
Abstract
BACKGROUND:
To investigate the use of calcineurin inhibitors (CNIs) in pregnant Japanese women and to evaluate their safety in infants.
METHODS:
Data were extracted from the claims database of the Japan Medical Data Center. The prevalence of CNIs was evaluated 180 days before pregnancy onset, during pregnancy, and within180-days post partum. We investigated the characteristics of the infants, including the presence of major malformations and their diagnoses, for 1 year after birth.
RESULTS:
A total of 91,865 pregnancies in 80,049 women were included. Fifty-three women were prescribed CNIs between 180-day before pregnancy onset and 180-day postpartum; 35 of the 53 women were prescribed the drugs during pregnancy, and 10 of their infants were born preterm. Three were diagnosed with major congenital malformations, such as patent ductus arteriosus. Six preterm infants presented with infant respiratory distress syndrome.
CONCLUSIONS:
No congenital anomalies were clearly attributable to the use of CNIs during pregnancy.
Introduction
Administration of calcineurin inhibitors (CNIs), tacrolimus, and cyclosporin A (CsA) is essential for recipients after solid organ transplantation to prevent rejection.
CNIs are also administered to patients with autoimmune diseases, such as systemic lupus erythematosus (SLE). SLE is a connective tissue disease designated as an intractable disease in Japan, and medical expenses for SLE were subsidized for approximately 61,835 patients in 2019 [1]. SLE is frequently observed in women in their 20 s and 40 s. Additionally, lupus activity is a predictor of poor pregnancy outcomes [2], and medications for SLE should be continued during pregnancy. Tacrolimus was prescribed to 20 of 132 (15%) pregnant Japanese women with rheumatic diseases such as SLE, anti-phospholipid syndrome, and rheumatoid arthritis (RA) [3].
Databases, including pregnancy cohorts, registries, and medical records, are widely used to evaluate drug safety. A drug-use survey of pregnant women with SLE in Sweden revealed that 1.9% of pregnant women used CsA [4]. The Japan Environment and Children’s Study, a nationwide birth cohort study, revealed that 0.67, 0.48, and 0.15% of pregnant women were using immunosuppressants and immunoregulatory medications before pregnancy diagnosis, before week 12 of pregnancy, and after week 12 of pregnancy, respectively [5].
In Japan, drug package inserts for CNIs were revised in 2018 based on overseas information, and pregnancy was excluded from the list of contraindications. Few studies have examined the safety of these drugs in the Japanese population. Izumi Y reported that two newborns born to patients with SLE were healthy for at least 3 years after birth [6]. Hiramatsu Y reported no adverse events in either the mothers or infants [7]. Another study reported that umbilical cord blood tacrolimus concentration at delivery was 71% that of the maternal blood [8]. In 2020, after revising the package insert, it was reported that an infant delivered by a mother who had undergone renal transplantation, whose umbilical vein tacrolimus level was within the therapeutic range, suffered acute kidney injury [9].
This study aimed to investigate the use of CNIs in pregnant Japanese women and evaluate the safety of their infants.
Methods
Source of data
Data were extracted from a large database of health insurance claims developed and maintained by JMDC Inc. (Tokyo, Japan) [10]. This database includes all inpatient, outpatient, and pharmacy claims received from insurers and is one of the largest claims databases in Japan. The claims included diagnoses classified according to the International Classification of Diseases, 10th revision (ICD-10), surgical and medical procedures, and prescribed medications. Standardized disease classifications and anonymous record linkages were used in the database [10]. Further details regarding this database can be found in our previous reports [11, 12].
Study population
We included mothers whose children were identified between January 2005 and November 2019, using the JMDC claims database. Mothers could be linked with their offspring through identification specific to each mother in the database if their infants were enrolled in the same health insurance society, which allows the identification of the month and year of birth (the date of birth is not made available to avoid re-identification), based on the infants’ eligibility information. We used a dataset made available on May 8, 2020, that included 7,447,761 men and women covered by health insurance between January 2005 and November 2019. Data of women who met the following eligibility criteria was extracted to evaluate prescriptions before, during, and after pregnancy: mothers whose infants were covered by the same health insurer during their birth month, mothers whose dates of pregnancy onset and delivery could be estimated, and those who exclusively belonged to one of several health insurance societies from 180-day before pregnancy onset through 180-day postpartum.
