shown in Fig. 1. A detailed analysis of the characteristics, management, and outcomes of the hydropic fetuses with a confirmed antenatal diagnosis is presented in Table 2. The most frequently identified cause of antenatal hydrops was fetal cardiac diseases in 19 (28.4%) cases, followed by twin- twin transfusion syndrome (TTTS)in the recipient twin in 3 (4.5%) cases, extracardiac anomalies 2 (3%) cases and tumor in 1 (1.5%) fetus. None of our patients had a positive finding on TORCH screening or evidence of fetal anemia on the MCA–PSV multiple of mean assessment. Moreover, antenatal genetic counseling was performed in 54 cases with the exclusion of fetal arrhythmia cases, full-term pregnancies, and dead fetuses. Nevertheless, antenatal invasive chromosomal, genetic, and metabolic testing was either refused by the mothers or, given to the lack of coverage by medical insurance, not performed due to the high cost. However, postnatal chromosomal analysis using karyotyping was possible in 21 patients: only one patient was proven to have Turner syndrome (45, XO) with associated aortic coarctation, and 20 cases were diagnosed as euploid. No patient in our cohort had any type of trisomy such as Down syndrome. Screening for neonatal inborn errors of metabolism was possible in three of the idiopathic cases but the results did not confirm any specific disorder.
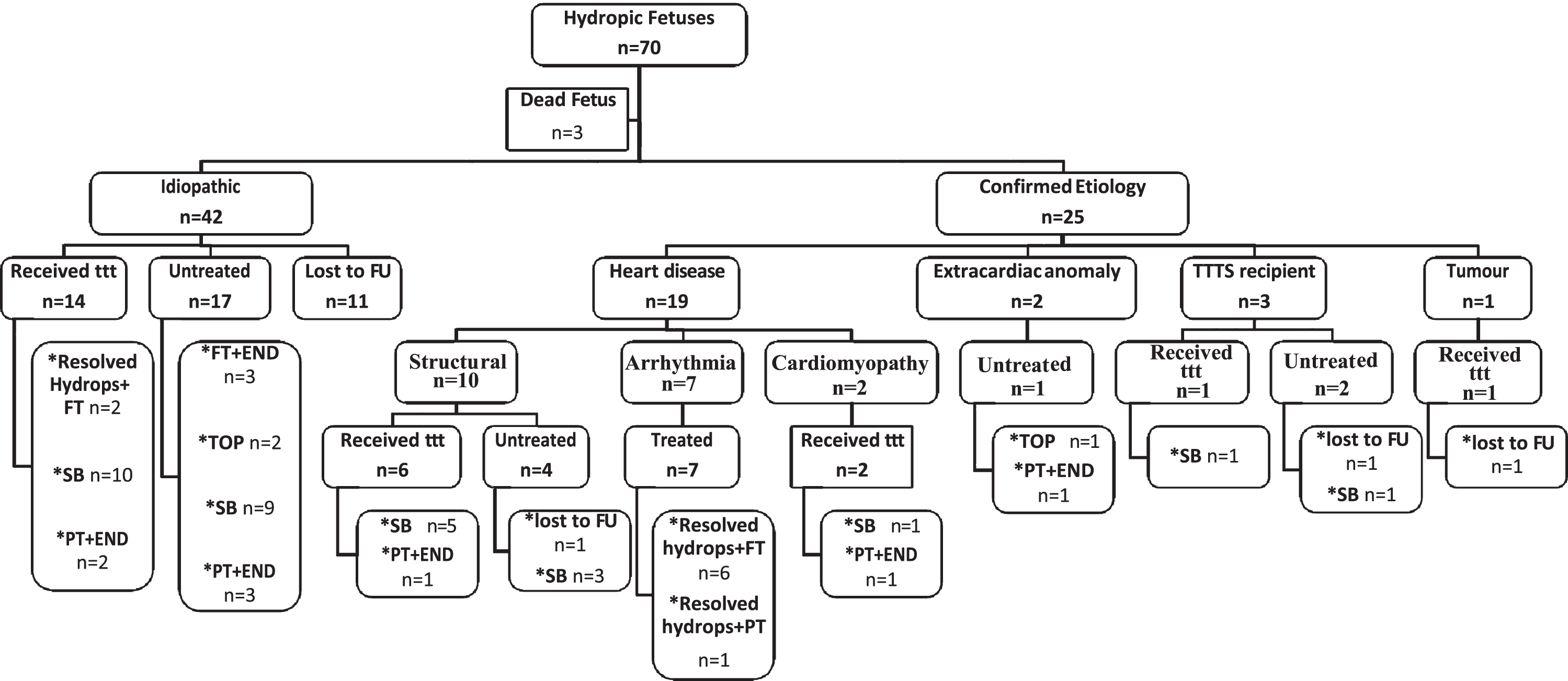
Study population including diagnostic categories and outcome. END: early neonatal death; FT: full tern; FU: follow up; PT: preterm; SB: stillborn, TOP: termination of pregnancy; TTTS: twin-twin transfusion syndrome; TTT: treatment.
