
Abstract
OBJECTIVE:
Postoperative hyperglycemia has been shown to be associated with higher morbidity and mortality in pediatric patients. Data on risk factors for neonatal patients is limited. The objective of this study was to identify pre- and intraoperative risk factors associated with postoperative glucose in neonates.
METHODS:
We conducted a retrospective cohort study of neonates after surgical procedures between January and December 2016 in a quaternary neonatal intensive care unit. The primary outcome was hyperglycemia defined as serum glucose ≥8.3 mmol/L during the first 4 hours postoperatively. Secondary outcomes included death and length of stay. We assessed the association of risk factors with the postoperative glucose.
RESULTS:
In total, 206 surgical procedures (171 patients) were evaluated, among which 178 had serum glucose values during the first 4 hours postoperatively available. The incidence of hyperglycemia was 54% (n = 96). The median (IQR) glucose during the first 4 hours in NICU was 8.4 (6.52–10.65) mmol/L. Risk factors for postoperative hyperglycemia were intraoperative glucose infusion rate (GIR) and gestational age. There was a non-linear relationship between gestational age and postoperative hyperglycemia. Mortality occurred in 6 (7%) in the no-hyperglycemia group and 3 (3%) in the hyperglycemia group (p = 0.31).
CONCLUSIONS:
Among the risk factors, intraoperative GIR was identified as a modifiable factor that can reduce postoperative hyperglycemia. A non-linear relationship of gestational age with postoperative glucose provides new insights that may help advance our understanding of the complex mechanisms of glucose homeostasis in neonates.
Introduction
Hyperglycemia is common in critically ill children [1, 2], especially in the perioperative period [3, 4] where there are alterations in glucose metabolism due to surgical stress, reduced metabolic rate and oxygen consumption. Studies in young children have shown significant morbidity and mortality [4–11]; with longer length of stay (LOS) in the intensive care unit, higher mortality in severely hyperglycemic patients [9], longer duration of mechanical ventilation [4, 11], higher inotrope use [11], nosocomial infections [5, 8], worse systemic and cerebral oxygen transport [7], seizures, and stroke [8]. Identified risk factors for postoperative hyperglycemia include age <31 days, higher preoperative severity of illness, intraoperative steroids, and longer duration of cardiopulmonary bypass [8]. However, previous studies on risk factors for postoperative hyperglycemia included mostly pediatric patients who underwent cardiac surgery, and data are limited for non-cardiac neonates.
Due to concerns regarding the association of postoperative hyperglycemia with adverse outcomes in the neonatal population, the aim of our study was to identify pre- and intraoperative risk factors for postoperative hyperglycemia in neonates.
Methods
A retrospective cohort study was conducted at the Hospital for Sick Children, Toronto, Canada, a children’s hospital whose quaternary neonatal intensive care unit (NICU) serves a catchment area of 75,000 births per year and has 800 admissions annually. There are no deliveries on-site, and 40% of admissions have a primary diagnosis of a surgical condition. Patients with surgical procedures during January 2016 to December 2016 were identified from the NICU clinical database and data was collected from electronic charts.
The study was approved by the Hospital for Sick Children Research Ethics Board.
Inclusion and exclusion criteria
Neonates admitted to the NICU who underwent surgical procedures in the operating room were included. For patients who had more than one procedure, each procedure was treated as a separate case. Patients were excluded if they had known hypoglycemia or hyperglycemia requiring glucagon or insulin infusions within 7 days preoperatively.
Clinical characteristics
Data collected included: demographics; surgical procedure details including, diagnosis, age, weight, duration, glucose intake intra-operatively, blood products received intraoperatively; preoperative details including: glucose intake, use of steroids ≤72 hours, need for vasopressors and/or inotropes ≤24 hours; postoperative details including: glucose ≤24 hours or until glucose level <11 mmol/L whichever occurred later, glucose intake, need for insulin ≤24 hours. Data on in-hospital death, age of death and NICU LOS were also collected.