Estimation of the dates of pregnancy onset and delivery
Neither the date of onset of pregnancy nor the date of delivery was available in the database. Therefore, these were estimated using previously described algorithms [12].
The date of pregnancy onset was estimated by subtracting the gestational age recorded as part of the diagnosis at the time of a specific visit from the date of diagnosis. For example, when “delivery at week 39” was entered, 39 weeks and 0 day was subtracted. If a woman made several visits with diagnoses specifying the gestational age, the latest gestational age was used. Given that gestational age at delivery represents the best obstetric estimate for clinical care [13], the gestational age is likely to have greater accuracy in later stages of pregnancy. Based on an assessment using administrative data from a university hospital, 92.8% of the estimated pregnancy onset dates were within ±7 days of the gold standard date of pregnancy onset [14].
Delivery dates were estimated based on delivery-related entries described in our previous reports and the birth months of infants [12, 15]. An algorithm was developed in which the earliest dates of the selected diagnoses and surgical procedures were regarded as delivery dates [12, 15]. In cases without such diagnoses or procedures, the earliest dates of any other delivery-related entry, including diagnoses, surgical and medical procedures, or injectable medications, were considered delivery dates. Based on an assessment using administrative data from a university hospital, 96.4% of the estimated delivery dates were within 7 days of the gold standard delivery date [14]. If birth months and years were available, delivery-related entries were used only when the date was within the infant’s birth month. In Japan, delivery is not always covered by health insurance, and related information is not recorded when delivery does not require procedures or medications covered by health insurance. In such cases, the 15th day of the neonatal birth month was considered the delivery date.
Labor induction is recommended in post term pregnancies (pregnancies that reach or extend beyond 294 days of gestation) because of the increased risk of perinatal mortality [16]. When the difference between the estimated dates of pregnancy onset and delivery exceeded 294 days, a gestational period of 294 days was uniformly assigned, and pregnancy onset was considered 294 days before the estimated delivery date. Pregnancies were divided into the first (from pregnancy onset to week 13 day 6 of gestation), second (week 14 day 0 through week 27 day 6), and third (week 28 day 0 until delivery) trimesters.
Prescriptions of calcineurin inhibitors
Tacrolimus and CsA were the CNIs evaluated in this study. Topical agents and ophthalmic suspensions containing CNIs were excluded from the analysis. The dispensing date was preferentially used; if the dispensing date was unavailable, the admission date was alternatively used. Because the month and year were available for each claim, each drug was assigned to the 15th day of the month when neither dispensing nor admission date was unavailable. The days of supply for each prescription were available in the database and used to determine the timing of exposure.
Collection of subject characteristics
Data on the characteristics of patients prescribed CNI during pregnancy were collected from the database. The following maternal characteristics at delivery were collected: age, daily CNI dose, and gestational age. Additionally, data on indications for CNI use, presence of multiple pregnancies, and administration of drugs with high risk of teratogenicity (etretinate, carbamazepine, thalidomide, cyclophosphamide, danazol, thiamazole, trimethadione, valproate, vitamin A (retinol), phenytoin, phenobarbital, mycophenolate, misoprostol, methotrexate, and warfarin) were collated [16]. We also collected information on infant characteristics, including major congenital malformations (MCMs) and diagnoses, within 1 year of delivery. If the infant had a MCM or was diagnosed with a serious diagnosis, we examined the maternal diagnosis and drug prescriptions other than CNIs. MCMs were defined using ICD-10 codes Q00–Q89, excluding the following minor congenital malformations: Q10, Q162, Q17–Q182, Q184–Q189, Q250, Q270, Q381, Q515, Q516, Q520–Q527, Q53, Q664–Q666, Q69, Q70, Q81-Q84, Q950-Q952, Q954, Q955, and Q959. The MCMs in the claims were validated against patient medical records at a university hospital, and the overall positive predictive value was 91.5% [17].