Cases of hydrops fetalis with an identified etiologic diagnosis
*Gestational age in weeks expressed as the mean±SD or absolute value for each case in small groups. **CVPS expressed as the median (interquartile range) or absolute value for each case in small groups. AS: aortic stenosis; AVSD: complete atrioventricular septal defect; CCAM: congenital cystic adenomatoid malformation; COA: coarctation of aorta; CVPS: cardiovascular profile score, DORV; double outlet right ventricle; END: early neonatal death, FT: full term, FU: follow up, GA: gestational age in weeks, HLHS; hypoplastic left heart syndrome; PA: pulmonary atresia; PT: preterm, SB: stillborn, SVT: supraventricular tachycardia; TOP: termination of pregnancy; TTTS: twin-twin transfusion syndrome; ttt: treatment.
Antenatal treatment was administered to 16/25 of the diagnosed cases. In cases of fetal tachyarrhythmias (n = 7), digoxin was administered to the mothers alone or in combination with either flecainide or sotalol. Resolution of hydrops was achieved in all the fetuses before birth with a 100% success rate, and all cases survived the neonatal period. Moreover, digoxin was used for fetal hydrops resulting from structural heart diseases (n = 6), dilated cardiomyopathy (n = 2), and TTTS recipient fetuses (n = 1). Unfortunately, seven fetuses were stillborn, and two were preterm and died in the first week of life.
Fetuses with idiopathic hydrops that were included in the study (n = 42) were subdivided into two groups after excluding the cases that were lost to follow-up: the first group included the untreated cases (n = 17), and the second group included the patients who received antenatal digoxin therapy (n = 14). In the untreated idiopathic hydrops group, the mean gestational age was 30.39±5.88 weeks, and the median CVPS at initial diagnosis was 6 (4–8). The outcomes in this group were full-term delivery with early neonatal death (n = 3), preterm delivery with early neonatal death (n = 3), stillbirth (n = 9), and termination for obstetric reasons (n = 2). On the other hand, the mean gestational age of the treated idiopathic category at the initial diagnosis was 24.8±4.6 weeks. Table 3 shows a detailed analysis of the treated cases of idiopathic hydrops fetalis. The mean duration of treatment was 5.4±5.94 days (2–16). Two fetuses had a complete antenatal resolution of hydrops after two weeks of digoxin therapy; however, we continued the medication until term. Nevertheless, no response was observed in the other idiopathic cases who received the medication. The outcomes were stillbirth (n = 10) and preterm birth with early neonatal death (n = 2). The difference in fetal CVPS before treatment and the CVPS two weeks after digoxin use was statistically nonsignificant because of the small sample size (P = 0.102).
Fetuses with idiopathic non-immune hydrops received antenatal therapy
CVPS: cardiovascular profile score, END: early neonatal death, FT: full-term, GA: gestational age, PT: preterm, TTT: Fetal treatment, VSD: ventricular septal defects, w: week.
The overall mortality rate in our hydrops cohort after excluding the cases that were lost to follow-up was 80.5%. All surviving cases received antenatal medical therapy, but none of the fetuses improved spontaneously.
Nonimmune hydrops is the worst complication of a wide variety of fetal diseases. Despite the abounding studies on NIHF, most of the reports in the literature discuss obstetrician-based management; however, the current work is considered the first approach for NIHF from fetal cardiological perspective.
NIHF has various etiologies; however, the most prevalent etiologic category differs from one study population to another, and regardless of the advances in the prenatal screening and breakthrough in investigatory tools, many cases of NIHF remain undiagnosed. In the current study, 62.6% of NIHF cases were idiopathic followed by 28.4% of cases being caused by fetal cardiac disorders, whether structural, rhythm, or myopathic. Comparable results were reported in an earlier study, in which more than half of the cases were considered idiopathic [12]. Idiopathic cases made up approximately one-third of the cohort in other series [13, 14]. In contrast, Bellini et al. found in a systemic review of 6361 NIHF fetuses that cardiovascular disorders were the most frequent category (21.7%) of NIHF followed by idiopathic NIHF (17.8%) [1]. The percentage of fetuses with an unknown etiology of NIHF was reported to be as low as 13% in another study [15].
The high percentage of idiopathic cases in our cohort is simulating early reports from the nineties of the previous century. This can be explained by limitations in the detection of metabolic, chromosomal, and genetic disorders antenatally, as is typical of developing countries. On the one hand, due to religious and cultural beliefs, the practice of pregnancy termination is limited, especially in Middle Eastern countries except in cases of obstetric indications. Hence, none of our patients consented to undergo an invasive procedure such as amniocentesis because the result would not have affected the termination decision. In addition, most of the families refused an autopsy of a stillborn or dead newborn due to cultural factors limiting the data available for a proper perinatal diagnosis. On the other hand, the expensive genetic and metabolic tests, as well as invasive diagnostic methods, are not usually covered by insurance nor are they available in most governmental hospitals. Therefore, these tests represent a considerable financial burden on families.