Surgical diagnoses/procedures were categorized as a) central nervous system: including hydrocephalus and meningitis requiring drainage; b) gastrointestinal (GI) congenital: including intestinal atresias, tracheo-esophageal/esophageal atresia, anorectal malformation, abdominal wall defects, malrotation/volvulus and meconium ileus without peritonitis and/or perforation; c) GI inflammatory: including necrotizing enterocolitis, bowel perforation, congenital GI diagnosis with bowel perforation and/or peritonitis; and d) others: including patent ductus arteriosus ligation, nephrectomy, bronchoscopy, excision of lung mass, and tracheotomy.
The glucose infusion rate (GIR) at a given time was calculated in mg/kg/min based on glucose concentration and rate of administration of all infusions (including intravenous maintenance fluids, parenteral nutrition, medication infusions diluted in dextrose-containing fluids). The GIR was collected at three different time points: immediately before surgery, during surgery, and within 24 hours after surgery. Enteral feeds did not contribute to the GIR immediately before surgery since all neonates were nil per os (NPO) due to their underlying GI pathology or due to anticipated/planned surgery. Glucose measurements were either by point-of-care testing (POCT) or serum glucose. When POCT and serum glucose were measured simultaneously (≤15 minutes apart), the serum glucose value was recorded.
Outcomes
The primary outcome was glucose in the first 4 hours after surgery. Secondary outcomes included NICU LOS, hypoglycemia (defined as glucose ≤2.6 mmol/L) within 4 hours after surgery, and death. Glucose was analyzed as a continuous variable and as a proportion with hyperglycemia defined as serum glucose ≥8.3 mmol/L [12, 13].
Statistical analysis
For patient characteristics, descriptive statistics were used. We screened for candidate risk factors based on their clinical relevance and correlation with predictors. Instead of p-value based selection commonly used in traditional regression, we selected risk factors for the primary outcome of postoperative glucose based on their ability to predict new observations. To this aim, we applied a boosting method [14] for risk factor selection, then quantified the association between the selected risk factors and outcome variable using multivariable regression. To reduce the potential influence of extreme observations on the fitted model, we log-transformed the postoperative glucose value.
We tuned the hyperparameters of the model using 5-fold cross-validations and chose the values that minimized prediction errors for the final risk factor model. After risk factor selection, we applied multivariable regression with restricted cubic splines with 4 interior knots to estimate the nonlinear associations between the selected risk factors and glucose value. Model coefficients of dichotomous or polytomous predictors were quantified as incremental effects adjusted for other risk factors.
Competing risk analysis was applied to assess LOS for the overall cohort and by hyperglycemic status during the first 4 hours postoperatively, with postoperative in-hospital death as the competing risk. The outcome variable was time-to-first-event, either discharged alive from the index hospitalization or in-hospital death. The difference in cumulative proportions was assessed using Gray’s tests. All analyses were conducted at the significance level of 5% using R with the rms [15, 16] and mboost [14] packages.
Results
During the study period, 206 surgical procedures were performed in 171 neonates. Among 178 surgeries with at least one glucose measurement in the first 4 hours postoperatively, hyperglycemia occurred in 96 (53.9%) cases. Median (IQR) glucose in the first 4 hours postoperatively was 8.4 (6.52–10.65) mmol/L. Table 1 depicts the baseline characteristics of neonates with and without postoperative hyperglycemia.
Baseline characteristics of neonates with and without postoperative hyperglycemia
Baseline characteristics of neonates with and without postoperative hyperglycemia
IQR: interquartile range; ASA: American Society of Anaesthesiology.
The following candidate risk factors were considered: gestational age (GA), gender, surgical diagnosis, weight at surgery, intraoperative GIR, blood product use intraoperatively, and duration of surgery. Using the boosting methods with 5-fold cross-validation, two risk factors were identified, namely intraoperative total GIR and GA. The nonlinear associations of the selected risk factors were estimated using multivariable linear regression. The adjusted R2 of the regression model was 16.9%. Figure 1A demonstrates the relationship between GA and postoperative glucose. A non-linear relationship is seen, where for preterm infants with GA 28 to 35 weeks, there was a positive correlation; as GA increased, the postoperative glucose increased. At 35 weeks, the relationship became reversed, with glucose decreasing as GA increased. Figure 1B shows the association between intraoperative total GIR and postoperative glucose. Each unit increase in intraoperative total GIR increased the log-transformed postoperative glucose by approximately 5.8% (Coef [95% CI] = 0.058 [0.034, 0.082], p < 0.001). For Fig. 1, the log-transformed glucose values were converted back to actual glucose values for clinical interpretability.