Data analyses
First, the prevalence of CNI prescriptions 180-day before pregnancy onset, during pregnancy, and were described. The prescription prevalence was also calculated for 180–91 days and 90–1 day before pregnancy for each trimester and for 1–90 days and 91–180 days postpartum. The characteristics of mothers who were prescribed CNI during pregnancy and those of their children were reviewed. All data were analyzed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Among the 7,447,761 men and women covered by health insurance between January 2005 and November 2019, 91,865 pregnancies in 80,049 women met eligibility criteria (Fig. 2). Delivery dates were estimated based on the earliest dates of selected diagnoses and surgical procedures for 45,150 deliveries, earliest dates of any other delivery-related entries for 8,855 deliveries, and 15th day of the neonatal birth month for 37,860 deliveries. A term of 294 days was uniformly assigned to the gestational period for 1,415 deliveries (1.5%) whose gestational period exceeded this value. There were 5,045 records of CNI prescriptions among the 91,865 deliveries. The timing of exposure was estimated from 4,783 (94.8%) and 212 (4.2%) records based on dispensing and hospitalization dates, respectively. For the other 50 (1.0%) records, the 15th day of the month and year recorded for each claim was used.
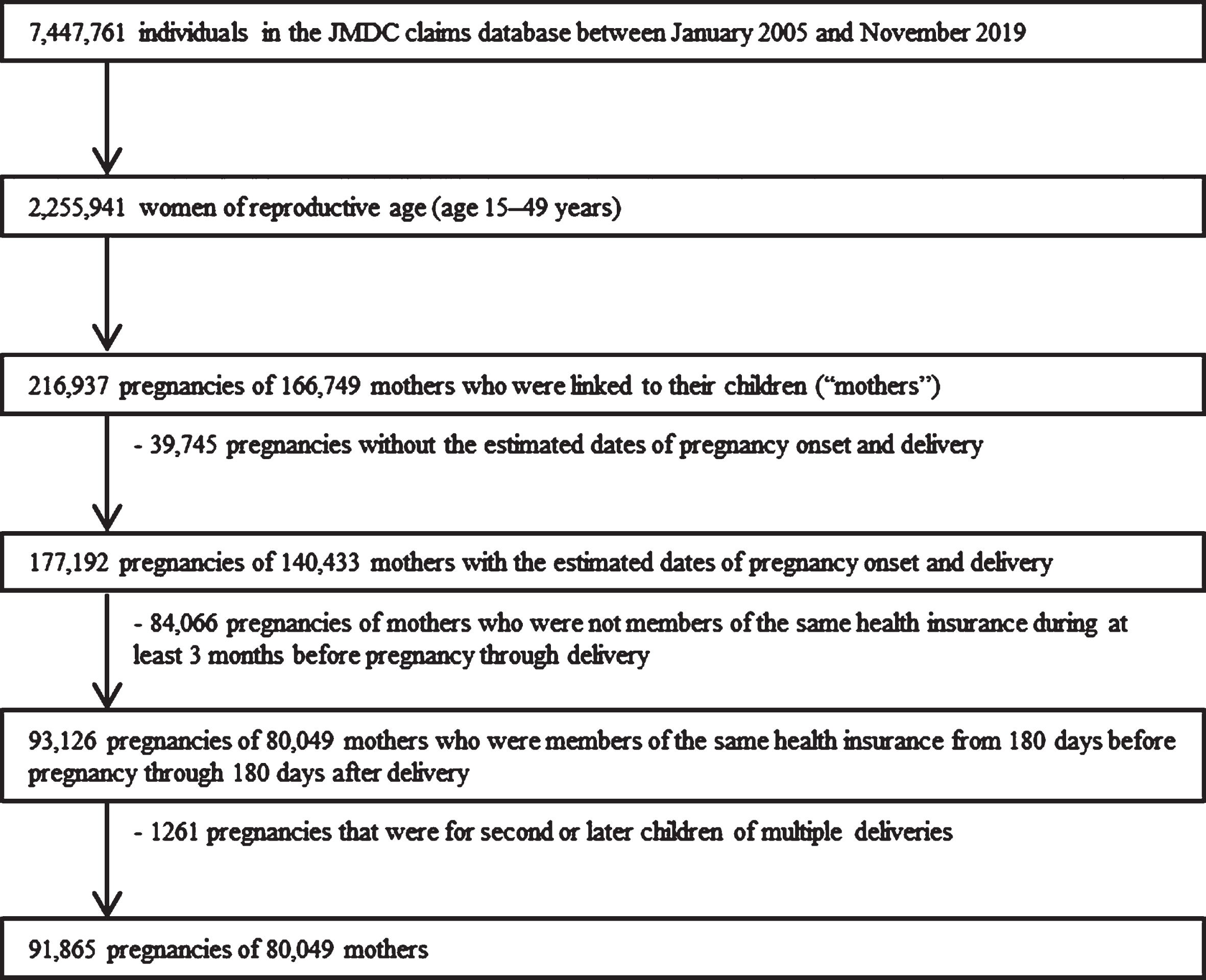
Flow chart showing the selection of the study population for data analysis.