Regarding the affected compartments with hydrops, the ascites-pleural-skin combination was the most frequent 19(28.2%). Our result matched the findings of Derderian et al., who found 28% of NIHF cases with the same combination and with no correlation between the absolute numbers of involved compartments, and survival [16]. Fetal cardiac diseases causing NIHF is not a separate etiologic entity but it has different subcategories that vary in terms of their outcomes and responses to antenatal therapies. In the current work, the hydropic fetuses with tachyarrhythmia had the most favorable outcomes. The seven included fetuses received antenatal antiarrhythmic therapies with complete hydrops resolution intrauterine occurring in 100% of cases, and they were all born alive. Starting antiarrhythmic medication for hydropic fetuses with arrhythmia is a class I/Level of evidence A recommendation by the American heart association [17]. Similar guidance was issued by the society of maternal-fetal medicine (SMFM) to treat fetal hydropic arrhythmia unless the gestational age is near-term [18]. Unlike fetal tachyarrhythmia, structural cardiac anomalies and dilated cardiomyopathy had unfavorable outcomes regardless of management. We used digoxin in nine non-arrhythmic hydropic fetuses with an identified diagnosis: TTTS (n = 1), dilated cardiomyopathy (n = 2), and structural heart diseases (n = 6). Nevertheless, the treatment results were not satisfactory as seven were stillborn, and two were preterm with early neonatal death. Our results were in opposition to the outcome of the antenatal digoxin utilization in previous studies. For cases of TTTS, digoxin was reported to reverse the hydrops antenatally and the fetuses were born alive [19–21]. Hydrops regression and improvement of ventricular systolic functions have also been described in fetal aortic stenosis [22] and Ebstein’s anomaly of the tricuspid valve [23]. Patel et al. analyzed the results of treating 14 hydropic fetuses with digoxin. Different etiologies were identified in their series (TTTS, cystic hygroma, sacrococcygeal teratoma, cardiomyopathy, and structural heart diseases). Ten fetuses were born alive, and four cases with severe hydrops died in utero [8]. The outcome of our group might be affected by the unavailability of fetal interventions in our center, such as in utero valvuloplasty for critical stenosis or laser for TTTS.
Hydrops can eventually lead to heart failure as a final pathway of demise. Moreover, alterations in CVPS parameters are considered signs of fetal congestive heart failure. Thus, the score was found to be a useful tool for mortality prediction in fetal hydrops, even in idiopathic cases [4, 5]. On the grounds of that, we evaluated the effect of digoxin on idiopathic hydrops fetalis as a manifestation of cardiac function impairment. The assessment of the digoxin effect in idiopathic hydrops has never been addressed in detail in previous research. Fourteen cases of idiopathic hydrops fetalis were given digoxin antenatal. Two fetuses demonstrated complete resolution of hydrops after treatment during the fetal stage and were born alive with an uneventful neonatal period while another fetus was born preterm and died on the day of birth. Unfortunately, the other 10 cases were stillborn. However, it is notable that none of the untreated cases survived the first day of life.
We did not encounter any significant complications associated with antenatal medical management in our series, but we had to delay digoxin intake in two cases of maternal hypokalemia until the condition was corrected. Complications from fetal therapy could be avoided by proper maternal assessment before initiation to exclude mothers with contraindications to the medications as well as by ongoing follow-up of both the mother and the fetus. Nevertheless, maternal counseling for fetal treatments should stress on the potential side effects and the predictable response based on the published data.
One of our study limitations is the retrospective nature of the work and another is the small number of cases in some etiologic categories that made it difficult to perform statistical comparisons. Another prospective study with a significant number of cases might be required to verify that the limited success we encountered in controlling idiopathic hydrops in utero did not occur purely by chance as some studies have documented possible spontaneous intrauterine improvement of fetal ascites or hydrops [13, 24]. Furthermore, it is possible that our cohort is not completely representative of hydrops in our population due to referral bias. Our work describes fetuses with hydrops requiring assessment by a fetal cardiologist. Thus, patients of congenital infections or fetal anemia might not be referred to a fetal cardiologist and may be managed entirely by the fetal medicine team.
Conclusion
Hydrops fetalis is considered the worst complication for a spectrum of diverse etiologies. Although some etiologies such as fetal tachyarrhythmia can be entirely treated antenatally, hydrops is associated with high mortality, especially hydrops due to structural and myopathic heart diseases as well as idiopathic category. Limited resources for advanced metabolic and genetic investigations in the setting of a low income developing country together with cultural aspects can raise the possibility of categorizing NIHF as idiopathic. Fetal idiopathic hydrops has a limited potential response to antenatal digoxin. However, the results need to be further verified on a larger population.
Funding
None.
Conflicts of interest
The authors declare that they have no competing interest