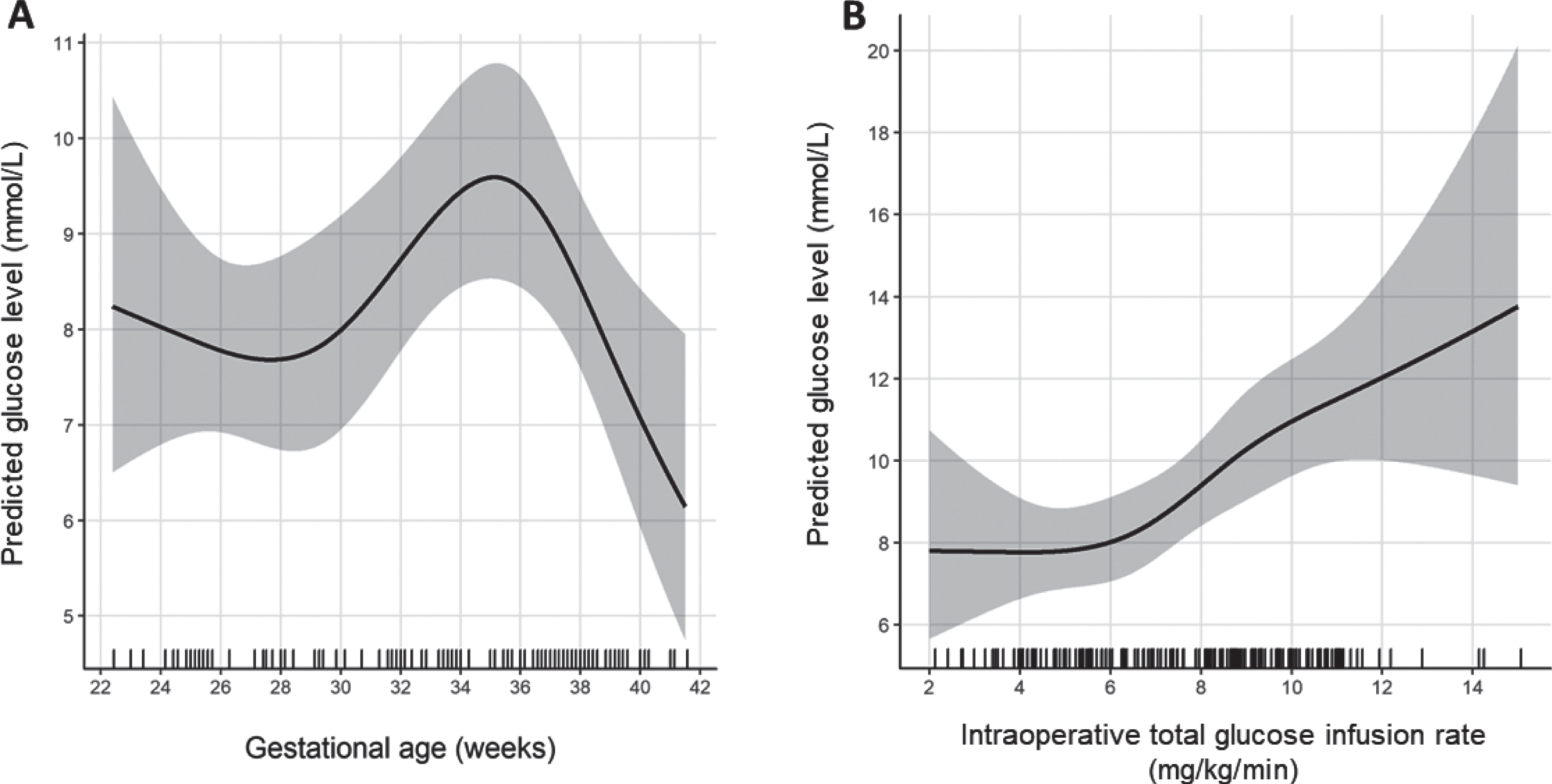
A) Effect of gestational age on postoperative glucose levels in the first 4 hours after surgery; B) Effect of intraoperative glucose infusion rate on postoperative glucose levels in the first 4 hours after surgery.