The mean age at delivery and the length of gestation were 32.4 years (standard deviation [SD]:4.5 years) and 270.1 days (SD: 13.3 days), respectively. Of the 91,865 deliveries, 91,605 (99.7%) were in the third trimester. At least one CNI was prescribed to 53 (5.8 per 10,000 deliveries) of the 91,865 women between 180-day before pregnancy onset and 180-day postpartum (Table 1). In total, 39 (4.2 per 10,000 deliveries), 35 (3.8 per 10,000 deliveries), and 37 (4.0 per 10,000 deliveries) women received at least one CNI prescription within 180-day before pregnancy, during pregnancy, and within 180-day postpartum, respectively (Table 1). The prevalence of CNI prescriptions decreased during the gestational period. The prevalence of CNI prescription increased after delivery.
Calcineurin inhibitor prescriptions between 180 days before pregnancy and 180 days postpartum
Based on the claims data, 35 of the 53 women were prescribed CNIs during pregnancy. The clinical characteristics of the patients and their infants are presented in Table 2. Thirteen mothers had an advanced maternal age of≥35 years. The mean gestational duration was 253.3 days (SD: 29.7 days). Ten infants were born preterm, six of whom were delivered by mothers with SLE. Two of the infants (nos.16 and 17) had the same mother. Of the 35 mothers, 29 were prescribed tacrolimus; the remaining were prescribed CsA. Twenty-six women were diagnosed with autoimmune diseases, including SLE (n = 13), RA (n = 6), and ulcerative colitis (n = 4), before delivery. Two and six mothers underwent liver transplantation and renal transplantation, respectively. Seven preterm infants had infant respiratory distress syndrome (IRDS, International Statistical Classification of Diseases (ICD)-10: P220).
Characteristics of maternal patients administrated calcineurin inhibitor in pregnany period AD: Atopic dermatitis, AOSD: Adult-onset Still’s disease, BD: Behçet disease, CNI: Calcineurin inhibitor, CsA: Cyclosporin A, IRDS: Infant respiratory distress syndrome, LT: Liver transplantation, mg/d: mg/day, MG: Myasthenia gravis, NS: Nephrotic syndrome, PDA: Patent ductus arteriosus, PsV: Psoriasis vulgaris, RA: Rheumatoid arthritis, RT: Renal transplantation, SLE: Systemic lupus erythematosus, SSc: Systemic sclerosis , UC: Ulcerative colitis
Three infants were diagnosed with MCM. One infant (no. 27) was delivered in very preterm (Table 2). The prescriptions received by the mother during pregnancy are shown in Fig. 1. The mother was prescribed warfarin until week 7 and day 3 of gestation. Heparin was prescribed after 5 weeks of gestation. None of the patients were prescribed teratogenic drugs other than warfarin within 180-day before pregnancy. The infant was diagnosed with low birth weight (LBW, ICD-10: P071) and patent ductus arteriosus (PDA, ICD-10: Q250). Diseases diagnosed in the mothers before and after pregnancy are shown in Table 3. The mother had several cardiovascular diseases prior to pregnancy. She was continuously prescribed tacrolimus (3 mg) throughout pregnancy.
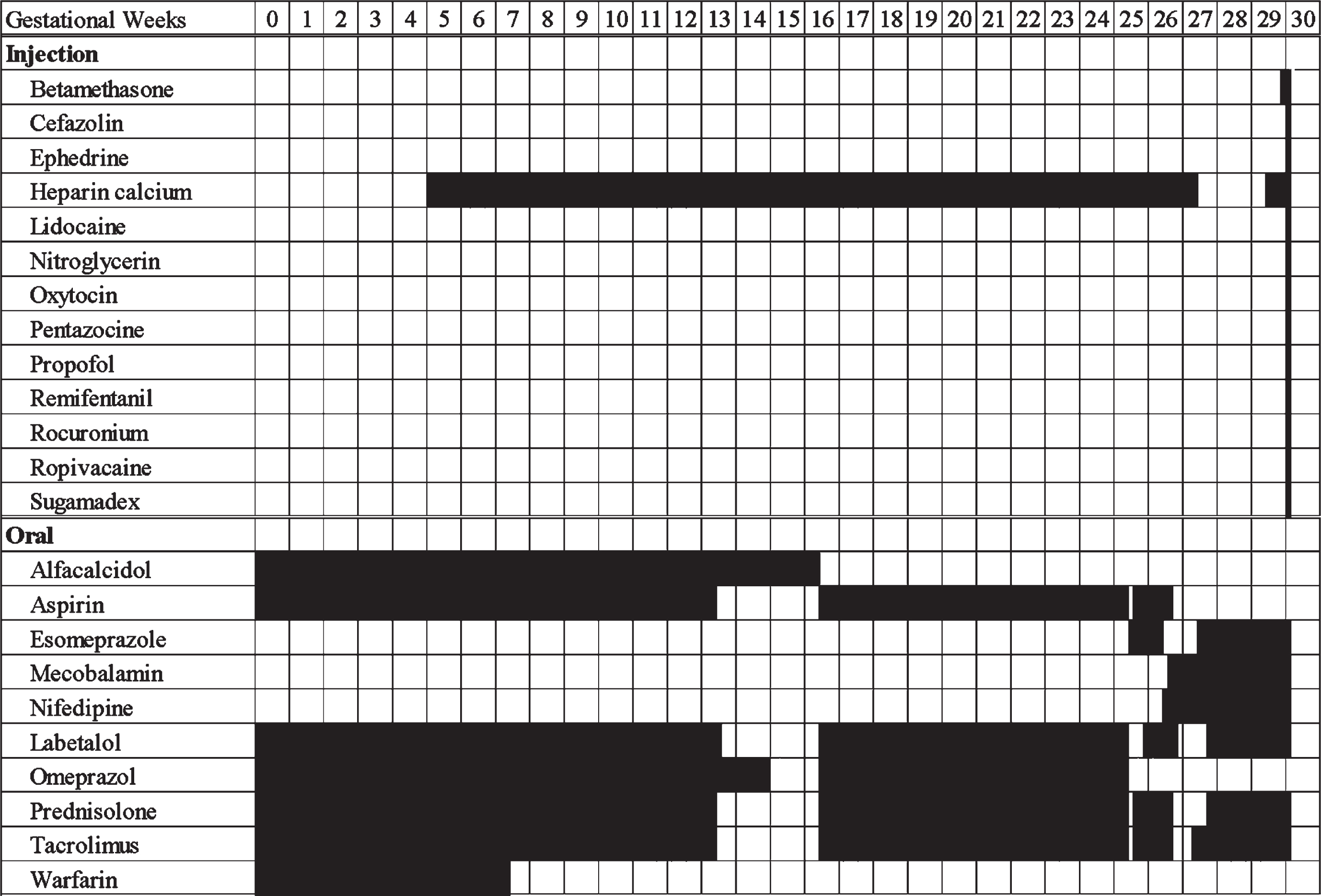
Administration schedule of the drugs between pregnancy onset and delivery in No.27 (Table 2) maternal patient. The maternal patient delivered her infant at week 30 day 1.