None of the patients required insulin ≤24 hours postoperatively. Hypoglycemia occurred in only 1 (0.5%) patient within 4 hours postoperatively. Mortality was 6 (7%) in the no hyperglycemia group and 3 (3%) in the hyperglycemia group (p = 0.31). As shown in Fig. 2, among non-hyperglycemic patients, 50.0% (95% CI = [40.3%, 62.1%]) were discharged by day 10; whereas, among hyperglycemic patients, 51.0% (95% CI = [42.0%, 62.1%] were discharged later, by day 13 (p = 0.93).
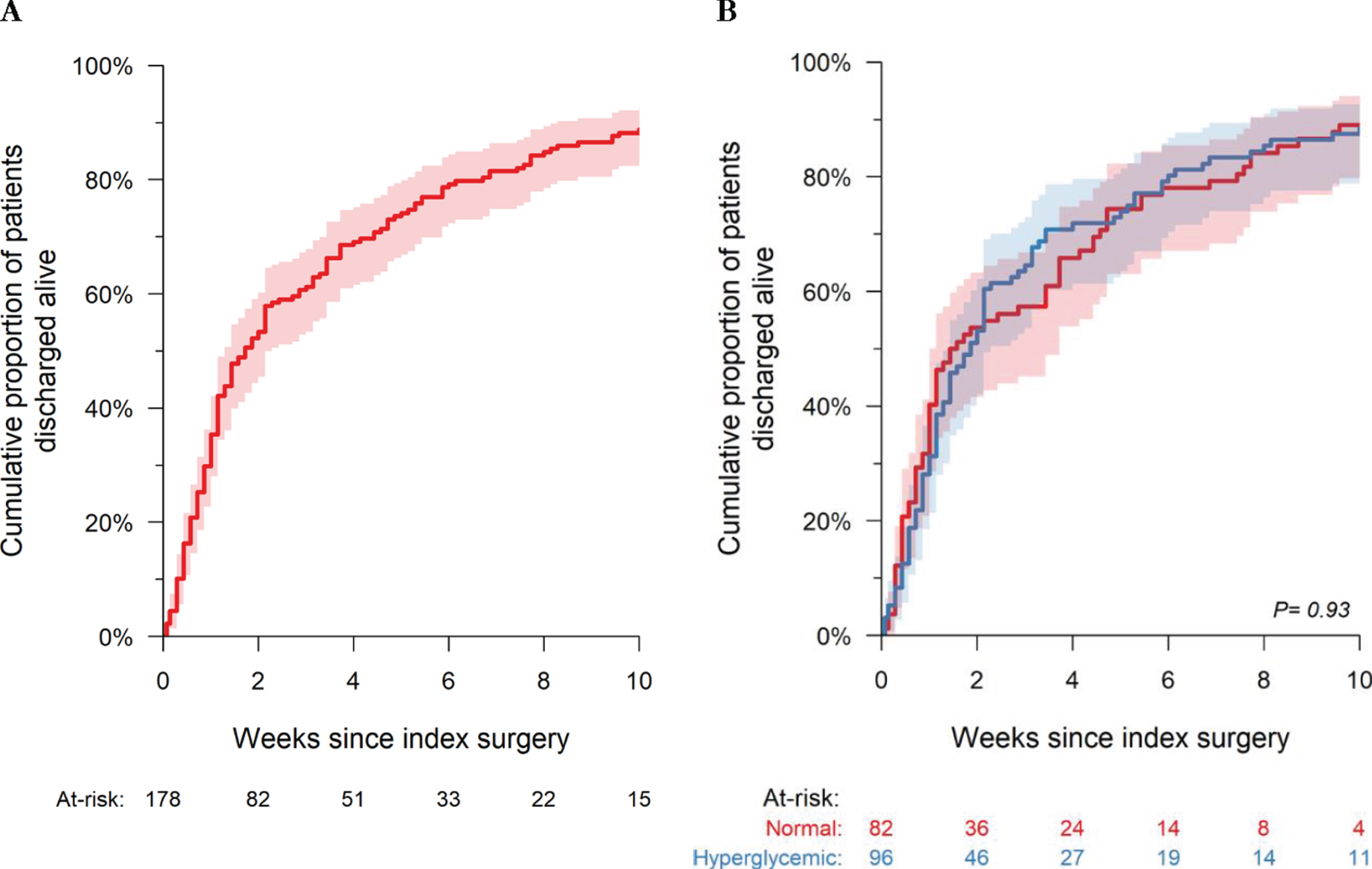
Competing risk analysis for mortality and length of stay for A) All cohort of neonates; B) Comparing patients with and without hyperglycemia in the first 4 hours postoperatively.
Our results add to the literature on the important topic of postoperative hyperglycemia in pediatric patients through the study of a predominantly general surgical NICU, in contrast with previous studies that included mostly pediatric cardiac ICUs. Our detailed analysis of the risk factors identified perioperative glucose infusion rate as a modifiable risk factor; and we also found a non-linear association between GA and postoperative glucose.
We found postoperative hyperglycemia in approximately 54% patients which is less than previous reports [9, 10] which reported rates of 80–90% among post-cardiac surgery pediatric patients, and defined hyperglycemia variably ranging from 6.1 to 12 mmol/L [5, 11]. Our lower rate may be due to differences in populations with more immature and younger patients in NICUs compared with pediatric/cardiac ICUs, and differences in the types of procedures. For example, previous studies included patients that underwent cardiopulmonary bypass [4, 8], whereas our cohort included mostly abdominal surgeries. Patients who undergo cardiopulmonary bypass frequently receive pre- and intraoperative steroids (21% in Moga et al. cohort [8] versus 3.3% in our sample) which may affect postoperative glucose. Our population had low rates of preoperative steroid use (n = 6) and they all occurred in the no hyperglycemia group. Due to this low preoperative steroid utilization, which may also be typical for other NICUs, we were unable to conduct meaningful analysis on the effect of steroids as a risk factor. In contrast to previous studies [8–10], we did not find that preoperative use of inotropic agents was associated with increased risk of postoperative hyperglycemia. However, inotrope use was infrequent in our cohort and our negative findings may be due to insufficient power. Despite this limitation, our preoperative study population and severity of illness is representative of the typical general surgical NICU.
None of our patients received interventions such as insulin, as reported by other publications [17]. In contrast to other studies [4, 10], we found no significant differences in the secondary outcomes of NICU LOS or mortality. However, LOS is more likely to be influenced by the underlying condition of the infant such as GA or diagnosis, rather than the complications of postoperative hyperglycemia.
Due to the heterogeneity of our study population, we were able to analyze a wide range of GAs as a risk factor. Importantly, GA was found to be a non-modifiable risk factor for postoperative hyperglycemia. Among preterm infants at GA < 35 weeks, a lower GA infant had lower postoperative glucose. However, at GA > 35 weeks, the relationship was reversed, with more mature infants having a lower postoperative glucose. To our knowledge, this is the first study reporting on an association between GA and postoperative glucose. The reasons for this non-linear relationship between GA and postoperative glucose require exploration. In the non-perioperative period, especially during the first week of life, preterm infants have a lower capacity for insulin secretion and peripheral glucose utilization that can increase the likelihood of hyperglycemia [12, 18]. Additionally, preterm infants are often subjected to higher GIRs and lipid emulsions in order to attain high caloric intakes to promote growth [19]. These factors can increase the risk for hyperglycemia. However, our finding that preterm infants who are more immature had a lower risk of postoperative hyperglycemia, demonstrates the complexity of metabolic interactions relating to glucose homeostasis across the GA spectrum.