Disease names diagnosed before and after pregnancy onset in no. 27 (Table 2) maternal patient
Pregnant women are cautious about medications [18]. Similarly, physicians hesitate to prescribe drugs for these patients. In Japan, 15.1% of pregnant women are advised to visit other hospitals when they consult departments other than obstetrics [19]. Moreover, 1,628 consultations regarding medication use during pregnancy and lactation were forwarded to the cooperating medical institutions of the Japan drug information institute in pregnancy [20]. However, most of these consultations are based on research targeting foreigners whose physique and gene expression differ from those of the Japanese population, making it necessary to conduct surveys targeting only Japanese participants. The strengths of our research are as follows: 1) it is based on data targeting the Japanese population, and 2) long-term follow-up of infants was performed for 1 year after birth.
In a retrospective study of pregnant women with SLE, the prescriptions of immunosuppressive agents administered during gestation were lower than those administered before pregnancy [4, 5]. Our study also suggested a decrease in the number of patients prescribed CNIs after pregnancy onset. In Japan, the package insert for CNIs was revised in 2018, and pregnancy was excluded from the list of contraindications. Therefore, the number of patients who discontinue treatment during pregnancy may decrease.
Infants delivered by patients with SLE are at risk of renal failure caused by neonatal lupus [21]. Renal failure is a well-known adverse effect of CNIs. Zheng S reported that tacrolimus concentrations in the umbilical cord (6.6±1.8 mcg/L) are within the therapeutic range [8]. Aktürk S reported that the infant of a mother administered 7.6 mg/day of tacrolimus developed acute kidney injury due to tacrolimus exposure, although the maternal blood concentration was within an appropriate range [9]. Therefore, exposure to tacrolimus through the placenta may cause renal failure in infants. Although no infants were diagnosed with kidney injury in this study, medical staff and new mothers should monitor infants for decreased urine output and consider measuring blood CNI levels, depending on the infant’s condition.
Our study included two mothers who had undergone liver transplantation for primary biliary cirrhosis (no.6, ICD-10: K743) or autoimmune hepatitis (no.20, ICD-10: K754). These diseases may necessitate organ transplantation.
Approximately 5% of infants in Japan are born prematurely. Although few participants received CNIs during pregnancy, 28.5% of infants in our study were delivered prematurely. This rate clearly exceeds that of preterm births in Japan. Maternal diagnosis and medical history, such as SLE, RA, and liver transplantation, may be the associated factors in our study. <The previous reports revealed that> fifteen to fifty percent of infants of mothers with SLE are delivered prematurely [22–26]. Another study indicated that 14.8% of patients with RA delivered preterm infants [27]. Ten of 31 mothers delivered prematurely after liver transplantation [28]. <However, in our study, we could not determine whether tacrolimus administration increased the preterm birth rate.> Tacrolimus administration to mothers with SLE did not affect the risk of preterm birth [29]. Nevers W mentioned that preterm delivery in tacrolimus-administered patients was related to the maternal condition and not to medication [30].
Pulmonary surfactant production is insufficient in infants born at <34 weeks gestation. The Safe Labor Consortium reported that IRDS was diagnosed in 10.5, 6, 2.8, 1, and 0.3% of infants born at the 34th, 35th, 36th, 37th, and≥38 weeks of gestation, respectively [31]; however, there were no reports concluding that IRDS was caused by CNI intake. In our study, six of the seven infants with IRDS were born preterm, and four of them were born at < 30 weeks of gestation. A full-term infant with IRDS (no.7) was diagnosed with “newborn affected by slow intrauterine growth, unspecified (ICD-10: P059).” IRDS in our study may have been caused by premature birth or slow intrauterine growth.
Two infants were diagnosed with sepsis, and one was diagnosed with congenital pneumonia. For the infant with sepsis (no.22), there was a time lag of more than two months from birth to the diagnosis of sepsis. The cause of the infection may not be exposure to the drug via the placenta. In contrast, the infants nos.12 and 33 were born extremely preterm and diagnosed with infectious disease at birth. The incidence of early-onset sepsis is very high among infants born at 22–28 weeks gestation (adjusted relative risk [RR]: 18.47, 95% confidence interval [CI]: 14.57–23.38) [32]. Premature birth may have contributed to the development of infectious disease.
Three of 35 infants (8.6%) in the present study were diagnosed with MCM. This rate was generally higher than that of malformations in the general population. Two infants with MCM were born to mothers with advanced maternal age of≥35 years. In a Japanese study, maternal age≥35 significantly increased birth defect risk (RR:1.89, 95% CI:1.23–2.91) [33].
Infants diagnosed with PDA were delivered by mothers diagnosed with SLE (nos.21, 27, and 33). Two of the three infants (nos.27 and 33) were delivered prematurely. PDA is often associated with premature birth and is observed at 4 days of age in 10% of infants born at 30–37 weeks of gestation [34]. PDA in infants delivered by mothers diagnosed with SLE is not directly caused by the mother’s condition [35]. In our study, one mother (no.27) was prescribed warfarin (probably for treating a cardiovascular disease), which is associated with a high risk of teratogenicity. Hou JW reported that infants delivered by mothers who were administered warfarin during pregnancy had PDA [36]. In our study, the mother was prescribed a heparin calcium injection, and ongoing warfarin therapy was discontinued after 5 weeks of gestation. It is highly likely that treatment was switched because of the discovery of pregnancy. Chan WS reported that replacing oral anticoagulants with heparin before 6 weeks of gestation reduced the risk of congenital fetal anomalies, including PDA [37]. Although the effects of warfarin cannot be completely ruled out, we hypothesized that preterm birth is the most significant contributor. However, one mother (no.21) with SLE and adult-onset Still’s disease (AOSD) delivered at full term. To the best of our knowledge, there have been no previous reports on the association between AOSD and PDA. Advanced maternal age may have contributed to the development of PDA because the mother was≥35 years at the delivery. Nevertheless, further studies are needed to rule out the adverse effects of CNIs.
Infant no.33 who had extremely LBW was diagnosed with congenital laryngomalacia (ICD-10: Q315). LBW is a strong predictor of laryngomalacia [38]. No reports have shown that drugs, including CNIs administered to the mother, are risk factors for the disease. We believe that LBW contributed the most to the development of laryngomalacia. Additionally, the infant had various comorbidities, such as retinopathy of prematurity (ICD-10: H351), hypothyroidism (ICD-10: E039), and necrotizing enterocolitis of the newborn (ICD-10: P77-). We believe that premature birth is the most important risk factor for these diagnoses [39, 40]. However, the infant had congenital tricuspid stenosis (ICD-10: I070). The cause of this disease is currently unknown, and information regarding its association with maternal medications is lacking.
This study has several limitations. First, it is based on data from a claims database. Therefore, the actual date of administration may not have been accurately reflected. Second, we could not collect data on the concentration of CNIs in the blood and breast milk. It is possible that the infants received doses of CNIs that differed significantly from expected doses. Third, maternal adherence to medication was not considered. Based on the estimated duration of drug use, there was a period during which mothers were not prescribed CNIs. We could not confirm whether the physician intentionally stopped the administration of CNIs or adjusted the number of prescription days because of poor maternal compliance. Fourth, this study included mothers from a claims database who could be linked to their liveborn children. We were unable to evaluate the safety of CNIs prescribed to women whose pregnancies ended in abortion or stillbirth.
Conclusion
Using the claims database, we found no congenital anomalies that could be attributed to CNI use during pregnancy.
Ethics statement
This study was approved by the Institutional Review Board of the Tohoku University School of Medicine on July 19, 2016 (registration number: 2016-1-230).
Footnotes
Acknowledgments
This work was supported by the Ministry of Health, Labour and Welfare of Japan under Grant (19K09746 and 20K16070). The authors would like to thank the Research Group for Health Administrative Data and Japan Medical Data Center Co., Ltd.
Disclosure statement
Tomofumi Ishikawa is an employee of Pfizer R&D, Japan. Tomofumi Ishikawa is also a research collaborator at Tohoku University and contributed to the present study independently of Pfizer R&D, Japan.