In the perioperative setting, there are major alterations in glucose metabolism due to baseline illness and the stress of the procedure; and stress-induced hormones such as catecholamines, cortisol and glucagon are secreted with resultant inhibition of insulin secretion and action, and increased hepatic glucose production and glucose release [12]. Anesthetic agents induce lower metabolic rates and oxygen consumption which can affect baseline needs. Thus in an intact endocrine system, the perioperative setting creates a state of higher glucose production and decreased utilization which can result in hyperglycemia. It is postulated that more immature infants may not be able to fully generate these responses, and thus have blunted hormonal responses resulting in less hyperglycemia.
We found that the main modifiable factor associated with postoperative hyperglycemia was intraoperative GIR, with higher glucose intake associated with higher postoperative glucose. The majority of patients were receiving a GIR of approximately 7–10 mg/kg/min which, in the non-perioperative period, usually provides an adequate caloric intake for the promotion of postnatal growth. Glucose intake can be reduced preemptively to reflect the new metabolic state that the infant will be subjected to during the stress of the surgical procedure. Such interventions may decrease postoperative hyperglycemia and avoid the need for other interventions such as insulin [17]. While we found a very low incidence of hypoglycemia in the immediate postoperative period, any interventions aimed at preventing hyperglycemia should monitor for hypoglycemia which can also have adverse consequences [20, 21]. The Association of Paediatric Anaesthesia Consensus Guideline on Perioperative Fluid Management in Children state that the majority of children over one month of age will maintain a normal blood sugar if given non-dextrose containing fluid during surgery, but that neonates in the first 48 hours of life should be given dextrose, and that preterm and term infants already receiving dextrose containing solutions should continue with them during surgery [22]. However, these consensus guidelines do not provide specific details on glucose infusion rates. Our results provide some guidance on the GIRs that neonates can receive to decrease the risk of postoperative hyperglycemia. Recently, the Children’s Hospitals Neonatal Consortium, an international collaborative of which the Hospital for Sick Children is a member, have targeted quality improvement interventions to reduce postoperative hyperglycemia. At the Hospital for Sick Children, we have implemented perioperative protocols for fluid management which have been successful in reducing rates of postoperative hyperglycemia (see Appendix for protocol).
Our study had several limitations. The retrospective nature of this study did not allow for standardization of timing and frequency of glucose measurements. We selected a 4 hour postoperative timeframe to capture glucose values near the early postoperative period. We utilized a cut-off of 4 hours postoperatively as our unit protocol is to perform close glucose monitoring for 4 hours postoperatively or longer if abnormal; thereafter, the frequency of monitoring is not standardized. Thus, although our cut-off for duration of evaluation was 4 hours postoperatively, it was likely that glucose values remained normal beyond this period. Continuous glucose monitoring over a longer period of time would provide valuable information, and subcutaneous devices have been utilized in other studies for this purpose [23–25]; however, they may be difficult to implement for the most immature and sickest patients due to limitations in the technical size of the devices. The generalizability of our results should be limited to the populations with similar demographics; namely, neonates and young infants up to 2 months old, who are in NICUs undergoing general surgical procedures, with procedure duration of maximum 3 hours.
Clinical outcomes related to postoperative glucose are important to measure; however, this was beyond the scope the study. Moreover, adverse outcomes were rare in our cohort. We did evaluate mortality and the utilization measure of NICU LOS, which was not statistically different between groups. In adults, higher rates of surgical site infections have been reported with postoperative hyperglycemia [26]. Although we collected data on infection rates including surgical site infections, the event rates were very low (1 surgical site infection in each group) which precluded any meaningful analysis. The impact of prolonged compared with transient postoperative hyperglycemia on relevant clinical outcomes is also an important area for further research.
Conclusion
We found that postoperative hyperglycemia was a common event in surgical neonates. GA was identified as a non-modifiable risk factor and had a non-linear relationship with postoperative glucose. Intraoperative GIR was a modifiable risk factor that can have a significant effect on postoperative glucose. These findings provide support to perform preemptive interventions to decrease the incidence of hyperglycemia. Careful selection of perioperative fluids with GIRs adjusted to support a lower metabolic state and high stress during surgery/anesthesia may decrease the incidence of postoperative hyperglycemia and potentially improve outcomes.
Funding
The authors have no financial relationships relevant to this article to disclose.
Conflicts of interest
The authors have no conflicts of interest relevant to this article to disclose.
Footnotes
Appendix